-
Treatment of Viral Conjunctivitis withAntiviral DrugsChrysanthi
L. Skevaki,1 Ioanna E. Galani,2 Michail V. Pararas,1 Konstantina P.
Giannopoulou3
and Athanassios Tsakris1
1 Department of Microbiology, School of Medicine, University of
Athens, Athens, Greece
2 Center of Immunology & Transplantation, Biomedical
Research Foundation of the Academyof Athens, Athens, Greece
3 First Department of Ophthalmiatrion Athinon, Athens Eye
Hospital, Athens, Greece
Contents
Abstract. . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . 3311. Methods of Literature
Review. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 333
1.1 Literature Search . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . 3331.2 Study Selection and Eligibility Criteria
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . 3331.3 Data Evaluation. . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . 333
2. Results . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . 3332.1 Aciclovir . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3332.2 Cidofovir . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . 3372.3 Famciclovir . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . 3392.4
Idoxuridine . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . 3412.5 Interferons. . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . 3412.6 RNA Interference. .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3422.7
Trifluridine . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . 3422.8 Valaciclovir . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . 3422.9 Other Compounds
Tested in Humans . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . 3432.10 Other
Compounds Tested in Animal or In Vitro Studies . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . 343
3. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . 344
Abstract Viral conjunctivitis is one of the most common
disorders observed inophthalmic emergency departments, yet no
established treatment exists. Lately,antiviral medications have
been introduced into clinical practice; however,a systematic review
focusing on their use and effectiveness in the treatmentof viral
conjunctivitis has not been previously reported. We systemically
re-viewed the literature to identify studies where antiviral drugs
were used totreat viral conjunctivitis. Currently, aciclovir,
trifluridine and valaciclovir arecommonly used as antiviral agents
to treat herpesvirus infections. Cidofovirhas been used
successfully to treat some cases of adenoviral
conjunctivitis,although toxicity has also been reported. The use of
other medications,such as idoxuridine, has been minimized in
clinical practice due to theirhigh toxicity. Interestingly, most of
the antiviral drugs developed are usedto treat herpesvirus
infections, while less progress has been made in the field
REVIEWARTICLE Drugs 2011; 71 (3):
331-3470012-6667/11/0003-0331/$55.55/0 2011 Adis Data Information
BV. All rights reserved.
-
of adenoviral infections. For other viral causes of
conjunctivitis, no effec-tive remedy is currently available, and
treatment focuses on the relief ofsymptoms. Caution should be
exercised when coadministering other phar-macological agents, such
as corticosteroids, because of emerging adverseeffects.
Conjunctivitis, commonly known as red eye,is one of the most
frequent ocular disorders ob-served in ophthalmic emergency
departments.[1,2]
Possible causes include an allergic reaction oran infection of
viral or bacterial origin. Acuteviral conjunctivitis is commonly
caused by var-ious serotypes of adenoviruses, but herpesvirusesand
varicella-zoster virus, which are DNA viruses,and the RNA viruses
picornaviruses, such asenterovirus serotype 70 (EV70) and
coxsackie-virus A24 variant (Cox A24), are also causes.[3]
Other less frequent causes of viral conjunctivitisusually occur
in association with a systemic ill-ness and include infections
caused by the DNAvirus Epstein-Barr virus, and the RNA
virusesinfluenza virus, paramyxovirus (e.g. Newcastledisease
virus), rubella virus and HIV.
Viral conjunctivitis is usually a benign andself-limiting
condition that may heal within a fewweeks, and can affect all ages.
Nevertheless, it canbe highly infectious and has been the cause
ofepidemic outbreaks worldwide,[4-8] thus constitut-ing a major
public health problem. Inflammationof the conjunctiva can also
occur in combinationwith corneal inflammation and subepithelial
in-filtrates, most commonly caused by adenovirusserotypes 8, 19 and
37, causing severe adenoviralkeratoconjunctivitis and epidemics.[9]
Epidemicconjunctivitis due to viruses is also a commonnosocomial
infection.[10-12] Local care and inter-ventions to minimize
transmission are thus the cor-nerstones for management for viral
conjunctivitis.
Among infectious causes of conjunctivitis,viral conjunctivitis
is the most common and, insome cases, coincides with a viral upper
respira-tory tract infection, with or without the presenceof
purulent discharges. Allergic conjunctivitis maybe seasonal or
perennial, and is mostly character-ized by itching and watery
discharges. The patientshistory, the presence of signs, such as
vesicles,ulcerations, crusting, discharge and chemosis,
during physical examination, as well as labora-tory tests,
assist in the definitive diagnosis of thecausative agent.[1]
Currently, there is no specific treatment forviral
conjunctivitis. Symptomatic relief may beachieved with cool
compresses and artificial tears.For severe cases of conjunctivitis
and keratitis,topical corticosteroid drops are prescribed for
therelief of symptoms caused by inflammation. How-ever, prolonged
use of corticosteroids increasesthe risk of adverse effects.
Recent advances in the field of infectious con-junctivitis have
introduced new diagnostic meth-ods and novel therapeutic agents.
Serological tests,ELISA, electron microscopy and polymerasechain
reaction techniques have been used for thelaboratory identification
of specific viral strainsthrough direct inspection or detection of
theirantigens and antibodies. Such methodologies, incombination
with the use of antiviral medica-tions, offer an alternative
therapeutic approachthat directly targets viral replication.
Viral replication takes place inside the infectedhost cells. DNA
viruses, in general, replicate in-side the cell nucleus and, in
many cases, dependon the host cell cycle, while RNA viruses
replicateprimarily in the cytoplasm, and their replicationis not so
strictly dependent on the host cell cycle.Viruses may rely on the
host polymerases fortheir replication, or they can encode their
ownpolymerases, such as adenoviruses, herpesvirusesand most RNA
viruses. Most antiviral drugs arenucleoside or nucleotide analogues
that inhibitviral replication by acting as chain terminatorsduring
DNA or RNA synthesis. Analoguescompete with the natural substrates,
and whenadded in the newly synthesized DNA or RNAchain, they do not
offer a binding position for aphosphodiester bond with the next
nucleotide.[13]
The rapidly increasing number of antiviral agentsis quite
promising; however, the efficacy of many
332 Skevaki et al.
2011 Adis Data Information BV. All rights reserved. Drugs 2011;
71 (3)
-
of these drugs in treating viral conjunctivitis isstill elusive.
Furthermore, some of these medica-tions have adverse effects.
The goal of this review is to evaluate ther-apeutic regimens for
viral conjunctivitis that arecurrently used in clinical practice or
are underdevelopment. We have thus summarized in-formation on
antiviral drugs that have been usedto treat viral conjunctivitis or
have been tested inexperimental systems, and which may prove
use-ful for the physician.
1. Methods of Literature Review
1.1 Literature Search
We systematically searched the MEDLINEdatabase using PubMed up
to December 2010.The keywords used were MESH terms:
viralconjunctivitis and antiviral drugs. Referencesof relevant
articles were also hand-searched.
1.2 Study Selection and Eligibility Criteria
Studies were selected if they included clinicaldata or
experimental animal data on the effect ofantiviral drugs for the
treatment of viral con-junctivitis. In addition, in vitro
experimental dataon the effect of antiviral drugs on the
replicationof clinically relevant viruses were included.
Reviewarticles were excluded, but were manually screenedfor
additional references. Finally, studies wereonly included if
written in English, German,French or Italian.
1.3 Data Evaluation
Studies including clinical or animal experi-mental data were
evaluated according to thestudy population, the type of infection,
the anti-viral agent used, the dosage regimen administeredand the
outcome of the disease. The in vitroexperimental data were analysed
based on theantiviral agent in use, the method by which
theeffectiveness of the antiviral agent was determined,and the
outcome of the experiment. The datawere evaluated and are presented
herewith basedon the PRISMA statement for reporting system-atic
reviews and meta-analyses.[14]
2. Results
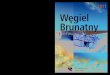
The process of study selection is depicted as aflow diagram,
according to PRISMA, in figure 1.Initially, 110 articles were
identified. In addition,17 articles were also included via a
hand-search ofreferences. A total of 56 studies, published be-tween
August 1969 and August 2010, were finallyincluded in this review.
Among the studies fur-ther analysed in the present review, 27 were
clin-ical studies, 17 were animal studies and 12 werein vitro
studies. We present the results of our re-view based on the
antiviral agent used in alpha-betical order. In addition, tables I,
II and IIIsummarize the clinical data, the animal and thein vitro
experimental studies, respectively.
