Embed Size (px)
Citation preview
Overview of Behavioral and Mental Health in Alaska
Gregg Knutsen, MSChair, Planning and Community Relations Committee, Anchorage/Fairbanks Community Mental Health Services Board of Directors
Jerry Jenkins, M.Ed., MACChief Executive Officer, Anchorage/Fairbanks Community Mental Health ServicesPresident, Alaska Behavioral Health Association
Mental Illness, Substance Abuse – Behavior Health
Will pay for services somewhere – direct, indirect
Identifiable Life versus Statistical Life
Recovery and Growth
Investing in programs during a recession
Government’s Role versus Government Efficiency
Access and Intensity of Services: Unable to see costs rise significantly
Early less cost better out
Continuum of Care
June 2, 2017Jenkins/Knutsen 2
Concepts and MessageHow do we deal with the inner drama of being human?
Mental health is “a state of well-being in which the individual:
Realizes abilities,
Cope with the normal stresses of life,
Can work productively and fruitfully, and
Able to make a contribution to his or her community.”
It is estimated that only about 17% of U.S adults are considered to be in a state of optimal mental health.
Definition: Mental Health
June 2, 2017Jenkins/Knutsen 3
Behavioral medicine is an interdisciplinary field combining both medicine and psychology
Concerned with the integration of knowledge in the:
Biological,
Behavioral,
Psychological, and
Social sciences relevant to health and illness.
There is emerging evidence that positive mental health is associated with improved health outcomes.
June 2, 2017Jenkins/Knutsen 4
Definition: Behavioral Health
Mental Health
All mental disorders are behavioral disorders
Not all behavioral disorders are mental disorders.
Behavioral Health
Downstream of Mental Health
Behaviors may contribute like lack of exercise, diet, habits
June 2, 2017Jenkins/Knutsen 5
Mental and BehavioralHealth Differences
Usually psychological factors (internal factors) dominate in mental disorders
Behavioral disorders physiological and sociological factors (external factors) may dominate.
Marriage/family counseling
Addiction treatment
Services providers: social workers, counselors, psychiatrists, neurologists, or physicians
