Embed Size (px)
Citation preview

OVERDOSE OVERDOSE & &
TOXIC INGESTIONSTOXIC INGESTIONS

What is an Overdose?What is an Overdose?
Exposure to excessive amounts of a Exposure to excessive amounts of a substance normally intended for substance normally intended for consumption.consumption.
Poisoning is the development of harmful Poisoning is the development of harmful effects following exposure to chemicals.effects following exposure to chemicals.
Pharmaceuticals are responsible for 41% Pharmaceuticals are responsible for 41% of poisonings and 75% of fatal poisonings.of poisonings and 75% of fatal poisonings.

Treatment OverviewTreatment Overview
Supportive CareSupportive Care
Prevention of toxin absorptionPrevention of toxin absorption
Enhancement of drug eliminationEnhancement of drug elimination
Administration of antidoteAdministration of antidote

Initial MeasuresInitial Measures Airway Airway
– Establish patent airway by positioning and Establish patent airway by positioning and suctioning.suctioning.
– Intubate if obtunded, comatose, no gag reflex .Intubate if obtunded, comatose, no gag reflex .
BreathingBreathing– Assess depth and rate .Assess depth and rate .– Pulse ox in all.Pulse ox in all.– ABG if suspicious . ABG if suspicious .

Initial MeasuresInitial Measures
CirculationCirculation– Treat with NS or pressors if hypotensiveTreat with NS or pressors if hypotensive– Assess for arrhythmiasAssess for arrhythmias
--D-Drugs (give all three)D-Drugs (give all three) Dextrose 50%,Dextrose 50%, Thiamine 100mg.Thiamine 100mg. Naloxone0.4 to 2mg & Naloxone0.4 to 2mg & consider Flumazenil consider Flumazenil (do not give flumazenil in TCA overdose(do not give flumazenil in TCA overdose, BZD dependency , BZD dependency
and seizure disorder)and seizure disorder)

Prevention of Toxin AbsorptionPrevention of Toxin AbsorptionEmesis:Emesis:-Now not performed. Replaced by lavage/charcoal-Now not performed. Replaced by lavage/charcoal-Contraindicated in corrosive poisonings/aspiration risk.-Contraindicated in corrosive poisonings/aspiration risk.
Gastric Lavage:Gastric Lavage: Indications:Indications: - Removal of gastric contents (within the first hour). Examination of gastric contents. Removal of gastric contents (within the first hour). Examination of gastric contents.
Facilitate charcoal. Facilitate charcoal.
Contraindications:Contraindications:- Do not do if patient comatose unless intubated. Also do not use if corrosives are Do not do if patient comatose unless intubated. Also do not use if corrosives are
ingested. (controversial)ingested. (controversial)
Technique:Technique: - Place patient in left lateral head down position if not intubated. Insert a soft lubricated Place patient in left lateral head down position if not intubated. Insert a soft lubricated
tube through mouth or nose into stomach. Aspirate and save contents and then tube through mouth or nose into stomach. Aspirate and save contents and then lavage repeatedly with 50-100ml of fluid until returns are clear .Use luke warm water lavage repeatedly with 50-100ml of fluid until returns are clear .Use luke warm water or saline. or saline.

