Embed Size (px)
Citation preview

Ovarian Cancer: Standards of Care and New Opportunities
Robert L. Coleman, M.D.Professor & Vice Chair, Clinical Research
Department of Gynecologic OncologyM.D. Anderson Cancer Center

Ovarian Cancer: Liner Notes Globally 7th most incident and lethal cancer
– New cases: 225,000 annually
– Deaths: 140,000 annually
Burden of disease is greater in developed countries
The incidence increases with age
Almost 75% of cases present with advanced stage III / IV disease
Risk of relapse of advanced stage disease is as high as 70%
CA Cancer, 2013
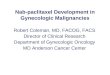
Ovarian Cancer: Natural History
Symptoms
Diagnosis
Chemotherapy #1
Staging
Evaluation? SLL
Progression
Chemo #2 Chemo #3+
SupportiveCare
Death
SecondarySurgery
Maintenance
Duration
Progression-Free Survival(12-28 mos)
Post Progression Survival(12-38 mos)

Surgical Management of Primary Ovarian Cancer
Theoretical: – Reduced the volume of hypoxic,
poorly perfused cells– Host immunocompetence is
improved with lower tumor burden– Recruitment of residual cells into G1
potentiating the effects of cytotoxic therapy
– Removal of chemoresistant clones
Practical:– “Biology vs Brawn”

0%
25%
50%
75%
100%
0 12 24 36 48 60 72 84 96 108 120 132 144
% P
rogr
essi
on-f
ree
Surv
ival
0 mm
1-10 mm
> 10 mm
HR (95%CI)
1-10 mm vs. 0 mm: 2.52 (2.26;2.81)
>10 mm vs. 1-10 mm: 1.36 (1.24;1.50)
log-rank: p < 0.0001
0%
25%
50%
75%
100%
0 12 24 36 48 60 72 84 96 108 120 132 144
% O
vera
ll Su
rviv
al
0 mm
1-10 mm
> 10 mm
HR (95%CI)
1-10 mm vs. 0 mm: 2.70 (2.37; 3.07)
>10 mm vs. 1-10 mm: 1.34 (1.21; 1.49)
log-rank: p < 0.0001
The Impact of Residual Tumor: What Is Optimal Debulking?
Generated from 3 prospective Phase III trials (OVAR 3,5, & 7)
N = 3126 pts
DuBois, Cancer (2009)115:1234

Primary Approach: What’s Best?
N Engl J Med (2010) 363:943
(years)
0 1 2 3 4 5 6 7 8
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment320 360 168 60 39 26 17 7 2
320 357 177 60 36 20 13 3 1
Upfront debulking surgery
Neoadjuvant chemotherapy
Progression-free survival
PDS: 12 mosNACT: 12 mosHR: 0.99 (0.87-1.13)
(years)
0 2 4 6 8 10
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment259 361 183 68 16 2
251 357 191 56 11 1
Upfront debulking surgery
Neoadjuvant chemotherapy
Overall survival
PDS: 29 monthsIDS: 30 monthsHR: 0.98 (0.85, 1.14)
PFS
OS

Neoadjuvant Chemotherapy in Ovarian Cancer
9/21/10 1/20/11

Primary Approach: What’s Best?
N Engl J Med (2010) 363:943
(years)
0 1 2 3 4 5 6 7 8
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment320 360 168 60 39 26 17 7 2
320 357 177 60 36 20 13 3 1
Upfront debulking surgery
Neoadjuvant chemotherapy
Progression-free survival
PDS: 12 mosNACT: 12 mosHR: 0.99 (0.87-1.13)
(years)
0 2 4 6 8 10
0
10
20
30
40
50
60
70
80
90
100
O N Number of patients at risk : Treatment259 361 183 68 16 2
251 357 191 56 11 1
Upfront debulking surgery
Neoadjuvant chemotherapy
Overall survival
PDS: 29 monthsIDS: 30 monthsHR: 0.98 (0.85, 1.14)
PFS
OS

CHORUSChemotherapy Or Upfront Surgery
RCOG
ICON-8
OV.21
Neoadjuvant Chemotherapy X 3-4 courses
Randomized
IV-Arm IP-ArmPac/Carbo + Pac/Carbo (IP) +
Pac (d8) Pac (IP, d8)
Pre-randomization Strata for NACT or PDS
Randomized
StandardPac/Carbo
Exp ADD-Pac/Carbo
Exp BDD - Pac/DD-Carbo