Continuum of prevention, intervention, treatment and recovery support services
June 2, 2017Jenkins/Knutsen 6
Behavioral and Mental HealthCommonality and Overlap
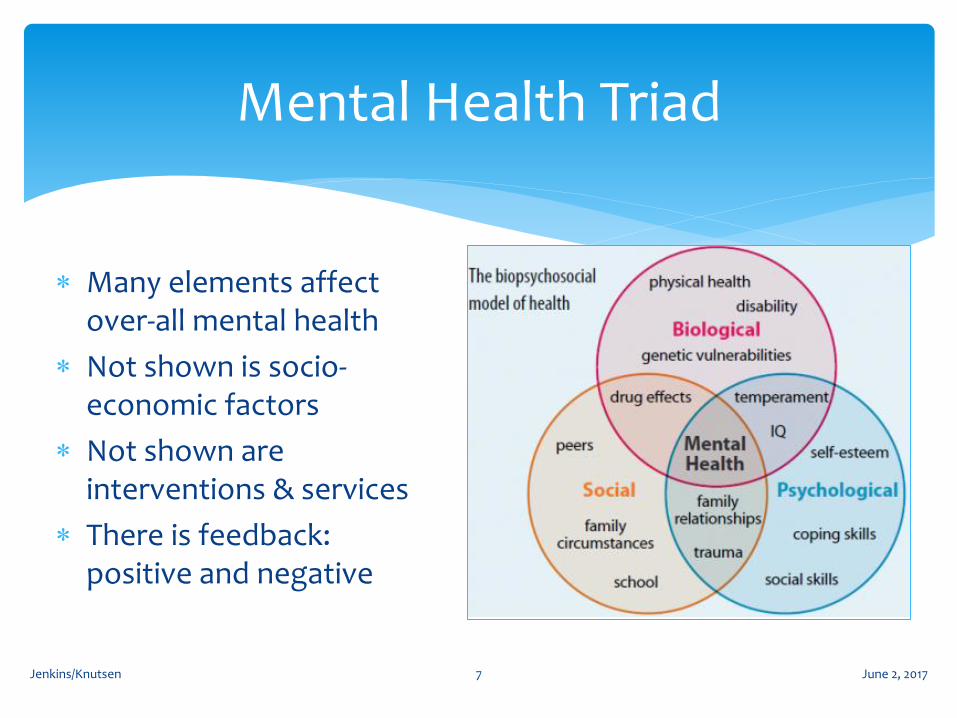
Mental Health Triad
June 2, 2017Jenkins/Knutsen 7
Many elements affect over-all mental health
Not shown is socio-economic factors
Not shown are interventions & services
There is feedback: positive and negative

Social & Economic Impacts
June 2, 2017Jenkins/Knutsen 8
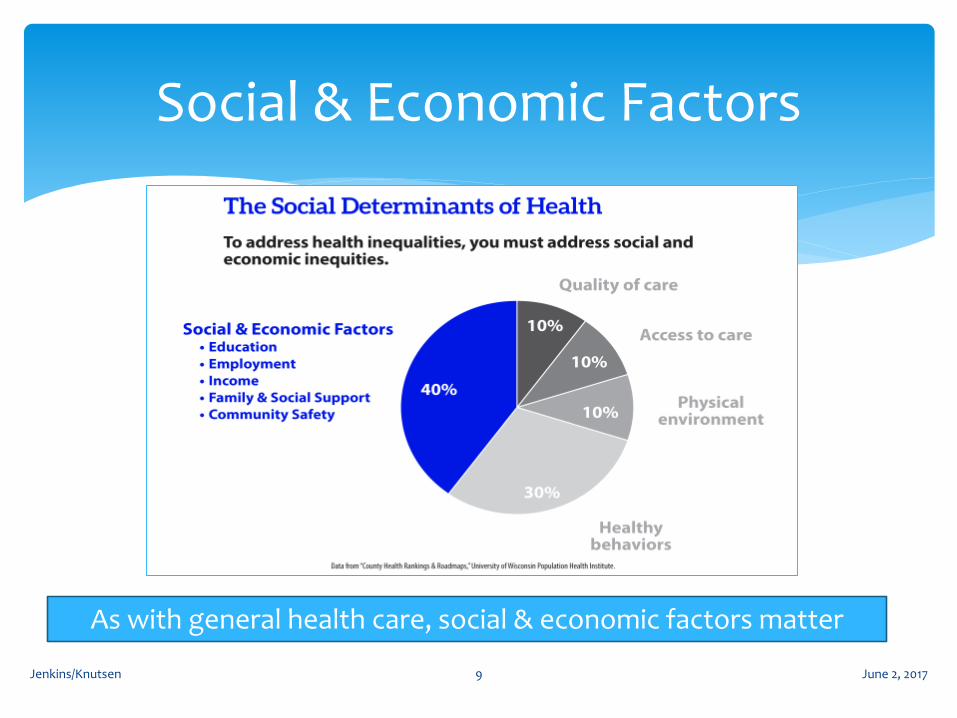
Social & Economic Factors
June 2, 2017Jenkins/Knutsen 9
As with general health care, social & economic factors matter
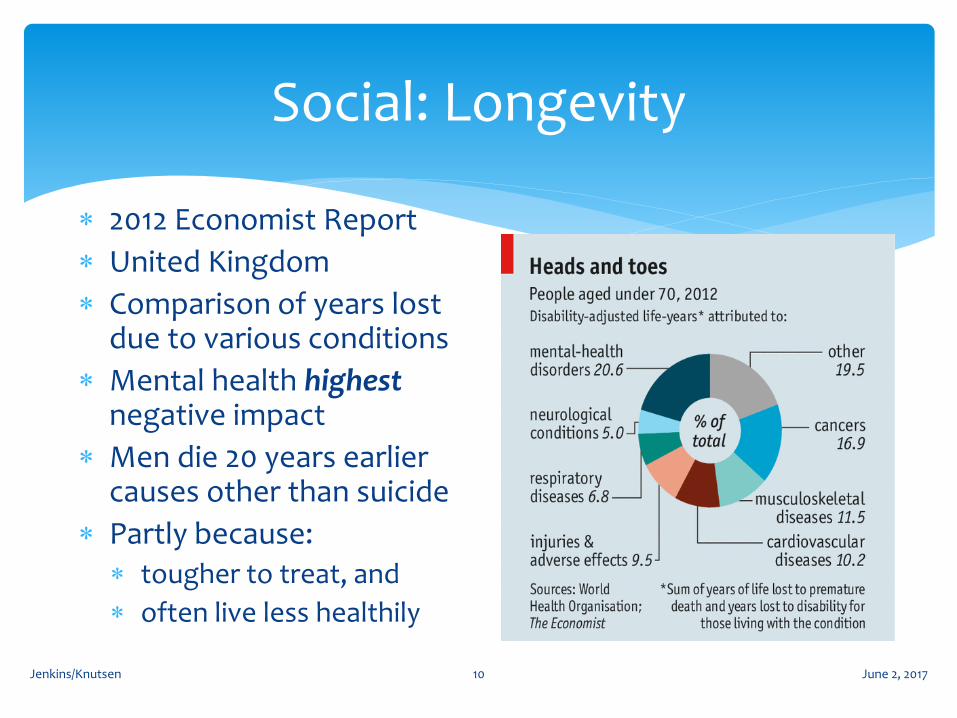
Social: Longevity
June 2, 2017Jenkins/Knutsen 10
2012 Economist Report
United Kingdom
Comparison of years lost due to various conditions
Mental health highestnegative impact
Men die 20 years earlier causes other than suicide
Partly because: tougher to treat, and
often live less healthily
June 2, 2017Jenkins/Knutsen 11
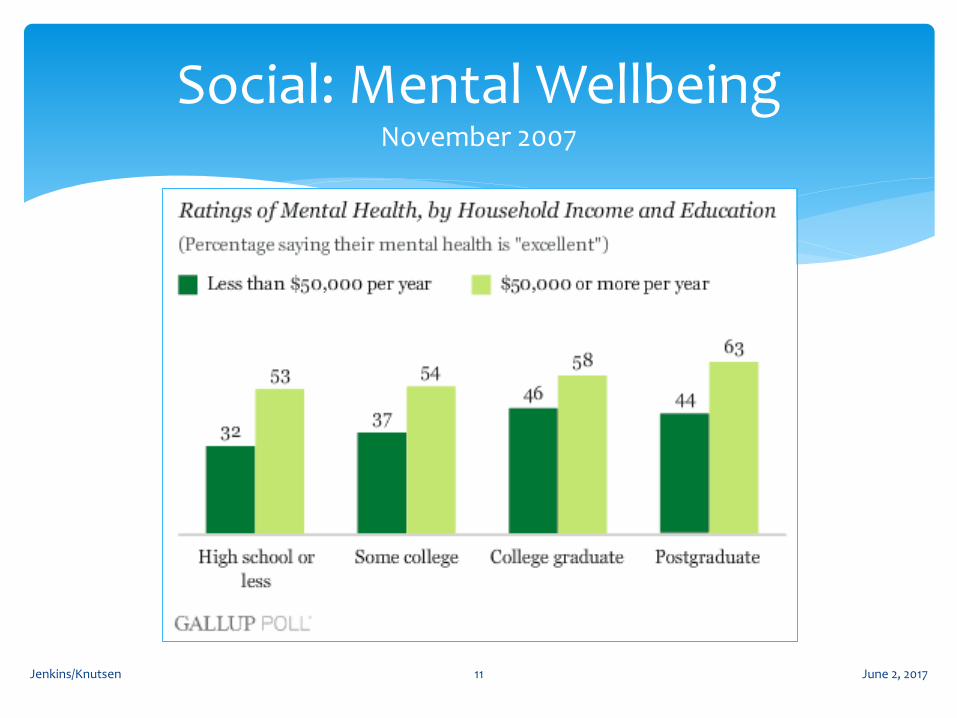
Social: Mental WellbeingNovember 2007
Estimates from several rich countries put the economic cost of mental illness at 3-4% of GDP.
