Embed Size (px)
Citation preview
Page 1 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
Outcomes Report Companion Guide March, 2021
The mission of the NCDR® is to improve the quality of cardiovascular patient care by providing information, knowledge and tools; implementing quality initiatives; and supporting research that improves patient outcomes.
The NCDR® is an initiative of the American College of Cardiology Foundation, with collaborative support from the Society for Cardiovascular Angiography and Interventions for the LAAO Registry .
CONFIDENTIALITY NOTICE This document contains information confidential and proprietary to the American College of Cardiology Foundation. This document is intended to be a confidential communication between ACCF and participants of the LAAO Registry and may involve information or material that may not be used, disclosed or reproduced without the written authorization of the ACCF. Those so authorized may only use this information for a purpose consistent with the authorization. Reproduction of any section of this document with permission must include this notice.

Page 2 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
Companion Guide to your NCDR® Outcomes Reports
Table of Contents Frequently Used Terminology………………………………………………………………………………3
Access to your Report4……………………………………………………………………………………..4 Specifications for Executive Summary Measures and Metrics……………………………………………..6 Section I: LAAO Episode of Care Metrics………………………………………………………………….7 Performance Measures………………………………………………………………………………….....7
Process Metrics……………………………………………………………………………………...……..7 1. Proportion of patients undergoing left atrial appendage occlusion evaluated for stroke risk using the CHA2DS2-VASc Risk score.……………………………………………………………………..………...7 2. Proportion of patients undergoing left atrial appendage occlusion evaluated for bleeding risk using the
HAS-BLED Risk score………………………………………………………………………………..…….9 3. Proportion of patients undergoing left atrial appendage occlusion procedure per FDA indications… ....10 Outcome Metrics…………………………………………………………………………………………..12 4. Proportion of left atrial appendage occlusion procedures successful…………………………………....12
5. Proportion of left atrial appendage occlusion procedures successful excluding those procedures canceled…………………………………………………………………………………………….……....13 6. Proportion of patients with a major complication either intra or post left atrial occlusion procedure and prior to discharge …………………………………………………………………………………….….…14
7. Proportion of patients experiencing a disabling or life threatening bleeding event intra or post left atrial appendage occlusion procedure and prior to discharge ……………………………………………..….….15 8. Proportion of patients who experience a stroke (ischemic or hemorrhagic), or systemic embolism or mortality intra or post procedure and prior to discharge…...........................................................................16
9. Proportion of patients who experience an ischemic stroke or systemic embolism intra or post procedure and prior to.....................................................................................................................................................17

Page 3 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
Overview The LAAO Registry Institutional Outcomes Report provides detailed analysis of a hospital's individual performance in relation to hospitals of similar volume and the entire registry population. This gives insight into care variations and quality improvement opportunities. The report provides the opportunity to compare hospital practice patterns to NCDR benchmarks.
Frequently Used Terminology
R4Q (Rolling Four Quarters)
The four (4) consecutive quarters included in this report. (Example: The 2011Q1 report includes 2010Q2, 2010Q3, 2010Q4 and 2011Q1. The “Q” in ‘R4Q” indicates the last quarter of the rolling four quarters).
Benchmark Inclusion Status
Indicates whether a submission will be included in the R4Q aggregated data (benchmark) and comparison group statistics. “Green,” “Yellow” and “Red” stoplights denote the status.
Green status A “Green” status indicates the submission (one quarter/timeframe) is included in the benchmark and comparison group statistics. The data has successfully passed all data assessment and completeness checks.
Yellow status A “Yellow” status indicates the submission (one quarter/timeframe) is not included in the benchmark and comparison group statistics. Data is displayed in the quarterly column, but is not included in the “My Hospital R4Q” summary. The data has not passed the overall completeness assessment checks.
Red status A “Red” status indicates the submission (one quarter/timeframe) is not included in the benchmark or comparison group statistics. Data is not displayed in the quarterly column.
Null status A null or blank status indicates no submission has been received for that quarter/timeframe. Data is not displayed in the quarterly column.
My Hospital R4Q The values for a metric/measure (over R4Q) of data submitted by your facility with a Benchmark Inclusion Status of “Green”.
All Hospital 50th Pctl The median (or midpoint or 50th percentile) of all participants’ aggregated data for the metric or measure. Half of all participants will be above the median, and half will be below. This value will correspond to the midpoint of the box/whisker plot with a Benchmark Inclusion Status of “Green”.
All Hospital 90th Pctl The 90th percentile of all participants’ aggregated data for the metric or measure. 10% of all participants will be above the 90 th percentile value, and 90% will be below. This value will correspond to the right-most endpoint of the box/whisker plot with a Benchmark Inclusion Status of “Green”.
DQR The online system used to check that data are well formed and complete. Data must first be submitted to the DQR to be included in the Outcomes Report.
Base The term Base identifies care provided during the patient’s Episode of Care that includes the index LAAO procedure.
Follow Up The LAAO Registry captures follow up care level information on patients for each procedure. Metrics are provided based upon patient status and care received at 45 days, 6 months, 1 year, and 2 years post procedure.
Page 4 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
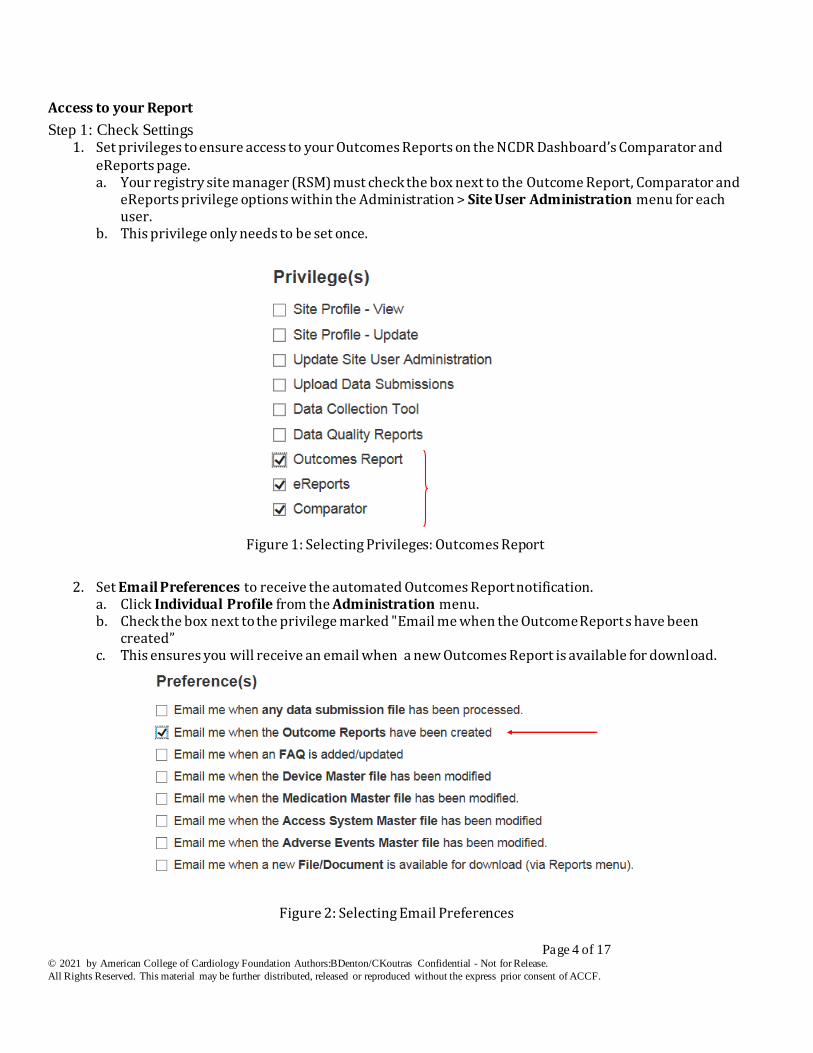
Access to your Report
Step 1: Check Settings 1. Set privileges to ensure access to your Outcomes Reports on the NCDR Dashboard’s Comparator and
eReports page. a. Your registry site manager (RSM) must check the box next to the Outcome Report, Comparator and
eReports privilege options within the Administration > Site User Administration menu for each user.
b. This privilege only needs to be set once.