Prevention of Toxin AbsorptionPrevention of Toxin AbsorptionActivated CharcoalActivated Charcoal
– Adsorbs almost all drugs and poisons. Poorly adsorbed substances are Adsorbs almost all drugs and poisons. Poorly adsorbed substances are Lithium, Potassium, Lithium, Potassium, alcohol, iron, cyanide.alcohol, iron, cyanide.
Indications:Indications: • All poisonings.All poisonings.
Contraindications:Contraindications:
• Comatose or obtunded unless given by gastric tube or intubated as drinking charcoal can Comatose or obtunded unless given by gastric tube or intubated as drinking charcoal can cause emesis.cause emesis.
• Ileus or intestinal obstruction. (delays expulsion of charcoal)Ileus or intestinal obstruction. (delays expulsion of charcoal)• Corrosive poisonings where endoscopy is planned .Corrosive poisonings where endoscopy is planned .
Technique:Technique: 60-100grams orally or via gastric tube .Repeat doses 20-30mg every 3-4 hours may be 60-100grams orally or via gastric tube .Repeat doses 20-30mg every 3-4 hours may be
used to hasten the elimination of some drugs (digoxin, theophylline and phenobarbitol) by used to hasten the elimination of some drugs (digoxin, theophylline and phenobarbitol) by adsorbing drug excreted into the gut lumen (entero hepatic circulation).adsorbing drug excreted into the gut lumen (entero hepatic circulation).
Prevention of Toxin AbsorptionPrevention of Toxin Absorption
Whole Bowel Irrigation: Cleanses the GI tractWhole Bowel Irrigation: Cleanses the GI tract
Indications:Indications: -Used for “body stuffers/packers” (People who swallow packets of drugs -Used for “body stuffers/packers” (People who swallow packets of drugs
for smuggling.)for smuggling.) - Massive iron ingestion - Massive iron ingestion
Technique:Technique: 2 Liters/hour of go-lytely electrolyte soln. Given via gastric tube at rate of 1-2 Liters/hour of go-lytely electrolyte soln. Given via gastric tube at rate of 1-
2L/hour until rectal effluent is clear. Patient must be able to sit to pass 2L/hour until rectal effluent is clear. Patient must be able to sit to pass contents. contents.

Increased drug removalIncreased drug removal
Urinary manipulationUrinary manipulation
Alkalization of urineAlkalization of urine: Salicylates, Phenobarbitol.: Salicylates, Phenobarbitol.
Forced diuresisForced diuresis: No longer recommended as it causes : No longer recommended as it causes electrolyte imbalances. electrolyte imbalances.
DialysisDialysis Known dialyzable drugs.Known dialyzable drugs. Severe states :coma, refractory hypotension, Severe states :coma, refractory hypotension,
hypothermia for quick effecthypothermia for quick effect Hepatic or renal failure where excretion of the drug may Hepatic or renal failure where excretion of the drug may
be compromised. be compromised.
Diagnosis of OverdoseDiagnosis of OverdoseHistory:History:
Dependent upon history obtained and Dependent upon history obtained and reliability of history. reliability of history.
Paramedics/Police will usually bring in pill Paramedics/Police will usually bring in pill bottles: Calculate the amount taken, and bottles: Calculate the amount taken, and always assume the worst case scenario.always assume the worst case scenario.

Diagnosis of OverdoseDiagnosis of Overdose Physical examinationPhysical examination
5P’s :5P’s :Pressure, Pulse rate , perspiration, pupils peristalsis .Pressure, Pulse rate , perspiration, pupils peristalsis .
Based on above three syndromes:Based on above three syndromes:Sympathomimetic syndrome :Sympathomimetic syndrome : Amphetamines, cocaine, ephedrine, psuedoephidrine, PCP (pupils Amphetamines, cocaine, ephedrine, psuedoephidrine, PCP (pupils
may be small) may be small)
Sympatholytic syndrome:Sympatholytic syndrome: Benzo, Barbiturates, other sedative hypnotics, opioids, clonidine.Benzo, Barbiturates, other sedative hypnotics, opioids, clonidine.
Cholinergic: Cholinergic: Nicotine, organophosphates, physostigmine. Nicotine, organophosphates, physostigmine.