Principle Approach: Iº Therapy
Chemotherapy
GOG-111
Cisplatin 75 mg/m2
Cytoxan 750mg/m2
Cisplatin 75 mg/m2
Paclitaxel 135 mg/m2
GOG-158
Cisplatin 75 mg/m2
Paclitaxel 135 mg/m2
Carboplatin AUC 7.5
Paclitaxel 175 mg/m2
GOG-172
Cisplatin 75 mg/m2
Paclitaxel 135 mg/m2
Day1: IV Paclitaxel 135 mg/m2
Day 2: IP Cisplatin 100mg/m2
Day 8: IP Paclitaxel 60 mg/m2
McGuire New Engl J Med (1996) 334:1Ozols, J Clin Oncol (2003) 21:3194Armstrong New Engl J Med (2006) 354:34
OS
Cytoxan/Cisplatin
- - - Paclitaxel/Cisplatin
PFS

International Phase III Experience
CP CPG CPPLD CTCP CGCP PLD-C CE Total
GOG0182-ICON5 864 864 862 861 861 4312
SCOTROC 538 539 1077
AGO-GINECO 635 647 1282
NSGO-EORTC-NCIC-GEICO 444 443 887
MITO 170 156 326
AGO-GINECO-GERCOR-NSGO 882 860 1742
NCIC-EORTC-GEICO OV16 410 409 819
MITO-2 410 410 820
Regimen Total: 4353 1724 1272 1426 861 539 1090 11265
No Significant Effect
More ≠ BetterDifferent ≠ Better

Moving The Bar: Primary Therapy
Dose-dense therapy
IP Chemotherapy
Biologics: Anti-angiogenesis, PARPi,
angiopoeitin inhibitors
Establishing a Front-Line Adjuvant Standard

Dose Dense: Weekly Therapy
Ovarian Epithelial, PP, FTFIGO Stage II-IV
Paclitaxel 180mg/m2
Carboplatin AUC 6.0 q 21 days (6-9 cycles)
Dose density: 60 mg/m2/wk
Paclitaxel 80mg/m2, days 1, 8, 15 Carboplatin AUC 6.0, day 1
q 21 days (6-9 cycles)Dose density: 80 mg/m2/wk (+33%)
Stratification; Residual disease: <1cm, > 1cmFIGO Stage : II vs. III vs. IVHistology : clear cell/mucinous vs serous/others
R
Katsumata, Lancet 2009

JGOG 3016: Long-Term Follow-Up
Katsumata N, ASCO Abstract 5003, 2012

iPocc JGOG Trial: SchemaEpithelial Ovarian Cancer
Stages II-IVIncluding Bulky Tumor
Paclitaxel 80 mg/m2 IV Day 1,8,15Carboplatin AUC 6 IV
Q21, 6-8 Cycles
Paclitaxel 80 mg/m2 IV Day 1,8,15Carboplatin AUC 6 IP
Q21, 6-8 Cycles
Primary Endpoint: PFS Secondary Endpoint: OS, Toxicity, QOLAccrual Goal: 746 pts / 511 events
Dose dense−TCipDose dense−TCiv
RANDOMIZATION

GOG-0218 study schema
Previously untreated epithelial ovarian, primary peritoneal, or
fallopian tube cancer
• Stage III optimal (macroscopic)
• Stage III suboptimal• Stage IV
n=1873
Stratification variables:• GOG performance status• Stage/debulking status
RANDOMIZ E
1:1:1
15 months
Paclitaxel 175 mg/m2
Carboplatin AUC 6
Placebo
IArm
Cytotoxic (6 cycles)
Maintenance(16 cycles)
(CP + PLA → PLA)
Carboplatin AUC 6
Paclitaxel 175 mg/m2
PlaceboBevacizumab15 mg/kg
II(CP + BEV→ PLA)
Bevacizumab 15 mg/kg
Carboplatin AUC 6
Paclitaxel 175 mg/m2 III(CP + BEV
BEV)
Burger et al. N Engl J Med 2011;365:2473-83
Establishing a Front-Line Adjuvant Standard

Stratification variables:• Stage & extent of debulking: I–III debulked
≤1cm vs stage I–III debulked >1 cm vs stage IV and inoperable stage III
• Timing of intended treatment start≤4 vs >4 weeks after surgery
• GCIG group
Schema
Academic-led, industry-supported trial to investigate use of bevacizumab and to support licensing
Paclitaxel 175 mg/m2
Carboplatin AUC 5/6
Carboplatin AUC 5/6
Paclitaxel 175 mg/m2
18 cycles
Rn=1528*
Bevacizumab 7.5 mg/kg q3w
1:1
*Dec 2006 to Feb 2009
Establishing a Front-Line Adjuvant Standard
Perrin, N Engl J Med 2011;365:2484-96

