Embed Size (px)
Citation preview

URINARY INCONTINENCE
Overview & Management
Dr. Hussam Hassan

H M Hassan
Definition of Urinary Incontinence
Involuntary loss of urine that is objectively demonstrable and that is severe enough to constitute a social or hygienic problem.

H M Hassan
ANATOMY

H M Hassan
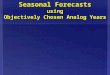
Urethra is stabilized during stress by three interrelated mechanisms
One mechanism :is reflex, or voluntary, closure of the pelvic floor
Contraction of the levator ani complex elevates the proximal urethra and bladder
neck, tightens intact connective tissue supports, and elevates the perineal body, which may
serve as a urethral backstop.

H M Hassan
The second mechanism involves intact connective tissue support to the
bladder neck and urethra The pubocervicovesical or anterior endopelvic
connective tissue in the area of the bladder neck is attached to the back of the pubic bone,
the arcus tendineus fascia pelvis, and the perineal membrane.
The pubourethral ligaments also suspend the middle portion of the urethra to the back of the pubic bone.

H M Hassan
The third mechanism mechanism involves 2 bundles of striated muscle, the
urethrovaginal sphincter and
the compressor urethrae
These muscles may aid in compressing the urethra shut during stress maneuvers
H M Hassan

H M Hassan
Hypermobility doesn’t always mean
Incontinence

H M Hassan
Urinary incontinenceEpidemiology
Although the prevalence of UI increases with age, UI should not be considered a normal part of the aging process.
For non institutionalized persons older than 60 years of age, the prevalence of UI ranges from 15 to 35 percent, with women having twice the prevalence of men
Approximately 53% of the homebound elderly are incontinent
(Urinary incontinence affects up to 7% of children older than 5 years, 10-35% of adults, and 50-84% of the elderly )

H M Hassan
CLASSIFICATION OF UI:1. Urgency Urinary Incontinence (UUI)`~22%
= involuntary leakage occurs with a strong, sudden, and uncontrollable desire to urinate as result of involuntary detrusor contraction.
2. Stress Urinary Incontinence (SUI): (49%)= involuntary leakage on effort or exertion or on sneezing or coughing, as a result of insufficient urethral closure pressure.

H M Hassan
3. Mixed Urinary Incontinence 29%= UUI + SUI marked by involuntary leakage associated with urgency and also with exertion, effort, sneezing, or coughing
4. Functional: due to reasons other than neuro-urologic and lower urinary tract dysfunction (eg, delirium, psychiatric disorders, urinary infection, reduced mobility)

H M Hassan
Transient: (Functional incontinence)Causes:
D: Delirium or acute confusion I: Infection (symptomatic UTI) A: Atrophic vaginitis or urethritis P: Pharmaceutical agents Psychological
disorders (depression, Excess urine production Restricted mobility Stool impaction
H M Hassan
Other types of UI Overflow incontinence is not a symptom or
condition but rather a term used to describe leakage of urine associated with urinary retention.
Extraurethral incontinence is the observation of urine leakage through channels other than the urethra (e.g : fistula or ectopic ureter) immediately after passing urine

H M Hassan
OCCULT STRESS INCONTINENCE
Stress incontinence on prolapse reduction is a term used to describe stress incontinence observed only after reduction of pelvic prolapse
kinking of the urethra caused by the prolapse itself provides for at least part of the continence mechanism
These patients may have a history of stress incontinence that improved and finally resolved as their prolapse worsened

H M Hassan
The diagnosis can be made by stress testing with the prolapse reduced or by pessary placement and pad testing
BUT incontinence procedures are not without their own morbidities and should not be performed unless necessary.

