Embed Size (px)
Citation preview

Journal of Oral Health and Dental Care
Open AccessReview Article
Multiple Radiographic Analysis (Systemic Disease): Dental Panoramic Radiography
Plauto Christopher Aranha Watanabe*, Vanessa Faria and Angela Jordão CamargoDepartment of Stomatology, Public Health and Forensic Dentistry, School of Dentistry of Ribeirão Preto, São Paulo University, Brazil
*Corresponding author: Plauto C. A. Watanabe, Email: [email protected]
Received: 16 November 2016; Accepted: 20 January 2017; Published: 27 January 2017
Abstract The purposes of this report, “Multiple Radiographic Analysis
(Systemic Disease), dental panoramic radiography” will be interpreted conditions which are spread out within the body rather than localized strictly to the tissues of the oral cavity. Our main goal is discussing different possibilities for analysis and research, highlighting a few different publications in this theme of study, using initial panoramic radiographic findings which have suggested widespread diseases of significance enough to affect the patient’s longevity and quality of life.
Keywords: Panoramic Radiography; Systemic Disease; Radiographic Analysis
IntroductionPanoramic radiography as a radiographic technique that produces
an image that includes both maxillary and mandibular dental arches and the surrounding structures as the maxillary sinus, nasal fossa, temporomandibular joints, styloid processes, and hyoid bone [1]. Although dentists might only concentrate on teeth and their supporting tissues when the examining panoramic radiographs, they should also be able to identify all other structures that appear in the image [2-4]. Panoramic imaging (also called ortopantomography) is a technique for producing a single image of the facial structures that includes both maxillary and the mandibular dental arch and their supporting structures. Paatero and Numata were the first to describe the principles of panoramic radiography [5].
During performance of this technique patient remains motionless while the x-ray source and the radiographic sensors move in opposite direction at one or more centers of rotation. These pivot points can be internal or external focal layers. Focal layer tomography or “focal plane” or “image layer” is the plan which is not blurred in the radiographic image. The panoramic radiography or pantomography is produced using tomography curved surface and it is performed by rotating a narrow radiation beam in a horizontal plane around a point / virtual axis (called rotation center) positioned within the oral cavity. Film / sensor head move in the opposite direction around the patient, who remains static. The blurring is determined by:
● Tube distance;
● Focal plane distance;
● Film distance;
● Tube rotation orientation.
The rotation center changes as the film / sensor and rotate head, allowing the image layer to adapt to the elliptical shape of dental arches. Horizontal and vertical dimensions are correlated only when the object is within a particular zone or cutting plane representing the image layer, which is better interpreted as the focal layer. In fact, this
zone corresponds to a three-dimensional area in which the structures are fairly focused or well defined. Thus, the patient should be positioned at the X-ray device should be such that the dental arches are positioned strictly within this cutting area, resulting in a sharp image of the teeth. Thus, each extra oral X-ray panoramic apparatus manufacturer recommends different layers of cutting, because, of course, dental arches are very different around the world.
The best and most modern equipment allows reaching the most different types of dental arches, always with maximum detail.
The Focal Layer is Determinative• From distance of the center of rotation to the central plane of the
image layer.
• For the wide long distance slot, narrow (the narrower the beam, the highest the layer of the image).
• Changes in film speed changes the position of the image layer.
• Increased film speed = the farthest image rotation center.
• Decreased film speed = image closer to the center of rotation.
So, it is like the image layer is formatted to match the different types / shapes of the dental arches. As a rule, the anterior region of the shear layer is narrower. Depending on the manufacturer, the number and position of rotating centers differ.
Advantages of Panoramic Radiograph• It has a unique dental examination by a panoramic representation
of the stomatognathic system, including temporomandibular joint (TMJ), styloid processes and maxillary sinuses;
• It allows the detection of functional and pathological relationship and its effects on the stomatognathic system;
• Provides a document to the treatment and preservation plan;
• Reduces radiation exposure by means of a rotational strategic system covering a large area (Figure 1).
Disadvantages of Panoramic Radiograph• Patients with extreme dental relations class II and III make it
impossible to obtain of great pictures of the segments of anterior teeth;
• The ratio for the focus-object object-film distance is not the same in all cases, resulting in a factor of constant expansion;
• Precise measurements are questioned;
• Structures that reside outside the focus layer can be superimposed on normal structures of the jaw and simulate pathology;
• Technical errors.
Prior IndicationsThe Panoramic Radiograph is indicated mainly in the first visit
of patients who refer to the dentist for a routine visit and / or specific needs such as pain, aesthetics, etc. In addition to this main indication, panoramic radiographs are usually indicated in situations where there is:
• A real suspicion, based on a clinical examination, extensive and / or active pathology outside the alveolar bone;
• Problems with third molars symptomatic in which the likely treatment will be followed;
Copyright © 2017 The Authors. Published by Scientific Open Access Journals LLC.

Citation: Watanabe PCA, Faria V, Camargo AJ. Multiple Radiographic Analysis (Systemic Disease): Dental Panoramic Radiography. J Oral Health Dent Care 2017; 1:007.
J Oral Health Dent Care 2017; 1:007Volume 1, Issue 1Watanabe et al.
based on the principle of radioprotection ALARA, or either, we must always use the lesser possible amount of radiation for the attainment of diagnostic information of our patients [8].
In addition, panoramic examinations may have the advantage of reduced radiation dose, cost and imaging of a larger area instead of periapical radiographs which have higher resolution in the image, particularly in the search for detail, for example, an accessory root canal. Panoramic radiography is effective in dental diagnosis and treatment planning [1]. Specifically, the status of dental development can be assessed using panoramic radiography. Third molars also should be evaluated in this age group for their presence, position, and stage
• Symptomatic problems with third molars with a likelihood that the treatment will be followed;
• Assessment for placement of dental implants;
• Trauma involving more than one tooth or suspicion of underlying bone damage;
• Participation periodontal involving “exchange” widespread with more than 5 mm, in which the equivalent diagnostic information needs more than 3 intraoral radiographs;
• Multiple extractions, in which the equivalent diagnostic information needs more than 3 intraoral radiographs;
• Evaluation of the growth and development of the maxillo-mandibular complex for orthodontics / orthopedic and orthognathic surgery.
In the context of panoramic radiographic image, there are several areas of interest for analysis / interpretation of extra oral radiographic technique (Figure 2), and the great view of the teeth, that is able to provide rich details in several other regions.
With the arrival of digital images and their image manipulation tools the radiographic Interpretation became more precise, and even increased this capability of diagnosis and radiographic analysis, for example, enabling the visualization of small carious lesions, excess / lack of material restorers, caries recurrence, etc. (Figure 3).