2.1 Aciclovir
Aciclovir is a guanosine analogue with anti-viral properties. It
is inactive until it becomesphosphorylated by viral thymidine
kinase, thus itdoes not affect uninfected cells. After
phosphor-ylation, aciclovir is incorporated into viral DNAand
blocks its replication. It is an establishedtreatment for herpes
simplex virus (HSV) infec-tions, which is administered topically,
orally orintravenously. Six studies were identified in
theliterature as using aciclovir in the treatment
ofconjunctivitis.[15-20] Three were clinical trials[15-17]
and three were case reports.[18-20]
In one clinical trial, 71 non-immunocompro-mised patients with
herpes zoster ophthalmicuswere treated with a 10-day course of oral
aciclovir(600mg five times daily). Aciclovir was well tol-erated
and significantly reduced the incidenceand severity of
complications of the infection.[15]
In addition, the long-term oral aciclovir admin-istration (12
months) for the treatment of ocularHSV infection was effective in
decreasing virusrecurrence.[16] Another clinical trial
comparedtopical versus oral aciclovir treatment for earlyherpes
zoster ophthalmicus. Fifty-seven patientsreceived either topical
aciclovir ointment or oralaciclovir 800mg, both five times daily
for 7 days,and were followed up for 12 months. The studyconcluded
that patients receiving topical aciclovirexhibited more ocular
complications than the
Antiviral Treatment for Viral Conjunctivitis 333
2011 Adis Data Information BV. All rights reserved. Drugs 2011;
71 (3)
-
orally treated group.[17] In a case report study, a95-year-old
woman diagnosed with ophthalmiczoster sine herpete was effectively
treated withintravenous aciclovir given at 10mg/kg threetimes daily
for 3 days, followed by oral aciclovirat 800mg five times daily for
14 days.[18] A14-year-old girl who presented with
Parinaudsoculoglandular syndrome, an uncommon mani-festation of
primary HSV type 1 (HSV-1) infec-tion, was treated with oral and
local aciclovir thatallowed improvement of her symptoms.[19]
Fi-nally, a 17-year-old man was treated with acic-lovir ointment 3%
w/w four times daily, togetherwith antibacterials and
corticosteroids, in orderto treat a suspected herpesvirus
infection; treat-ment with aciclovir was interrupted after 2
days,when it was determined that keratoconjunctivitis
was due to the coexistence of adenoviral andAcanthamoeba
infection.[20]
A study involving rabbits showed that a 3%aciclovir ointment
applied topically one to fivetimes daily during an acute ocular HSV
infectionwas beneficial in reducing conjunctivitis occur-rence
among other ophthalmic complications,but was not effective in
preventing conjunctivitiswhen applied 24 hours after viral
inoculation. Inaddition, aciclovir was not effective in
eradicatingestablished latent HSV infection.[42]
Despite its inability to eradicate latent infec-tion,[71]
therapeutic and/or prophylactic admin-istration of aciclovir is
considered a standardantiviral therapy for several manifestations
ofHSV infection. In addition to aciclovir, twosecond-generation
antiviral agents, famciclovir
Iden
tifica
tion
Scre
enin
gEl
igib
ility
Incl
uded
110 articles identified throughPubMed search
17 additional articles identifiedthrough hand-search
100 articles screened
56 full-text articlesassessed for eligibility
56 articles included inqualitative synthesis
44 full-text articles excludedbecause of no relevancy
toantiviral treatment or viral conjunctivitis Focus on other
disease (n = 19) No treatment mentioned (n = 19) Non-antiviral
therapy used (n = 3) Reviews (n = 3)
27 articles excluded No abstract available (n = 12) Articles
written in non-eligible
languages (n = 15)
127 total articles
Fig. 1. Flow diagram of the selection process of articles
eligible for inclusion in this review.
334 Skevaki et al.
2011 Adis Data Information BV. All rights reserved. Drugs 2011;
71 (3)
-
Table I. Summary of clinical data on therapeutic regimens used
to treat viral conjunctivitis
Study (year) Infectious agent Drug Treatment Study groups
Efficacya
Cobo et al.[15]
(1986)
HZO Aciclovir Oral 600mg, five times daily
for 10 d
Aciclovir vs placebo (n =71) Well tolerated, reduced
incidenceand severity
Uchoa et al.[16]
(2003)
HSV Aciclovir Oral 400mg, twice daily for
12 or 18mo
Aciclovir 12mo (n= 18) vs 18mo(n =22)
Decrease in virus recurrence after
long-term treatment
Neoh et al.[17]
(1994)
HZO Aciclovir Topical ointment or oral
800mg, both five times
daily for 7 d
Topical vs oral (n =57) More ocular complications inthe
topically treated group
Goon et al.[18]
(2000)
HZO Aciclovir IV 10mg/kg, three times dailyfor 3 d, then oral
800mg,
five times daily for 14 d
n =1 Efficient treatment
Parentin
et al.[19] (2007)
HSV-1 Aciclovir Oral and local n =1 Improvement of symptoms
Gajdatsy
et al.[20] (2000)
Adenovirus and
Acanthamoeba
Aciclovir, antibacterials
and corticosteroids
Topical ointment 3% w/w,four times daily for 2 d
n =1 Aciclovir treatment wasinterrupted when infectious
agent was determined
Gordon et al.[21]
(1996)
Adenovirus Cidofovir Topical eye drops 0.2%,four times daily for
8 d
n =1 Resolution of clinical sings in theinfected eye,
prophylaxis from
infection in the noninfected eye
Castleton and
Kottaridis[22]
(2007)
Adenovirus
subgroup D
Cidofovir IV 1mg/kg, three times weeklyfor 4wk
n =1 Successful treatment
Hillenkamp
et al.[23] (2001)
Adenovirus Cidofovir, ciclosporin or
cidofovir + ciclosporinTopical eyedrops 0.2% (1%ciclosporin eye
drops), four
times daily for 21 d
Cidofovir vs ciclosporin vs
cidofovir + ciclosporin vs sodiumchloride (control) [n =39]
No acceleration of resolution vs
natural course in any of the
therapeutic regimens
Hillenkamp
et al.[24] (2002)
Adenovirus Cidofovir, ciclosporin or
cidofovir + ciclosporinTopical eyedrops 1%, fouror ten times
daily (1%ciclosporin 1% eyedropsfour times daily) for 21 d
Cidofovir four times daily (n= 9) vs cidofovirten times daily
(n= 5) vs cidofovir andciclosporin four times daily (n= 10)
vssodium chloride four times daily (control)
[n = 10]
Cidofocir treatment led to
reduction in the frequency of
corneal opacities, but was
accompanied by adverse effects
Tyring et al.[25]
(2001)
HZO Famciclovir or aciclovir Oral 500mg, three times daily
for 7 d (famciclovir); oral
800mg, five times daily for 7 d
(aciclovir)
Famciclovir (n = 251) vs aciclovir(n =203)
The two drugs had equal
efficiency, but famciclovir provided
a better dosing regimen
Dudgeon
et al.[26] (1969)
Adenovirus Idoxuridine Topical ointment 0.5%, every3 h during
the day and every
6 h during the night for 7 d
Idoxuridine (n= 35) vs placebo (n =35) No beneficial effect of
idoxuridineover placebo
Continued next page
Antiv
iralTreatm
entforViral
Conjunctiv
itis335
2011AdisData
Inform
atio
nBV.Allrig
htsreserved.
Drugs2011;71(3)
-
Table I. Contd
Study (year) Infectious agent Drug Treatment Study groups
Efficacya
Adams et al.[27]
(1984)
Adenovirus Plasmid-derived
IFNa-2ND IFNa-2 vs placebo (n = 14) No effect on disease
duration
or virus shedding
Romano
et al.[28] (1980)
Adenovirus HuIFNb orcorticosteroids
Topical 12 105 referenceunits daily divided into 810
drops
HuIFNb vs corticosteroids vs placebo Reduction in length of
disease inHuIFNb-treated groups
Wilhelmus
et al.[29] (1987)
Adenovirus HuIFNb Topical 7.5 105 IU/mL,five times daily for
1wk
HuIFNb vs placebo (n =37) Improvement only when left eyeswere
infected
Hutter[30] (1990) Ad8 IFNa or trifluridine orpovidine-iodine
or
combinations
ND n =150 Best results observed withpovidone-iodine
Rossa and
Sundmacher[31]
(1991)
ND IFN Topical eye drops, once daily
for 12 d
n =130 Prevention of highly contagiousviral
keratoconjunctivitis
Romano and
Sadan[32]
(1988)
Adenovirus, HZO or
HSV-1
HuIFNb Topical cream 20000 IU/g(for HSV-1 and HZO);
topical eye drops
500 0001000 000U
(for Ad and HSV-1)
ND Efficient in prophylaxis and
duration of disease when applied
early during infection
Ward et al.[33]
(1993)
ND Trifluridine or
dexamethasone or
artificial tears
Topical eye drops n =74 No beneficial effect of trifluridineover
other regimens
Colin and
Chastel[34]
(1985)
HSV-1 Trifluridine Topical eye drops 1% n =6 Successful
treatment
Hu et al.[35]
(2004)
Vaccinia virus Trifluridine and
vaccinia immune
globulin
Topical eye drops 1% for 14 d(trifluridine); IV single-dose
vaccinia immune globulin
n =1 Successful treatment
Fillmore et al.[36]
(2004)
Vaccinia virus Trifluridine or
trifluridine + vacciniaimmune globulin
Topical eye drops 1%(trifluridine); IV single-dose
vaccinia immune globulin
Trifluridine (n= 10) vs trifluridine +vaccinia immune globulin
(n= 1)
Successful treatment
Wander[37]
(1984)
HSV Trifluridine Topical eye drops, several
times daily
NA Prophylactic treatment in immune
suppressed patients
Continued next page
336Skevaki
etal.