H M Hassan
Diagnosis
ALL Patients history, physical examination, and urinalysis. measurement of postvoid residual volume.
In selected patients:
Voiding diary Cotton swab test Cough stress test Cystoscopy Urodynamic studies Radiologic evaluation (as indicated)
H M Hassan
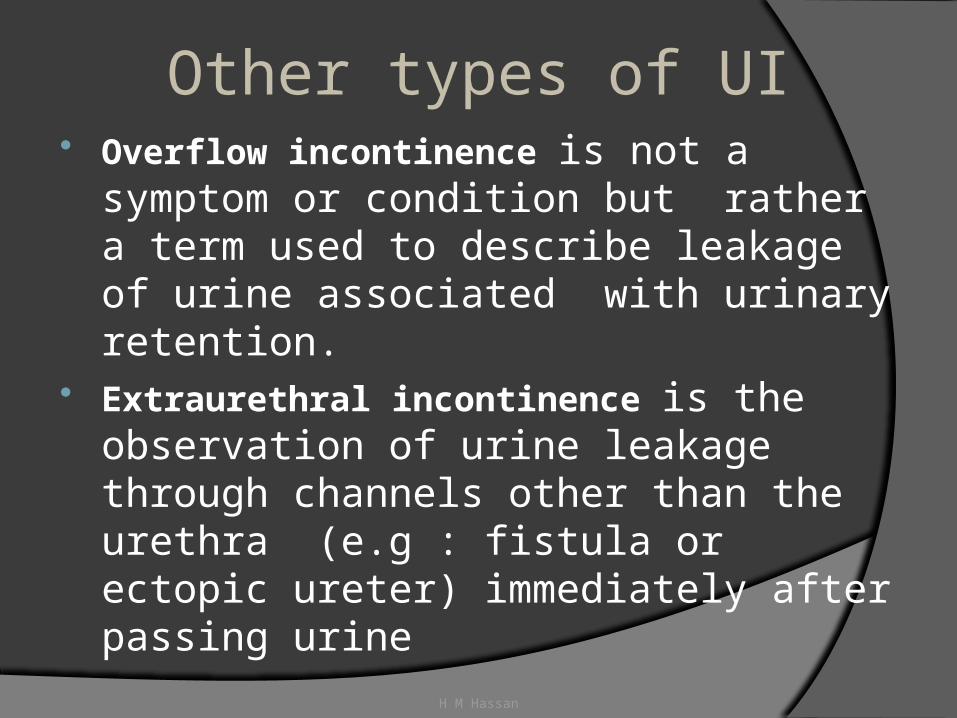
Q-tip (cotton swab) Test

H M Hassan
Criteria for further evaluation Uncertain diagnosis and inability to develop
a reasonable treatment plan
Failure to respond to the patient's satisfaction to an adequate therapeutic trial.
Consideration of surgical intervention, particularly if previous surgery failed or the patient is a high surgical risk.

H M Hassan
The presence of comorbid conditions:incontinence associated with recurrent
symptomatic UTI persistent symptoms of difficult bladder
emptying history of previous anti-incontinence surgery
or radical pelvic surgery

H M Hassan
The presence of comorbid conditions:prostate nodule, asymmetry, or other
suspicion of prostate cancer abnormal PVR urine neurologic condition, such as multiple
sclerosis and spinal cord lesions or injury Hematuria without infection.

H M Hassan
History Severity and quantity of urine lost and frequency
of incontinence episodes Duration of the complaint and whether problems
have been worsening Triggering Factors or events (eg, cough,
sneeze, lifting, bending, feeling of urgency, sound of running water, sexual activity/orgasm)

H M Hassan
History (cont…) Constant Versus Intermittent urine loss Associated Frequency, urgency, dysuria,
pain with a full bladder History of urinary tract infections (UTIS) Concomitant Fecal Incontinence or
pelvic organ prolapse Coexistent complicating or exacerbating
medical problems

H M Hassan
History (cont…)
Obstetrical history, including difficult deliveries, grand multiparity, forceps use, obstetrical lacerations, and large babies
History of PELVIC SURGERY, especially prior incontinence procedures, hysterectomy, or pelvic floor reconstructive procedures
Other urologic procedures

H M Hassan
Spinal and central NERVOUS SYSTEM SURGERY
Lifestyle issues, such as SMOKING, ALCOHOL OR CAFFEINE abuse, and occupational and recreational factors causing severe or repetitive increases in intra-abdominal pressure
MEDICATIONS

H M Hassan
Relevant complicating
Medical problems may include the following: Chronic cough
Chronic obstructive pulmonary disease (COPD)
Congestive heart failure
DIABETES MELLITUS OBESITY Connective tissue disorders
Postmenopausal HYPOESTROGENISM CNS OR SPINAL CORD DISORDERS
Chronic UTIS
Urinary tract stones Benign prostatic hyperplasia Cancer of pelvic organs

H M Hassan
Medications that may be associated with UI
Alpha-adrenergic agonists (urinary retention)Alpha-adrenergic blockers (stress
incontinence)Anticholinergic agents (urinary retention)Antidepressants (urinary retention)Beta-adrenergic agonists (urinary retention)Calcium-channel blockers (urinary retention)Diuretics (frequency)

H M Hassan
Physical Examination
A focused physical examination should be performed
Vulvae/Vagina/Urethral Meatus (hypoestrogenemia/caruncle)
Urethra
(hypermobility/tenderness/diverticulum) Pelvic Organ Prolapse

H M Hassan
Pelvic Exam Neurologic Assessment (perineal
sensation, anal sphincter tone) pulbo-cavernous reflex
Cotton Swab Test(the Q-tip will rotate >30 degrees) Pad Test(Intravesical methylene blue, oral
phenazopyridine:1g\hour-4g\24hour)

H M Hassan
Specialized diagnostic tests
Urodynamic tests. Endoscopic tests. Imaging tests.

