Embed Size (px)
Citation preview
Overcoming the Barriers of Clinical Overcoming the Barriers of Clinical
Translation: The Abacavir ExampleTranslation: The Abacavir Example
Elizabeth J. Phillips, MD, FRCPC, FRACPElizabeth J. Phillips, MD, FRCPC, FRACPProfessor & Director, Centre for Clinical Pharmacology Professor & Director, Centre for Clinical Pharmacology
& Infectious Diseases, Murdoch University& Infectious Diseases, Murdoch UniversityRoyal Perth Hospital, Sir Charles Gairdner HospitalRoyal Perth Hospital, Sir Charles Gairdner Hospital
Perth, Western AustraliaPerth, Western Australia
ASCEPT December 1, 2009
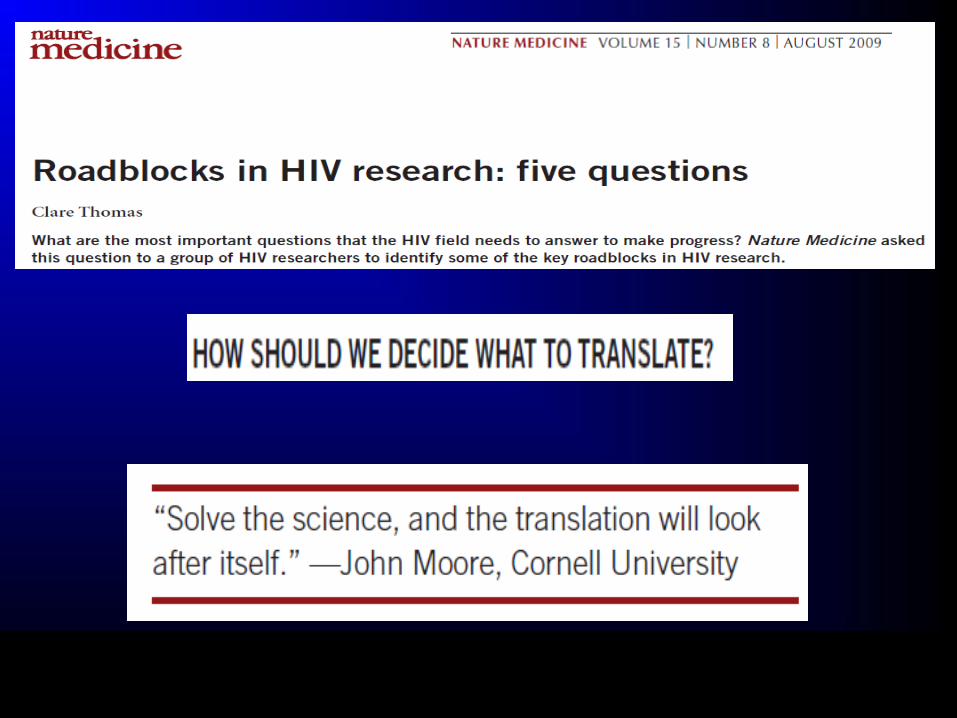
Translation is an Active ProcessTranslation is an Active Process
Pharmacogenetic/genomicDiscovery
-Intepretable and cost-effective test -broad uptake in clinical practice -positive impact on patient effiacy and/or safety
“Lost in Translation”
<1%
>99%
-improved understanding of pathophysiology of disease, mechanism of drug efficacy, toxicity-identification of new therapeutic targets

T1T1T4: The Translational ParadigmT4: The Translational Paradigm
Step 1 - A discovery with a potential applicationStep 1 - A discovery with a potential application
Step 2 - Generation of high-level clinical evidenceStep 2 - Generation of high-level clinical evidence
- Basic science supports biological - Basic science supports biological plausibility plausibility
Step 3 - Delivery of research to the clinicStep 3 - Delivery of research to the clinic