2011AdisData
Inform
atio
nBV.Allrig
htsreserved.
Drugs2011;71(3)
-
(see section 2.3) and valaciclovir (see section 2.8),have
recently been introduced in clinical practicefor the treatment of
viral conjunctivitis caused byherpesviruses.
2.2 Cidofovir
Cidofovir, also known as HPMPC
[(S)-1-(3-hydroxy-2-phosphonylmethoxypropyl)cytosine],is an acyclic
nucleoside phosphonate, which hasbeen used for the treatment of
cytomegalovirusretinitis in patients with AIDS. Maintenancetherapy
with cidofovir involves an infusion onlyonce every 2 weeks, making
it a convenient treat-ment option. Two case reports[21,22] and two
clinicaltrials[23,24] assessing the effect of cidofovir in
viralconjunctivitis were identified.
The first case report involved a 31-year-oldwoman who was
treated with cidofovir for ade-noviral conjunctivitis. Cidofovir
was used as a0.2% solution four times daily for 8 days, result-ing
in resolution of clinical signs and symptoms inthe infected eye,
and preventing spread of infec-tion in the uninfected eye.[21] In
the second casereport, a 44-year-old man with
haemorrhagicadenoviral keratoconjunctivitis was successfullytreated
with intravenous cidofovir 1mg/kg threetimes weekly for 4
weeks.[22] In a clinical trial,cidofovir was used as 0.2% eye drops
alone, or incombination with 1% ciclosporin eye drops fourtimes
daily for a period of 21 days, to treat 39 pa-tients with acute
adenoviral keratoconjunctivitis.The use of cidofovir and
ciclosporin alone or co-administered did not accelerate the
improvementof clinical symptoms of acute adenoviral
kerato-conjunctivitis compared with the natural courseof the
infection.[23] In a second clinical study con-ducted by the same
research team, 34 patients withrecent onset of acute adenoviral
keratoconjunctivi-tis were treated using a higher dose of topical
cido-fovir (1%) with or without 1% ciclosporin for21 days. The
higher dose of cidofovir lowered thefrequency of severe corneal
opacities, but was ac-companied by local adverse effects, such as
erythemaof the lids and injection of the conjunctiva.[24]
In vitro, cidofovir and other nucleoside mono-phosphate
analogues, such as HPMPA
[(S)-9-(3-hydroxy-2-phosphonomethoxypropyl)adenine]Ta
bleI.Contd
Study(year)
Infectiousagent
Drug
Treatm
ent
Studygroups
Efficacya
Zaaletal.[38]
(2001)
VZV
Valaciclovir
Oral1000mg,threetimesdaily
for10d
n=21
Resolutionofvirusinfection,not
complete
resolutionof
inflammation
Colin
etal.[39]
(2000)
HZO
Valacicloviroraciclovir
Oral1000mg,threetimesdaily
for7d(valaciclovir);oral
800mg,fivetimesdaily
for7d
(aciclovir)
Valaciclovir(n=56)vsaciclovir(n=54)
Both
drugsequally
welltolerated
andeffectiveinpreventingocular
complications;valaciclovir
providedabetterdosingscheme
Teuchner
etal.[40](2005)
Ad3,Ad4,Ad8,
Ad19andAd37,
enterovirusesor
staphylococci
N-chlorotaurineor
gentamicin
Topicaleyedrops1%
for7d
N-chlorotaurine(n=33)vs
gentamicin(n=27)
N-chlorotaurinewaswelltolerated
andshortenedthedurationof
illness
Pelletieretal.[41]
(2009)
Adenovirus
Povidone-iodineand
dexamethasone
Topicaleyedrops0.4%
povidone-iodine/0.1%
dexamethasone,fourtimes
daily
for5d
n=6
Clinicalresolutionanddecrease
inviraltitre
aBasedonthestatementsoftheauthors.
Ad=adenovirusserotype;HSV=herpessimplexvirus;HuIFN=humaninterferon;HZO=herpeszosterophthalmicus;IFN=interferon;IV=intravenous;NA=notapplicable;
ND=notdeterm
ined;VZV=varicella
zostervirus.
Antiviral Treatment for Viral Conjunctivitis 337
2011 Adis Data Information BV. All rights reserved. Drugs 2011;
71 (3)
-
Table II. Summary of antiviral regimens for viral conjunctivitis
tested in experimental animal models
Study (year) Experimental
animal model
Infection agent Drug Treatment Efficacya
Trousdale and
Nesburn[42]
(1982)
New Zealand
white rabbit
HSV-1 parent McKrae
strain and idoxuridine- or
vidarabine-resistant
variants
Aciclovir, idoxuridine or
vidarabine
Topical, eye drops 3%, 15 timesdaily; IV 50mg/kg, twice
daily(aciclovir)
Aciclovir reduced conjunctivitis occurrence
only when applied prophylactically; IV
aciclovir suppressed infection in the nervous
system
Romanowski
et al.[43] (2001)
New Zealand
white rabbit
Ad5 clinical isolate Cidofovir or placebo Topical, eye drops
0.5% or 1%,twice daily for 7 d
Reduction in viral titres only when applied
prophylactically; no ocular toxicity was
observed
Gordon
et al.[44] (1994)
New Zealand
white rabbit
Ad5 clinical isolates Cidofovir or placebo Topical, eye drops
0.1% or 0.2%,29 times daily for up to 10 d
Reduction in viral titres and duration of
shedding when applied therapeutically;
ocular toxicity was observed in high doses
Romanowski
et al.[45] (1997)
New Zealand
white rabbit
Ad5 clinical isolate Cidofovir, cidofovir +corticosteroids or
placebo
Topical, eye drops 1%, twice daily for3 d (cidofovir); topical,
eye drops 1%,four times daily for 14 d
(corticosteroids)
Cidofovir reduced viral titres and duration of
shedding when applied therapeutically.
Corticosteroids reversed the antiviral activity
of cidofovir
Romanowski
et al.[46] (2001)
New Zealand
white rabbit
Ad5 prototype VR-5 strain
and three in vitro isolated
cidofovir-resistant
variants
Cidofovir or placebo Topical, eye drops 0.5%, twice dailyfor 7
d
Significant antiviral activity against parental
but not resistant isolates
Kaneko
et al.[47] (2004)
Cotton rat Ad5 prototype Cidofovir or placebo Topical, eye drops
1%, twice dailyfor up to 14 d
Reduction in viral titres when applied
therapeutically
Fontenelle
et al.[48] (2008)
Cat FHV-1 Cidofovir or placebo Topical, eye drops 0.5%, twice
dailyfor 10 d
Decrease in viral shedding and severity
of disease
Inoue et al.[49]
(2009)
Japanese
white rabbit
Absence of infection Cidofovir, zalcitabine,
stavudine or placebo
Topical, eye drops 1%, four timesdaily for 14 d
Adverse effects observed: redness
of eyelids and conjunctival injection by all
drugs; narrowing of lacrimal canaliculus by
cidofovir
Malik et al.[50]
(2009)
Cat FHV-1 Famciclovir Oral 62.5mg (~15mg/kg), once dailyfor 7 d,
then twice daily for 736d
Well tolerated, positive impact on the
condition
Tokumaru[51]
(1975)
Hamster and
rabbit
HSV and vesicular
stomatitis virus
Tilorone dihydrochloride
as IFN inducer
Topical solution Improvement in conjunctivitis occurrence
Bitko et al.[52]
(2007)
BALB/cmouse
RSV siRNA against RSV Topical solution 1 nmol dose given
once
Prevented infection when applied
prophylactically but not therapeutically
Stiles[53]
(1995)
Cat FHV-1 Idoxuridine, vidarabine,
trifluridine, antibacterials,
atropine, corticosteroids or
human IFNa
Topical (for all antiviral agents);
oral (human IFNa)Difficult to determine superiority of the
various antiviral treatments
Mohanty
et al.[54] (1980)
Calf Bovine rhinotracheitis
virus
2-deoxy-D-glucose Topical solution Reduced severity of disease
when applied
prophylactically and therapeutically
Continued next page
338Skevaki
etal.
2011AdisData
Inform
atio
nBV.Allrig
htsreserved.