H M Hassan
Urodynamic studies
Parameters measured during urodynamic evaluation
1. Post void residual volume (PVR)
2. Uroflow
3. Pressure flow study
4. Cystometrogram (CMG)
5. Abdominal Leak-Point Pressure (ALPP)
6. Video urodynamics

H M Hassan
Urodynamics
(UDS) is the most accurate tool available for the assessment of LUT function
UDS should be strongly considered before intervention in:
failed previous treatment or surgery mixed incontinence obstructive symptoms neurologic disease
H M Hassan
Cystoscopy
It should be performed in patients who present with: urinary urgency findings suggestive of a diverticulum or fistula Hematuria other irritative symptoms Particularly : if they have previously undergone a previous
anti-incontinence procedure pelvic radiation pelvic prolapse repair

H M Hassan
Treatment Overview Stress incontinence: Pelvic floor physiotherapy, anti-
incontinence devices, Medical treatment and surgery
Urge incontinence: Changes in diet, behavioral modification, pelvic-floor exercises, and/or medications and new forms of surgical intervention
Mixed incontinence: Pelvic floor physical therapy, anticholinergic drugs, and surgery
Overflow incontinence: Catheterization regimen or diversion
Functional incontinence: Treatment of the underlying cause

H M Hassan
Kegel Contractions
Exercises of the pelvic floor musculature 15 deliberate, quick, hard contractions of 10
second duration with 15 second intervals of muscle relaxation
3 times a day for a total of 45 contractions Approximately 6-12 weeks of exercises are
required before improvement is noted, and 3-6 months are needed before maximal
benefit is reached

H M Hassan
Medical treatmentSUI
Alpha-adrenergic Agonists: Pseudoephedrine Norepinephrine Ephedrine Hormone Duloxetine

H M Hassan
alpha-adrenergic agonists Pseudoephedrine hydrochloride is
found in cough and cold preparations and antihistamines.
Sudafed . Adult
- Nonextended release: 60 mg PO qidExtended release: 120 mg PO bid
Pediatric
- Not established

H M Hassan
Hormone
Hormone replacement therapy (HRT) maintain and restore the health of urethral tissues in women
vaginal estrogen is given at 0.5-2.0g per day.

H M Hassan
Duloxetine not approved by FDA
Balanced inhibitor of serotonin and norepinephrine reuptake
increases serotonin and norepinephrine levels in the sacral spinal cord, thereby enhancing pudendal nerve activity, which leads to increased contraction of the urethral sphincters
Duloxetine(cymbalta®) 60mg bid re-evaluated after 2-4 W A multicenter, double-blind, randomized, placebo-
controlled study in 2,758 women Reduction in IEF in 51% (drug) vs. 31% (placebo) at 6
weeks

H M Hassan
SURGERY

H M Hassan
Approaches for Stress Incontinence
Abdominal approaches○ Retropubic colpo-suspension
BurchMarshall-Marchetti-Krantz (MMK)
Contemporary○ Pubo-vaginal sling○ Tension free vaginal tape (TVT)○ Trans-obturator tape (TOT)

H M Hassan
Retropubic Colpo-suspension

H M Hassan

H M Hassan
MMK BURCH

H M Hassan

H M Hassan

H M Hassan
Tension Free vaginal Taping (TVT):
Through a small vaginal incision, permanent mesh-like material is placed underneath the urethra and anchored to the abdominal muscles above the pubic bone.
General anesthesia or local anesthesia is required.
Advantages Less invasive, Small incisions- Local anesthesia Same day or overnight surgery stay Return to work in 2 - 3 weeks

H M Hassan

H M Hassan
Transobturator Sling (TOT) The transobturator sling (tot sling) is subfascial, ie
the needle or the sling NEVER enters the retropubic space.