Initial Laboratory EvaluationInitial Laboratory Evaluation
EKGEKG
Basic ChemistryBasic Chemistry– Calculate anion gapCalculate anion gap
• ABG ABG
Drug ScreenDrug Screen
Serum Osmolality Serum Osmolality (calculate osmolar (calculate osmolar gap)gap)
Quantitative Drug Quantitative Drug LevelsLevels

AcetaminophenAcetaminophen
PathophysiologyPathophysiology Acetaminophen is metabolized by the Acetaminophen is metabolized by the
cytochrome P450 pathway to a toxic cytochrome P450 pathway to a toxic intermediate that is detoxified by glutathione. intermediate that is detoxified by glutathione. With acute acetaminophen overdose With acute acetaminophen overdose hepatocellular glutathione is depleted allowing hepatocellular glutathione is depleted allowing the toxic intermediate to attack cell proteins and the toxic intermediate to attack cell proteins and cause cell necrosis. Patients with enhanced cause cell necrosis. Patients with enhanced cytochrome P450 activity like alcoholics and cytochrome P450 activity like alcoholics and anticonvulsant users are at greater risk of anticonvulsant users are at greater risk of hepatotoxicity. hepatotoxicity.
AcetaminophenAcetaminophen
Dose:Dose:Acute ingestion: >7.5 grams/24 hours is toxic – just a guideline!Acute ingestion: >7.5 grams/24 hours is toxic – just a guideline!Chronic ingestion: >4 grams a day.Chronic ingestion: >4 grams a day.
Symptoms:Symptoms: 11stst 24 hours to 48 hours-Asymptomatic. 24 hours to 48 hours-Asymptomatic. 24-48 hours – Rise of aminotransfersases, jaundice, 24-48 hours – Rise of aminotransfersases, jaundice,
encephalopathy. encephalopathy.
Treatment:Treatment:Lavage & Activated Charcoal indicated.Lavage & Activated Charcoal indicated.Rumack-Matthew Rumack-Matthew Nomogram utilized to decide whether treatment Nomogram utilized to decide whether treatment with with N-acetylcysteineN-acetylcysteine is required. is required.


AcetaminophenAcetaminophen N-Acetylcysteine increases the availability of N-Acetylcysteine increases the availability of glutathione, decreasing hepatic toxicity.glutathione, decreasing hepatic toxicity.
If patient has a toxic level, give the full course (usually If patient has a toxic level, give the full course (usually 17 doses). 140mg/kg orally followed by 70mg/kg. 17 doses). 140mg/kg orally followed by 70mg/kg.
May be helpful even up to 36 hours after ingestionMay be helpful even up to 36 hours after ingestion
If uncertain about the timing of ingestion and at high If uncertain about the timing of ingestion and at high risk patients (alcoholics, CytP450 inducing drug takers, risk patients (alcoholics, CytP450 inducing drug takers, liver disease) use lower line.liver disease) use lower line.
Remember: Nomogram not useful for chronic Remember: Nomogram not useful for chronic overdoses and for overdoses that may be associated overdoses and for overdoses that may be associated with ingestion of another drug that delays GI motility.with ingestion of another drug that delays GI motility.
The AlcoholsThe AlcoholsMethanolMethanol
Found in windshield wipers .Methanol is Found in windshield wipers .Methanol is metabolized to formaldehyde and formic acid metabolized to formaldehyde and formic acid which acts as toxin.which acts as toxin.
Symptoms may not appear for 12-18 hours Symptoms may not appear for 12-18 hours because toxins must accumulate, may be because toxins must accumulate, may be longer if ingested with ethanol because EtOH longer if ingested with ethanol because EtOH inhibits metabolism inhibits metabolism
Symptoms: CNS depression, visual changes Symptoms: CNS depression, visual changes with with blurring/blindnessblurring/blindness, abdominal pain, N/V, abdominal pain, N/V
Labs: Wide Labs: Wide anion gapanion gap metabolic acidosis with metabolic acidosis with osmolar gap >10osmolar gap >10