Drugs2011;71(3)
-
and 20-nor-cyclic guanosine monophosphate, havedemonstrated
significant inhibitory activity againstcommon clinical ocular
isolates and standardadenoviral serotypes (1, 5, 8 and 19) related
toviral conjunctivitis.[59] In addition, in a series ofexperiments
in the New Zealand rabbit ocularmodel, topical administration of
cidofovir sig-nificantly reduced adenovirus serotype 5 (Ad5)ocular
titres and shortened the duration of shed-ding in comparison with
control eyes when admin-istered prophylactically[43] or after an
establishedAd5 infection.[44,45] In one of these studies, com-bined
treatment with corticosteroids significantlyreversed the antiviral
activity of cidofovir;[45]
therefore, caution should be taken when treatingsymptomatic
adenoviral ocular infection. In an-other study performed with the
New Zealandrabbit ocular model, although topical cidofovirtreatment
demonstrated significant antiviral activityagainst the parental Ad5
strain, three cidofovir-resistant variants of this virus were
identified.[46]
The antiviral effect of cidofovir was also testedusing the
cotton rat model for adenovirus sero-types 4, 8 and 37,[47] and
with primary ocular felineherpesvirus-1 infection in cats,[48]
where the in-hibitory effect of cidofovir on viral replicationwas
confirmed. Finally, another study examinedthe possible adverse
effects from the use of cido-fovir, as well as of zalcitabine and
stavudine, whichhave been used for the treatment of HIV, in
ade-novirus infections; a solution containing 1% ofeach
aforementioned agent was administered aseye drops to healthy female
Japanese albino rabbitsfour times daily for 14 days. Redness of
eyelidsand conjunctival injection were observed in allstudy groups,
while narrowing of the lacrimalcanaliculus was observed in the
cidofovir group.[49]
2.3 Famciclovir
Famciclovir is a guanine analogue used for thetreatment of
various herpesvirus infections, mostcommonly for herpes zoster. It
is a prodrug formof penciclovir with improved oral
bioavailability.Famciclovir displays the same antiviral spectrumas
aciclovir in regards to herpesviruses. Only oneclinical study so
far has reported famciclovir forthe treatment of viral
conjunctivitis.[25]Ta
bleII.Contd
Study(year)
Experimental
animalmodel
Infectionagent
Drug
Treatm
ent
Efficacya
Brandt
etal.[55](1996)
BALB/c
mouse
HSV-1
KOSstrain
Peptidomimeticribonucleotide
reductaseinhibitororplacebo
Topicalcream
0.1%,1%
or5%,six
timesdaily
for3d,thenfourtimes
daily
for4d
Reducedseverityofinfectionandviral
sheddingatthehigherdoseused
Epstein
etal.[56](2006)
NewZealand
whiterabbit
Ad5prototypeVR-5
strain
Cobaltchelate
orplacebo
Topicalsolution25or50mg/m
L,
69timesdaily
for21d
Reduceddiseaseseverityandviraltitresby
allconcentrationsandfrequenciesusedvs
placebo
Trousdale
etal.[57](1994)
Cottonrat
Ad5wild-type300
Ganciclovirorplacebo
Topicaleyedrops0.3%,
1%
or3%
for21d
Decreaseinincidence,durationandvirus
titrewith3%
ganciclovir,althoughnot
statistically
significant
Romanowski
etal.[58](2009)
NewZealand
whiterabbit
Ad5clinicalisolate
ddC,cidofovirorplacebo
Topicaleyedrops2%
or3%,four
timesdaily
for7d(ddC);topical,eye
drops0.5%,twicedaily
for7d
(cidofovir)
ddCwasmore
efficientthancidofovirin
reducingviraltitresintheearlyphaseof
infection
aBasedonthestatementsoftheauthors.
Ad5=adenovirusserotype5;ddC=2
0 ,30
-dideoxycytidine;FHV=felineherpesvirus;HSV=herpessimplexvirus;IFN=interferon;IV=intravenous;RSV=respiratory
syncytialvirus;
siRNA=small-interferingRNA.
Antiviral Treatment for Viral Conjunctivitis 339
2011 Adis Data Information BV. All rights reserved. Drugs 2011;
71 (3)
-
A large clinical study comprising of 454 pa-tients with
ophthalmic herpes zoster of the tri-geminal nerve V1 branch took
place in 87 centresworldwide and compared the efficacy and safetyof
famciclovir with aciclovir. Famciclovir 500mgwas administered three
times daily and aciclovir800mg five times daily, both orally for 7
days.The percentage of patients who experienced an
ocular manifestation, such as conjunctivitis, ker-atitis and
glaucoma, during the study was similarfor the famciclovir and
aciclovir groups, demon-strating that there was no difference
between thetwo therapeutic agents. Nevertheless, as is the casewith
valaciclovir, famciclovir provides patientswith a more convenient
dosing regimen thanaciclovir.[25]
Table III. Summary of antiviral regimens for viral
conjunctivitis tested in in vitro experimental systems
Study (year) Experimental system Infectious agent Drug
Efficacya
Gordon et al.[59]
(1991)
A549 human alveolar epithelial
cells
Ad1, Ad5, Ad8
or Ad19
Cidofovir (HPMPC) or
HPMPA or 20-nor-cyclicGMP
Inhibition of viral replication;
cidofovir was the least toxic
Langford
et al.[60] (1988)
Changs human conjunctival
cells
Cox A24 Human IFNa or IFNb Both equally reduced virus
infectionand production
Langford
et al.[61] (2003)
Human conjunctival and lens
cells
EV70 Rabbit or human serum
IFNaIFNa enhanced the protective effect ofserum, observed only
in conjunctival cells
Langford
et al.[62] (1983)
WISH human amniotic
epithelial cells, Changs human
conjunctival cells and RK-13
rabbit kidney cells
Ad3, Cox
A24, EV70
or HSV-1(F)
Human IFNa, IFNb orIFNg antiviralantibodies
Synergistic effect of treatments in
reducing viral production, which was
dependent on the type of IFN
Jun et al.[63]
(2008)
Primary human conjunctival
cells
Cox A24 siRNA against the cis-
acting replication
element of Cox A24
Decrease of viral replication
Jun et al.[64]
(2011)
MRC5 human lung fibroblasts
and primary human
conjunctival cells
Cox A24 or
EV70
siRNA against the viral
polymerase 3D gene of
both viruses
Cytoprotective effect; decrease in viral
replication protein synthesis
Tan et al.[65]
(2008)
Human rhabdomyosarcoma
cells
EV70 siRNA against the viral
polymerase 3D gene of
EV70
Prevention of viral replication when the
siRNA was added prophylactically;
reduction of viral production when added
after infection
Monnerat
et al.[66] (2006)
A549 human alveolar epithelial
cells
Ad8 Povidone-iodine Effective against free adenovirus but
not
against intracellular adenoviral particles in
already infected cell; low cytotoxicity for
healthy cells
Uchio et al.[67]
(2007)
A549 human alveolar epithelial
cells
Ad3, Ad4,
Ad8, Ad19
or Ad37
Zalcitabine, stavudine,
nevirapine, indinavir or
amprenavir
Zalcitabine and stavudine reduced
adenoviral replication
Langford
et al.[68] (1985)
WISH human amniotic
epithelial cells
Cox A24 or
EV70
Arildone, IFNb orArildone + IFNb
Arildone reduced viral replication and did
not affect IFN production; additive effect of
arildone and IFNb in reducing viral titres
Langford
et al.[69] (1995)
Changs human conjunctival,
Hep-2 laryngeal and glioma
cells
Cox A24 or
EV70
Benzimidazoles Inhibition of virus production and of the
viral cytopathogenic effect
Johansson
et al.[70] (2007)
Human corneal epithelial cells Ad37 Multivalent sialic acid
conjugated to HAS
or monosaccharidic
sialic acid
Multivalent sialic acid conjugated to HAS
was more efficient in preventing infection
of cells
a Based on the statements of the authors.
Ad =adenovirus serotype; Cox A24 = coxsackie virus A24 variant;
EV70= enterovirus 70; GMP =guanosine monophosphate; HAS =humanserum
albumin; HPMPC=
(S)-1-(3-hydroxy-2-phosphonylmethoxypropyl)cytosine; HPMPA=
(S)-9-(3-hydroxy-2-phosphonomethoxypropyl)a-denine; HSV=herpes
simplex virus; IFN= interferon; siRNA= small-interfering RNA.