Monarc Needle Design TOT
Helical Needles
H M Hassan

H M Hassan
Transobturator Landmarks
Obturator canal
Urethra
SAFE ENTRY ZONE of MONARC
NEEDLE
Adductor longus

H M Hassan
Monarc Needle Passage

H M Hassan
Monarc Mesh PositionSPARC/TVT

H M Hassan
TVT-O

H M Hassan
Mini Arc

H M Hassan
TVT-S

H M Hassan
MiniArc(TVT-s) Data
Kennelly M et al. J Urol (In Press) Multi-center study with 188 patients and 12 month
follow-up Mean operative time – 11 minutes Mean length of stay – 9.5 hours Mean pain score (0-10) at discharge – 1.3
Cough-stress Test negative in 90.6 % One-hour PWT < 1 g in 84.5 % Adverse events included UTI (4.3%), temporary
retention (3.2%), dyspareunia (2.1%) and vaginal extrusion (2.1%)

H M Hassan
The meta-analysis by Jarvis which reviewed over 20 000 patients who had undergone the procedures
Procedure First procedure (%) Recurrent incontinence (%) Bladder buttress 67.8 ND MMK 89.5 ND Burch colposuspension 89.8 82.5 Bladder neck suspension 86.7 86.4 Slings 93.9 86.1 Injectables 45.5 57.8

H M Hassan
Retropubic vs Transobturator
•2010 multi-center trial with 12-month follow-up Equivalent objective success Transobturator approach has more leg
weakness/ groin numbness Retropubic approach has more bladder injuries
and de novo voiding dysfunction TVT exhibited higher incidence of bladder
perforation (7% vs. 0%) and more postoperative voiding dysfunction (Barber et al 2008)

H M Hassan

H M Hassan
Complications:
Difficulty urinating and incomplete emptying of the bladder (urinary retention), although this is usually temporary
Urinary tract infection Difficult or painful intercourse Bladder injury in the two national registries ranges from
2.7% to 3.8%. Hemorrhage is relatively rare vaginal, urethral, and intravesical erosion The erosion rate reported in the literature for
polypropylene mesh is 0.5% to 1.3%

H M Hassan
Surgery Keypoints Surgery does not restore the same mechanism
of continence. BUT a compensatory approach
The surgeon’s preference, coexisting problems, and anatomic features and general health condition
There is lack of a clear consensus as to which procedure is most effective but contemporary practice is shifting to the “loose” urethral sling

H M Hassan
MMK, placement of sutures through the pubic symphysis incurs the risk of osteitis pubis in 0.9% to 3.2% of patients
The Burch should be regarded as the standard open retropubic procedure for incontinence in primary or secondary surgery with proven long-term success

H M Hassan
The risk of temporary urinary retention lasting more than 4 weeks postoperatively is 5% for all retropubic suspensions
All patients should be counseled before surgery about the potential need for intermittent self-catheterization

H M Hassan
Burch may aggravate posterior vaginal wall weakness, predisposing to enterocele.
Most studies have not demonstrated a significant difference between (Burch) and pubovaginal slings.
At this time, the TVT procedure appears to be at least equivalent to the Burch and in general is probably better.

H M Hassan
Bulking Agents For the treatment of low-threshold stress
incontinence Collagen (bovine) and Durasphere
(carbon-coated beads) typically employed in past
Coaptite (Calcium hydroxyl petite) Introduced via intra-urethral or peri-urethral
injection Improvement seen in approximately 70% of
patients

H M Hassan

H M Hassan
Indicated when surgery fails to correct stress incontinence.
Post radical Prostatectomy
The device consists of a cuff which is placed around the bladder neck.
A balloon reservoir, containing fluid is placed in the peritoneal cavity or under the anterior rectus sheath, and a small pump is situated in one labium major (scrotum)
Artificial Urinary Sphincter

H M Hassan

H M Hassan
Under normal conditions the cuff is full with fluid thus closing the bladder neck.
When voiding is desired the pump is pressed to force the fluid in the cuff to go back into the balloon reservoir so that voiding can occur.
The cuff then gradually refills over the next few minutes.

H M Hassan
AUS Much longer mean follow-up 3 to 7.7 years •Continent (0-1 pads) –59-91% •Complications –Urethral atrophy 4-10%,
erosion 4-10%, infection 1-14%, mechanical failure 0-29%
•Most revisions are within first 36-48 months
•Long-term mechanical failure rate: 36% at 10 years

H M Hassan
Medscape Updated: Oct 7, 2013 CAMPBELL-WALSH UROLOGY, TENTH EDITION 2012
THANKS FOR LESTINING

H M Hassan