Figure 1: Selecting Privileges: Outcomes Report
2. Set Email Preferences to receive the automated Outcomes Report notification.
a. Click Individual Profile from the Administration menu. b. Check the box next to the privilege marked "Email me when the Outcome Report s have been
created” c. This ensures you will receive an email when a new Outcomes Report is available for download.
Figure 2: Selecting Email Preferences
Page 5 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
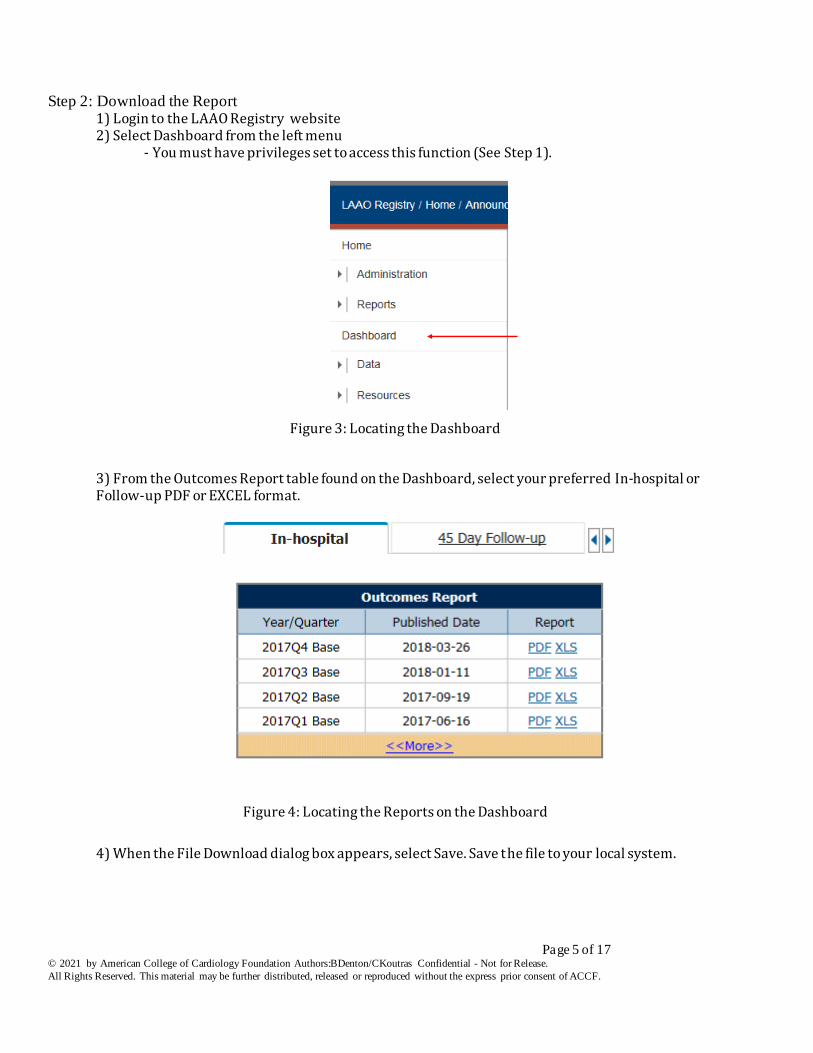
Step 2: Download the Report 1) Login to the LAAO Registry website 2) Select Dashboard from the left menu - You must have privileges set to access this function (See Step 1).
Figure 3: Locating the Dashboard
3) From the Outcomes Report table found on the Dashboard, select your preferred In-hospital or Follow-up PDF or EXCEL format.
Figure 4: Locating the Reports on the Dashboard
4) When the File Download dialog box appears, select Save. Save the file to your local system.
Page 6 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
Specifications for Executive Summary Measures and Metrics
Executive Summary The Executive Summary contains metrics as well as some graphs: 1. Metrics are divided into three sections: Performance,Outcome and Process Metrics. These are used to support self assessment and quality improvement at the provider, hospital, and/or health care system level.
a. Detail Line - This refers to the line number in the Detail Section of the report. Each of the metrics refers to lines in the LAAO Registry report. b. My Hospital -Refers to the “My Hospital R4Q %” column of the Detail Section of the report. This is the value for your institution over the rolling four quarters (R4Q) period. c. All Hospitals 50th Percentile – refers to the performance of the hospital at the mid-point. Half of the hospitals performed better and half performed worse. d. All Hospitals 90th Percentile – refers to the performance of the hospital at the 90th percentile. 10% of the hospitals performed better and 90% performed worse. The 90th percentile or greater is considered “best practice”.
Page 7 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
Section I: LAAO Episode of Care Metrics
Performance Measures Endorsed by the National Quality Forum and appropriate for public reporting. None currently for the LAAO Registry.
Process Metrics
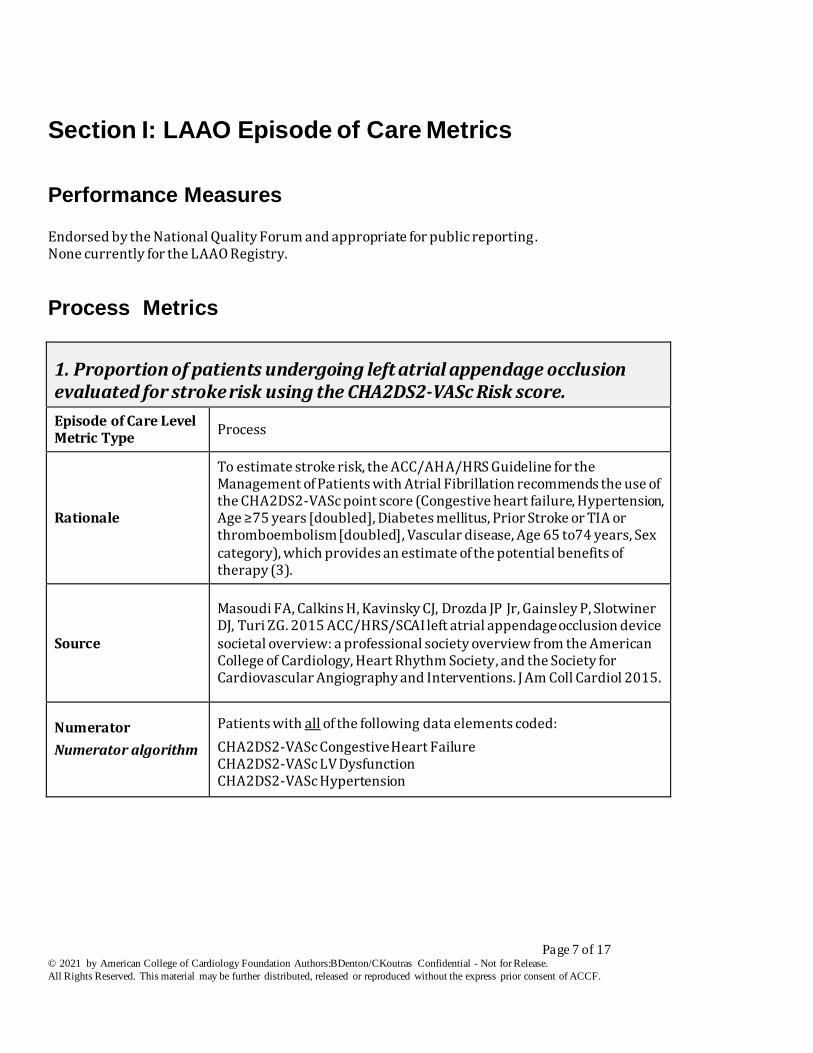
1. Proportion of patients undergoing left atrial appendage occlusion evaluated for stroke risk using the CHA2DS2-VASc Risk score.