340 Skevaki et al.
2011 Adis Data Information BV. All rights reserved. Drugs 2011;
71 (3)
-
In addition, in a small-scale study (n = 10) onfeline
herpesvirus-1-associated disease in cats,famciclovir was well
tolerated and, in all cases,had a positive impact on the animals
condition;however, no untreated controls or animals thatreceived
another therapeutic regimen were in-cluded in the study.[50]
2.4 Idoxuridine
Idoxuridine, a modified form of deoxyuridine,is a nucleoside
analogue, which is incorporatedinto viral DNA during replication
and blocks basepairing. It is used as an anti-herpesvirus
drug.Effective treatment of herpetic keratitis withidoxuridine was
first reported in 1962,[72] and formany years idoxuridine was the
only antiviral agentavailable for its treatment. We identified a
clinicaltrial involving 70 patients with conjunctivitis whowere
treated with 0.5% idoxuridine ointment orplacebo, applied several
times daily for 7 days.Idoxuridine treatment did not have any
influencein the typical course of the disease.[26]
Idoxuridinetreatment has been reported to be associated withhigh
toxicity. The adverse effects arising fromtopical application of
idoxuridine have been re-viewed elsewhere.[73]
2.5 Interferons
Interferons (IFNs) are natural proteins pro-duced by cells in
response to viral infection andaim to control viral spread. Our
search identifiedsix clinical evaluations of the effect of IFNs
inviral conjunctivitis.[27-32] Five of these were
clinicaltrials[27-31] and one summarized clinical data.[32]
Plasmid-derived IFNa-2 or placebo was usedto treat a total of 14
patients with adenoviralconjunctivitis. The authors found no
statisticallysignificant effect of the IFN used on diseaseduration
or virus shedding, although they ob-served a tendency towards
asymptomatic infec-tion in the second eye in the IFN-treated
groupversus the control group.[27] Topical applicationof human
fibroblast-derived IFNb (HuIFNb)was used in the treatment of
epidemic kerato-conjunctivitis caused by an adenovirus. A total
of12 105 reference units daily, divided into eightto ten drops,
reduced the length of the disease
compared with corticosteroid- and placebo-trea-ted groups.[28]
In another clinical trial involving37 participants, HuIFNb was
again topicallyadministered (7.5 105 IU/mL, one drop fivetimes
daily for 1 week) to patients with adeno-viral
keratoconjunctivitis. Improvement with top-ical HuIFNb compared
with placebo was foundto be statistically significant when left
eyes wereaffected, but not when right eyes were involved,an
observation that could not be explained by theauthors.[29] In a
larger-scale clinical trial, a totalof 150 patients with
keratoconjunctivitis, due toadenovirus serotype 8 (Ad8), were
randomly treatedwith exogenous IFNa combined with other
med-ications; however, this regimen proved less effi-cient than
polyvinylpyrrolidone-iodine treatment.In the same study, no
prophylactic effect of IFNaon uninflamed fellow eyes was
observed.[30] Ofnote, another large-scale clinical trial
reportedthe prevention of highly contagious viral
kerato-conjunctivitis by an unidentified virus in 123 of130
patients in total after topical IFN applica-tion. The treatment
comprised of one drop pereye daily for a period of 12 days.[31]
Finally,clinical data collected from the use of HuIFNb,either in
the form of cream (20 000 IU/g) to treatHSV-1 and herpes zoster
ophthalmicus, or in theform of eye drops (500 0001 000 000U) for
thetreatment of adenovirus infections, proved to beefficient in
shortening the course of the diseasewhen applied in the eyes of
patients who were inthe early stages of the viral
infection.[32]
In animal models of hamster and rabbit cornea,IFN production was
induced by treatment withthe chemical compound tilorone
dihydrochloride,used to treat HSV and vesicular stomatitis
virus.This compound was reported to have promisingresults in
improving conjunctivitis.[51]
In a study comprised of in vitro data, naturaland recombinant
human IFNs (rIFNa and rIFNb)added to Changs human conjunctival cell
cul-tures, which were infected with epidemic isolatesof Cox A24,
were shown to inhibit Cox A24 in-fection with varying effectiveness
depending onthe Cox A24 isolate and the type of IFN used.[60]
In another study, IFNa enhanced the protectiveeffect of rabbit
and human sera with regards toEV70 infection of conjunctival
epithelial cells.[61]
Antiviral Treatment for Viral Conjunctivitis 341
2011 Adis Data Information BV. All rights reserved. Drugs 2011;
71 (3)
-
The possibility of a synergistic antiviral effect ofIFNa, IFNb
or IFNg plus specific antibodyagainst EV70, Cox A24, adenovirus
serotype 3(Ad3) and HSV was investigated in Changsconjunctival
cells. Combinations of 10 units ofanti-EV70 and anti-Cox A24 with
50 units ofIFNa, IFNb or IFNg resulted in an enhancedinhibition of
virus yields, which was greater thanthe sum of the individual
effects; the results weresimilar for Ad3.[62]
In summary, the data existing from the use ofIFNs in the
treatment of viral conjunctivitis areencouraging. Nevertheless,
there are reports thatfailed to observe a beneficial effect of
IFNs. Thesite of infection, time of IFN application, doseand type
of IFN, as well as viral sensitivity to IFNare critical to the
efficacy of this type of treatment.
2.6 RNA Interference
RNA interference is an emerging technologythat aims to block
gene expression. Three in vitrostudies and one animal study
evaluated the use ofsmall-interfering RNA (siRNA) molecules
forreplication inhibition of viruses responsible forthe development
of viral conjunctivitis.[52,63-65]
An siRNA targeting a conserved region ofCox A24 was assessed for
its antiviral potential inan in vitro system of HeLa or primary
humanconjunctival cells infected with several variantsand clinical
isolates of Cox A24. Viral replicationin these cells was decreased
when the specificsiRNA was administered.[63] The same researchteam,
2 years later, developed a novel siRNA thattargeted a conserved
region of both EV70 andCox A24, which was able to decrease
replicationand protein synthesis of both viruses in MRC5and primary
human conjunctival cells.[64] In ad-dition, an siRNA against EV70
reduced viralRNA in a rhabdomyosarcoma cell line when ad-ministered
prior to or shortly after infection.[65]
In a mouse model of respiratory syncytial virus(RSV) infection
of the eye, synthetic anti-RSVsiRNA, applied topically shortly
before viral in-oculation, prevented spread of infection in theeye
and lung; in contrast, when siRNAwas addedat different timepoints
after RSV infection, it of-fered little or no protection.[52]
2.7 Trifluridine
Trifluridine (trifluorothymidine) is also a pyr-imidine
nucleoside; however, it appears to be moreeffective and less toxic
than idoxuridine. Our searchfound six evaluations on the treatment
of viralconjunctivitis with trifluridine, two of which areclinical
trials[30,33] and four are case reports.[34-37]
In a clinical study that included 150 patientswith Ad8 infection
who were treated at random,trifluorothymidine drops in combination
withexogenous IFNawas less successful than povidone-iodine
administration.[30] In addition, randomtreatment of 74 patients
with epidemic kerato-conjunctivitis did not show any beneficial
effectof trifluridine over treatment with dexametha-sone or
artificial tears.[33] In a case series, six pa-tients with a
previous medical history of herpetickeratitis were treated with
trifluridine early onthe course of the HSV-1 conjunctivitis,
showinga fast recovery.[34] Another case report involveda
26-year-old woman who was treated success-fully with a 14-day
course of topical trifluridine incombination with a single dose of
intravenousvaccinia immune globulin for conjunctival
infec-tion.[35] Sixteen confirmed or probable cases ofocular
vaccinia infection occurred in the US De-partment of Defenses
Smallpox Vaccination Pro-gramout of a total of 450293 smallpox
vaccinationsand some of them were successfully treated withtopical
trifluridine 1%.[36] Finally, Wander[37]proposed prophylactic
trifluridine treatment for pa-tients with a history of ocular HSV
who were toundergo immune suppression, although, accordingto the
author, no therapy to date has significantlydecreased the
recurrence rate for HSV infections.
In a study involving 17 cats with ocular herpes-virus disease,
topical trifluridine treatment did notprove to be superior to
idoxuridine or vidarabine.[53]
In summary, trifluridine treatment has been usedto treat cases
of conjunctivitis caused by adeno-viruses, herpesviruses or
smallpox. Nevertheless,current data in regards to its efficacy are
ambiguous.
2.8 Valaciclovir
Valaciclovir is the esterified prodrug of acic-lovir, to which
it is converted in vivo. As such, it
342 Skevaki et al.
2011 Adis Data Information BV. All rights reserved. Drugs 2011;
71 (3)
-
has greater bioavailability than acyclovir and isused to treat
HSV infections and herpes zoster.