The AlcoholsThe AlcoholsEthylene GlycolEthylene Glycol
Found in antifreeze.Found in antifreeze.3 distinct clinical phases3 distinct clinical phases due to the toxic metabolites due to the toxic metabolites glycolate, glyoxalate, and oxalateglycolate, glyoxalate, and oxalate– First 12 hours: First 12 hours: CNS effectsCNS effects
appears intoxicatedappears intoxicated– 12-24 hours: 12-24 hours: Cardiopulmonary effectsCardiopulmonary effects
Increased HR, RR and BPIncreased HR, RR and BPCHF, respiratory distress syndrome, circulatory collapseCHF, respiratory distress syndrome, circulatory collapse
– 24-72 hours: 24-72 hours: Renal effectsRenal effectsATN with ARFATN with ARF
Wide Wide anion gap metabolic acidosisanion gap metabolic acidosis with with osmolar gap osmolar gap >10>10Metabolized to oxalic acid. Metabolized to oxalic acid. Calcium oxalate crystalsCalcium oxalate crystals seen in urine 33% of the timeseen in urine 33% of the time

The AlcoholsThe AlcoholsEthylene GlycolEthylene GlycolOxalate crystalsOxalate crystals

The AlcoholsThe AlcoholsTreatment of Methanol and Ethylene Glycol Treatment of Methanol and Ethylene Glycol
IngestionIngestionRapid DiagnosisRapid Diagnosis– Hx suspicious for useHx suspicious for use– Wide anion gap with a wide osmolar gap, then order serum Wide anion gap with a wide osmolar gap, then order serum
level and begin:level and begin:
EthanolEthanol infusion (not used as much) to keep blood infusion (not used as much) to keep blood alcohol >100. alcohol >100.– Competitively inhibits metabolism of MeOH and EG by Competitively inhibits metabolism of MeOH and EG by
alcohol dehydrogenase, has a 10-20 greater affinity than alcohol dehydrogenase, has a 10-20 greater affinity than MeOH and 100 times that of EGMeOH and 100 times that of EG
– Is continued until measured levels are zeroIs continued until measured levels are zero
FomepizoleFomepizole (4-methylpyrazole) – more common (4-methylpyrazole) – more common– A competitive inhibitor of alcohol dehydrogenaseA competitive inhibitor of alcohol dehydrogenase– Is an alternative to EtOH infusion. Is an alternative to EtOH infusion.
DDialysisialysis for severe cases (serum level > 50mg/dl, refractory for severe cases (serum level > 50mg/dl, refractory acidosis)acidosis)

The AlcoholsThe AlcoholsIsopropyl AlcoholIsopropyl Alcohol
Found in rubbing alcohol and paint thinnersFound in rubbing alcohol and paint thinnersCNS effects are twice as potent and twice as CNS effects are twice as potent and twice as long acting as EtOHlong acting as EtOHSymptoms are similar to EtOH intoxication, Symptoms are similar to EtOH intoxication, severe posioning causes early onset coma, severe posioning causes early onset coma, respiratory depression, and respiratory depression, and hypotensionhypotensionHemorrhagic gastritisHemorrhagic gastritis is a characteristic is a characteristic findingfindingKetosis without acidosisKetosis without acidosis– Metabolized to acetoneMetabolized to acetone– Ketonemia/ketonuria and Ketonemia/ketonuria and osmolol gaposmolol gap with with
minimal or no acidosis is unique characteristicminimal or no acidosis is unique characteristic
Treatment is supportive with dialysis if patient Treatment is supportive with dialysis if patient continues to deteriorate.continues to deteriorate.

Tricyclic AntidepressantsTricyclic Antidepressants Most dangerous of overdoses.Most dangerous of overdoses.
(25% of fatalities occur in patients who are awake, alert, and in (25% of fatalities occur in patients who are awake, alert, and in NSR at time of presentation)NSR at time of presentation)
Clinical findings & TreatmentsClinical findings & Treatments
(1) (1) Anticholinergic:Anticholinergic: Tachycardia, dry mouth, flushed skin, decreased peristalsis. Tachycardia, dry mouth, flushed skin, decreased peristalsis.
(2) (2) Cardiotoxicity:Cardiotoxicity: Quinidine like effect. Blocks sodium channels. Therefore Quinidine like effect. Blocks sodium channels. Therefore
widening of the QRS interval , ventricular arrhythmias, AV widening of the QRS interval , ventricular arrhythmias, AV nodal block. nodal block.