Anti-VEGF Targeting: FrontlinePFS
Perren, NEJM (2011) 365:2484Burger, NEJM (2011) 365:2473
HR: 0.7310.4 vs 13.9 mosMedian D: 3.5 mos
HR: 0.8717.4vs 19.8 mosMedian D: 2.4 mos
GOG 218 ICON7

Anti-VEGF Targeting: FrontlineOverall Survival
Perren, NEJM (2011) 365:2484Burger, NEJM (2011) 365:2473
GOG 218 ICON7

00.10.20.30.40.50.60.70.80.91.0
0 6 12 18 24 30 36
02468
101214161820
0 6 12 18 24 30 36
-15
-10
-5
0
5
10
15
20
25
30
0 6 12 18 24 30 36
0.00.10.20.30.40.50.60.70.80.91.0
0 6 12 18 24 30 36
14 vs 173 months’ difference
13.3 vs 16.5 3 months’ difference
Time (months) Time (months)
GOG-0218 ICON7 (III suboptimal and IV subgroup)
GOG-0218 and ICON7: Restricted Means Estimate – Benefit During Exposure Only?
Research Arm Research Arm
Research Arm Research Arm

GOG Ovarian Strategy: 262
262Suboptimal
(> 1 cm Residual)Neoadjuvant allowed
CT Perfusion Scan
IV Paclitaxel 80 mg/m2 weeklyIV Carboplatin AUC 6 q 3 wkIV Bevacizumab 15 mg/kg (optional)
IV Paclitaxel 175 mg/m2
IV Carboplatin AUC 6IV Bevacizumab 15 mg/kg (optional)
Bevacizumab q 3 wk(If chosen)
Maintenance to Progression
N: 702/625 (OPEN only for ACRIN ComponentPrimary endpoint: PFS

Phase III GOG 252 Schema
IV Paclitaxel 80 mg/m2 days 1, 8, 15IV Carboplatin AUC 6 day 1
Bevacizumab 15 mg/kg q3w†
IV Paclitaxel 80 mg/m2 days 1, 8, 15IP Carboplatin AUC 6 day 1
Bevacizumab 15 mg/kg q3w†
IV Paclitaxel 135 mg/m2 day 1 IP Cisplatin 75 mg/m2 day 2IP Paclitaxel 60 mg/m2 day 8Bevacizumab 15 mg/kg q3w†
RAN
DO
MIZ
ATIO
NN
= 1
250
Walker JL. Am Soc Clin Oncol Ed Book. 2009:308-312.
N: 1554 (CLOSED)Primary endpoint: PFS
Cycles 1-6* Cycles 7-22*
Bevacizumab 15 mg/kg q3w
*Each cycle is 3 weeks; †Begin cycle 2.
Bevacizumab 15 mg/kg q3w
Bevacizumab 15 mg/kg q3w

Other Pursuits in Front-Line Therapy
VEGF TKI’s
– Nintedanib (BIBF1120)
PARPi
– Veliparib (OVM1102)
Angiopoeitin inhibitors
– TRINOVA-3: Trebananib (AMG-386)

Bottom Line…
Determine good candidates for surgery
– Potential for better selection tools, e.g. Laparoscopy
Optimal radical resection
– Goal: R0
Adjuvant therapy
– IP and dose dense are my favorite options
– Good place for clinical trial

Maintenance: The Stakes are High!
Symptoms
Diagnosis
Chemotherapy #1
Staging
Evaluation? SLL
Progression
Chemo #2 Chemo #3+
SupportiveCare
Death
SecondarySurgery
Maintenance
What we know…• Rate of response is high (CR + PR) >75%• Second assessment operations find disease > 40% of CR’s• Clinical CR’s have >50% recurrence risk at 2 years• Pathological CR’s have >40% risk at 2 years• Option applies to CR’s and documented PR’s

Maintenance Therapy ScorecardMaintenance Beneficial?
Strategy No YesProlonged Initial Therapy ✓
Short Duration / Non-Cross Resistant Chemotherapy ✓
High-Dose Chemotherapy ✓
Intraperitoneal ✓
Interferon- ✓
Anti-CA-125 Ab ✓
Biologic Agent (MMPI, bevacizumab*) ✓ ✓*
Paclitaxel (6 months) ✓Paclitaxel (1 year) ✓#
Erlotinib ✓