- Quality assurance, valid, efficient and - Quality assurance, valid, efficient and
inexpensive lab testing and lab
report easy to interpret
Step 4 - Evaluation of test in real clinical practice
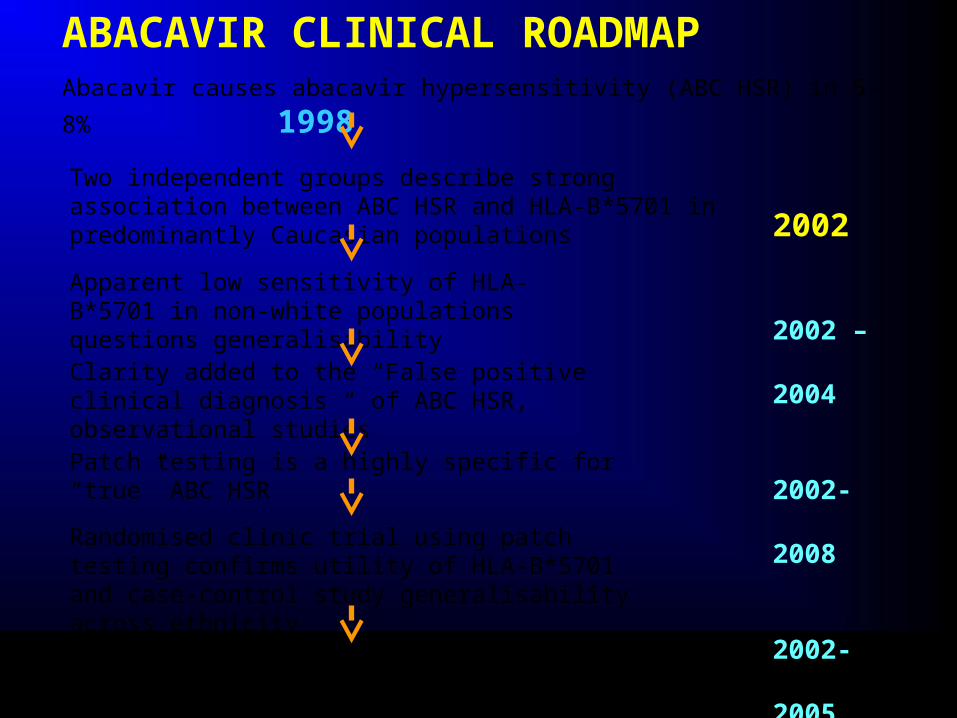
Abacavir causes abacavir hypersensitivity (ABC HSR) in 5-8% 1998
Two independent groups describe strong association between ABC HSR and HLA-B*5701 in predominantly Caucasian populations
Apparent low sensitivity of HLA-B*5701 in non-white populations questions generalisability
Clarity added to the “False positive clinical diagnosis “ of ABC HSR, observational studies
Patch testing is a highly specific for “true” ABC HSR
Randomised clinic trial using patch testing confirms utility of HLA-B*5701 and case-control study generalisability across ethnicity
Widespread uptake into clinic in developed world, incorporation into treatment guidelines, test reimbursed
ABACAVIR CLINICAL ROADMAP
2002
2002 – 2004
2002- 2008
2002- 2005
2008
2008
HLA-B*5701 & Abacavir
Lancet March 30, 2002
Lancet March 2, 2002
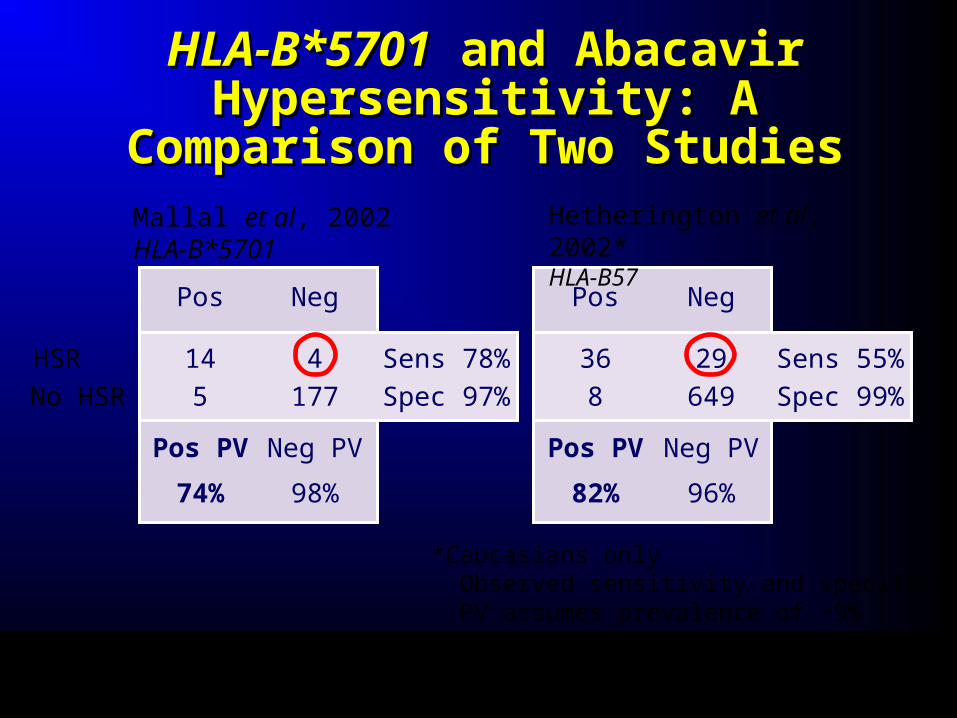
HLA-B*5701HLA-B*5701 and Abacavir and Abacavir Hypersensitivity: A Comparison Hypersensitivity: A Comparison
of Two Studiesof Two Studies
*Caucasians only Observed sensitivity and specificity PV assumes prevalence of ~9%
Pos Neg
Mallal et al, 2002HLA-B*5701
Hetherington et al, 2002*HLA-B57
14 4
5 177
Pos PV Neg PV
74% 98%
HSR
No HSR
Sens 78%
Spec 97%
Pos Neg
36 29
8 649
Pos PV Neg PV
82% 96%
Sens 55%
Spec 99%
Mallal, et al. Lancet 2002;359:727-2.Hetherington, et al. Lancet 2002;359:1121-2.