“The Selection of Patients for X-Ray Examination”, US Food and Drug Administration Center for Devices and Radiological Health (FDA/CDRH) guidelines were first published in 1987 spurred by concern about the US population’s total exposure to radiation from all sources. These referential guidelines were updated in 2004 following work by a joint panel of the American Dental Association and FDA [6]. The updated guidelines expanded the use of panoramic examination as an alternate baseline dental radiographic examination, recognizing that panoramic technology has improved. The latest version is the Dental Radiographic Examinations: Recommendations for Patient Selection and Limiting Radiation Exposure (revised 2012) [7]. The authors highlight that the panoramic x-ray is used in the routine of all the types of patients. Its use also has endorsement of “Ordinance 453 of the Health Department – ANVISA – Brazil”, in the recommendation
Figure 1: Simulation of the beam in fan-shaped collimated output hillock in the X-ray equipment.
Figure 2: Areas of interest in the panoramic radiograph for radiographic interpretation.
B
A C
Figure 3: Digital panoramic images demonstrating some image manipulation tools such as zoom (A and C), and Smart sharpening application filter (B) that allows you to analyze details such as decay, lack / excess restorative materials, and bone quality (cortical and trabecular).

Citation: Watanabe PCA, Faria V, Camargo AJ. Multiple Radiographic Analysis (Systemic Disease): Dental Panoramic Radiography. J Oral Health Dent Care 2017; 1:007.
J Oral Health Dent Care 2017; 1:007Volume 1, Issue 1Watanabe et al.
osteoporosis since they are correlated with systemic bone mineral density (BMD) values measured with dual-energy x-ray absorptiometry (DXA). Another factor to study is the Fractal Dimension, trabecular area per total area (TrA/TA), and connectivity on PR. Moreover, fractal dimension (FD) of trabecular bone has been associated with bone strength [15,16]. However, little is known on the difference in diagnostic performance among the above-mentioned methods. Thus,
of development. Taking posterior bitewing radiographs of new adult patients was found to be reducing the number of radiological findings and the diagnostic yield of panoramic radiography. In addition, the following clinical indicators for panoramic radiography were identified as the best predictors for useful diagnostic yield: suspicion of teeth with periapical pathologic conditions, presence of partially erupted teeth, caries lesions, swelling, and suspected unerupted teeth and agree with the Guidelines when it cites that from 30 to 50 percent of edentulous patients have exhibited abnormalities in panoramic radiographs [7].
The main disadvantage of panoramic radiology was that the image does not display the fine anatomic detail available on intraoral periapical radiographs. However, with the implementation of modern digital systems, many of these limitations are now in the past [9].
Dental AnomaliesFusion and gemination is not an uncommon finding and has
affected most primary dentition and permanent maxillary incisors, and the authors reported an unique case in literature involving a posterior molar, first seen on a routine panoramic radiograph (Figure 4) and confirm by axial CBCT (Figure 5), assuming being a fusion of the second and third molars or gemination/twinning of a second molar [9]. In case of endodontic involvement several articles report technicians of successful non-surgical endodontic treatment [10,11]. The authors concluded that the alteration, although it is common in other regions, did not have any case in the literature involving “second and third” molar. Highlighting those patients also has numerous anomalies, agenesis of 35 tooth and forth molar presence. In this case, the radiology does not close diagnosis, but brings an important discussion about possible dental findings and shows the importance of a great clinical judgment and evaluation.
Radiomorphometrics IndicesPanoramic radiomorphometric indices can be correlated and
compare precision, sensitivity and specificity by analyses of fractal dimension (FD) for screening low bone mineral density (BMD) [12]. The authors highlighted the panoramic radiography in this context because it is commonly used as an initial dental examination. Furthermore, it is fast and low-cost and uses low-dose X-radiation. PR are useful to diagnose systemic [13] and alveolar bone quality by assessing the width and shape of the inferior mandibular cortex [14]. These measurements have been described as indices to predict
Figure 4: Initial panoramic radiography of patient. Observe the mandibular right side. Below, periapical and Cone Beam tomography of the same region show details about the Double Tooth.
Figure 5: Axial view; the sequence showed initially three separate roots (IMG: 23 and 24), the next slice begins “fusion” of the mesial root with the “median” root. Slices IMG: 26 and IMG: 27, the pulp chamber is shared (the junction of the pulp chamber or the pulp portion of these roots), and finally showed the union, the mesial and median root are covered by dentin and is seen the distal root canal.

Citation: Watanabe PCA, Faria V, Camargo AJ. Multiple Radiographic Analysis (Systemic Disease): Dental Panoramic Radiography. J Oral Health Dent Care 2017; 1:007.
J Oral Health Dent Care 2017; 1:007Volume 1, Issue 1Watanabe et al.
• The ratio of the thickness of the mandibular cortex (measured along a line perpendicular to the mandible base at the level of the center of the mental foramen) to the distance between the inferior margin of the base of the mandible and its maximum limit
• Normal cortex for thickness greater than or equal to 3 mm and abnormal cortical density for thickness lower than 3 mm.
For qualitative analysis, the same set of radiographs was also classi-fied according to the mandibular cortical index (MCI) of Klemetti [19], which qualita tively evaluates the endosteal border of the man dibular cortex, classifying it as C1 (normal) when smooth and homogeneous, C2 (low density) when exhibiting half-moon defects, and as C3 (osteo-porosis) when porous with tapered and thinned cortical width.
In order to determine the QQPI index (qualitative and quantitative panoramic index), the two analy ses are combined for the same panoramic radio graph, yielding the following classifications: Q1 = mandibular cortex classified as C1, accord ing to MCI, and PMI ≥ 3 mm; Q2 = mandibular cortex classified a s C 2, according to MCI, and PMI < 3 mm; Q3 = mandibular cortex classified as C3, according to MCI, and PMI < 3 mm.
The index applied in the present study (QQPI) proposes the use of both methodologies suggested by the mentioned authors [19,21], combining quantitative and qualitative analyses of the mandible and observing both the thickness and aspect of the mandibular cortex in determining density, with three possible diagnostic outcomes: normal (Q1), low density (Q2) and osteoporosis (Q3). In conclusion, the authors rated that the results of this study allowed confirmation of digital panoramic radiography as a useful method for detecting morphologic age-related changes in the mandible and creation of a single quantitative and qualitative panoramic in dex (QQPI) to aid in the diagnosis of mandibular low density /osteoporosis.
Camargo et al. [22] has conducted a study comparing two radiological methods evaluation of bone density in postmenopausal women.
They selected panoramic radiography images and carpal radiography, corresponding to 68 female patients, aged between 49 and 80 years old. For the evaluation of radiological images obtained by the carpal radiography (Figure 7) it was applied the method of the radiogrammetry. According to the results of this study it is possible to conclude that there is correlation between the presences of a mandibular bone density low level observed in the radiograph panoramic patients in the sample, with the low bone density presented in the carpal radiography [22].