Maintenance Trials: Ongoing
Bevacizumab (GOG 252, 262)
Pazopanib (OVAR-16)
Nintedanib (BIBF 1120)
Trebananib (TRINOVA-3)
CVAC: Muc-1 Dendritic Cell vaccine
PARPi,
pvKLH + OPT-821 [GOG-255] (II° maintenance)
FAKi (GSK2256098) – GOG concept approved 8/11
EOC, PP, FT cancer
PaclitaxelX 12 mos
CTI-2103X 12 mos
No Treatment
PaclitaxelCarboplatin
GOG-212
N = 1100 patientsSurvival primary endpoints
QOL endpoints 28

Bottom Line…
Experimental but evidence of PFS impact has been demonstrated
I always have the conversation (longest of any counseling session) but it is only infrequently taken by the patient

Recurrent Therapy: Ovarian Cancer
Symptoms
Diagnosis
Chemotherapy #1
Staging
Evaluation? SLL
Progression
Chemo #2 Chemo #3+
SupportiveCare
Death
Maintenance
SecondarySurgery
What we know (Recurrence): • Nearly all patients will succumb to progression• Options are plentiful • Nothing a “homerun”

Treatment Free Interval: Traditional Model
Time from last platinum exposure (TFI)
TreatmentCompletion 6 mos
Platinum Resistant/Refractory Platinum Sensitive
Non-Platinum Treatment Platinum Retreatment

Treatment-Free Interval and Survival
Lauraine, Proc ASCO #829, 2002
0-3 Prog 0-3 Non PD 3-12 mos 12-18 mos 18+ mos
PFS (days) 90 176 174 275 339
OS (days) 217 375 375 657 957
Response (%) 9 24 35 52 62
Day
s1000
900
800
700
600
500
400
300
200
100
Percen
tage
100
90
80
70
60
50
40
30
20
10

Control Experimental N TTP (wks) P OS (wks) P Comment
Paclitaxel Topotecan 226 14 vs 23 NS 43 vs 61 NS 50% Cross-over
Paclitaxel (bolus)
Paclitaxel (weekly)
208 38 vs 26 NS 34 vs 59 NS Less toxicity w/ weekly
Paclitaxel Oxaliplatin 86 14 vs 12 NS 37 vs 42 NS 74% platinum resistant
Topotecan PLD 481 17 vs 16 NS 57 vs 60 NS 54% resistant; OS benefit in sensitive
Paclitaxel PLD 214 22 vs 22 NS 56 vs 46 NS All pts taxane-naïve
Topotecan Treosulfan 357 22 vs 12 0.001 56 vs 48 0.02 2nd – 3rd line therapy
PLD Gemcitabine 195 16 vs 13 NS 59 vs 55 NS
PLD Gemcitabine 153 16 vs 20 NS 55 vs 50 NSresistant
56% platinum resistant
PLD or Topotecan
Canfosfamide 461 19 vs 9 <0.01 59 vs 37 (PLD:62 vs Topo:47)
<0.0001 ASSIST-1 trialAll 3rd line
PLD Patupilone 802 16 vs 16 NS 55 vs 57 NS RR: 8% vs 18% (patupilone)
Summary of Phase III Single Agent Trials: Resistant Ovarian Cancer