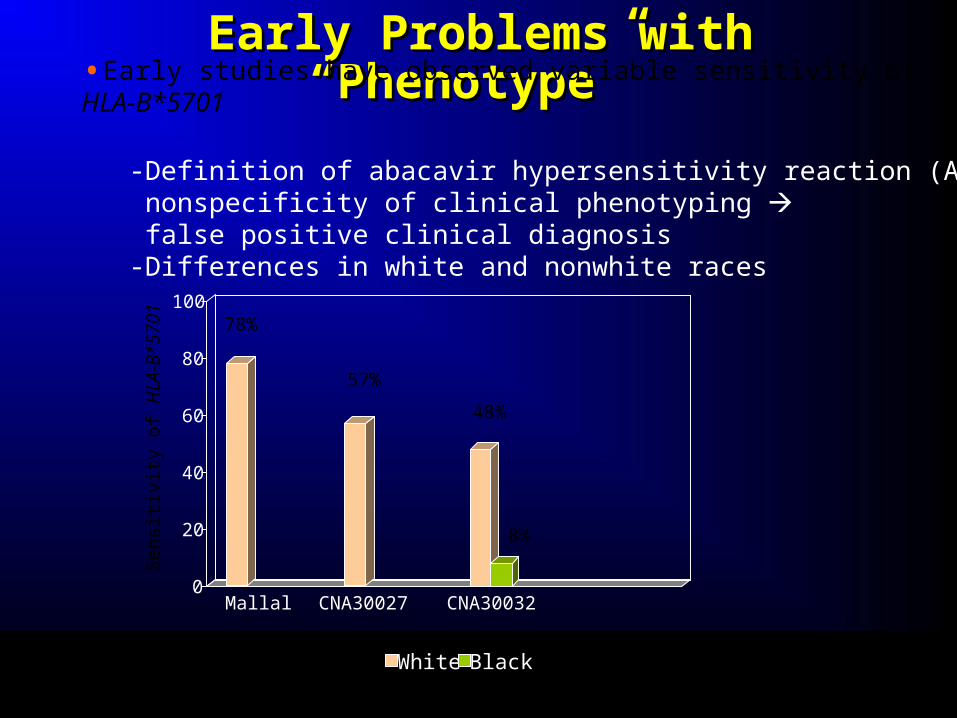
Early Problems with “Phenotype” Early Problems with “Phenotype”
0
20
40
60
80
100
Mallal CNA30027 CNA30032
White Black
78%
57%
48%
8%
•Early studies have observed variable sensitivity of HLA-B*5701
-Definition of abacavir hypersensitivity reaction (ABC HSR) nonspecificity of clinical phenotyping false positive clinical diagnosis-Differences in white and nonwhite races
Sens
itivity
of H
LA-B
*570
1
Mallal et al. Lancet 2002Hughes et al. Pharmacogenomics 2004

Phenotypic Uncertainty of Abacavir HSRPhenotypic Uncertainty of Abacavir HSR
Blinded StudyBlinded Study Abacavir Abacavir GroupsGroups
Zidovudine or Zidovudine or indinavirindinavir
CNA3005CNA3005 19/268 (7%)19/268 (7%) 6/265 (2%)6/265 (2%)
CNA30024CNA30024 27/324 (8%)27/324 (8%) 10/325 (3%)10/325 (3%)
Total CasesTotal Cases 46/592 (7.8%)46/592 (7.8%) 16/590 (2.7%)16/590 (2.7%)
Cases in CNA30024 as reported by Investigators in the ABC HSR CRF Module
Hernandez, et al. ADR/Lipodystrophy 2003.
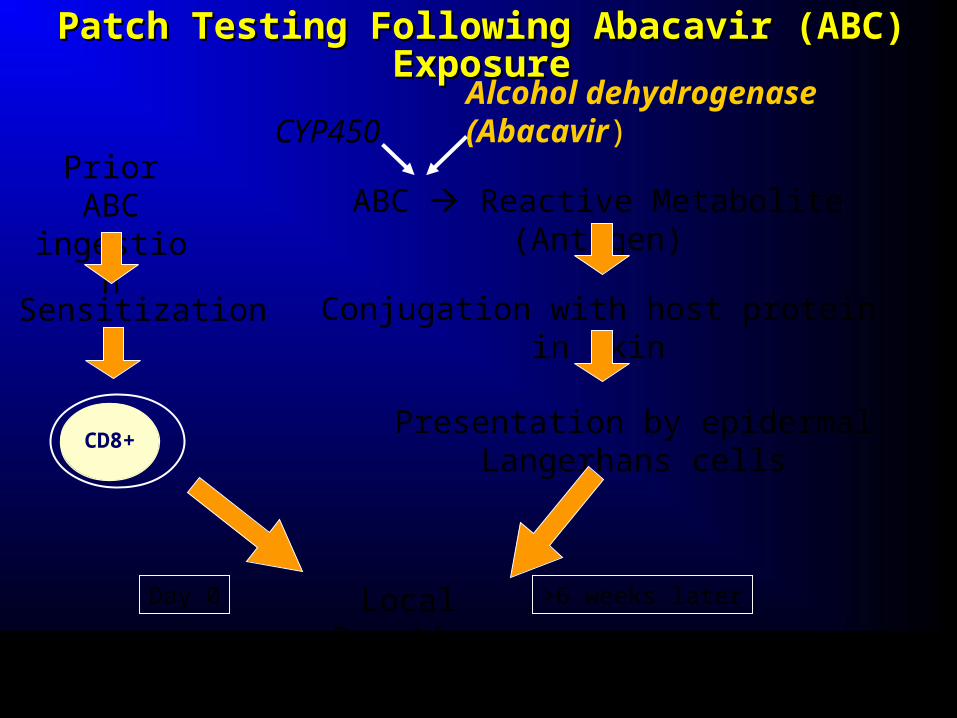