Episode of Care Level Metric Type
Process
Rationale
To estimate stroke risk, the ACC/AHA/HRS Guideline for the Management of Patients with Atrial Fibrillation recommends the use of the CHA2DS2-VASc point score (Congestive heart failure, Hypertension, Age ≥75 years [doubled], Diabetes mellitus, Prior Stroke or TIA or thromboembolism [doubled], Vascular disease, Age 65 to74 years, Sex category), which provides an estimate of the potential benefits of therapy (3).
Source
Masoudi FA, Calkins H, Kavinsky CJ, Drozda JP Jr, Gainsley P, Slotwiner DJ, Turi ZG. 2015 ACC/HRS/SCAI left atrial appendage occlusion device societal overview: a professional society overview from the American College of Cardiology, Heart Rhythm Society, and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2015.
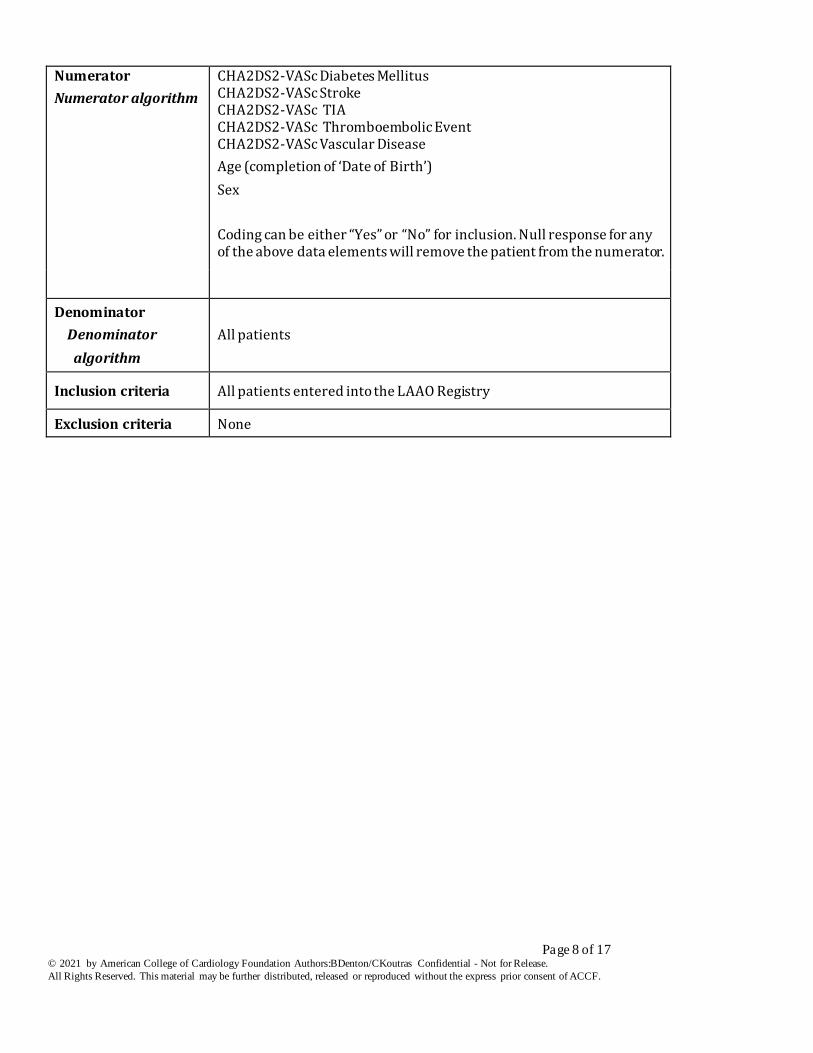
Numerator
Numerator algorithm
Patients with all of the following data elements coded:
CHA2DS2-VASc Congestive Heart Failure CHA2DS2-VASc LV Dysfunction CHA2DS2-VASc Hypertension
Page 8 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
Numerator
Numerator algorithm
CHA2DS2-VASc Diabetes Mellitus CHA2DS2-VASc Stroke CHA2DS2-VASc TIA CHA2DS2-VASc Thromboembolic Event CHA2DS2-VASc Vascular Disease
Age (completion of ‘Date of Birth’)
Sex
Coding can be either “Yes” or “No” for inclusion. Null response for any of the above data elements will remove the patient from the numerator.
Denominator
Denominator
algorithm
All patients
Inclusion criteria All patients entered into the LAAO Registry
Exclusion criteria None
Page 9 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
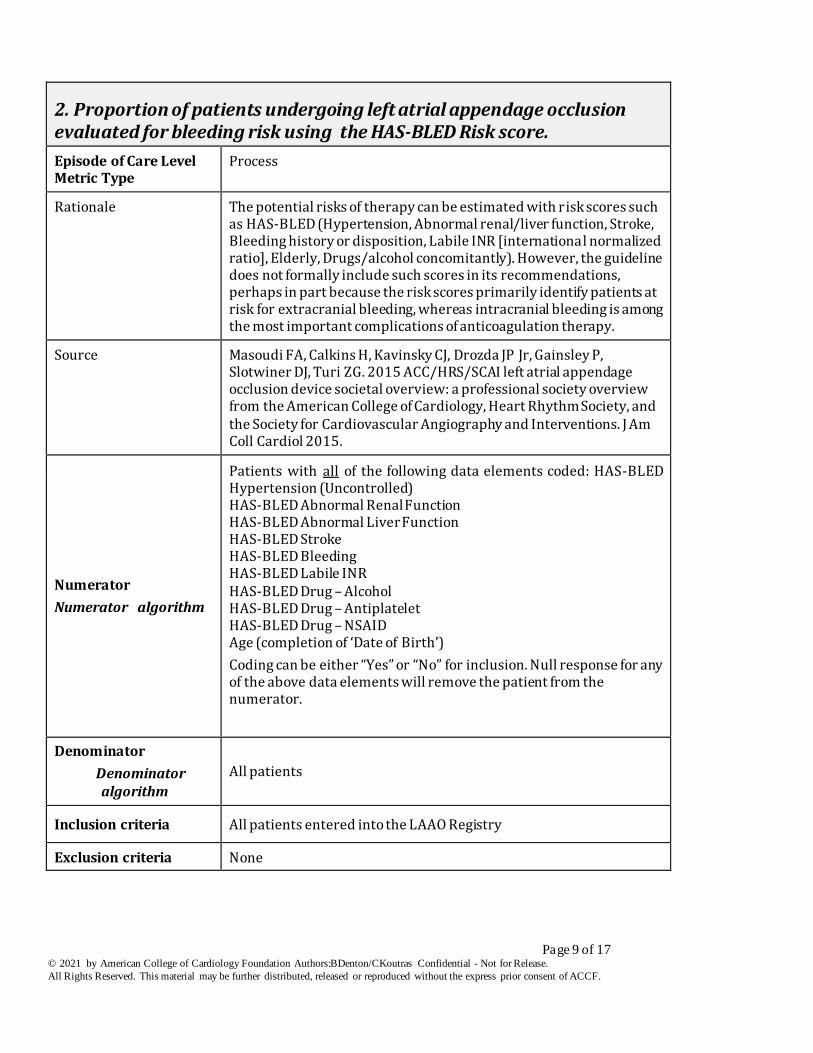
2. Proportion of patients undergoing left atrial appendage occlusion evaluated for bleeding risk using the HAS-BLED Risk score.