Control Experimental N TTP (wks) P OS (wks)
P Comment
PLDPLD +
Trabectedin228 16 vs 17.4 NS N/A N/A RR: 16 vs 23%
Chemo(Paclitaxel weekly,
Gemcitabine, Topotecan)
Chemo + Bevacizumab 361 14.8 vs 29.1 <0.001 N/A N/A
RR: 12% vs 27%(RECIST)
Summary of Phase III Combination Trials: PR
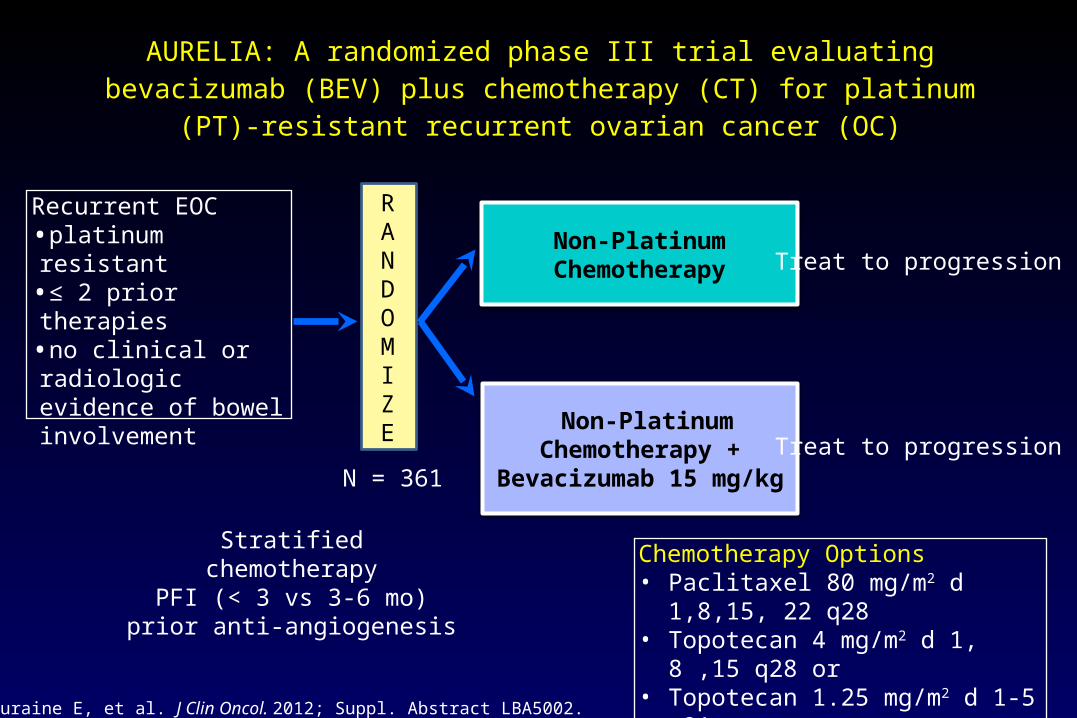
AURELIA: A randomized phase III trial evaluating bevacizumab (BEV) plus chemotherapy (CT) for platinum (PT)-resistant recurrent ovarian
cancer (OC)
Recurrent EOC•platinum resistant•≤ 2 prior therapies•no clinical or radiologic evidence of bowel involvement
Non-Platinum Chemotherapy
RANDOMIZE Non-Platinum Chemotherapy
+ Bevacizumab 15 mg/kg
Chemotherapy Options• Paclitaxel 80 mg/m2 d 1,8,15, 22 q28• Topotecan 4 mg/m2 d 1, 8 ,15 q28 or • Topotecan 1.25 mg/m2 d 1-5 q21• PLD 40 mg/m2 d 1 q28
Stratifiedchemotherapy
PFI (< 3 vs 3-6 mo)prior anti-angiogenesis
Treat to progression
Treat to progressionN = 361
Pujade-Lauraine E, et al. J Clin Oncol. 2012; Suppl. Abstract LBA5002.
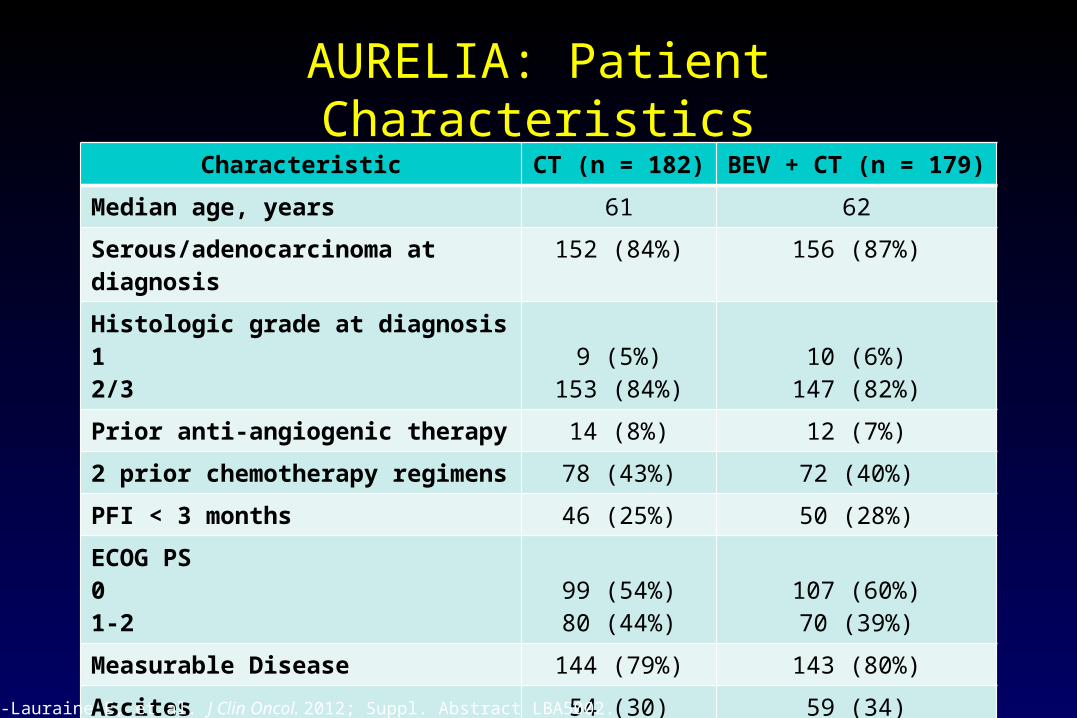
AURELIA: Patient CharacteristicsCharacteristic CT (n = 182) BEV + CT (n = 179)
Median age, years 61 62
Serous/adenocarcinoma at diagnosis 152 (84%) 156 (87%)Histologic grade at diagnosis12/3
9 (5%)153 (84%)
10 (6%)147 (82%)
Prior anti-angiogenic therapy 14 (8%) 12 (7%)2 prior chemotherapy regimens 78 (43%) 72 (40%)PFI < 3 months 46 (25%) 50 (28%)ECOG PS01-2
99 (54%)80 (44%)
107 (60%)70 (39%)
Measurable Disease 144 (79%) 143 (80%)Ascites 54 (30) 59 (34)
Pujade-Lauraine E, et al. J Clin Oncol. 2012; Suppl. Abstract LBA5002.