We found two studies in the literature in whichvalaciclovir was
used for the treatment of viralconjunctivitis.[38,39] In one of
these articles, oralvalaciclovir was administered at 1000mg
threetimes daily for 10 days. No placebo or other treat-ment group
was included in this study and, there-fore, conclusions regarding
the efficacy of this drugcannot be drawn.[38] In contrast, a study
includ-ing 110 immunocompetent patients with herpeszoster
ophthalmicus compared the efficacy andsafety of valaciclovir with
aciclovir. Valaciclovirwas administered as two 500mg tablets
threetimes daily and aciclovir as one 800mg tablet fivetimes daily,
both for 7 days. The two drugs wereshown to be equally tolerable
and effective inpreventing ocular complications of herpes
zosterophthalmicus, including conjunctivitis, superficialand
stromal keratitis, and pain. However, theauthors considered
valaciclovir to be advantageousversus aciclovir because it provides
a better dos-ing regimen. This study was mainly descriptiveand no
statistical evaluation was performed.[39]
2.9 Other Compounds Tested in Humans
Additional agents that do not directly blockviral replication
have also been used for thetreatment of viral conjunctivitis. An
endogenousagent that has been mainly characterized for
itsantimicrobial activity, N-chlorotaurine, has beentested for
tolerability and efficacy in patients withepidemic
keratoconjunctivitis. Treatment for 7 dayswith eye drops containing
a 1% aqueous solutionof N-chlorotaurine (n = 33) or the
antibacterialgentamicin (n = 27) as a control was well toleratedand
shortened the duration of illness in patientswith infections caused
by a variety of microbes,such as adenovirus types 3, 4, 8, 19 and
37, en-teroviruses or staphylococci.[40]
The broad-spectrum bactericide povidone-iodine, which is a
stable chemical complex ofpolyvinylpyrrolidone and elemental
iodine, hasbeen used as a 0.4% ophthalmic suspension incombination
with 0.1% dexamethasone to treatadenoviral conjunctivitis. The
suspension wasgiven four times daily for 5 days. The results of
the study were regarded as promising by the au-thors; however,
no placebo control patients wereincluded, thus precluding any
definitive conclu-sions.[41] In vitro, povidone-iodine was highly
ef-fective against free adenovirus but less effectiveagainst
intracellular adenoviral particles in al-ready infected
cells.[66]
2.10 Other Compounds Tested in Animalor In Vitro Studies
Many compounds that have not been used yetin clinics have been
reported to have an antiviraleffect against conjunctivitis-relevant
viral strains.In one study, ocular instillation of
2-deoxy-D-glucose markedly reduced the severity of viral-induced
conjunctivitis and keratoconjunctivitis incalves. Of note, the drug
was effective both whengiven at the onset of the infection and
after clin-ical conjunctivitis had already developed.[54]
A peptidomimetic compound, named BILD 1263,which blocks the
ribonucleotide reductase ofHSV-1, was used to treat HSV-1
KOS-infectedmice; the treatment was shown to prevent signs
ofconjunctivitis.[55] The antiviral potency of topicalcobalt
chelate CTC-96 was tested in New Zealandwhite rabbits infected with
Ad5, an in vivo modelof adenoviral keratoconjunctivitis most
similar tohuman disease; CTC-96 treatment resulted inmilder
inflammation of the conjunctiva com-pared with the placebo-treated
group.[56] Treat-ment with 3% ganciclovir reduced adenovirustitres
in cotton rat eyes.[57] Finally, 3% and 2%20,30-dideoxycytidine
treatments were significantlymore efficacious than 0.5% cidofovir
treatmentagainst ocular Ad5 infection in the New Zealandwhite
rabbit replication model.[58]
In an in vitro study with A549 cells, whichevaluated the
efficiency of various anti-HIV agentsagainst adenoviruses,
zalcitabine and stavudine,two nucleoside reverse transcriptase
inhibitors,showed significant activity for adenovirus sero-types 3,
4, 8, 19 and 37; in contrast, nevirapine,a non-nucleoside reverse
transcriptase inhibitor,and indinavir and amprenavir, which are
bothprotease inhibitors, were ineffective against
adeno-viruses.[67] In addition, arildone inhibited theinfectivity
of acute haemorrhagic conjunctivitis
Antiviral Treatment for Viral Conjunctivitis 343
2011 Adis Data Information BV. All rights reserved. Drugs 2011;
71 (3)
-
viruses EV70 and Cox A24 in human amnionicWISH cells in
vitro.[68] The benzimidazoles en-viroxime (LY 122772) and
enviradene (LY 127123)inhibited EV70 and Cox A24 infection of
con-junctival and laryngeal cells in vitro.[69] Finally,multivalent
sialic acid conjugated to human serumalbumin prevented adenovirus
serotype 37 frombinding to and infecting human corneal
epithelialcells 1000-fold more efficiently than mono-saccharidic
sialic acid.[70]
3. Conclusion
We have systematically reviewed the availableliterature and
summarized our findings concern-ing the use of antiviral
medications for the treat-ment of viral conjunctivitis. Most of the
antiviralmedications currently in clinical use target DNAviruses:
mainly herpesviruses, but also adeno-viruses. Data on antiviral
agents targeting RNAviruses as causes of conjunctivitis are
mostlylimited to animal and in vitro studies. Identifica-tion of
the causative viral agent in clinical prac-tice is thus of crucial
importance. Subsequently,the type of treatment should be selected
depen-ding on the severity of symptoms and the mag-nitude of
possible consequences, since severeconjunctivitis, as in the case
of epidemic kerato-conjunctivitis, requires aggressive
management.
Of note, reported cases of chronic con-junctivitis have been
related to corticosteroidtreatment that prolongs viral infection.
Indeed,two studies of the Ad5/New Zealand white rabbitocular model
showed that corticosteroid treat-ment significantly enhanced viral
replication andincreased the duration of viral shedding.[74,75]
Inaddition, topical application ofNSAIDswas shownto be ineffective
in controlling replication of ade-novirus serotypes 1, 5, 8 or 19
in the New Zealandwhite rabbit ocular model.[76] Corticosteroids
arealso contraindicated for the treatment of HSV-1ocular
infections. Treatment of conjunctivitiscaused by HSV-1 with
corticosteroids could leadto increased viral replication and,
possibly, her-petic epithelial keratitis.[77] Thus, caution is
rec-ommended in the use of this type of treatment inviral
conjunctivitis, since it may lead to enhancedrisk of viral
transmission and epidemics.
Additional approaches have been used overthe years for the
management of conjunctivitis.Vaccination against viral strains
causing con-junctivitis has been unsuccessfully used in thepast.
Military recruits were vaccinated for ade-novirus serotypes 4 and 7
between 1971 and 1996,but the vaccine is currently unavailable
after twofatal cases were reported.[78] In recent years, anumber of
viruses have been shown to directlyinterfere with programmed cell
death or apopto-sis, an active process of cellular
self-destructionthat plays an important role during development,but
also acts as a defence mechanism against viralinfections.[79] Viral
products can either blockapoptosis to prevent premature cell death
andmaximize viral progeny, or they can promoteapoptosis to enhance
their spread. Recently, itwas shown that glycyrrhizic acid disrupts
latentinfection of HSV in Kaposi sarcoma by selec-tively inducing
cell death of the HSV-infectedcells.[80] Study of the viral
processes that block orinduce apoptosis may provide opportunities
forfuture drug interventions.
Finally, significant advances in the treatmentof viral
conjunctivitis have been achieved overrecent years with specialized
medications thatblock viral proliferation, which are reported on
inthis review. Many of these are used in clinicalpractice, while
others have proved their useful-ness only in animal or in
vitromodels. Issues suchas efficacy and toxicity still raise
questions.Nevertheless, drugs such as aciclovir, trifluridineand
valaciclovir are the main agents used for themanagement of
conjunctivitis of herpetic origin.In a recent retrospective review
on the effect ofprophylactic oral antiviral treatment on HSV
re-currences in a community-based cohort, oral an-tiviral
prophylaxis was associated with a de-creased risk of recurrence of
several eye disorderscaused by HSV.[81] Further research is
required inorder to find efficacious yet tolerable dosage re-gimens
of antiviral drugs.
Acknowledgements
No sources of funding were used to assist in the prepara-tion of
this review. The authors have no conflicts of interestthat are
directly relevant to the content of this review.