Episode of Care Level Metric Type
Process
Rationale The potential risks of therapy can be estimated with risk scores such as HAS-BLED (Hypertension, Abnormal renal/liver function, Stroke, Bleeding history or disposition, Labile INR [international normalized ratio], Elderly, Drugs/alcohol concomitantly). However, the guideline does not formally include such scores in its recommendations, perhaps in part because the risk scores primarily identify patients at risk for extracranial bleeding, whereas intracranial bleeding is among the most important complications of anticoagulation therapy.
Source Masoudi FA, Calkins H, Kavinsky CJ, Drozda JP Jr, Gainsley P, Slotwiner DJ, Turi ZG. 2015 ACC/HRS/SCAI left atrial appendage occlusion device societal overview: a professional society overview from the American College of Cardiology, Heart Rhythm Society, and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2015.
Numerator
Numerator algorithm
Patients with all of the following data elements coded: HAS-BLED Hypertension (Uncontrolled) HAS-BLED Abnormal Renal Function HAS-BLED Abnormal Liver Function HAS-BLED Stroke HAS-BLED Bleeding HAS-BLED Labile INR HAS-BLED Drug – Alcohol HAS-BLED Drug – Antiplatelet HAS-BLED Drug – NSAID Age (completion of ‘Date of Birth’)
Coding can be either “Yes” or “No” for inclusion. Null response for any of the above data elements will remove the patient from the numerator.
Denominator
Denominator algorithm
All patients
Inclusion criteria All patients entered into the LAAO Registry
Exclusion criteria None
Page 10 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
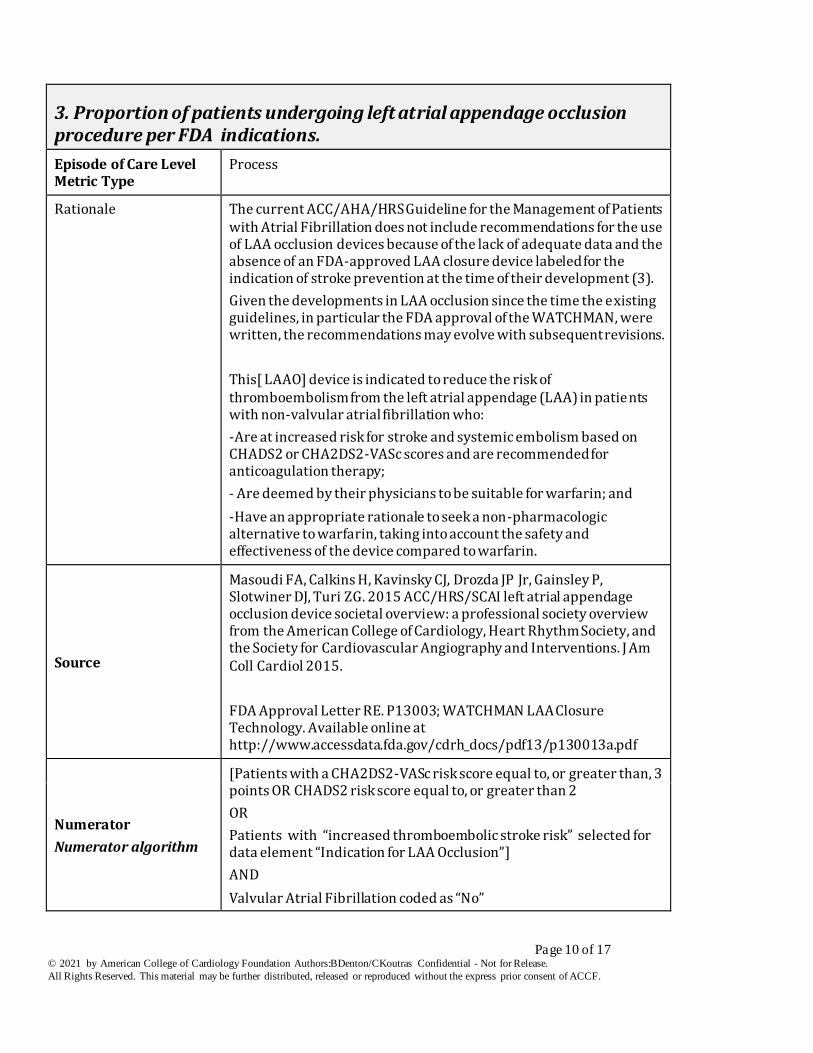
3. Proportion of patients undergoing left atrial appendage occlusion procedure per FDA indications.
Episode of Care Level Metric Type
Process
Rationale The current ACC/AHA/HRS Guideline for the Management of Patients with Atrial Fibrillation does not include recommendations for the use of LAA occlusion devices because of the lack of adequate data and the absence of an FDA-approved LAA closure device labeled for the indication of stroke prevention at the time of their development (3).
Given the developments in LAA occlusion since the time the existing guidelines, in particular the FDA approval of the WATCHMAN, were written, the recommendations may evolve with subsequent revisions.
This[ LAAO] device is indicated to reduce the risk of thromboembolism from the left atrial appendage (LAA) in patients with non-valvular atrial fibrillation who:
-Are at increased risk for stroke and systemic embolism based on CHADS2 or CHA2DS2-VASc scores and are recommended for anticoagulation therapy;
- Are deemed by their physicians to be suitable for warfarin; and
-Have an appropriate rationale to seek a non-pharmacologic alternative to warfarin, taking into account the safety and effectiveness of the device compared to warfarin.
Source
Masoudi FA, Calkins H, Kavinsky CJ, Drozda JP Jr, Gainsley P, Slotwiner DJ, Turi ZG. 2015 ACC/HRS/SCAI left atrial appendage occlusion device societal overview: a professional society overview from the American College of Cardiology, Heart Rhythm Society, and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2015.