AURELIA Progression-Free Survival
1.0
0.8
0.6
0.4
0.2
0.0
6 12
Time (months)
Est
imat
ed
Pro
babi
lity
18 3024
182 93 37 8 1 1 0 020179 140 88 18 4 1 149
0
BEV + CT
CTNumber at risk
Events, n (%)
Median PFS, months
(95% CI)
166 (91%)
3.4
(2.2-3.7)
135 (75%)
CT(n = 182)
BEV + C T(n = 179)
6.7
(5.7-7.9)
HR (unadjusted)
(95% CI)
Log-rnak P-value(2-sided, unadjusted)
0.48
(0.38-0.60)
< 0.001
3.4 6.7
Pujade-Lauraine E, et al. J Clin Oncol. 2012; Suppl. Abstract LBA5002.

Subgroup analysis of PFS
aUnadjusted. bMissing n=8
Subgroup No. of patients
Median PFS, months
HRaBEV + CT
betterCT
better CT BEV + CT
All patients 361 3.4 6.7 0.48
Age, years <65 ≥65
228133
3.43.5
6.07.8
0.490.47
PFI, monthsb <3
3‒6
96
257
2.1
3.6
5.4
7.8
0.53
0.46
Measurable disease, cm
No (<1)
Yes (1‒<5)
Yes (≥5)
74
126
161
3.7
3.3
3.3
7.5
7.5
6.0
0.46
0.50
0.47
Ascites Yes
No
113
248
2.5
3.5
5.6
7.6
0.40
0.48
Chemotherapy Paclitaxel
PLD
Topotecan
115
126
120
3.9
3.5
2.1
10.4
5.4
5.8
0.46
0.57
0.32
0.2 0.3 0.5 1 2 3 4 5

Summary of best overall response rates
Responders (RECIST and/or CA-125) (n=350)
RECIST responders (n=287) CA-125 responders (n=297)05
101520253035404550
12.6 11.8 11.6
30.927.3
31.8
CT BEV + CT
aTwo-sided chi-square test with Schouten correction
p=0.001ap<0.001a p<0.001a
Patie
nts
(%)

AURELIA: Conclusions No alarming safety signals
– PLD – HFS, paclitaxel – neuropathy, all: myelosuppression) Toxicity may relate to exposure (longer on experimental arms) Bevacizumab augments outcomes (response, PFS) of standard
chemotherapy Paclitaxel may benefit to greater degree Await OS data CAVEATS
– Not placebo-controlled– Pretreatment characteristics: 80% measurable, 30% ascites, 8% prior AA
therapy– Each arm is equivalent to RP2

Bottom Line…
For platinum-resistant disease, I like:
– Weekly paclitaxel ± bevacizumab
– PLD
– Gemcitabine + cisplatin (q 2 wk infusion)
Try HARD to get onto clinical trial
– Lots of options with interesting new agents

NCCN Guidelines Version 2013Therapy for Relapse > 6 months
NCCN Clinical Practice Guidelines in Oncology. Ovarian Cancer v.1.2013. Available at: http://www.nccn.org

DESKTOP-I: Surgical Endpoint of Surgery at Relapse
no residualsmedian OS 45.2 mo
residuals > 10 mm
residuals 1-10 mm
Surv
ival
pro
babi
lity
0
1.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
0 12 24 36 48
Months from Randomization