In another similar study also use panoramic radiography [23] has aimed to analyze the importance of panoramic and carpal radiographs for evaluation of edentulous individuals in different ages, demonstrating the contribution of different dental radiographic techniques in detecting patients with signs of osteoporosis. The panoramic radiographs were performed to measure the thickness of the mandibular cortical index (mental index—MI and gonial index—GI; Figure 8), and evaluation of the morphology of the mandibular cortical shape (Klemetti classification).
The authors concluded that there was positive correlation between age and indices of quantitative assessment (IM, IG, BMI) and qualitative (analysis Klemetti) on panoramic and carpal radiographs. Age is a risk factor for the onset of osteoporosis.
Dental DiagnosisCamargo et al. [24], has reported a case of the undifferentiated
osteosarcoma of the mandible oblique line first seen on panoramic radiographs for patient who had their appointments in private radiology dental clinics for implants planning [24]. According to World Health Organization (WHO), osteosarcoma (OS) is the most common primary
the aim of this study was to assess the diagnostic performance of panoramic radiomorphometric indices and parameters in detecting low bone density. The authors concluded that the analyzed test, FD offers a significant and relatively high sensitivity, for screening low systemic bone density. Furthermore, the diagnostic performance results and significant correlations found in this study suggest that it is possible to obtain evidences of the trabecular bone pattern by assessing panoramic radiographic images.
Alonso et al. [17] studied validation of cone-beam computed tomography as a predictor of osteoporosis using the Klemetti classification. The authors have concluded that individuals with osteoporosis are also more likely to show erosions; thus, individuals could be classified into three distinct groups: C1 – the margin of the cortex is clear and sharp on both sides; C2 – endosteal surface defects are semi lunar; C3 – the cortical layer is extremely porous (Figure 6) [17]. A systematic review evaluated the accuracy (relative to DXA) of the different panoramic morphometric indices, and, based on the findings, it suggested future studies to examine ways of controlling the limitation of the magnification/distortion of PAN in order to attain more reliable conclusions precisely [18]. Seeking to address this limitation, the present study aims at evaluating the validity of CBCT in assessing mandibular bone quality using the Klemetti classification of inferior mandible morphology for the diagnosis of mandibular bone quality. To this end, the classification obtained from CBCT images was compared to that derived from panoramic images. It was concluded that The Klemetti index [19] should not be used to assess osteoporosis on CBCT cross-sectional slices; on the other hand, this imaging modality has great potential for performing osteoporosis analysis, because the inferior mandible cortex is given visibility in its extension by dynamic evaluation.
Haddad et al. [20] has devised a qualitatively and quantitatively reliable index for screening chan ges in mandibular bone density based on digital panoramic radiographs [20]. The quantitative analysis was based on the panoramic mandibular index8 (PMI) proposed by Benson et al. in 1991, which defines [21]:
Figure 6: Drawing and panoramic radiograph cuts to exemplify the Rating or Index of Klemetti.

Citation: Watanabe PCA, Faria V, Camargo AJ. Multiple Radiographic Analysis (Systemic Disease): Dental Panoramic Radiography. J Oral Health Dent Care 2017; 1:007.
J Oral Health Dent Care 2017; 1:007Volume 1, Issue 1Watanabe et al.
malignant tumor of bone, accounting for approximately 35 percent of cases, followed by chondrosarcoma (25%), and Ewing sarcoma (16%), and occurs predominantly in patients younger than age of twenty, and in this group 80% occur in long bones of the extremities [25]. Osteosarcoma of the jaw (JOS) is a rare, aggressive malignancy constituting 5% to 13% of all cases of skeletal OS [26]. The signs and symptoms of JOS include pain, parestesia, regional swelling and the patients can report loose teeth, changes of teeth position or changes in prosthesis adaptation [27].
The diagnostic is obtained through the X-ray examinations, Computed Tomography (CT) and pathologic analyses. Panoramic radiography remains the primary way of diagnosis, in which the image “sun ray” shows pathognomonic signal, although CT images provide high quality and excellent anatomic resolution, providing visualization of tumor calcification and cortical bone involvement, being of great importance in the diagnostic and treatment planning. The emergence of this disease at the trigonoretromolar region (oblique line) is the novelty of this clinical case. In the most cases the growth of the lesion is low.
The case report presented a Caucasian patient, female, 82 years old, who consulted a private dental radiology clinic to perform radiographic
documentation for placement of implants. During anamnesis reported difficulty to open the mouth. In the clinical evaluation, it was detected a discrete area of fibrous consistency, asymptomatic, with no changes in color and volume in the oral mucosa, located in the right retromolar triangle. Panoramic radiographic examination showed radiopaque area with a sun-ray appearance located above the external oblique line on the right side (Figure 9).
The important point in this case report is the fact that the lesion was a radiographic finding. Despite the patient had reported difficulty to open the mouth, she showed no symptomatology described previously. Another point was the sex and age of the patient. The lesion found in the panoramic radiograph can generate other diagnostic hypotheses. The fibrous dysplasia involving the jaws, the disease tends to appear in the early stages in life. The classic radiographic appearance is a “groundless” or “orange peel” effect, a mixed pattern of radiolucent, showing irregular and heavy radiopaque foci; this has been described as a “smoke” pattern [28]. Osteomyelitis of the jaws of a chronic nature has findings consistent with swelling, pain, purulence, intraoral or extra oral draining fistulae; positive radiographic finding is lesion with diffuse sclerosing [29].
Osteoma is a benign osteogenic lesion characterized by the proliferation of compact or trabecular bones, clinically, the peripheral osteoma is usually asymptomatic but can cause swelling and asymmetry, radiographically the lesion appears as a well-circumscribed radiopacity [30]. The final diagnosis is made by biopsy and histopathological analysis. In this reported case, it was performed an m-resection of the mandible. Resection with surgical margins is the most important factor for prognosis and provides a 5 years survival rate of 80% [31]. Bony margins for resection should at least be 2 cm from the clinical radiographic edge or the nearest suture in the mid face. Soft tissue margins around an osteosarcoma resection should be 2 cm or more assessed with frozen section. Adjuvant chemotherapy or radiotherapy seems to be efficacious [32]. The treatment of osteosarcoma of the jaws should be approached in two ways. Radical surgery is the primary treatment for (OS) of long bones as well as jaws, although it cannot be contemplated as the sole treatment. The additional use of radiotherapy was left to the discretion of the treating physician but was generally encouraged in cases of incomplete resection [33].
The clinical importance of this case report is that the lesion was a radiographic finding, since the patient had no symptoms, and the diagnosis was made due the indication for placement of implants. The diagnostic is obtained through the x-ray examinations (panoramic, periapical, occlusal), CT and pathologic analyses should be the earliest possible. Prognostic is associated with several variables, such as tumor location, initial size, existence or absence of metastasis, gender, age, cytogenetic chances and responds to chemotherapy pre-surgery.