Tricyclic AntidepressantsTricyclic Antidepressants
Rx: Rx: Admit in Telemetry. Admit in Telemetry. Alkalinization either using sodium bicarbonate and Alkalinization either using sodium bicarbonate and
hyperventilation if intubated to a pH of 7.45-7.55. The sodium in hyperventilation if intubated to a pH of 7.45-7.55. The sodium in the NaHCO3 alleviates depression of the sodium channels. Also the NaHCO3 alleviates depression of the sodium channels. Also acidosis impairs sodium channels so alkalinization beneficial. acidosis impairs sodium channels so alkalinization beneficial.
Manage arrhythmias with lidocaine, magnesium, isoproterenol, Manage arrhythmias with lidocaine, magnesium, isoproterenol, and pacing and pacing
• Neurologic:Neurologic: Seizures. ( Note due to absence of sweating and seizures Seizures. ( Note due to absence of sweating and seizures
hyperthermia can occur)hyperthermia can occur)
Rx: benzodiazepines. Rx: benzodiazepines.

SalicylatesSalicylatesAspirin, methyl salicylate (various OTC drugs)Aspirin, methyl salicylate (various OTC drugs)Pathophysiology:Pathophysiology:
Uncouple cellular oxidative phosphorylation and Uncouple cellular oxidative phosphorylation and cause anaerobic metabolism (lactic acidosis) and heat cause anaerobic metabolism (lactic acidosis) and heat production.production.
Salicylates directly stimulate respiratory centers in Salicylates directly stimulate respiratory centers in the brainstem.the brainstem.
Mixed respiratory alkalosis with metabolic acidosis. Mixed respiratory alkalosis with metabolic acidosis. (wide anion gap).(wide anion gap).
Coagulopathy present secondary to platelet Coagulopathy present secondary to platelet dysfunction and decreased synthesis of coagulation dysfunction and decreased synthesis of coagulation factors (salicylate induced hypoprothrombinemia).factors (salicylate induced hypoprothrombinemia).

SalicylatesSalicylates
Symptoms:Symptoms:Dose dependantDose dependant acute ingestion (> 200mg/kg) or chronic excessive dosing .acute ingestion (> 200mg/kg) or chronic excessive dosing .Severe: Agitation, Coma, CV collapse,Severe: Agitation, Coma, CV collapse, pulmonary edema, hyperthermia & pulmonary edema, hyperthermia & death.death.
Labs:Labs: Suspect in any anion gap metabolic acidosis Suspect in any anion gap metabolic acidosis Salicylate level elevated salicylate level.Salicylate level elevated salicylate level. ABG : Shows mixed Met acidosis & resp alkalosis. ABG : Shows mixed Met acidosis & resp alkalosis.
SalicylatesSalicylates
Therapy:Therapy:
General: General: Activated charcoal( 10:1 by weight).Activated charcoal( 10:1 by weight). NaHCO3: Critical for therapy as acidosis NaHCO3: Critical for therapy as acidosis
promotes the entry of salicylic acid into the cells. promotes the entry of salicylic acid into the cells. (keep>7.4).(keep>7.4).
Specific:Specific:Urinary alkalization . Urinary alkalization . Hemodialysis ( >1000-2000mg/L after acute Hemodialysis ( >1000-2000mg/L after acute
overdose or> 60-70mg/dl with sub acute or overdose or> 60-70mg/dl with sub acute or chronic overdose).chronic overdose).