Secondary Cytoreduction: Multivariate Analysis Who Benefits?
Tay, Obstet Gynecol 99:1008, 2002

Secondary Cytoreductive Surgery
Chi DS, et al. Cancer. 2006;106(9):1933-1939.
DFI = disease-free interval; mos = months; SC = secondary cytoreduction.
DFI Single Site Multiple Sites: No Carcinomatosis Carcinomatosis
6-12 mos Suggest SC Offer SC No SC
12-30 mos Suggest SC Suggest SC Offer SC
> 30 mos Suggest SC Suggest SC Suggest SC
Goal of surgery: No gross residual disease

AGO-OVAR DESKTOP III (Protocol AGO - OVAR OP.4)
EOC, FT, PP• PFI > 6•No prior recurrence
chemotherapy•Complete resection
seems feasible and positive AGO score:
• PS ECOG 0• No ascites > 500 ml• Prior complete
debulking or initial FIGO I/II
Secondary Cytoreduction
Chemo
Regimens post-randomization• Carboplatin/paclitaxel• Carboplatin/gemcitabine• Carboplatin/PLD
No surgery
R
N = 150/408 planned

PI: Coleman
Recurrent Ovarian, PPT and FT CancerTFI ≥ 6 mos
Yes No
Randomize
Surgery No Surgery CarboplatinPaclitaxel or Gemcitabine
CarboplatinPac or Gem
Bevacizumab
Bevacizumab
GOG-213
To Chemotherapy Randomization
Randomize
Surgical Candidate?

A randomized trial evaluating cytoreductive surgery in patients with platinum-sensitive recurrent ovarian cancer
RANDOMIZE
Cytoreductivesurgery
Platinum-basedchemotherapy*
Primary outcome: OSSecondary outcome: PFS, QoL, Complications
No surgery
SOC I Shanghai Gynecologic Oncology Group
Available at: http://www.clinicaltrials.gov/ct2/show/NCT01611766 Accessed March 04, 2013.
N=420Platinum-sensitive, first relapserecurrent cancer of the
ovaries, fallopian tubes, orperitoneum
PFI > 6 mosNo prior chemotherapy
for this 1st relapse
Complete secondary cytoreduction predicting score (iMODEL)• FIGO stage• Residual disease after primary
surgery • PFI• PS ECOG• CA125• Ascites at recurrence

Outcomes in Recurrent Ovarian Cancer: PS
Trial Treatment RR (%) PFS (mo) HR OS (mo) HR
ICON 4 (n = 802) C 54 9
0.76 P < 0.001
240.82
P = 0.02C + P 66 12 29
AGO(n = 366) C 31 5.8
0.72P = 0.003
17.30.96
P = 0.73GC 47 8.6 18
OVA-301(n = 417)
PLD ? 7.5 0.73P=0.017
24.1 0.83P = 0.11PLD + Trab ? 9.2 27.0
CALYPSO (n = 976) C + P – 9.4
0.82 P = 0.005
33.00.99
P = 0.94C + PLD – 11.3 30.7
OCEANS (n = 484)
GC + PL 57 8.4 0.48 P < 0.0001
35.2* 1.03*
P = 0.84GC + BV 79 12.4 33.3
*Data still maturing.
Take home messages:• PFS appears to be impacted from combination therapy• No OS effect to date• Post progression survival is dramatically increasing

Bottom Line…
For Platinum-sensitive disease, I like:
– Secondary cytoreduction if small volume and remote recurrence
» However, I try HARD to get on clinical trial as this is a very biased situation
– Platinum-based doublets
» PLD, Gemcitabine and Paclitaxel with carboplatin
» If I give gemcitabine doublet I give with bevacizumab
Lots of new trials coming online here as well

Ovarian Cancer: Novel Targets
Matei, Expert Opin Investig Drugs (2007) 16:1227

Developmental Therapeutics: Targets
PericyteTumor
Endothelium
Tumor Cell
Microenvironment

Trebananib: Phase III Studies
Weekly paclitaxel + Trebananib
ClinicalTrials.gov. NCT01204749.
Weekly paclitaxel + placebo
RRecurrent ovarian,FT, PP cancer
R
Pegylated Liposomal Doxorubicin (PLD) + Trebananib
Pegylated Liposomal Doxorubicin (PLD) + placebo
N = 900Primary Objective: PFSSecondary Objectives: OS, RR (RECIST and CA-125), Safety, pK, QOL
TRINOVA-1 Phase III Trial
TRINOVA-2 Phase III Trial
Recurrent ovarian,FT, PP cancer

