Embed Size (px)
Citation preview

Outline of presentation
1) Key messages
2) HFA
3) Thoughtful physicians: Difficult Questions
4) EBM
5) Measurement Iterative Loop
6) COPCORD / WHO / ILAR Studies
7) In conclusion ……

•Listen•Listen•Listen
listen & generate
hypothesescross examine to gather
data for hypothesis testingtest
hypothesesis one of the hypotheses
valid?
TAKE ACTION
The cyclic process of differential diagnosis
NO
YES

How do I select the appropriate diagnostic test?
1) Diagnostic tests RARELY reveal a patient’s true state with certainty.
2) Test selection should be restricted to those
diagnostic tests whose results could change
physician’s mind as to what should be done
for a patient.
3) Physicians often start treatment despite
uncertainty about true state of patient.

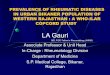
Number of diagnostic hypotheses remaining during
The steps of evaluating a symptom
0
5
10
15
c h ie f c o mp la in t h isto ry p h ysic a l e xa m te sts
Number of diagnoses to be considered
chief complaint
history
physical exam tests

Equal chance of occurring or not occurring
Certain not to occur
Probability of disease - 1
0 0.5 1.0
Certain to occur

Posterior Probability
Prior Probability
Probability of disease - 2
0 0.5 1.0

P[disease] = 0.06
Probability of disease - 3
0 0.5 1.0

EBM: Essential Steps & Flowchart1) Convert information needs into answerable
questions
2) Track down, with maximum efficiency, the best evidence with which to answer them (from the clinical examination, the diagnostic laboratory, the published literature, or other sources)
3) Critically appraise that evidence performance for its validity (closeness to the truth) & usefulness (clinical applicability)
4) Apply the results of this appraisal in clinical practice
5) Evaluate performance

Best Evidence
Clinical knowledge, experience,
skills, guts, flair
Patient Preferences
Fig : Flowchart of evidence-based medicine (adapted from Jenicek7)
Diagnosis, Therapy, Prognosis
Performance

Clinical aphorisms
1) If you hear hoofbeats, think of horses, not zebras
2) Rare manifestations of common diseases are
often more likely than common manifestations of rare diseases
3) If a test is unlikely to change the management of the patient, don’t do the test
4) If a test result surprises you, repeat the test
before taking action
5) The first priority in differential diagnosis is to
think about the diseases you can’t afford to miss

Outline of presentation
1) Key messages
2) HFA
3) Thoughtful physicians: Difficult Questions
4) EBM
5) Measurement Iterative Loop
6) COPCORD / WHO / ILAR Studies
7) In conclusion ……

Burden of Illness (Assessment)
Etiology or Causation
Community Effectiveness
Efficiency
Synthesis & Implementation
of Program
Monitoring & Reassessment
Policy Process
Measurement Iterative Loop
Diagnosis
Therapy
Prognosis

Relevance of population based studies
* Prevalence
* Incidence
* Risk factors
* Protective factors
* Knowledge, Attitude, Practice & Behavior

Relevance of population based studies - 1
Prevalence = No. of affected persons present in
the population at a specific time
--------------------------------------------- No. of persons in the
population at that time
Implication : - Useful measure of burden of disease - Age/gender prevalence- Valuable for planning health services & allocating resources (M)- Spectrum of disease seen (mild /moderate
/severe)

Relevance of population based studies - 2
Incidence : No. of new cases that occur during a specific period of time
-----------------------------------------population at risk of
developing the disease
Implication :
Helpful in exploring the relationship of an exposure & the risk of disease e.g. sore throat & RF Rheumatic fever –
“licks the joint and bites the heart”

Relevance of population based studies - 3
Risk factors :
Factors associated with occurrence ofdisease – most likely to be present
prior tothe onset of disease
Implication :
Risk factors – potential causal implications
eg. Hypertension & heart disease

Relevance of population based studies - 4
Protective factors :
Those which appear to have an inverse association with the presence or
developmentof disease
Implication :
For potential treatment or even prevention of
disorders eg. Low fat diet & atherosclerosis

Relevance of population based studies - 5
Knowledge, Attitude, Practice, & Behavior
(KAPB) Studies: Assess the knowledge,attitude, practice & behavior of a
particular disease in the population
Implication:
- Health behavior- Treatment seeking behavior- Compliance of treatment

