Embed Size (px)
Citation preview

CASE REPORT
Outpatient Treatment of Spontaneous PneumothoraxUsing an Improved Pocket Sized Heimlich Valve
K Y Chan, MRCSEd, M Fikri-Abdullah, FRCS, M Sa;;ad, FRCS, S M Adeeb, MS
Division of Cardiothoracic Surgery, Department of Surgery, Hbspital Universiti Kebangsaan Malaysia, Cheras, 56000,Kuala Lumpur
Introduction
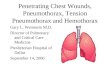
Pneumothorax is a common problem encounteredin medical practice. The conventional underwaterseal drainage system is technically cumbersome tomanage, and restricts patient ambulation. TheHeimlich valve, first introduced in 1968, has gainedwidespread acceptance. It was originally designedto allow emergency treatment of pneumothorax onthe battle front lines so that servicemen wouldsurvive to receive definitive care at the fieldhospital. The earlier devices had deficiencies. Theconnectors on each end are similar in the Heimlichflutter valve. Hence, it is dangerous if connected byan inexperienced person in the reverse manner.The Pneumostat™ (Atrium Medical Corporation,USA) is an improved device with· more safetyfeatures and a small chamber to collect pleural fluid(Fig. 1). It has a closed drainage system with an airleak detector added. It can be attached to any size
chest drain and be clipped to the patient's garment.The collected fluid in the chamber can be removedfrom the Leur port. We report the first two patientsin Malaysia who used this device at homesuccessfully in October 2002.
Case Report
Case IA sixty-year-old man with chronic obstructiveairway disease was admitted with an acuteshortness of breath for one day. There was norecent fever, trauma or chest pain. He had asimilar episode two years previously and a chestdrain was inserted for left sided pnuemothorax.Since then, he had stopped smoking. There wasno family history of asthma. Clinically, the patientwas tachypnoeic at rest, with reduced air entry onthe left side of the chest. On 4 Umin of oxygen via
This article was accepted: 15 April 2003Corresponding Author: Chan Kin Yoong, Department of Surgery, Hospital Universiti Kebangsaan Malaysia, Cheras, 56000 KualaLumpur
Med J Malaysia Vol 58 No 4 October 2003 597

CASE REPORT
nasal prong, arterial blood gas showed pH: 7.46;POz: 62mmHg; PCOz: 35.4mmHg; OzSat: 92.8%;HC03: 26.9mmollL. His chest X-ray showed leftpneumothorax with minimal pleural effusion. Achest drain was inserted into the left pleural spaceand bubbling of air noted in the underwater sealdrainage system. The .patient was treated withregular nebuliser, chest physiotherapy, and arepeated chest x-ray showed lung expansion.After chest tube removal, the patient redevelopedshortness of breath. The chest X-ray showedrecurrent pneumothorax with evidence of apicalbullae. The patient was planned for video-assistedthoracoscopic bullectomy and talc pleurodesis.After adequate pre-operative optimisation, thelung function test still showed severe lungimpairment with FEVl: 0.89L; FVC: 2.02L; ratio of44% and PEFR 3.1L /sec. A decision was thenmade for the patient to continue on chest drainageas surgery was deemed high risk. ThePneumostat" device was used to replaceconventional underwater seal drainage. Thisallowed the patient to ambulate. He wasdischarged a few days later with the device afterconfirmation of lung expansion. On follow-up atsecond week, the lung was fully expanded (Fig. 2)and the device was removed. The patient wassatisfied with the home use of the device and hewas well since then.
ease 2A 56-year-old woman, who is a known case ofpulmonary lymphangiomyomatosis, was admittedwith shortness of breath for one day. She was onthe waiting list for lung transplantation and haddeveloped recurrent pneumothoraces in the past,Clinically there was decreased air entry andhyperresonance on' her right side of the chest,' Thearterial blood gas showed pH: 7.3; POz: 55mmHG;PCOz: 42mmHg, OzSat: 86.4%; HC03: 21.2mmol/L,A chest X-ray confirmed a large, right sidedpneumothorax. A chest tube was inserted and anunderwater seal drainage was used. Followinginitial clinical improvement, the chest tube wasremoved. However, the pneumothorax recurredand this time Pneumostat" was used. She wassent home with the device on the next day. At theoutpatient clinic follow up, the chest tube wasremoved with chest X-ray showed no residualpneumothorax.
Discussion
The Pneumostat" device is designed forpneumothorax with the added feature of a 30mlchamber to collect pleural fluid. The fluid can beremoved repeatedly via the Leur port using asyringe without a needle. It has an internalmechanical one-way valve with a built-in vent.
Fig 1:
598
Size and position ofdevice in relation topatient
Fig 2: Chest X-ray at the beginning and two weeks'with the use of device
Med J Malaysia Vol 58 No 4 October

Outpatient Treatment of Spontaneous Pneumothorax Using an Improved Pocket Sized Heimlich Valve
Because air leaves the system through a vent, andnot the distal end, there is only one possible wayto attach the device to chest tube. The only accessto the device is through the Luer port. Therefore,the patient cannot place foreign objects into thedevice which can compromise device function.The device is latex free and does not have to betaped to patient's chest. It has a clip that can attachitself to patient's garment. The device moves freelyand remains in gravity dependent in variousposition adapted by the patient.
One of the main advantages of the Pneumonstat'is allowing early ambulation which can preventdeep vein thrombosis and pulmonary embolism.Immediately after connecting to the device, bothpatients were able to walk around in the ward.This allows early restoration of lung function,improved patient motivation and independence.Our patients clinically and radiologicallydemonstrated optimum drainage of pleural air andfluid. Both patients eventually requested for anearly discharge from hospital. The shorter hospital
stay can reduce patient's expenses and avoidnosocomial infection.
There are safety precautions for using the device athome. The doctor needs to recheck the drain andif necessary to re-stitch the drain with strong nonabsorbable suture before the patient goes homeAt home, regular wound inspection and redressingcan be done at a nearby clinic. The patient musthave easy access to the nearby hospital. In theevent that symptom of shortness of breath recurs,he should to go to the hospital.
Previous reports showed the Heimlich valve usewas beneficial in patients with penumocysticcarinii, cystic fibrosis and metastaticpneumothorax'<. Similar device was designed inthe past for post transthoracic-biopsypneumothorax. The Pneumostat" is a convenientand effective alternative to conventionalunderwater seal drainage. It allows many patientsto be treated successfully on an outpatient basis.
1. Driver AG, Peden JG, Adams HG et al. Heimlichvalve treatment of pneumocystis carinii associatedpneumothorax. Chest 1991; 100: 281-2.
2. Edenborough FP, Hussain I, Stableforth DE. Use ofa Heimlich flutter valve for pneumothorax in cysticfibrosis. Thorax 1994; 49: 117-9.
Med J Malaysia Vol 58 No 4 October 2003
3. Hengel PV, Bergh TH. Heimlich valve treatment andoutpatient management of bilateral metastaticpneumothorax. Chest 1994; 105: 1586-7.


![Dist-GAN: AnImproved GAN using Distance Constraints...Dist-GAN: AnImproved GAN using Distance Constraints Ngoc-Trung Tran[0000−0002−1308−9142], Tuan-Anh Bui[0000−0003−4123−262],](https://img.pdfslide.net/doc/110x75/60aad22afa8ec440d64b3f4c/dist-gan-animproved-gan-using-distance-constraints-dist-gan-animproved-gan.jpg)