FDA Approval Letter RE. P13003; WATCHMAN LAA Closure Technology. Available online at http://www.accessdata.fda.gov/cdrh_docs/pdf13/p130013a.pdf
Numerator
Numerator algorithm
[Patients with a CHA2DS2-VASc risk score equal to, or greater than, 3 points OR CHADS2 risk score equal to, or greater than 2
OR
Patients with “increased thromboembolic stroke risk” selected for data element “Indication for LAA Occlusion”]
AND
Valvular Atrial Fibrillation coded as “No”
Page 11 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
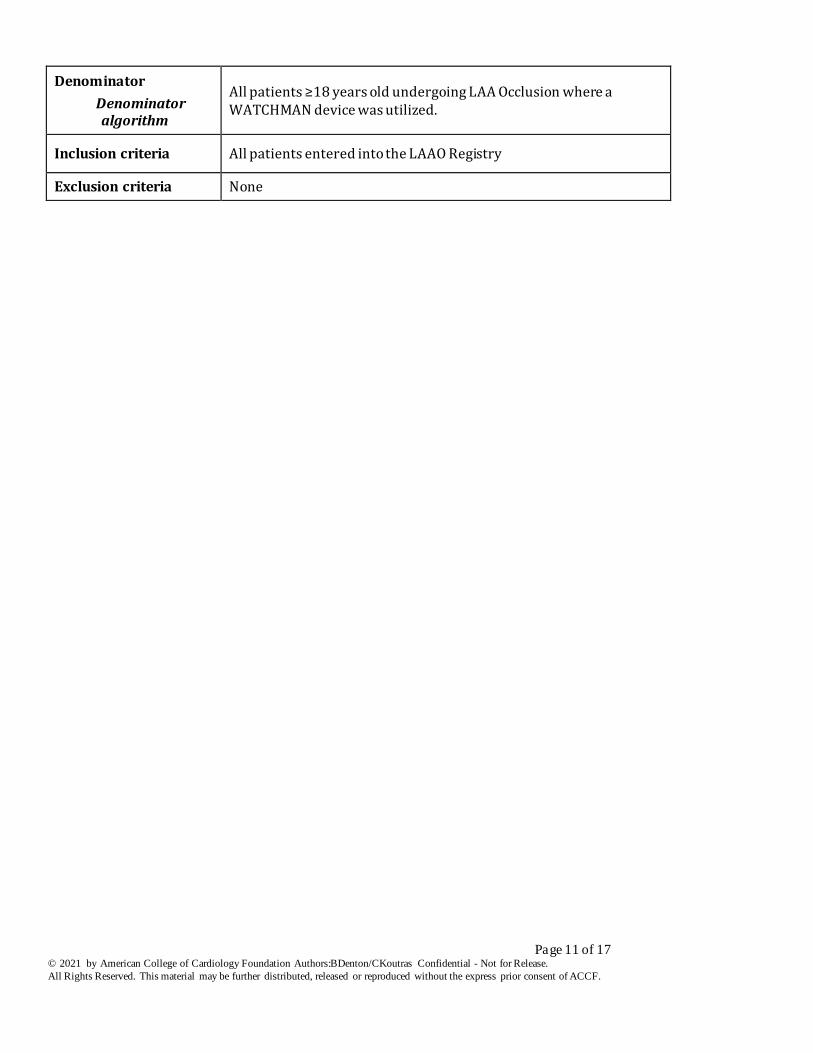
Denominator
Denominator algorithm
All patients ≥18 years old undergoing LAA Occlusion where a WATCHMAN device was utilized.
Inclusion criteria All patients entered into the LAAO Registry
Exclusion criteria None
Page 12 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
Outcome Metrics
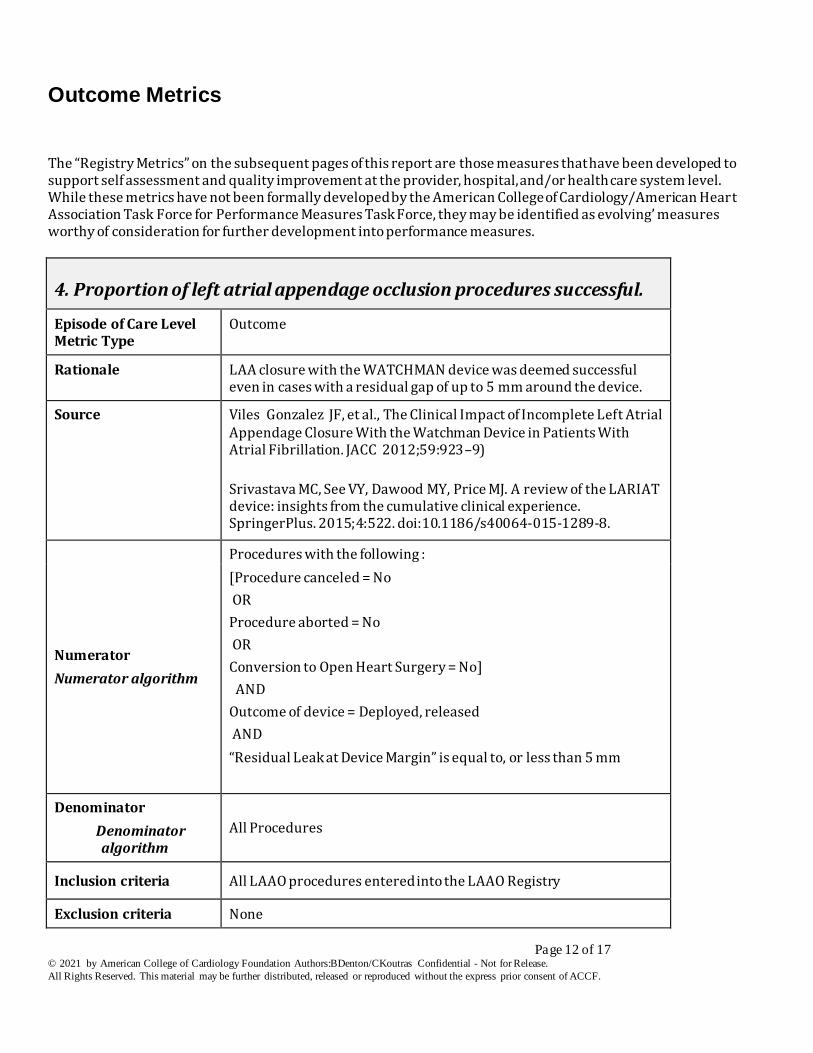
The “Registry Metrics” on the subsequent pages of this report are those measures that have been developed to support self assessment and quality improvement at the provider, hospital, and/or health care system level. While these metrics have not been formally developed by the American College of Cardiology/American Heart Association Task Force for Performance Measures Task Force, they may be identified as evolving’ measures worthy of consideration for further development into performance measures.
4. Proportion of left atrial appendage occlusion procedures successful.
Episode of Care Level Metric Type
Outcome
Rationale LAA closure with the WATCHMAN device was deemed successful even in cases with a residual gap of up to 5 mm around the device.
Source Viles Gonzalez JF, et al., The Clinical Impact of Incomplete Left Atrial Appendage Closure With the Watchman Device in Patients With Atrial Fibrillation. JACC 2012;59:923–9)
Srivastava MC, See VY, Dawood MY, Price MJ. A review of the LARIAT device: insights from the cumulative clinical experience. SpringerPlus. 2015;4:522. doi:10.1186/s40064-015-1289-8.