While panoramic radiograph should not be prescribed primarily for
Figure 7: Measurement of Metacarpal Index using Radioimp software.
Figure 8: Mental index—MI and gonial index.
Figure 9: Panoramic radiograph showing the radiopaque lesion with a sun-ray appearance located above the external oblique line on the right side.

Citation: Watanabe PCA, Faria V, Camargo AJ. Multiple Radiographic Analysis (Systemic Disease): Dental Panoramic Radiography. J Oral Health Dent Care 2017; 1:007.
J Oral Health Dent Care 2017; 1:007Volume 1, Issue 1Watanabe et al.
detection of non-maxillofacial conditions, it is incumbent upon the health practitioner to be cognizant of panoramic image features that are indicative of systemic health.
Systemic DiseaseHypoparathyroidismMendonça et al. [34], has studied the impact of PhPT on bone mineral
density (BMD), on the frequency of subclinical vertebral fracture and on mandible morphometry [34]. The bone mineral density (BMD) of lumbar spine, total hip and 1/3 radius, radiographic evaluation of vertebral morphometry, panoramic radiography of the mandible, and biochemical evaluation of mineral metabolism and bone remodeling were evaluated in both groups. In the panoramic radiography were projected areas of interest that are used for the determination of the Mental Index and Goniac Index, as previously described [35,36]. The results show that panoramic radiography of the mandible is a useful tool for the recognition of bone disorders in PhPT. Furthermore, the panoramic radiography of the mandible was especially useful to capture the reduction in cortical thickness in another bone site. These results suggest that PhPT has a great impact on bone structure which is not necessarily detected by BMD density. Subclinical vertebral fracture was identified in more than 60% of PhPT patients, including those exhibiting high BMD. Panoramic radiography of the mandible should be thoroughly scrutinized to determine its place in the diagnosis or screening of osteoporosis. This site was useful to reveal cortical changes in PhPT. Panoramic radiography has the additional advantage of relying on a dentist for the screening of osteoporotic patients. The study encourages further investigation to determine the role of PTH as hormone replacement therapy in postsurgical hypoparathyroidism.
HyperparathyroidismMendonça et al. [37] has also studied the Skeletal and metabolic
characterization in primary hyperparathyroidism (HPTP) before and after the surgical cure to assess quantitatively the evolution of bone marrow adiposity and its relationship with the maintenance of bone mass and the changes in mandibular bone in patients with HPTH submitted to parathyroidectomy, as well as the influence of insulin resistance status in HPTP and its effect on bone metabolism [37]. There was a negative correlation between BMD at all sites and bone marrow adiposity during the preoperative period, a fact that was not observed for mandibular cortical thickness. Quantitative evaluation of the mandible revealed a significant difference in extracellular matrix mineralization on the right side between the preoperative and postoperative determinations in the HPTP group (p=0.04). Conclusion: During the cure of HPTP there is an increase in BMD at predominantly, trabecular bone sites, whereas bone gain is impaired in the forearm. Bone marrow adiposity may be one of the causes of impaired bone resistance in HPTP. The behavior of mandibular bone may differ from that to other cortical areas such as the forearm.
A study of panoramic and periapical radiographs of 42 patients on haemodialysis and having renal osteodystrophy, demonstrated a progressive increase in periodontal disease, loss of lamina dura, deviation in the trabecular pattern, brown tumor “pseudocyst” formation and pulp calcifications [38].
Bandeira et al. [39] tells the Brazilian experience of the severe and soft primary hiperparatireoidismo in Pernanbuco-Brazil. The authors had cited that in severe disease pathological fractures are frequently seen, especially in long bones of the lower extremities, and also loss of lamina dura of the teeth and salt-and-pepper appearance of the skull. At authors institution, including outpatients and inpatients, the prevalence in postmenopausal women is 1.3%.
The jawbones are bones that require great attention of the dentist, since in these areas, the teeth often inserted need to receive dental
restorations. Currently these rehabilitations are made with the help of dental implants, and the panoramic radiograph becomes the preferred method for analyzing the structural condition of these bones and their relationship with important surrounding structures. It should be emphasized that the phase in which this type of rehabilitation treatment becomes necessary, in general, coincides with the decline phase of bone mass, having as main target women in post - menopausal.
For many years, the relationship of the jawbone with PHPT was restricted to manifestation of the disease at this site, the brown tumor [40,41]. So, other aspects that could be present on radiographs ended up being less valued and not interpreted as early signs of the disease. With the advancement in knowledge of bone metabolic changes during the evolution of primary hyperparathyroidism, the radiographic examination of the facial bones became a tool with great potential to evaluate the association of these changes and their impact on the bones of the face.
Several studies initiated the evaluation of mandibular bone and jaw in patients with PHPT by periodontal changes that these individuals began to develop, generating an impairment of the stomatognathic system and the evolution of the disease [42]. The authors was not meant to evaluate the periodontal status of patients with PHPT, however we found that during the six months while repeating the panoramic radiograph, some patients had tooth loss. A recent study evaluated the thickness of the mandibular cortical bone, the presence of the hard layer, the occurrence of brown tumor and the presence of the mandibular torus in patients with HPTP. These authors found that the cortical levels were decreased in patients with PHPT compared to the control group [43]. Similar to the study RAI, the data from this study show that patients with HPTP present in cortical thickness values mental foramen region; and the angle region gonial smaller than a reference population that corresponds to 3 mm and 1 mm, respectively. However, there was no significant difference between PHPT and control groups in this study. The authors also draw attention to the evaluation of this cortical bone site that has not shown significant gain after parathyroidectomy. Thus, this result may be more of a foothold in the confirmation that the cortical impairment in PHPT does not present the same pattern of recovery after curing the trabecular bone.
In addition to the mandibular cortical thickness, assessed in panoramic radiographs the morphology of the mandibular cortex according to the classification proposed by Klemetti (1994). It was possible to verify that individuals with PHPT showed no index Klemetti C-1, that is none showed normal Klemetti index. Meanwhile, 60% of patients have had index Klemetti 2 and 40% were compatible with standard 3, resulting in greater loss of bone quality. To compare, in 12% of the control group subjects had Klemetti index 1 and none had standard 3 Klemetti. Surgical cure of primary hyperparathyroidism had a positive impact among patients with lower Klemetti index (Figure 10). Thus, the authors were able to conclude that the quantitative and qualitative study of mandibular bone in PHPT provided data that encourage the use of panoramic radiography face as an examination aid in the diagnosis of bone metabolic diseases, since the mandibular cortical thickness showed behavior similar to region of 1/3 of the forearm, except ECMMd. Even with Klemetti technique it was observed that morphological changes of
Figure 10: Panoramic radiograph showing the inferior mandibular cortical, male patient, Klemetti Class III.