Beta BlockersBeta BlockersMost toxic is PropranololMost toxic is PropranololSymptoms:Symptoms:
Cardiac: Bradycardia, AV blockade, hypotension.Cardiac: Bradycardia, AV blockade, hypotension. Rx: Atropine or Isoproterenol if noRx: Atropine or Isoproterenol if no response give Glucagon. May needresponse give Glucagon. May need temporary pacing. temporary pacing.
CNS: Delerium, coma, or seizures. CNS: Delerium, coma, or seizures. Rx:Ativan for seizuresRx:Ativan for seizures Electrolyte: Hyperkalemia and hypoglycemiaElectrolyte: Hyperkalemia and hypoglycemia

Ca Channel BlockersCa Channel BlockersSymptoms include bradycardia, conduction Symptoms include bradycardia, conduction delays, impaired contractility, and delays, impaired contractility, and hypotensionhypotensionGastric lavage and activated charcoalGastric lavage and activated charcoal– May consider whole bowel irrigation for sustained May consider whole bowel irrigation for sustained
release preparationsrelease preparations
May respond to atropine, isoproterenol, or May respond to atropine, isoproterenol, or pacing IVF pacing IVF If no response IV calcium chloride or calcium If no response IV calcium chloride or calcium gluconate to treat hypotension and gluconate to treat hypotension and conduction defects.conduction defects.Glucagon is occasionally beneficial in severe Glucagon is occasionally beneficial in severe toxicitytoxicity
DigitalisDigitalis
Pathophysiology: 2 main effects: Blocks AV node & blocks Na/K ATPase. The blockade Pathophysiology: 2 main effects: Blocks AV node & blocks Na/K ATPase. The blockade of Na/K ATPase increases intracellular Ca and causes delayed after depolarizations of Na/K ATPase increases intracellular Ca and causes delayed after depolarizations (which can cause VPC and VT). Toxic: Therapeutic ratio is very narrow.(which can cause VPC and VT). Toxic: Therapeutic ratio is very narrow.
Acute overdose: GI: Nausea, vomiting. Acute overdose: GI: Nausea, vomiting. Cardiac: Bradycardia, cardiac arrhythmias mostly ventricular.Cardiac: Bradycardia, cardiac arrhythmias mostly ventricular. Electrolyte: Hyperkalemia.Electrolyte: Hyperkalemia.
Chronic: Hypokalemia, hypomagnesemia as patients are on diuretics. Hypokalemia Chronic: Hypokalemia, hypomagnesemia as patients are on diuretics. Hypokalemia aggravates dig toxicity.aggravates dig toxicity.
Treatment:Treatment:Bradycardia can be controlled with atropine or temporary pacingBradycardia can be controlled with atropine or temporary pacingLidocaine for ventricular arrhythmiasLidocaine for ventricular arrhythmiasDigibind (digoxin-specific Fab antibody fragments) is effective in rapidly reversing life-Digibind (digoxin-specific Fab antibody fragments) is effective in rapidly reversing life-threatening intoxicationsthreatening intoxications– Is cleared via renal excretionIs cleared via renal excretion– 40 mg vial neutralizes ~0.6 mg of digoxin40 mg vial neutralizes ~0.6 mg of digoxin

Atropine & AnticholinergicsAtropine & Anticholinergics
Drugs with anticholinergic effects:Drugs with anticholinergic effects: AtropineAtropine Antihistamines: BenadrylAntihistamines: Benadryl MushroomsMushrooms TCATCAEffects:Effects:Symptoms: Dry mouth, thirst, blurring of vision, constipation. Symptoms: Dry mouth, thirst, blurring of vision, constipation. Signs: Psychosis, dilated pupils, fever, ileus, urinary Signs: Psychosis, dilated pupils, fever, ileus, urinary
retention.retention.
Rx:Rx:Charcoal (can give late as there is delayed gut emptying)Charcoal (can give late as there is delayed gut emptying)Physostigmine (with ECG monitoring).Physostigmine (with ECG monitoring).

CyanideCyanide Situations:Situations: Fires-HCN gas is a component of smoke in fires Fires-HCN gas is a component of smoke in fires Apricot pitsApricot pits Nitroprusside infusion Nitroprusside infusion Acetonitrile (finger nail glue removers) has CNAcetonitrile (finger nail glue removers) has CN
Pathophysiology:Pathophysiology: Rapidly absorbed by any route (GI, skin, inhalation)Rapidly absorbed by any route (GI, skin, inhalation) Inhibits cytochrome oxidase , cellular respiration. Switches to Inhibits cytochrome oxidase , cellular respiration. Switches to
anaerobic metabolism and therefore lactic acidosis occurs.anaerobic metabolism and therefore lactic acidosis occurs.