Patch Testing Following Abacavir (ABC) ExposurePatch Testing Following Abacavir (ABC) Exposure
Presentation by epidermal Langerhans cells
Sensitization
Local Reaction
ABC Reactive Metabolite (Antigen)
Alcohol dehydrogenase (Abacavir)
Conjugation with host protein in skin
CYP450
CD8+
Prior ABC ingestion
Day 0 >6 weeks later
Phillips et al AIDS 2002;16:223, Phillips et al AIDS 2005;19:979. Phillips E, Mallal S. Mol Diag Ther 2009;13:19
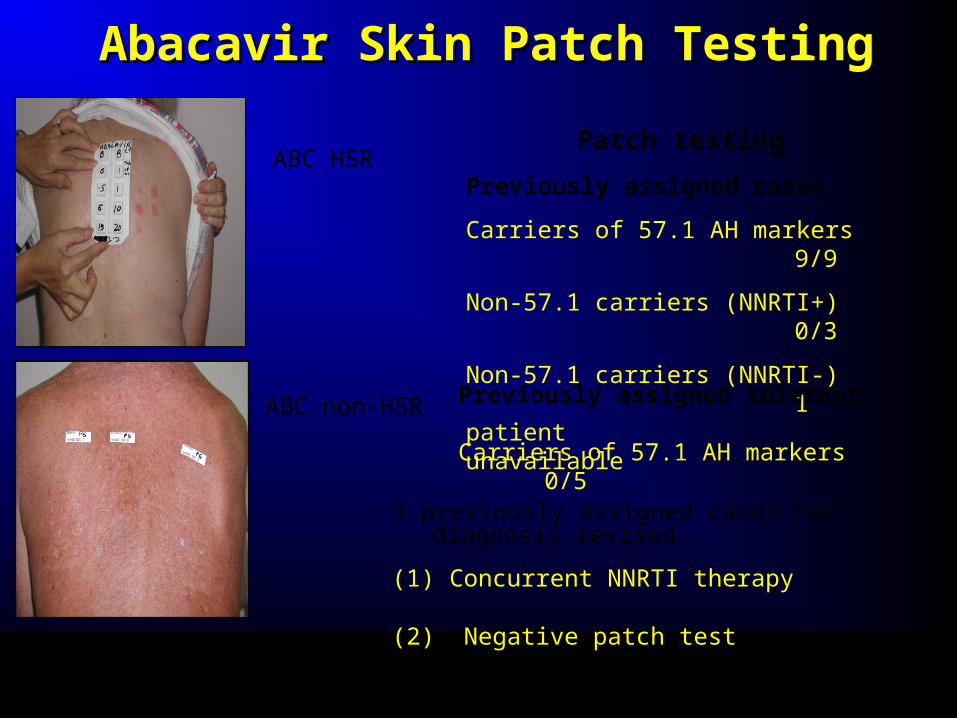
Abacavir Skin Patch TestingAbacavir Skin Patch Testing
3 previously assigned cases had diagnosis revised
(1) Concurrent NNRTI therapy
(2) Negative patch test
Patch testing
Previously assigned cases
Carriers of 57.1 AH markers 9/9
Non-57.1 carriers (NNRTI+) 0/3
Non-57.1 carriers (NNRTI-) 1 patient unavailable
ABC HSR
ABC non-HSR Previously assigned tolerant Carriers of 57.1 AH markers 0/5
Martin, et al. PNAS 2004;23;101:4180-5.
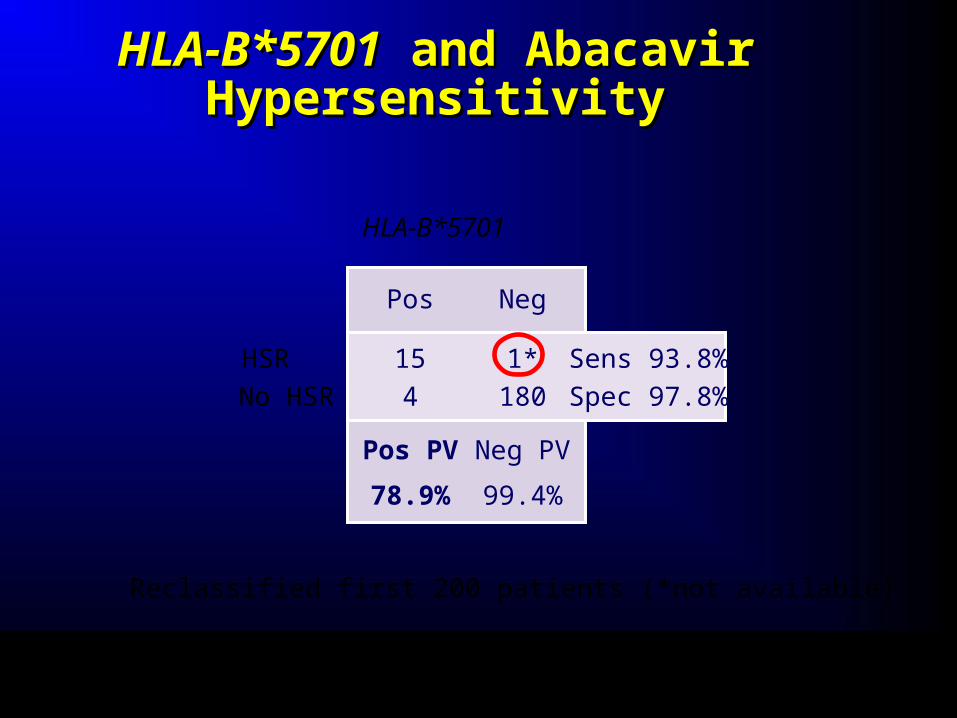
HLAHLA--BB**57015701 and Abacavir and Abacavir HypersensitivityHypersensitivity
Reclassified first 200 patients (*not available)
Martin, et al. PNAS 2004;23;101:4180-5.