Citation: Watanabe PCA, Faria V, Camargo AJ. Multiple Radiographic Analysis (Systemic Disease): Dental Panoramic Radiography. J Oral Health Dent Care 2017; 1:007.
J Oral Health Dent Care 2017; 1:007Volume 1, Issue 1Watanabe et al.
the mandibular cortical can be found in patients with HPTP even for a six-month follow-up. Thus, these tools ensure that dental professionals have knowledge to recognize changes in the bones of the face to suggest osteometabolic changes as in PHPT.
OsteoporosisOsteoporosis is defined by the World Health Organization (WHO),
a disease characterized by low bone mass and microarchitectural deterioration of bone tissue leading to bone fragility and a consequent increase in the risk of fracture [44] is currently considered as a serious global public health problem, with high levels of morbidity and mortality and high prevalence in developed and developing countries. This is a systemic metabolic disorder characterized by slowly progressive decrease in bone mass, by compromising the integrity of the bone structure, reduction of its strength and the involvement of bone fractures, even in minimal efforts. The person has no signs and symptoms in the early stages of the disease; it is also known as a “silent disease.” The signs and symptoms appear later, when bone density decreases to cause bone fracture or collapse, which can lead to pain and bone deformity [45].
Recent research devoted primarily to investigate and detect diseases within a shorter period of time, aimed at early diagnosis and prevention of diseases. With the increasing life expectancy of the population and the importance in the quest for healthy aging, it becomes extremely important the clinical and social knowledge of chronic diseases that interfere significantly in one’s quality of life such as osteoporosis (Figure 11).
In Brazil, the prevalence of osteoporosis is little known, but by Kowalski [46] that measured the use of resources and annual cost for patients with osteoporosis, pos-menopausal in the clinic of osteoporosis of the UNIFESP, the annual average cost for patient was approximately $ 442,00/patient. However, Araujo et al. [47] has assessed the direct cost during hospitalization for an osteoporotic hip fracture in Brazilian private health care system, by health plan companies’ perspective, so the authors concluded that this cost had assess in approximately $ 6.900. The study “Osteoporosis - Brazil Year 2000”, developed by 300 medical specialists, estimated that less than a third of Brazilians with osteoporosis are diagnosed, and that only 20 % of those known to be affected are treated [47,48].
Triage better, and earlier, patients to perform DXA whole body, is a key strategy in the fight against this disease. The panoramic radiograph has been used in routine dental care worldwide, thanks mainly to the great technological development in recent decades, and as a clinical protocol has the backing of the International Guide Radiographic Prescription.
Panoramic radiography covers important anatomical structures and has a low cost can be of great value to dentistry providing the dentist the diagnosis of bone quality of the jaws. For these reasons and because of the panoramic radiograph can continue to be used for diagnosis of low bone mineral density in the cortex of the mandible [49-52]. Evaluation the characterization of the cortical walls of the mandibular canal in patients with osteopenia/ osteoporosis, hoping to indicate whether there is the correlation between mandibular bone quality and systemic bone quality or not it’s an important question [53].
Panoramic radiography has been used to screen patients with low bone mineral density (BMD) evaluating the thickness and shape of the mandibular cortical [49,5054,55].
For these reasons and because panoramic radiograph is already used for diagnosis of low bone mineral density in the mandibular cortex [49-52] Camargo 2013 has evaluated the characterization of the mandibular canal walls (Figure 12) to evaluate changes caused
by osteopenia/ osteoporosis, checking for correlation between the mandibular bone quality and systemic bone quality.
Camargo (2013) divided the sample into three groups according to DXA exam: Group N (n = 26) normal in three sites (forearm, hip and spine), Group E (n = 18) with osteopenia at the three sites and Group O (n = 8) with osteoporosis in the three sites. The DXA and panoramic radiography were performed in the same period. All panoramic radiographs had been done using a Veraviewepocs Digital unit (J. Morita Mfg. Corp., Kyoto, Japan) and DXA performed by HOLOGIC® (Waltham, MA, USA). To study the pattern of the cortical bone of the mandibular canal, we use an adaptation of morphological analysis methodology proposed by White and Rudolph [56].
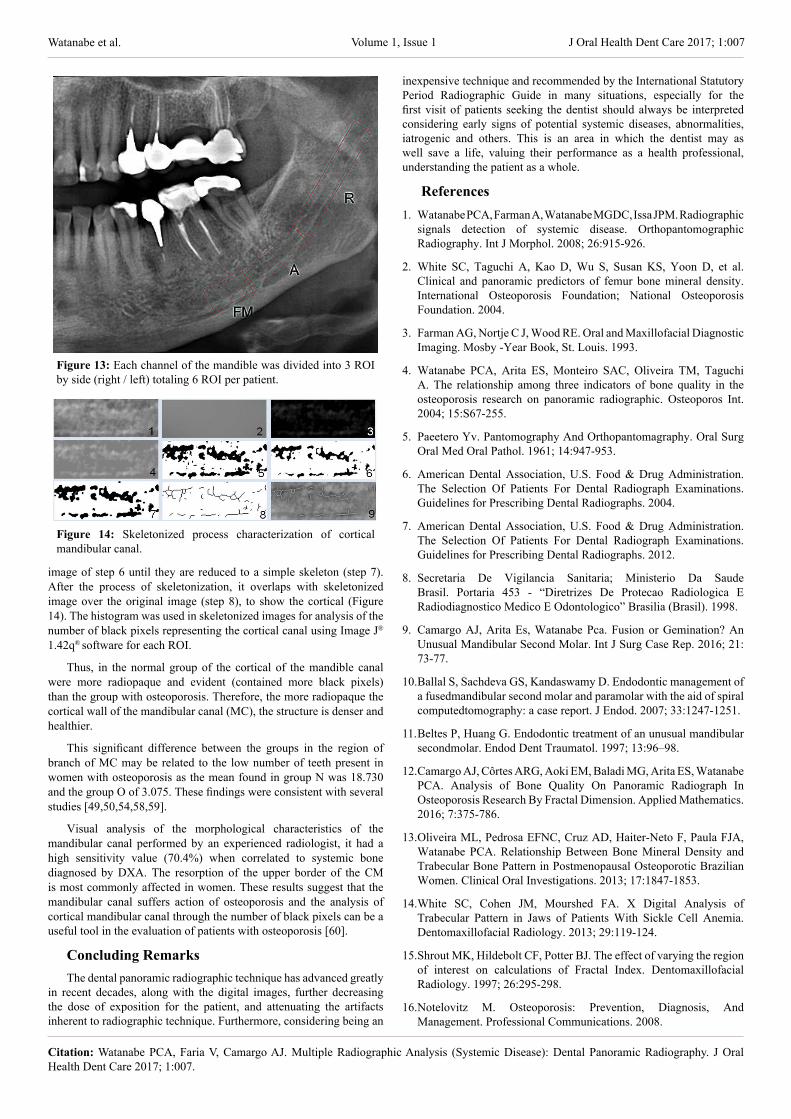
After selection of radiography was performed trimming of hemi-arches on both sides (left / right) focusing on the region of the mandibular canal using a computer software ADOBE ® PHOTOSHOP ® CS3 v.10.0 (Adobe Systems Incorporated, San Jose, California, USA). From this stage, it was performed a cutting of the regions of mandibular canal: after the mental foramen (MF) angle region (A) and branch region(R) selecting the canal, bilaterally, along its entire length (Figure 13).