344 Skevaki et al.
2011 Adis Data Information BV. All rights reserved. Drugs 2011;
71 (3)
-
References1. Cronau H, Kankanala RR, Mauger T. Diagnosis and
management of red eye in primary care. Am Fam Physician2010 Jan
15; 81 (2): 137-44
2. Kumar NL, Black D, McClellan K. Daytime presentationsto a
metropolitan ophthalmic emergency department. ClinExperiment
Ophthalmol 2005 Dec; 33 (6): 586-92
3. Weber CM, Eichenbaum JW. Acute red eye: differentiatingviral
conjunctivitis from other, less common causes. Post-grad Med 1997
May; 101 (5): 185-6, 9-92, 95-6
4. Chu PY, Ke GM, Chang CH, et al. Molecular epidemiologyof
coxsackie A type 24 variant in Taiwan, 2000-2007. J ClinVirol 2009
Aug; 45 (4): 285-91
5. Khan A, Sharif S, Shaukat S, et al. An outbreak of
acutehemorrhagic conjunctivitis (AHC) caused by coxsackievirusA24
variant in Pakistan. Virus Res 2008 Oct; 137 (1): 150-2
6. Madhavan HN, Malathy J, Priya K. An outbreak of
acuteconjunctivitis caused by Coxsackie virus A 24 [letter].Indian
J Ophthalmol 2000 Jun; 48 (2): 159
7. Uchio E, Yamazaki K, Ishikawa H, et al. An epidemic ofacute
haemorrhagic conjunctivitis caused by enterovirus 70in Okinawa,
Japan, in 1994. Graefes Arch Clin Exp Oph-thalmol 1999 Jul; 237
(7): 568-72
8. Tan DS, Yin-Murphy M, Kandiah S. An outbreak of
acuteconjunctivitis caused by coxsackievirus A24 in Kuala-Lumpur,
Malaysia, 1978. Southeast Asian J Trop MedPublic Health 1980 Mar;
11 (1): 24-7
9. Gottsch JD. Surveillance and control of epidemic
kerato-conjunctivitis. Trans Am Ophthalmol Soc 1996; 94: 539-87
10. Hamada N, Gotoh K, Hara K, et al. Nosocomial outbreakof
epidemic keratoconjunctivitis accompanying environ-mental
contamination with adenoviruses. J Hosp Infect2008 Mar; 68 (3):
262-8
11. Kaneko H, Maruko I, Iida T, et al. The possibility of
humanadenovirus detection from the conjunctiva in asympto-matic
cases during nosocomial infection. Cornea 2008 Jun;27 (5):
527-30
12. Levandowski RA, Rubenis M. Nosocomial conjunctivitiscaused
by adenovirus type 4. J Infect Dis 1981 Jan; 143 (1):28-31
13. De Clercq E, Neyts J. Antiviral agents acting as DNA orRNA
chain terminators. Handb Exp Pharmacol 2009;(189): 53-84
14. Moher D, Liberati A, Tetzlaff J, et al. Preferred
reportingitems for systematic reviews andmeta-analyses: the
PRISMAstatement. PLoS Med 2009 Jul 21; 6 (7): e1000097
15. Cobo LM, Foulks GN, Liesegang T, et al. Oral acyclovir inthe
treatment of acute herpes zoster ophthalmicus. Oph-thalmology 1986
Jun; 93 (6): 763-70
16. Uchoa UB, Rezende RA, Carrasco MA, et al. Long-termacyclovir
use to prevent recurrent ocular herpes simplexvirus infection. Arch
Ophthalmol 2003 Dec; 121 (12): 1702-4
17. Neoh C, Harding SP, Saunders D, et al. Comparison of
to-pical and oral acyclovir in early herpes zoster ophthalmi-cus.
Eye (Lond) 1994; 8 (Pt 6): 688-91
18. Goon P, Wright M, Fink C. Ophthalmic zoster sine herpete.J R
Soc Med 2000 Apr; 93 (4): 191-2
19. Parentin F, Molin GD, DAgaro P, et al. Parinauds
ocu-loglandular syndrome due to herpes simplex virus type 1.Ocul
Immunol Inflamm 2007 Mar-Apr; 15 (2): 139-41
20. Gajdatsy AD, Kosmin A, Barrett GD. Coexistent adeno-viral
keratoconjunctivitis and Acanthamoeba keratitis.Clin Experiment
Ophthalmol 2000 Dec; 28 (6): 434-6
21. Gordon YJ, Naesens L, DeClercq E, et al. Treatment
ofadenoviral conjunctivitis with topical cidofovir [letter].Cornea
1996 Sep; 15 (5): 546
22. Castleton A, Kottaridis PD. A case of red eye post
allo-geneic stem cell transplantation. Bone Marrow Transplant2007
Feb; 39 (4): 241-2
23. Hillenkamp J, Reinhard T, Ross RS, et al. Topical
treatmentof acute adenoviral keratoconjunctivitis with 0.2%
cidofo-vir and 1% cyclosporine: a controlled clinical pilot
study.Arch Ophthalmol 2001 Oct; 119 (10): 1487-91
24. Hillenkamp J, Reinhard T, Ross RS, et al. The effects
ofcidofovir 1% with and without cyclosporin A 1% as atopical
treatment of acute adenoviral keratoconjunctivitis:a controlled
clinical pilot study. Ophthalmology 2002May;109 (5): 845-50
25. Tyring S, Engst R, Corriveau C, et al. Famciclovir for
oph-thalmic zoster: a randomised aciclovir controlled study. BrJ
Ophthalmol 2001 May; 85 (5): 576-81
26. Dudgeon J, Bhargava SK, Ross CA. Treatment of adeno-virus
infection of the eye with 5-iodo-20-deoxyuridine: adouble-blind
trial. Br J Ophthalmol 1969 Aug; 53 (8): 530-3
27. Adams Jr CP, Cohen EJ, Albrecht J, et al. Interferon
treat-ment of adenoviral conjunctivitis. Am J Ophthalmol 1984Oct
15; 98 (4): 429-32
28. Romano A, Revel M, Guarari-Rotman D, et al. Use of hu-man
fibroblast-derived (beta) interferon in the treatment ofepidemic
adenovirus keratoconjunctivitis. J Interferon Res1980 Fall; 1 (1):
95-100
29. Wilhelmus KR, Dunkel EC, Herson J. Topical human fi-broblast
interferon for acute adenoviral conjunctivitis.Graefes Arch Clin
Exp Ophthalmol 1987; 225 (6): 461-4
30. Hutter H. Epidemic keratoconjunctivitis: treatment
resultsduring an epidemic. Klin Monatsbl Augenheilkd 1990 Sep;197
(3): 214-7
31. Rossa V, Sundmacher R. Local prevention with interferonof
epidemic conjunctivitis caused by a currently uni-dentifiable
virus. Klin Monatsbl Augenheilkd 1991 Sep;199 (3): 192-4
32. Romano A, Sadan Y. Ten years of experience with
humanfibroblast interferon in treatment of viral
ophthalmicinfections. Metab Pediatr Syst Ophthalmol 1988; 11
(1-2):43-6
33. Ward JB, Siojo LG, Waller SG. A prospective, maskedclinical
trial of trifluridine, dexamethasone, and artificialtears in the
treatment of epidemic keratoconjunctivitis.Cornea 1993 May; 12 (3):
216-21
34. Colin J, Chastel C. Early treatment of ocular herpes
simplex:apropos of 6 cases of herpetic conjunctivitis. J Fr
Ophtal-mol 1985; 8 (12): 801-2
35. Hu G,WangMJ, Miller MJ, et al. Ocular vaccinia
followingexposure to a smallpox vaccinee. Am J Ophthalmol 2004Mar;
137 (3): 554-6
36. Fillmore GL, Ward TP, Bower KS, et al. Ocular complica-tions
in the Department of Defense Smallpox VaccinationProgram.
Ophthalmology 2004 Nov; 111 (11): 2086-93
37. Wander AH. Herpes simplex and recurrent corneal disease.Int
Ophthalmol Clin 1984 Summer; 24 (2): 27-38
Antiviral Treatment for Viral Conjunctivitis 345
2011 Adis Data Information BV. All rights reserved. Drugs 2011;
71 (3)
-
38. Zaal MJ, Volker-Dieben HJ, Wienesen M, et al. Long-itudinal
analysis of varicella-zoster virus DNA on theocular surface
associated with herpes zoster ophthalmicus.Am J Ophthalmol 2001
Jan; 131 (1): 25-9
39. Colin J, Prisant O, Cochener B, et al. Comparison of
theefficacy and safety of valaciclovir and acyclovir for
thetreatment of herpes zoster ophthalmicus. Ophthalmology2000 Aug;
107 (8): 1507-11
40. Teuchner B, Nagl M, Schidlbauer A, et al. Tolerability
andefficacy of N-chlorotaurine in epidemic keratoconjuncti-vitis: a
double-blind, randomized, phase-2 clinical trial.J Ocul Pharmacol
Ther 2005 Apr; 21 (2): 157-65
41. Pelletier JS, Stewart K, Trattler W, et al. A
combinationpovidone-iodine 0.4%/dexamethasone 0.1%
ophthalmicsuspension in the treatment of adenoviral
conjunctivitis.Adv Ther 2009 Aug; 26 (8): 776-83
42. Trousdale MD, Nesburn AB. Evaluation of the
antiherpeticactivity of acyclovir in rabbits. Am J Med 1982 Jul 20;
73(1A): 155-60
43. Romanowski EG, Yates KA, Gordon YJ. Antiviral pro-phylaxis
with twice daily topical cidofovir protects againstchallenge in the
adenovirus type 5/New Zealand rabbitocular model. Antiviral Res
2001 Dec; 52 (3): 275-80
44. Gordon YJ, Romanowski EG, Araullo-Cruz T. TopicalHPMPC
inhibits adenovirus type 5 in the New Zealandrabbit ocular
replication model. Invest Ophthalmol Vis Sci1994 Nov; 35 (12):
4135-43
45. Romanowski EG, Araullo-Cruz T, Gordon YJ.
Topicalcorticosteroids reverse the antiviral effect of topical
cido-fovir in the Ad5-inoculated New Zealand rabbit ocularmodel.
Invest Ophthalmol Vis Sci 1997 Jan; 38 (1): 253-7
46. Romanowski EG, Gordon YJ, Araullo-Cruz T, et al.
Theantiviral resistance and replication of
cidofovir-resistantadenovirus variants in the New Zealand White
rabbit ocularmodel. Invest Ophthalmol Vis Sci 2001 Jul; 42 (8):
1812-5
47. Kaneko H, Mori S, Suzuki O, et al. The cotton rat model
foradenovirus ocular infection: antiviral activity of
cidofovir.Antiviral Res 2004 Jan; 61 (1): 63-6
48. Fontenelle JP, Powell CC, Veir JK, et al. Effect of
topicalophthalmic application of cidofovir on experimentally
in-duced primary ocular feline herpesvirus-1 infection in cats.Am J
Vet Res 2008 Feb; 69 (2): 289-93
49. Inoue H, Sonoda KH, IshikawaM, et al. Clinical evaluationof
local ocular toxicity in candidate anti-adenoviral agentsin vivo.