Outline of presentation
1) Key messages
2) HFA
3) Thoughtful physicians: Difficult Questions
4) EBM
5) Measurement Iterative Loop
6) COPCORD / WHO / ILAR Studies
7) In conclusion ……

The Bhigwan (India) COPCORD Study: Publications
- The Bhigwan (India) COPCORD : Methodology & First Information ReportA Chopra, J Patil, V Billampelly, J Relwani, HS TandaleAPLAR Journal of Rheumatoloty, September 1997
- Prevalence of Rheumatic diseases in a Rural Population in Western India: A WHO-ILAR COPCORD Study
A Chopra, J Patil, V Billampelly, J Relwani, HS Tandale J Assoc Physicians India, February 2001
- Pain & disability, perceptions & beliefs of a Rural Indian Population : A WHO-ILAR COPCORD study
A Chopra, M Saluja, J Patil, HS Tandale The Journal of Rheumatology, 2002

The Bhigwan (India) COPCORD : Methodology & First Information
Report - 1
Study objective : Well stated
Study population : Characteristics well defined &
compared with national level (generalizability)
Study team : COPCORD team & good representation of local resources (manpower)
Study design : Cross-sectional community based study
Chopra et al. APLAR Journal of Rheumatology
September 1997

The Bhigwan (India) COPCORD : Methodology & First Information
Report - 2
Study instruments :
Standardized COPCORD questionnaires
- Questions translated to local language
- Validated on 50 referral patients (General population) Chopra et al. APLAR Journal of Rheumatology September 1997

The Bhigwan (India) COPCORD : Methodology & first information report
- 3
Survey teams : Trained Community Health Workers
COPCORD Medical Team : One rheumatologist, one
orthopedic surgeons, one rural doctor, two rheumatology research associates
Data collection :
- House to house daily visits- Daily operations were supervised - Due care was taken to look at the NON
respondents- Results well presented
Chopra et al. APLAR Journal of Rheumatology September 1997

Prevalence of Rheumatic diseases in a Rural Population in Western India: A WHO-ILAR COPCORD Study - 1
- Prevalence data from 1st rural Indian COPCORD survey in Bhigwan
- Cross-sectional survey : n = 6034
- Significant rural spectrum of rheumatic-musculoskeletal symptoms/diseases (RMSD)
Chopra et al. JAPI 2001

Prevalence of Rheumatic diseases in a Rural Population in Western India: A WHO-ILAR COPCORD Study - 2
Chopra et al. JAPI 2001
Conditions Prevalence Remarks Rheumatoid arthritis 0.5 %
(95% CI 0.3-0.7)Highest ever reported from an Asian Rural COPCORD study
Osteoarthritis 5.8% -Inflammatory arthritis 0.9% -Soft tissue rheumatism – general
3.2% -
Soft tissue rheumatism - regional
2.3 % -

Pain & disability, perceptions & beliefs of a Rural Indian Population :
A WHO-ILAR COPCORD study
- < 25% of patients perceive that they have severe problem which influences their work ability & personal life
- 21% did not perceive a need to see a doctor
Implications :
- Health seeking behavior - Treatment & Compliance- Cost & quality of life implications
Chopra et al. The Journal of Rheumatology 2002

Outline of presentation
1) Key messages
2) HFA
3) Thoughtful physicians: Difficult Questions
4) EBM
5) Measurement Iterative Loop
6) COPCORD / WHO / ILAR Studies
7) In conclusion ……

Burden of Illness (Assessment)
Etiology or Causation
Community Effectiveness
Efficiency
Synthesis & Implementation
of Program
Monitoring & Reassessment
Policy Process
Measurement Iterative Loop
Diagnosis
Therapy
Prognosis

RecoveryDeath
Incidence
Relationship between incidence & prevalence
Prevalence

In conclusion …..
1) Key messages
2) HFA
3) Thoughtful physicians: Difficult Questions
4) EBM
5) Measurement Iterative Loop
6) COPCORD / WHO / ILAR Studies
7) In conclusion ……

Inferior doctors treated the patient’s
disease,
Mediocre doctors treat the patient as a
person,
Superior doctors treat the community as a
whole.
- Huang Lee,
2600 BC