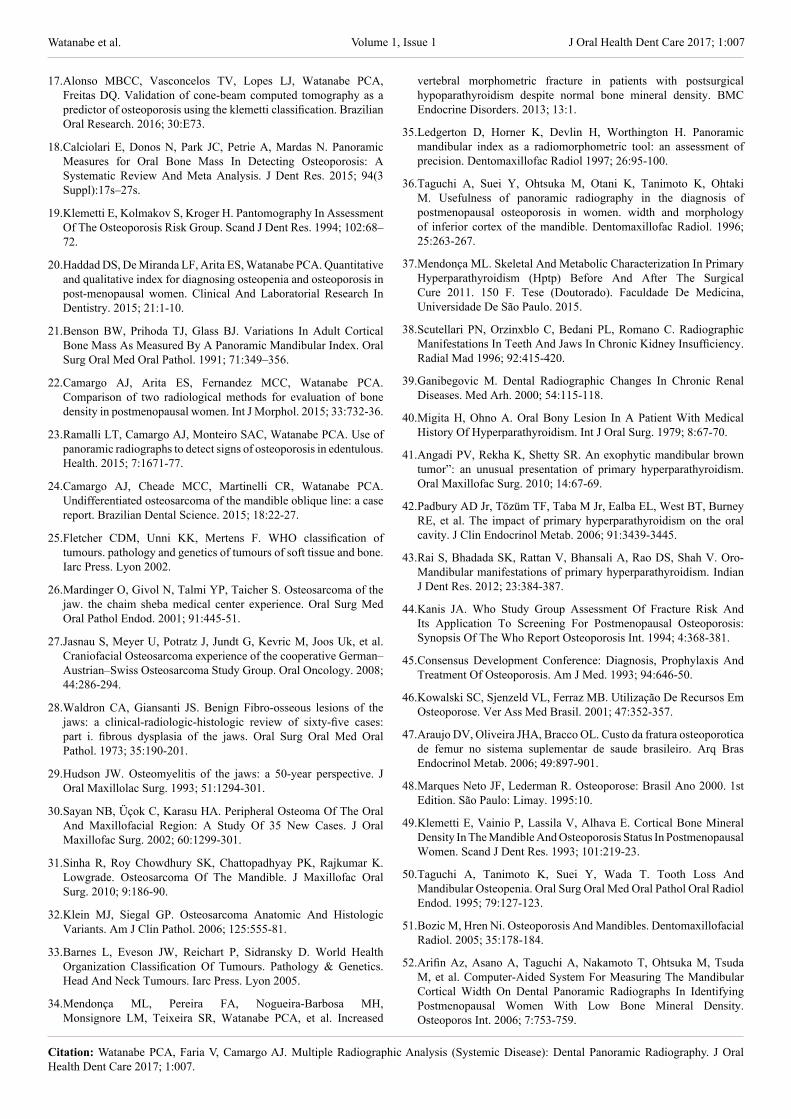
This division of the canal was necessary because of its slightly curved anatomy, thereby was limited to the clipping only in mandibular canal. Regions of interest (ROI) were defined from the anatomy of each patient. In each clipping of the mandibular canal was performed duplicating the original image (step 1) before performing the blurring of image using Gaussian filter (sigma = 35 pixels) (step 2) in Image J® 1.42q® (National Institutes of Health, USA) software. The resulting image is subtracted from the original image (step 1-step 2), and added 128 (half value of the grayscale contrast scale 256) (step 3). The image binarization is performed on a threshold value of brightness of 128 (step 4), transforming the image into black and white. The image taken is eroded (step 5) and dilated (step 6) for noise reduction. Lastly it is performed to characterize the cortical on the canal with “skeletonization”
Figure 11: Brazil life expectancy in relation to The USA and Mexico.
Figure 12: Panoramic radiography shows the characteristics of the mandibular canal, both sides and superior and inferior walls.
Citation: Watanabe PCA, Faria V, Camargo AJ. Multiple Radiographic Analysis (Systemic Disease): Dental Panoramic Radiography. J Oral Health Dent Care 2017; 1:007.
J Oral Health Dent Care 2017; 1:007Volume 1, Issue 1Watanabe et al.
image of step 6 until they are reduced to a simple skeleton (step 7). After the process of skeletonization, it overlaps with skeletonized image over the original image (step 8), to show the cortical (Figure 14). The histogram was used in skeletonized images for analysis of the number of black pixels representing the cortical canal using Image J® 1.42q® software for each ROI.
Thus, in the normal group of the cortical of the mandible canal were more radiopaque and evident (contained more black pixels) than the group with osteoporosis. Therefore, the more radiopaque the cortical wall of the mandibular canal (MC), the structure is denser and healthier.
This significant difference between the groups in the region of branch of MC may be related to the low number of teeth present in women with osteoporosis as the mean found in group N was 18.730 and the group O of 3.075. These findings were consistent with several studies [49,50,54,58,59].
Visual analysis of the morphological characteristics of the mandibular canal performed by an experienced radiologist, it had a high sensitivity value (70.4%) when correlated to systemic bone diagnosed by DXA. The resorption of the upper border of the CM is most commonly affected in women. These results suggest that the mandibular canal suffers action of osteoporosis and the analysis of cortical mandibular canal through the number of black pixels can be a useful tool in the evaluation of patients with osteoporosis [60].
Concluding RemarksThe dental panoramic radiographic technique has advanced greatly
in recent decades, along with the digital images, further decreasing the dose of exposition for the patient, and attenuating the artifacts inherent to radiographic technique. Furthermore, considering being an
inexpensive technique and recommended by the International Statutory Period Radiographic Guide in many situations, especially for the first visit of patients seeking the dentist should always be interpreted considering early signs of potential systemic diseases, abnormalities, iatrogenic and others. This is an area in which the dentist may as well save a life, valuing their performance as a health professional, understanding the patient as a whole.
References1. Watanabe PCA, Farman A, Watanabe MGDC, Issa JPM. Radiographic
signals detection of systemic disease. Orthopantomographic Radiography. Int J Morphol. 2008; 26:915-926.