EC145 Phase III Randomized Study Design in Patients with Platinum Resistant Ovarian Cancer
Blinded Randomized study comparing EC145 + PLD vs. PLD alone
Platinum Resistant patients
~600 Patients randomized 2:1
Study objectives:
– Compare PFS between arms
– Independent radiology review
– OS in EC20 ++ patients

PARP Inhibitors in the Clinic
Nature 2005
BRCA +/+
BRCA -/-
BRCA +/-
1000x

Olaparib Development: Lessons Learned
1Phase I – MTD 400 mg BID– Expansion Phase (N=39 BRCA+) = responses
» Platinum-sensitive > resistant Phase II (BRCA+)
– Dose effect (100 mg BID vs 400 mg BID)2
– PARPi is best measured by PK (AUCss)2 – Is as active as PLD (RP2)3
Phase II (BRCA-wt)– HRD exists as somatic event (30%)4
– RR seen in BRCA-wt, high grade serous5
– Genomic signature may identify these patients6
1Fong, NEJM 20092Audeh Lancet 20103Kaye, ASCO 20114TCGA, 20115Gehlmon, Lancet 20116Konstantinopoulos, JCO 2010

Study 19: Maintenance Olaparib
Olaparib 400 mg po bid
Randomized 1:1
Placebopo bid
Patient eligibility:• Platinum-sensitive high-grade serous ovarian cancer • 2 previous platinum regimens • Last chemotherapy: platinum-based with a maintained response• Stable CA125 at trial entry• Randomization stratification factors:
– Time to disease progression on penultimate platinum therapy– Objective response to last platinum therapy – Ethnic descent
– Primary ENDPOINT: PFS
Treatment until disease
progression
Ledermann, N Engl J Med 2012

Study 19: Secondary Maintenance
Ledermann, N Engl J Med 2012

PARP Inhibitors in Clinical TrialsAgent Administration Phase Comments
Olaparib(AZD-2281)
Oral I, II, III Single Agent and Combination, BRCA and non-BRCA, Platinum-sensitive and resistant, Primary and Recurrent
AZD-2461 Oral I FIH, Solid Tumors
VeliparibABT-888
Oral I, II Single Agent and Combination, BRCA and non-BRCA, Platinum-sensitive and resistant, Primary and Recurrent
(GOG-9923, PIS1004, GOG-280)
BMN 673 Oral I, II BRCA mutation carriers, Platinum Sensitive
CEP-9722 Oral I Combination, Solid Tumors
E7016 Oral I Combination, Solid Tumors
Niraparib(MK4827)
Oral I, II Single Agent and Combination, BRCA and non-BRCA, Platinum-sensitive and resistant
Rucaparib(CO-338)
Oral I, II BRCA mutation carriers, Platinum Sensitive
AG014699 IV II Single Agent, BRCA, Platinum-sensitive and resistant
Iniparib (BSI-201)
IV II, III Combination (Gem/Cis or Carbo), Platinum-sensitive and resistant
Available at: http://www.clinicaltrials.gov.

2013:Phase III Studies in Ovarian Cancer*Front-line added to chemotherapy then as Maintenance
1. Bevacizumab (GOG 262 imaging biomarker study)2. BIBF 1120 (OVAR 12) - closed3. Trebananib (GOG 3001/TRINOVA-3)
Maintenance alone4. Polyglutamate paclitaxel (GOG 212)5. Pazopanib (OVAR 16) - closed6. CVAC (MUC-1)
Platinum-resistant recurrent ovarian cancer 7. Karenitecin8. Trebananib (with Paclitaxel/TRINOVA-1 [closed] or PLD/TRINOVA-2)9. Vintafolide (with PLD)
Platinum-sensitive recurrent ovarian cancer10. Bevacizumab (with chemotherapy - GOG 213)11. Trebananib (with PLD or Paclitaxel)12. Trabectedin with PLD (in 6 – 12 month group/INOVATYON)13. Water soluble formulation of Paclitaxel
*Phase II studies of PARP inhibitors, and Cabozantinib may lead to FDA approval
PLD = Pegylated Liposomal Doxorubicin

Take Home Messages Ovarian cancer is a heterogeneous disease Molecular sub-classification can describe dependency on different
driving/survival mechanisms in otherwise morphologically similar tumors– Consistent patterns of chromosomal change suggests interdependency within
individual tumors
Target discovery has led to a flood of clinical trial development– Most promising: angiogenesis, PI3K, HRD, EMT
Lagging are strategic solutions for induced and adaptive responses to treatment and study designs
Need for new composite endpoints (FDA discussions underway)

Thanks!