Numerator
Numerator algorithm
Procedures with the following :
[Procedure canceled = No
OR
Procedure aborted = No
OR
Conversion to Open Heart Surgery = No]
AND
Outcome of device = Deployed, released
AND
“Residual Leak at Device Margin” is equal to, or less than 5 mm
Denominator
Denominator algorithm
All Procedures
Inclusion criteria All LAAO procedures entered into the LAAO Registry
Exclusion criteria None
Page 13 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
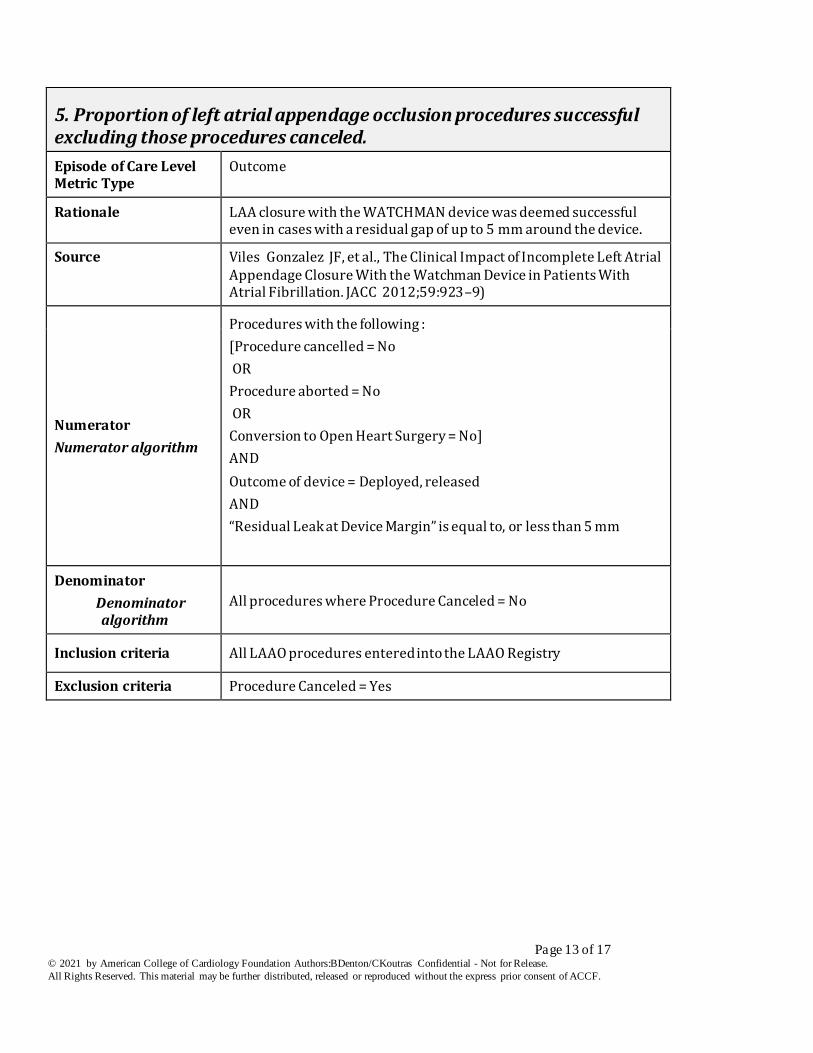
5. Proportion of left atrial appendage occlusion procedures successful excluding those procedures canceled.
Episode of Care Level Metric Type
Outcome
Rationale LAA closure with the WATCHMAN device was deemed successful even in cases with a residual gap of up to 5 mm around the device.
Source Viles Gonzalez JF, et al., The Clinical Impact of Incomplete Left Atrial Appendage Closure With the Watchman Device in Patients With Atrial Fibrillation. JACC 2012;59:923–9)
Numerator
Numerator algorithm
Procedures with the following :
[Procedure cancelled = No
OR
Procedure aborted = No
OR
Conversion to Open Heart Surgery = No]
AND
Outcome of device = Deployed, released
AND
“Residual Leak at Device Margin” is equal to, or less than 5 mm
Denominator
Denominator algorithm
All procedures where Procedure Canceled = No
Inclusion criteria All LAAO procedures entered into the LAAO Registry
Exclusion criteria Procedure Canceled = Yes
Page 14 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
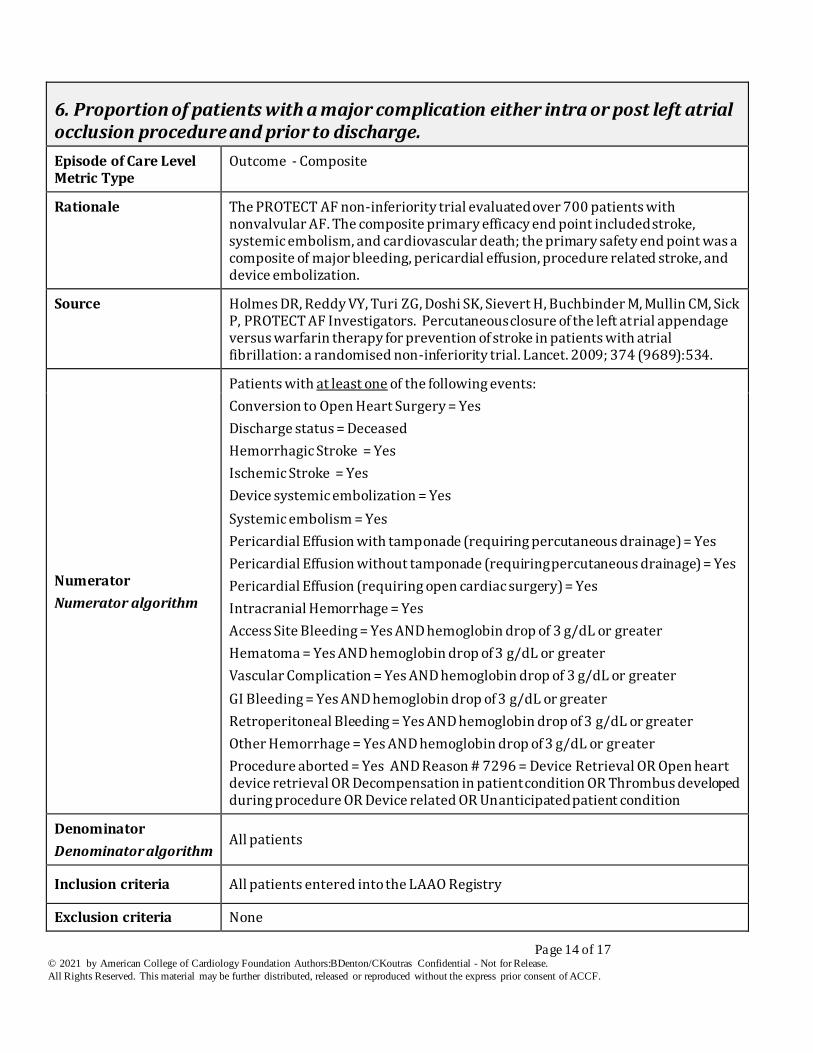
6. Proportion of patients with a major complication either intra or post left atrial occlusion procedure and prior to discharge.
Episode of Care Level Metric Type
Outcome - Composite
Rationale The PROTECT AF non-inferiority trial evaluated over 700 patients with nonvalvular AF. The composite primary efficacy end point included stroke, systemic embolism, and cardiovascular death; the primary safety end point was a composite of major bleeding, pericardial effusion, procedure related stroke, and device embolization.