2. White SC, Taguchi A, Kao D, Wu S, Susan KS, Yoon D, et al. Clinical and panoramic predictors of femur bone mineral density. International Osteoporosis Foundation; National Osteoporosis Foundation. 2004.
3. Farman AG, Nortje C J, Wood RE. Oral and Maxillofacial Diagnostic Imaging. Mosby -Year Book, St. Louis. 1993.
4. Watanabe PCA, Arita ES, Monteiro SAC, Oliveira TM, Taguchi A. The relationship among three indicators of bone quality in the osteoporosis research on panoramic radiographic. Osteoporos Int. 2004; 15:S67-255.
5. Paeetero Yv. Pantomography And Orthopantomagraphy. Oral Surg Oral Med Oral Pathol. 1961; 14:947-953.
6. American Dental Association, U.S. Food & Drug Administration. The Selection Of Patients For Dental Radiograph Examinations. Guidelines for Prescribing Dental Radiographs. 2004.
7. American Dental Association, U.S. Food & Drug Administration. The Selection Of Patients For Dental Radiograph Examinations. Guidelines for Prescribing Dental Radiographs. 2012.
8. Secretaria De Vigilancia Sanitaria; Ministerio Da Saude Brasil. Portaria 453 - “Diretrizes De Protecao Radiologica E Radiodiagnostico Medico E Odontologico” Brasilia (Brasil). 1998.
9. Camargo AJ, Arita Es, Watanabe Pca. Fusion or Gemination? An Unusual Mandibular Second Molar. Int J Surg Case Rep. 2016; 21: 73-77.
10. Ballal S, Sachdeva GS, Kandaswamy D. Endodontic management of a fusedmandibular second molar and paramolar with the aid of spiral computedtomography: a case report. J Endod. 2007; 33:1247-1251.
11. Beltes P, Huang G. Endodontic treatment of an unusual mandibular secondmolar. Endod Dent Traumatol. 1997; 13:96–98.
12. Camargo AJ, Côrtes ARG, Aoki EM, Baladi MG, Arita ES, Watanabe PCA. Analysis of Bone Quality On Panoramic Radiograph In Osteoporosis Research By Fractal Dimension. Applied Mathematics. 2016; 7:375-786.
13. Oliveira ML, Pedrosa EFNC, Cruz AD, Haiter-Neto F, Paula FJA, Watanabe PCA. Relationship Between Bone Mineral Density and Trabecular Bone Pattern in Postmenopausal Osteoporotic Brazilian Women. Clinical Oral Investigations. 2013; 17:1847-1853.
14. White SC, Cohen JM, Mourshed FA. X Digital Analysis of Trabecular Pattern in Jaws of Patients With Sickle Cell Anemia. Dentomaxillofacial Radiology. 2013; 29:119-124.
15. Shrout MK, Hildebolt CF, Potter BJ. The effect of varying the region of interest on calculations of Fractal Index. Dentomaxillofacial Radiology. 1997; 26:295-298.
16. Notelovitz M. Osteoporosis: Prevention, Diagnosis, And Management. Professional Communications. 2008.
Figure 13: Each channel of the mandible was divided into 3 ROI by side (right / left) totaling 6 ROI per patient.
Figure 14: Skeletonized process characterization of cortical mandibular canal.
Citation: Watanabe PCA, Faria V, Camargo AJ. Multiple Radiographic Analysis (Systemic Disease): Dental Panoramic Radiography. J Oral Health Dent Care 2017; 1:007.
J Oral Health Dent Care 2017; 1:007Volume 1, Issue 1Watanabe et al.
17. Alonso MBCC, Vasconcelos TV, Lopes LJ, Watanabe PCA, Freitas DQ. Validation of cone-beam computed tomography as a predictor of osteoporosis using the klemetti classification. Brazilian Oral Research. 2016; 30:E73.
18. Calciolari E, Donos N, Park JC, Petrie A, Mardas N. Panoramic Measures for Oral Bone Mass In Detecting Osteoporosis: A Systematic Review And Meta Analysis. J Dent Res. 2015; 94(3 Suppl):17s–27s.
19. Klemetti E, Kolmakov S, Kroger H. Pantomography In Assessment Of The Osteoporosis Risk Group. Scand J Dent Res. 1994; 102:68–72.
20. Haddad DS, De Miranda LF, Arita ES, Watanabe PCA. Quantitative and qualitative index for diagnosing osteopenia and osteoporosis in post-menopausal women. Clinical And Laboratorial Research In Dentistry. 2015; 21:1-10.
21. Benson BW, Prihoda TJ, Glass BJ. Variations In Adult Cortical Bone Mass As Measured By A Panoramic Mandibular Index. Oral Surg Oral Med Oral Pathol. 1991; 71:349–356.
22. Camargo AJ, Arita ES, Fernandez MCC, Watanabe PCA. Comparison of two radiological methods for evaluation of bone density in postmenopausal women. Int J Morphol. 2015; 33:732-36.
23. Ramalli LT, Camargo AJ, Monteiro SAC, Watanabe PCA. Use of panoramic radiographs to detect signs of osteoporosis in edentulous. Health. 2015; 7:1671-77.
24. Camargo AJ, Cheade MCC, Martinelli CR, Watanabe PCA. Undifferentiated osteosarcoma of the mandible oblique line: a case report. Brazilian Dental Science. 2015; 18:22-27.
25. Fletcher CDM, Unni KK, Mertens F. WHO classification of tumours. pathology and genetics of tumours of soft tissue and bone. Iarc Press. Lyon 2002.
26. Mardinger O, Givol N, Talmi YP, Taicher S. Osteosarcoma of the jaw. the chaim sheba medical center experience. Oral Surg Med Oral Pathol Endod. 2001; 91:445-51.
27. Jasnau S, Meyer U, Potratz J, Jundt G, Kevric M, Joos Uk, et al. Craniofacial Osteosarcoma experience of the cooperative German–Austrian–Swiss Osteosarcoma Study Group. Oral Oncology. 2008; 44:286-294.
28. Waldron CA, Giansanti JS. Benign Fibro-osseous lesions of the jaws: a clinical-radiologic-histologic review of sixty-five cases: part i. fibrous dysplasia of the jaws. Oral Surg Oral Med Oral Pathol. 1973; 35:190-201.
29. Hudson JW. Osteomyelitis of the jaws: a 50-year perspective. J Oral Maxillolac Surg. 1993; 51:1294-301.
30. Sayan NB, Üçok C, Karasu HA. Peripheral Osteoma Of The Oral And Maxillofacial Region: A Study Of 35 New Cases. J Oral Maxillofac Surg. 2002; 60:1299-301.
31. Sinha R, Roy Chowdhury SK, Chattopadhyay PK, Rajkumar K. Lowgrade. Osteosarcoma Of The Mandible. J Maxillofac Oral Surg. 2010; 9:186-90.