Pos Neg
HLA-B*5701
15 1*
4 180
Pos PV Neg PV
78.9% 99.4%
Sens 93.8%
Spec 97.8%
HSR
No HSR
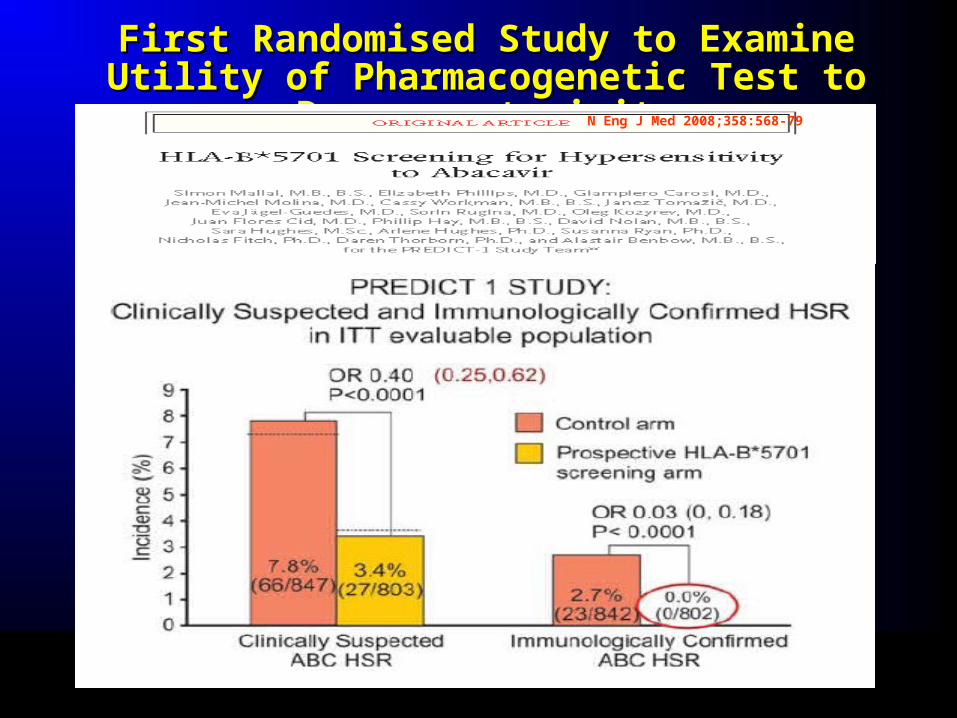
First Randomised Study to Examine Utility of First Randomised Study to Examine Utility of Pharmacogenetic Test to Decrease toxicityPharmacogenetic Test to Decrease toxicity
N Eng J Med 2008;358:568-79

High Negative Predictive Value of HLA-High Negative Predictive Value of HLA-B*5701 Generalised Across RaceB*5701 Generalised Across Race
SPT-pos(n=42/42)
100%
CS-HSR(n=57/130)
44%
Control(n=194/202)
96%
SPT-pos(n=5/5)
100%
CS-HSR(n=10/69)
14%