Source Holmes DR, Reddy VY, Turi ZG, Doshi SK, Sievert H, Buchbinder M, Mullin CM, Sick P, PROTECT AF Investigators. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet. 2009; 374 (9689):534.
Numerator
Numerator algorithm
Patients with at least one of the following events:
Conversion to Open Heart Surgery = Yes
Discharge status = Deceased
Hemorrhagic Stroke = Yes
Ischemic Stroke = Yes
Device systemic embolization = Yes
Systemic embolism = Yes
Pericardial Effusion with tamponade (requiring percutaneous drainage) = Yes
Pericardial Effusion without tamponade (requiring percutaneous drainage) = Yes
Pericardial Effusion (requiring open cardiac surgery) = Yes
Intracranial Hemorrhage = Yes
Access Site Bleeding = Yes AND hemoglobin drop of 3 g/dL or greater
Hematoma = Yes AND hemoglobin drop of 3 g/dL or greater
Vascular Complication = Yes AND hemoglobin drop of 3 g/dL or greater
GI Bleeding = Yes AND hemoglobin drop of 3 g/dL or greater
Retroperitoneal Bleeding = Yes AND hemoglobin drop of 3 g/dL or greater
Other Hemorrhage = Yes AND hemoglobin drop of 3 g/dL or greater
Procedure aborted = Yes AND Reason # 7296 = Device Retrieval OR Open heart device retrieval OR Decompensation in patient condition OR Thrombus developed during procedure OR Device related OR Unanticipated patient condition
Denominator
Denominator algorithm All patients
Inclusion criteria All patients entered into the LAAO Registry
Exclusion criteria None
Page 15 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
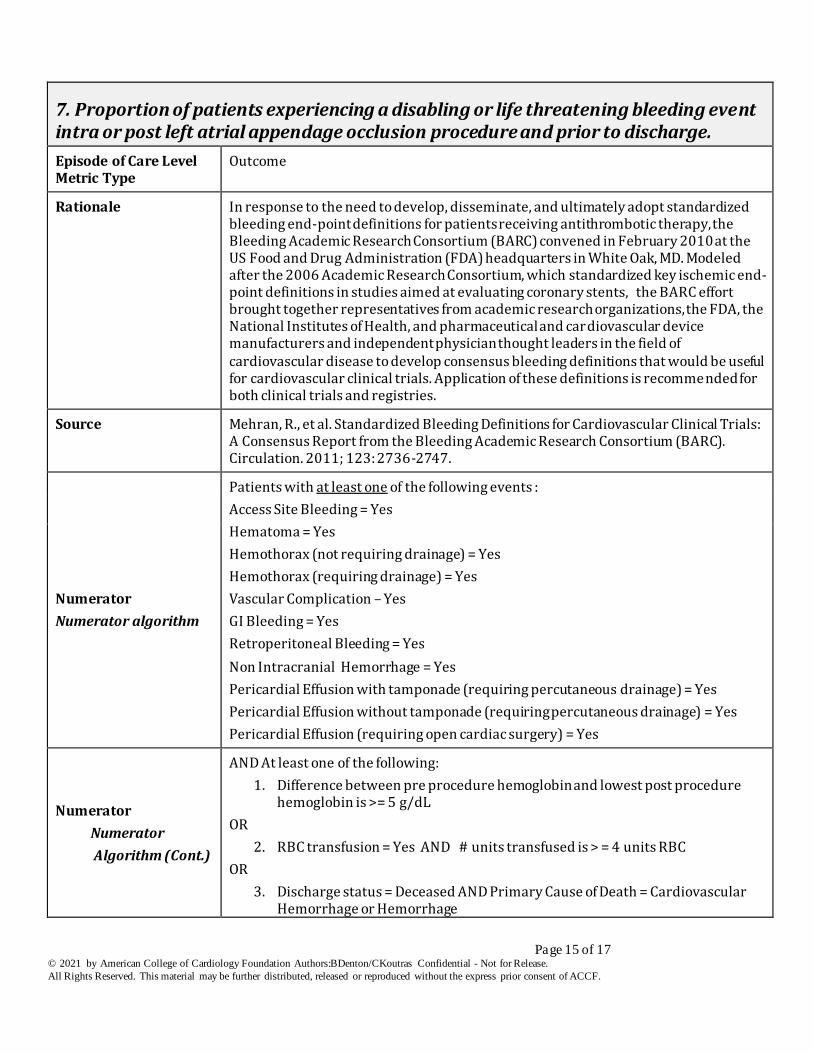
7. Proportion of patients experiencing a disabling or life threatening bleeding event intra or post left atrial appendage occlusion procedure and prior to discharge.
Episode of Care Level Metric Type
Outcome
Rationale In response to the need to develop, disseminate, and ultimately adopt standardized bleeding end-point definitions for patients receiving antithrombotic therapy, the Bleeding Academic Research Consortium (BARC) convened in February 2010 at the US Food and Drug Administration (FDA) headquarters in White Oak, MD. Modeled after the 2006 Academic Research Consortium, which standardized key ischemic end-point definitions in studies aimed at evaluating coronary stents, the BARC effort brought together representatives from academic research organizations, the FDA, the National Institutes of Health, and pharmaceutical and cardiovascular device manufacturers and independent physician thought leaders in the field of cardiovascular disease to develop consensus bleeding definitions that would be useful for cardiovascular clinical trials. Application of these definitions is recommended for both clinical trials and registries.
Source Mehran, R., et al. Standardized Bleeding Definitions for Cardiovascular Clinical Trials: A Consensus Report from the Bleeding Academic Research Consortium (BARC). Circulation. 2011; 123: 2736-2747.
Numerator
Numerator algorithm
Patients with at least one of the following events :
Access Site Bleeding = Yes
Hematoma = Yes
Hemothorax (not requiring drainage) = Yes
Hemothorax (requiring drainage) = Yes
Vascular Complication – Yes
GI Bleeding = Yes
Retroperitoneal Bleeding = Yes
Non Intracranial Hemorrhage = Yes
Pericardial Effusion with tamponade (requiring percutaneous drainage) = Yes
Pericardial Effusion without tamponade (requiring percutaneous drainage) = Yes
Pericardial Effusion (requiring open cardiac surgery) = Yes
Numerator
Numerator
Algorithm (Cont.)