32. Klein MJ, Siegal GP. Osteosarcoma Anatomic And Histologic Variants. Am J Clin Pathol. 2006; 125:555-81.
33. Barnes L, Eveson JW, Reichart P, Sidransky D. World Health Organization Classification Of Tumours. Pathology & Genetics. Head And Neck Tumours. Iarc Press. Lyon 2005.
34. Mendonça ML, Pereira FA, Nogueira-Barbosa MH, Monsignore LM, Teixeira SR, Watanabe PCA, et al. Increased
vertebral morphometric fracture in patients with postsurgical hypoparathyroidism despite normal bone mineral density. BMC Endocrine Disorders. 2013; 13:1.
35. Ledgerton D, Horner K, Devlin H, Worthington H. Panoramic mandibular index as a radiomorphometric tool: an assessment of precision. Dentomaxillofac Radiol 1997; 26:95-100.
36. Taguchi A, Suei Y, Ohtsuka M, Otani K, Tanimoto K, Ohtaki M. Usefulness of panoramic radiography in the diagnosis of postmenopausal osteoporosis in women. width and morphology of inferior cortex of the mandible. Dentomaxillofac Radiol. 1996; 25:263-267.
37. Mendonça ML. Skeletal And Metabolic Characterization In Primary Hyperparathyroidism (Hptp) Before And After The Surgical Cure 2011. 150 F. Tese (Doutorado). Faculdade De Medicina, Universidade De São Paulo. 2015.
38. Scutellari PN, Orzinxblo C, Bedani PL, Romano C. Radiographic Manifestations In Teeth And Jaws In Chronic Kidney Insufficiency. Radial Mad 1996; 92:415-420.
39. Ganibegovic M. Dental Radiographic Changes In Chronic Renal Diseases. Med Arh. 2000; 54:115-118.
40. Migita H, Ohno A. Oral Bony Lesion In A Patient With Medical History Of Hyperparathyroidism. Int J Oral Surg. 1979; 8:67-70.
41. Angadi PV, Rekha K, Shetty SR. An exophytic mandibular brown tumor”: an unusual presentation of primary hyperparathyroidism. Oral Maxillofac Surg. 2010; 14:67-69.
42. Padbury AD Jr, Tözüm TF, Taba M Jr, Ealba EL, West BT, Burney RE, et al. The impact of primary hyperparathyroidism on the oral cavity. J Clin Endocrinol Metab. 2006; 91:3439-3445.
43. Rai S, Bhadada SK, Rattan V, Bhansali A, Rao DS, Shah V. Oro-Mandibular manifestations of primary hyperparathyroidism. Indian J Dent Res. 2012; 23:384-387.
44. Kanis JA. Who Study Group Assessment Of Fracture Risk And Its Application To Screening For Postmenopausal Osteoporosis: Synopsis Of The Who Report Osteoporosis Int. 1994; 4:368-381.
45. Consensus Development Conference: Diagnosis, Prophylaxis And Treatment Of Osteoporosis. Am J Med. 1993; 94:646-50.
46. Kowalski SC, Sjenzeld VL, Ferraz MB. Utilização De Recursos Em Osteoporose. Ver Ass Med Brasil. 2001; 47:352-357.
47. Araujo DV, Oliveira JHA, Bracco OL. Custo da fratura osteoporotica de femur no sistema suplementar de saude brasileiro. Arq Bras Endocrinol Metab. 2006; 49:897-901.
48. Marques Neto JF, Lederman R. Osteoporose: Brasil Ano 2000. 1st Edition. São Paulo: Limay. 1995:10.
49. Klemetti E, Vainio P, Lassila V, Alhava E. Cortical Bone Mineral Density In The Mandible And Osteoporosis Status In Postmenopausal Women. Scand J Dent Res. 1993; 101:219-23.
50. Taguchi A, Tanimoto K, Suei Y, Wada T. Tooth Loss And Mandibular Osteopenia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 79:127-123.
51. Bozic M, Hren Ni. Osteoporosis And Mandibles. Dentomaxillofacial Radiol. 2005; 35:178-184.
52. Arifin Az, Asano A, Taguchi A, Nakamoto T, Ohtsuka M, Tsuda M, et al. Computer-Aided System For Measuring The Mandibular Cortical Width On Dental Panoramic Radiographs In Identifying Postmenopausal Women With Low Bone Mineral Density. Osteoporos Int. 2006; 7:753-759.

Citation: Watanabe PCA, Faria V, Camargo AJ. Multiple Radiographic Analysis (Systemic Disease): Dental Panoramic Radiography. J Oral Health Dent Care 2017; 1:007.
J Oral Health Dent Care 2017; 1:007Volume 1, Issue 1Watanabe et al.
53. Camargo AJ. Characterization The mandibular canal walls to evaluate possible changes caused by osteoporosis. Thesis. 2013.
54. Taguchi A, Tanimoto K, Suei Y, Otani K, Wada T. Oral Signs As Indicators Of Possible Osteoporosis In Elderly Women. Oral Surg Oral Meo Oral Pathol Oral Radiol Endod. 1995; 80:612-616.
55. Taguchi A, Ohtsuka M, Nakamoto T, Naito K, Tsuda M, Kudo Y, et al. Identification Of Post-Menopausal Women At Risk Of Osteoporosis By Trained General Dental Practitioners Using Panoramic Radiographs. Dentomaxillofac Radiol. 2007; 36:149-154.
56. White Sc, Rudolph Dj. Alterations Of The Trabecular Pattern Of The Jaws In Patients With Osteoporosis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 88:628-635.
57. Taguchi A, Suei Y, Ohtsuka M, Otani K, Tanimoto K, Hollender
Lg. Relationship Between Bone Mineral Density And Tooth Loss In Elderly Japanese Women. Dentomaxillofac Radiol. 1999; 28:219-223.
58. Taguchi A, Ohtsuka M, Tsuda M, Nakamoto T, Kodama I, Inagaki K, et al. Risk Of Vertebral Osteoporosis In Post-Menopausal Women With Alterations Of The Mandible. Dentomaxillofac Radiol. 2007; 36:143-148.
59. Vaishnav K, Shah D, Patel P. A Panoramic Evaluation Of The Mandibular Canal Wall Resorption In Relation To Diabetes, Thyroid And Asthma In Edentulous Patients. J Int Health. 2010; 2:27-32.
60. Alonso Mbcc, Oliveira-Santos C, Monteiro Sac, Watanabe Pca. Morphological Analysis Of The Mandibular Canal In Panoramic Radiographs Of The Jaws As An Indicator Of Bone Mineral Density. Osteoporos Int. 2012; 23:485-486.





