Control(n=204/206)
99%
White Black
Sens
itivity
/Spe
cifici
ty o
f HLA
-B*5
701
and
95%
CI
OR: White IC-HSR 1945 [110-34352]; CS-HSR 19[8-48] Black IC-HSR 900 [30-21045]; CS-HSR 17[4-164]
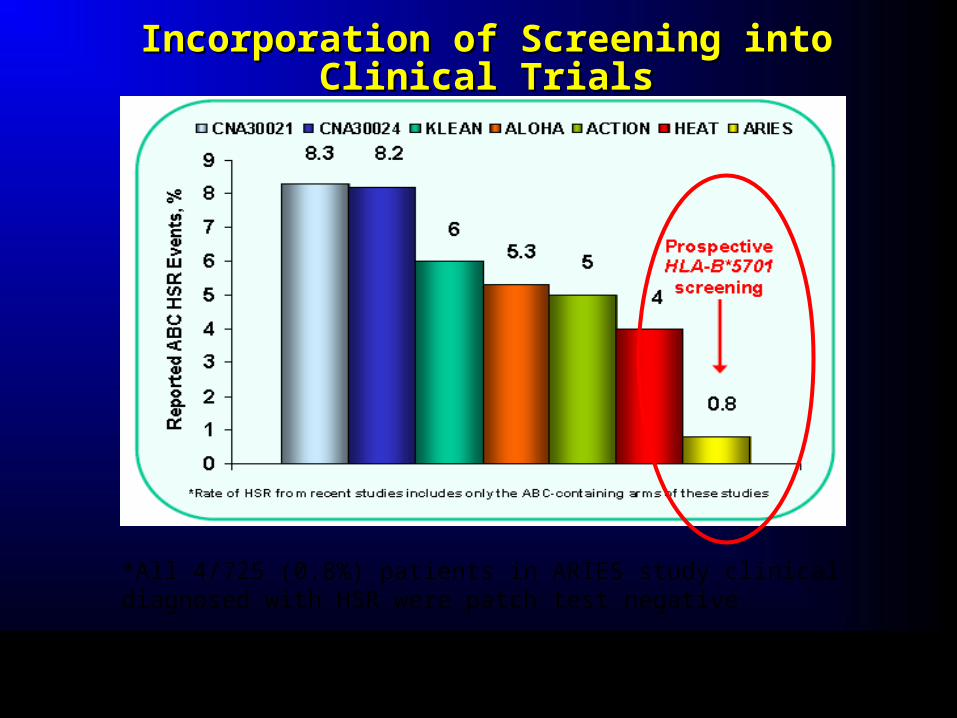
Incorporation of Screening into Clinical TrialsIncorporation of Screening into Clinical Trials
*All 4/725 (0.8%) patients in ARIES study clinical diagnosed with HSR were patch test negative
AIDS 2008;22(13):1673-5
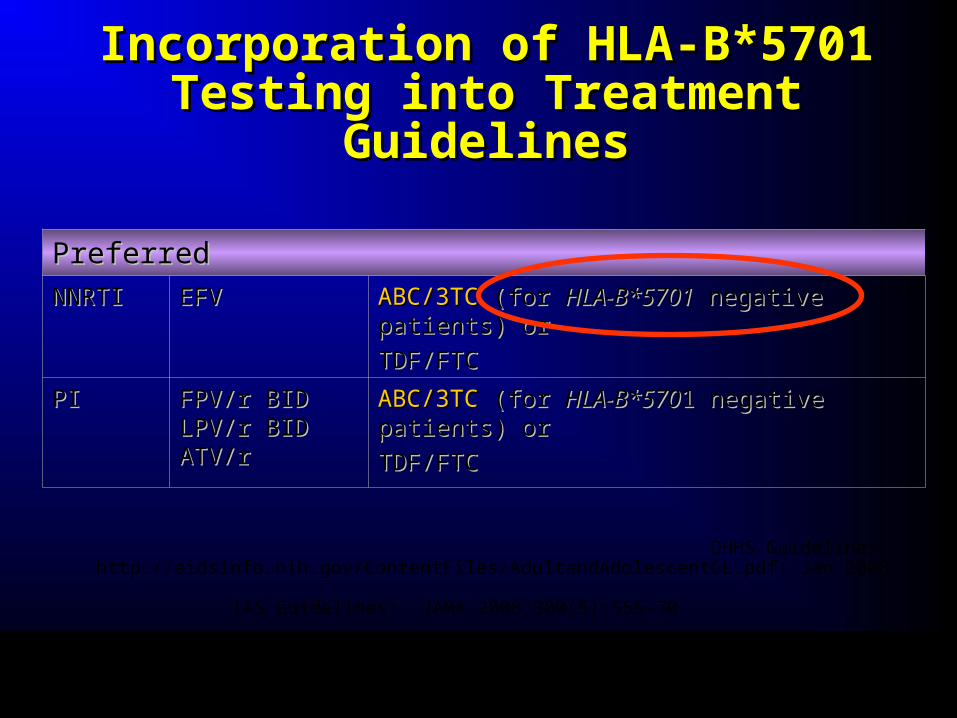
DHHS Guidelines: http://aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf: Jan 2008.