Ophthalmologica 2009; 223 (4): 233-8
50. Malik R, Lessels NS, Webb S, et al. Treatment of
felineherpesvirus-1 associated disease in cats with famciclovirand
related drugs. J Feline Med Surg 2009 Jan; 11 (1): 40-8
51. Tokumaru T. The mode of inhibition of herpes simplex
andvesicular stomatitis ocular viral infections in the rabbit
andhamster by an interferon inducer tilorone dihydrochloride.Res
Commun Chem Pathol Pharmacol 1975 Jun; 11 (2):289-301
52. Bitko V, Musiyenko A, Barik S. Viral infection of the
lungsthrough the eye. J Virol 2007 Jan; 81 (2): 783-90
53. Stiles J. Treatment of cats with ocular disease attributable
toherpesvirus infection: 17 cases (1983-1993). J Am Vet MedAssoc
1995 Sep 1; 207 (5): 599-603
54. Mohanty SB, Rockemann DD, Tripathy RN. Chemother-apeutic
value of 2-deoxy-D-glucose in infectious bovine
rhinotracheitis viral infection in calves. Am J Vet Res 1980Jul;
41 (7): 1049-51
55. Brandt CR, Spencer B, Imesch P, et al. Evaluation of
apeptidomimetic ribonucleotide reductase inhibitor with amurine
model of herpes simplex virus type 1 ocular disease.Antimicrob
Agents Chemother 1996 May; 40 (5): 1078-84
56. Epstein SP, Pashinsky YY, Gershon D, et al. Efficacy
oftopical cobalt chelate CTC-96 against adenovirus in a cellculture
model and against adenovirus keratoconjunctivitisin a rabbit model.
BMC Ophthalmol 2006; 6: 22
57. Trousdale MD, Goldschmidt PL, Nobrega R. Activity
ofganciclovir against human adenovirus type-5 infection incell
culture and cotton rat eyes. Cornea 1994 Sep; 13 (5):435-9
58. Romanowski EG, Yates KA, Gordon YJ. The in vitro andin vivo
evaluation of ddC as a topical antiviral for ocularadenovirus
infections. Invest Ophthalmol Vis Sci 2009Nov; 50 (11): 5295-9
59. GordonYJ, Romanowski E,Araullo-Cruz T, et al.
Inhibitoryeffect of (S)-HPMPC, (S)-HPMPA, and 20-nor-cyclic GMPon
clinical ocular adenoviral isolates is serotype-dependentin vitro.
Antiviral Res 1991 Jul; 16 (1): 11-6
60. Langford MP, Kadi RM, Ganley JP, et al. Inhibition
ofepidemic isolates of coxsackievirus type A 24 by re-combinant and
natural interferon alpha and interferonbeta. Intervirology 1988; 29
(6): 320-7
61. Langford MP, Orillac R, Chen D, et al. Systemic and
ocularantibody responses to inactivated acute hemorrhagic
con-junctivitis (AHC) virus; enterovirus 70 (EV70). Ocul Im-munol
Inflamm 2003 Sep; 11 (3): 197-209
62. Langford MP, Villarreal AL, Stanton GJ. Antibody
andinterferon act synergistically to inhibit enterovirus,
adeno-virus, and herpes simplex virus infection. Infect Immun1983
Jul; 41 (1): 214-8
63. Jun EJ, NamYR, Ahn J, et al. Antiviral potency of a
siRNAtargeting a conserved region of coxsackievirus A24. Bio-chem
Biophys Res Commun 2008 Nov 14; 376 (2): 389-94
64. Jun EJ,WonMA, Ahn J, et al. An antiviral
small-interferingRNA simultaneously effective against the most
prevalententeroviruses causing acute hemorrhagic
conjunctivitis.Invest Ophthalmol Vis Sci 2011; 52 (1): 58-63
65. Tan EL, Marcus KF, Poh CL. Development of RNAinterference
(RNAi) as potential antiviral strategy againstenterovirus 70. J Med
Virol 2008 Jun; 80 (6): 1025-32
66. Monnerat N, Bossart W, Thiel MA. Povidone-iodine
fortreatment of adenoviral conjunctivitis: an in vitro study.Klin
Monatsbl Augenheilkd 2006 May; 223 (5): 349-52
67. Uchio E, Fuchigami A, Kadonosono K, et al. Anti-adeno-viral
effect of anti-HIV agents in vitro in serotypes
inducingkeratoconjunctivitis. Graefes Arch Clin Exp Ophthalmol2007
Sep; 245 (9): 1319-25
68. Langford MP, Carr DJ, Yin-Murphy M. Activity of ar-ildone
with or without interferon against acute hemor-rhagic
conjunctivitis viruses in cell culture. AntimicrobAgents Chemother
1985 Oct; 28 (4): 578-80
69. Langford MP, Ball WA, Ganley JP. Inhibition of the
en-teroviruses that cause acute hemorrhagic conjunctivitis(AHC) by
benzimidazoles; enviroxime (LY 122772) andenviradone (LY 127123).
Antiviral Res 1995 Aug; 27 (4):355-65
346 Skevaki et al.
2011 Adis Data Information BV. All rights reserved. Drugs 2011;
71 (3)
-
70. Johansson SM, Nilsson EC, Elofsson M, et al.
Multivalentsialic acid conjugates inhibit adenovirus type 37
frombinding to and infecting human corneal epithelial
cells.Antiviral Res 2007 Feb; 73 (2): 92-100
71. Stuart-Harris C. The epidemiology and clinical
presentationof herpes virus infections. J Antimicrob Chemother
1983Sep; 12 Suppl. B: 1-8
72. Kaufman HE, Nesburn AB, Maloney ED. Cure of
vacciniainfection by 5-iodo-20-deoxyuridine. Virology 1962 Dec;18:
567-9
73. Angra SK. IDU ocular toxicity. Indian J Ophthalmol 1977Jul;
25 (2): 38-41
74. Romanowski EG, Roba LA, Wiley L, et al. The effects
ofcorticosteroids of adenoviral replication. Arch Ophthalmol1996
May; 114 (5): 581-5
75. Romanowski EG, Yates KA, Gordon YJ. Short-termtreatment with
a potent topical corticosteroid of an acuteocular adenoviral
infection in the New Zealand white rab-bit. Cornea 2001 Aug; 20
(6): 657-60
76. Gordon YJ, Araullo-Cruz T, Romanowski EG. The effectsof
topical nonsteroidal anti-inflammatory drugs on adeno-viral
replication. Arch Ophthalmol 1998 Jul; 116 (7): 900-5
77. Dawson CR, Togni B. Herpes simplex eye infections:
clinicalmanifestations, pathogenesis and management. SurvOphthalmol
1976 Sep-Oct; 21 (2): 121-35
78. Two fatal cases of adenovirus-related illness in
previouslyhealthy young adults: Illinois, 2000.MMWRMorbMortalWkly
Rep 2001 Jul 6; 50 (26): 553-5
79. OBrien V. Viruses and apoptosis. J Gen Virol 1998 Aug; 79(Pt
8): 1833-45
80. Curreli F, Friedman-Kien AE, Flore O. Glycyrrhizic
acidalters Kaposi sarcoma-associated herpesvirus latency,triggering
p53-mediated apoptosis in transformed B lym-phocytes. J Clin Invest
2005 Mar; 115 (3): 642-52
81. Young RC, Hodge DO, Liesegang TJ, et al. Incidence,
re-currence, and outcomes of herpes simplex virus eye diseasein
Olmsted County, Minnesota, 1976-2007: the effect oforal antiviral
prophylaxis. Arch Ophthalmol 2010 Sep; 128(9): 1178-83
Correspondence: Dr Chrysanthi L. Skevaki, 41 Fidipidou str,11527
Athens, Greece.E-mail: [email protected]
Antiviral Treatment for Viral Conjunctivitis 347
2011 Adis Data Information BV. All rights reserved. Drugs 2011;
71 (3)
-
Reproduced with permission of the copyright owner. Further
reproduction prohibited without permission.
Treatment of Viral Conjunctivitis with Antiviral DrugsAbstract1.
Methods of Literature Review1.1 Literature Search1.2 Study
Selection and Eligibility Criteria1.3 Data Evaluation
2. Results2.1 Aciclovir2.2 Cidofovir2.3 Famciclovir2.4
Idoxuridine2.5 Interferons2.6 RNA Interference2.7 Trifluridine2.8
Valaciclovir2.9 Other Compounds Tested in Humans2.10 Other
Compounds Tested in Animal orInVitro Studies
3. ConclusionAcknowledgementsReferences