AND At least one of the following:
1. Difference between pre procedure hemoglobin and lowest post procedure hemoglobin is >= 5 g/dL
OR
2. RBC transfusion = Yes AND # units transfused is > = 4 units RBC
OR
3. Discharge status = Deceased AND Primary Cause of Death = Cardiovascular Hemorrhage or Hemorrhage
Page 16 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
Denominator
Denominator algorithm
All patients
Inclusion criteria All patients entered into the LAAO Registry
Exclusion criteria None
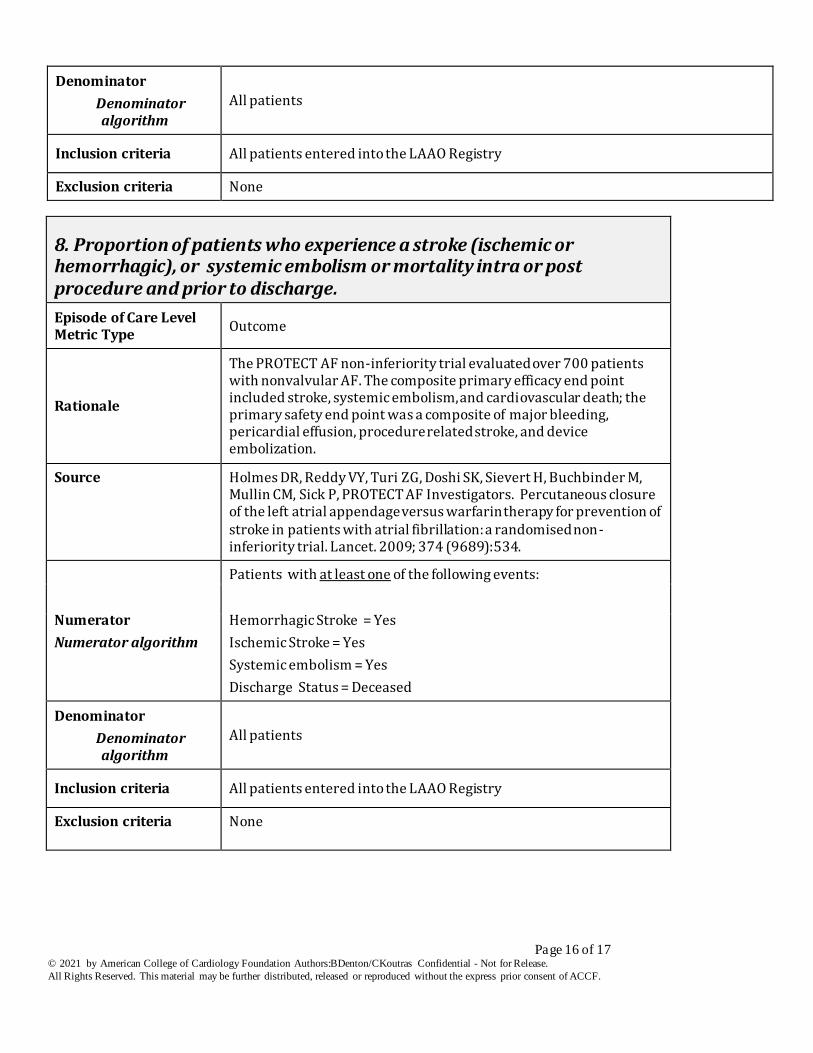
8. Proportion of patients who experience a stroke (ischemic or hemorrhagic), or systemic embolism or mortality intra or post procedure and prior to discharge.
Episode of Care Level Metric Type
Outcome
Rationale
The PROTECT AF non-inferiority trial evaluated over 700 patients with nonvalvular AF. The composite primary efficacy end point included stroke, systemic embolism, and cardiovascular death; the primary safety end point was a composite of major bleeding, pericardial effusion, procedure related stroke, and device embolization.
Source Holmes DR, Reddy VY, Turi ZG, Doshi SK, Sievert H, Buchbinder M, Mullin CM, Sick P, PROTECT AF Investigators. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet. 2009; 374 (9689):534.
Numerator
Numerator algorithm
Patients with at least one of the following events:
Hemorrhagic Stroke = Yes
Ischemic Stroke = Yes
Systemic embolism = Yes
Discharge Status = Deceased
Denominator
Denominator algorithm
All patients
Inclusion criteria All patients entered into the LAAO Registry
Exclusion criteria None
Page 17 of 17 © 2021 by American College of Cardiology Foundation Authors:BDenton/CKoutras Confidential - Not for Release. Last update 8/20/2020
All Rights Reserved. This material may be further distributed, released or reproduced without the express prior consent of ACCF.
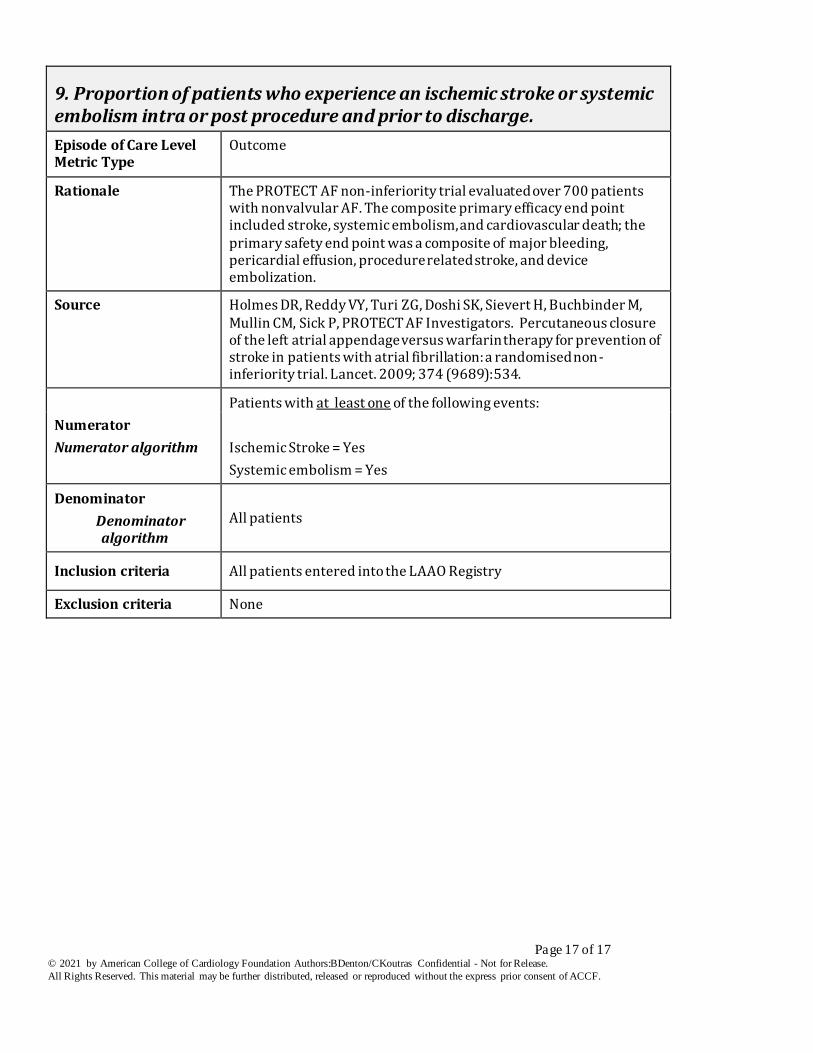
9. Proportion of patients who experience an ischemic stroke or systemic embolism intra or post procedure and prior to discharge.
Episode of Care Level Metric Type
Outcome
Rationale The PROTECT AF non-inferiority trial evaluated over 700 patients with nonvalvular AF. The composite primary efficacy end point included stroke, systemic embolism, and cardiovascular death; the primary safety end point was a composite of major bleeding, pericardial effusion, procedure related stroke, and device embolization.
Source Holmes DR, Reddy VY, Turi ZG, Doshi SK, Sievert H, Buchbinder M, Mullin CM, Sick P, PROTECT AF Investigators. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet. 2009; 374 (9689):534.
Numerator
Numerator algorithm
Patients with at least one of the following events:
Ischemic Stroke = Yes
Systemic embolism = Yes
Denominator
Denominator algorithm
All patients
Inclusion criteria All patients entered into the LAAO Registry
Exclusion criteria None