IAS Guidelines: JAMA 2008;300(5):555-70
PreferredPreferred
NNRTINNRTI EFVEFV ABC/3TCABC/3TC (for (for HLA-B*5701HLA-B*5701 negative patients) or negative patients) or
TDF/FTCTDF/FTC
PIPI FPV/r BIDFPV/r BIDLPV/r BIDLPV/r BIDATV/rATV/r
ABC/3TCABC/3TC (for (for HLA-B*570HLA-B*5701 negative patients) or1 negative patients) or
TDF/FTCTDF/FTC
Incorporation of HLA-B*5701 Testing Incorporation of HLA-B*5701 Testing into Treatment Guidelinesinto Treatment Guidelines
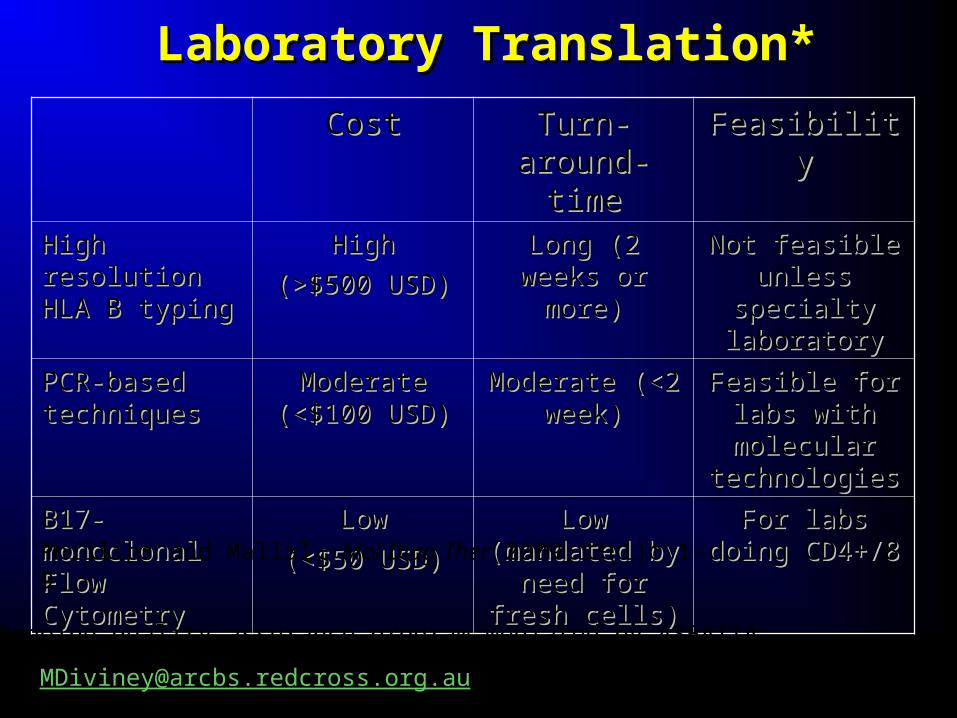
Laboratory Translation*Laboratory Translation*
CostCost Turn-around-Turn-around-timetime
FeasibilityFeasibility
High resolution High resolution HLA B typingHLA B typing
HighHigh
(>$500 USD)(>$500 USD)
Long (2 weeks Long (2 weeks or more)or more)
Not feasible Not feasible unless specialty unless specialty
laboratorylaboratory
PCR-based PCR-based techniquestechniques
Moderate Moderate (<$100 USD)(<$100 USD)
Moderate (<2 Moderate (<2 week)week)
Feasible for labs Feasible for labs with molecular with molecular technologiestechnologies
B17-monoclonal B17-monoclonal Flow CytometryFlow Cytometry
LowLow
(<$50 USD)(<$50 USD)
Low (mandated Low (mandated by need for fresh by need for fresh
cells)cells)
For labs doing For labs doing CD4+/8 CD4+/8
*Ongoing quality assurance program mediated by ASEATTA
Phillips and Mallal, Mol Diag Ther 2009;13(1): 1-9

Cytosol
(1) Abacavir
(5) ER
HLA-B*5701 Class I MHC
Tapasin
TAP
B2m
(1) Abacavir
H 2 N
H O
O NN
N
(9) Pro-inflammatory cytokines
(8)Abacavir specific CD8+ T-cell
(6) Golgi
N
Unknown cytosolic protein?
(3) Proteosome
(4) Haptenated peptide
(10) Hypersensitivity symptoms
Cytosol
Hsp-70?
ADH Abacavir(2) Metabolism
ADH?
Reactive metabolite
(7) Surface of APC
(7) Surface of APC
HLA-B*5701+
TcR
abacavir hapten
OH
R
R
H
R
H
R
H
R
H
R
H
R
HR
H
R
H
N
R
H(4) Haptenated peptide
OH
R R=
H2N N
NH
NN APC
APC
Phillips E and Mallal S. Mol Diag Ther 2009;13(1): 1-9
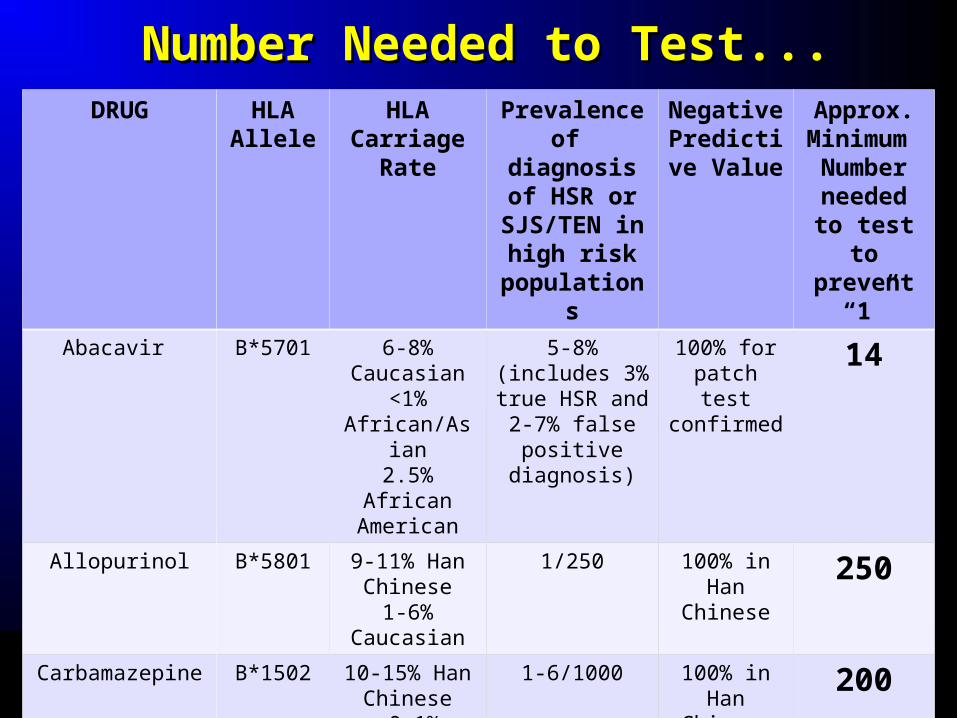
Number Needed to Test...Number Needed to Test...DRUG HLA
AlleleHLA
Carriage Rate
Prevalence of diagnosis
of HSR or SJS/TEN in
high risk populations
Negative Predictive
Value
Approx. Minimum Number
needed to test to
prevent “1”
Abacavir B*5701 6-8% Caucasian
<1% African/Asian2.5% African
American
5-8% (includes 3% true HSR
and 2-7% false positive
diagnosis)
100% for patch test confirmed
14
Allopurinol B*5801 9-11% Han Chinese
1-6% Caucasian
1/250 100% in Han
Chinese
250
Carbamazepine B*1502 10-15% Han Chinese<0.1%
Caucasian
1-6/1000 100% in Han
Chinese
200
Challenges to Translation – Challenges to Translation – Beyond AbacavirBeyond Abacavir
More prospective studies needed but difficulties in More prospective studies needed but difficulties in generating high level evidence for generic drugs (???generating high level evidence for generic drugs (???funding)funding)