CyanideCyanide
Symptoms:Symptoms: Headache, dizzinness, abdominal pain, nausea. Followed quickly Headache, dizzinness, abdominal pain, nausea. Followed quickly
by syncope, shock and coma.by syncope, shock and coma.
Labs:Labs: Unexplained lactic acidosisUnexplained lactic acidosis High Venous O2 sats (>90%) as tissues fail to take up oxygen.High Venous O2 sats (>90%) as tissues fail to take up oxygen.
Treatment:Treatment: Remove from site of exposureRemove from site of exposure Charcoal: CN is poorly adsorbed ,therefore larger doses.Charcoal: CN is poorly adsorbed ,therefore larger doses. “ “Pack” available consists of Amylnitrite, Sodium nitrite and Na Pack” available consists of Amylnitrite, Sodium nitrite and Na
thiosulfate. thiosulfate.
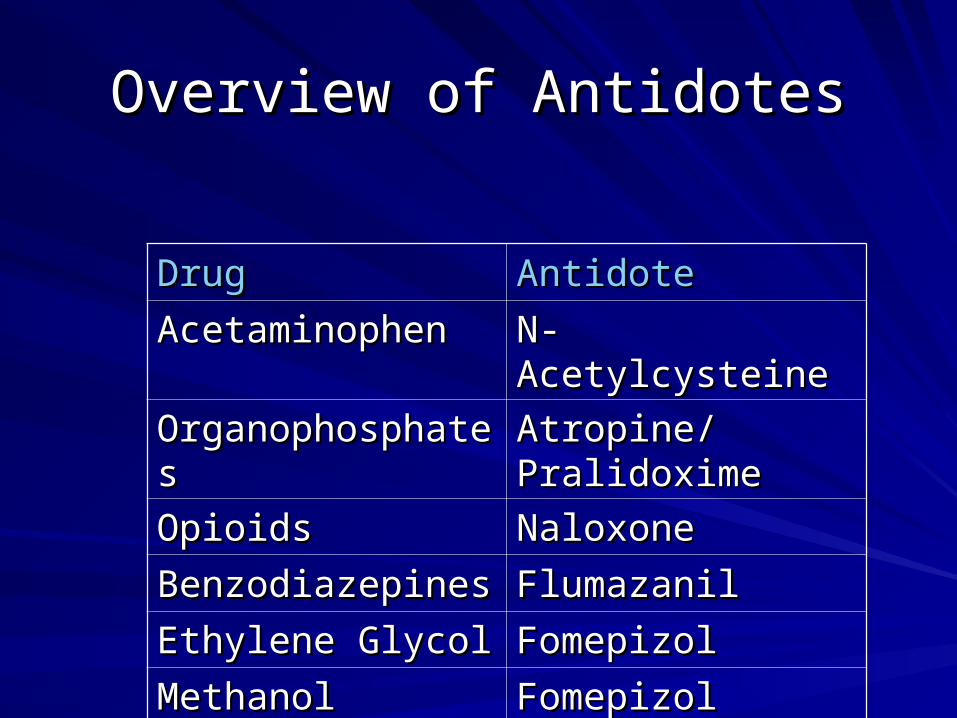
Overview of AntidotesOverview of Antidotes
DrugDrug AntidoteAntidote
AcetaminophenAcetaminophen N-AcetylcysteineN-Acetylcysteine
OrganophosphatesOrganophosphates Atropine/Atropine/PralidoximePralidoxime
OpioidsOpioids NaloxoneNaloxone
BenzodiazepinesBenzodiazepines FlumazanilFlumazanil
Ethylene GlycolEthylene Glycol FomepizolFomepizol
MethanolMethanol FomepizolFomepizol