Generalisation difficulties for other drugs (negative Generalisation difficulties for other drugs (negative predictive value of HLA-B*5801 and HLA-B*1502 will be predictive value of HLA-B*5801 and HLA-B*1502 will be <<<100% in Caucasians)<<<100% in Caucasians)
Specificity of phenotype (lack of “patch test” Specificity of phenotype (lack of “patch test” equivalents)equivalents)
Single gene/allele associations will be unlikely for most Single gene/allele associations will be unlikely for most drugsdrugs
AcknowledgmentsAcknowledgmentsAcknowledgmentsAcknowledgments
Simon Mallal Simon Mallal James McCluskeyJames McCluskey
David NolanDavid Nolan Dianne Cheesman Dianne Cheesman
IIan Jamesan James Tess Lethborg Tess Lethborg
Mina JohnMina John Tony PurcellTony Purcell
Annalise MartinAnnalise Martin Emma Hammond Emma Hammond
Annette Patterson Annette Patterson Mandvi Bharafway Mandvi Bharafway
Campbell WittCampbell Witt Richard Harrigan Richard Harrigan
Frank ChristiansenFrank Christiansen Andri Rauch Andri Rauch
Rom KreugerRom Kreuger Amalio Telenti Amalio Telenti
Susan HerrmannSusan Herrmann Hansjakob Furrer Hansjakob Furrer
Coral-Ann AlmeidaCoral-Ann Almeida Julio Montaner Julio Montaner
GSK and PREDICT-1 and SHAPE investigators and study teamsGSK and PREDICT-1 and SHAPE investigators and study teams
National Health and Medical Research Council of Australia National Health and Medical Research Council of Australia
Simon Mallal Simon Mallal James McCluskeyJames McCluskey
David NolanDavid Nolan Dianne Cheesman Dianne Cheesman
IIan Jamesan James Tess Lethborg Tess Lethborg
Mina JohnMina John Tony PurcellTony Purcell
Annalise MartinAnnalise Martin Emma Hammond Emma Hammond
Annette Patterson Annette Patterson Mandvi Bharafway Mandvi Bharafway
Campbell WittCampbell Witt Richard Harrigan Richard Harrigan
Frank ChristiansenFrank Christiansen Andri Rauch Andri Rauch
Rom KreugerRom Kreuger Amalio Telenti Amalio Telenti
Susan HerrmannSusan Herrmann Hansjakob Furrer Hansjakob Furrer
Coral-Ann AlmeidaCoral-Ann Almeida Julio Montaner Julio Montaner
GSK and PREDICT-1 and SHAPE investigators and study teamsGSK and PREDICT-1 and SHAPE investigators and study teams
National Health and Medical Research Council of Australia National Health and Medical Research Council of Australia
Participants and clinical staff involved in the Western Australian HIV Cohort Study
Western AustralianHIV Cohort Study
Western AustralianHIV Cohort Study
Canadian Foundation for AIDS Research
Canadian Dermatology Foundation
“In the middle of difficulty lies opportunity”
“We can’t solve problems by using the same kind of thinking we used when we created them”
Albert Einstein 1878-1955