Economist, 2012
“The economic cost of mental illness will be more than cancer, diabetes, and respiratory ailments put
together.”
Thomas InselDirectorNational Institute of Mental Health, USADavos, 2015
June 2, 2017Jenkins/Knutsen 12
Estimated Total Costof Mental Illness
Comparison of Severe Mental Illness (SMI) and no SMI (National Institute Mental Health) SMI episode serious impairment at least 30 days
Without SMI ≈ $38,853 annually
With SMI ≈ $22,545 annually
Societal loss estimated $192.3 Billion
The total loss is combination of: 75% income income reduction
25% no income
June 2, 2017Jenkins/Knutsen 13
Earnings Impacts (2008)

Intervention and Treatment: Location & Timing
June 2, 2017Jenkins/Knutsen 14
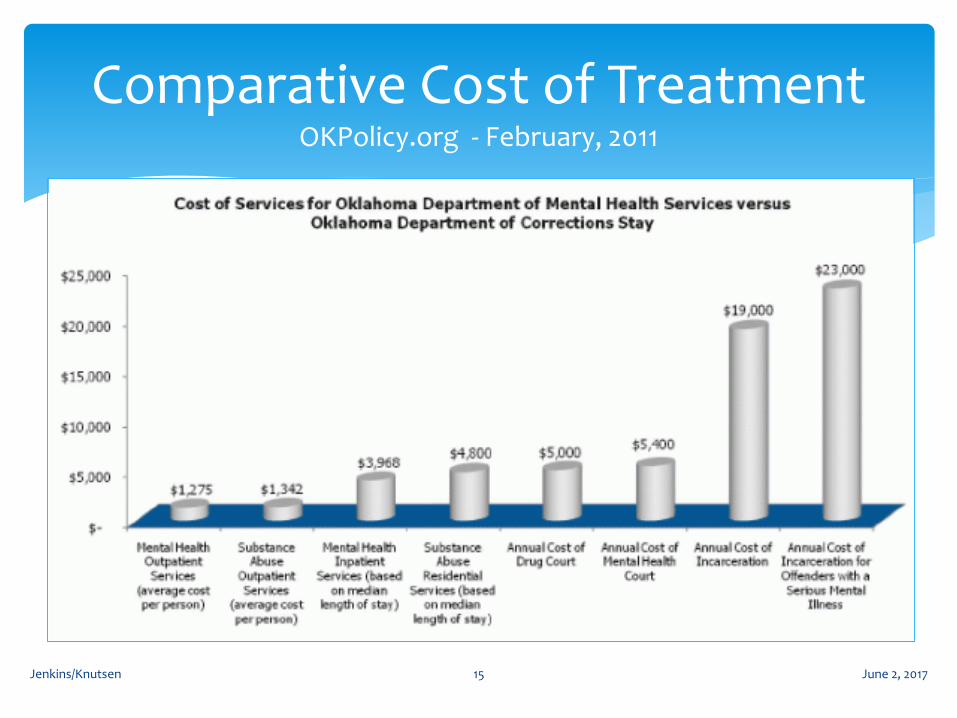
June 2, 2017Jenkins/Knutsen 15
Comparative Cost of TreatmentOKPolicy.org - February, 2011
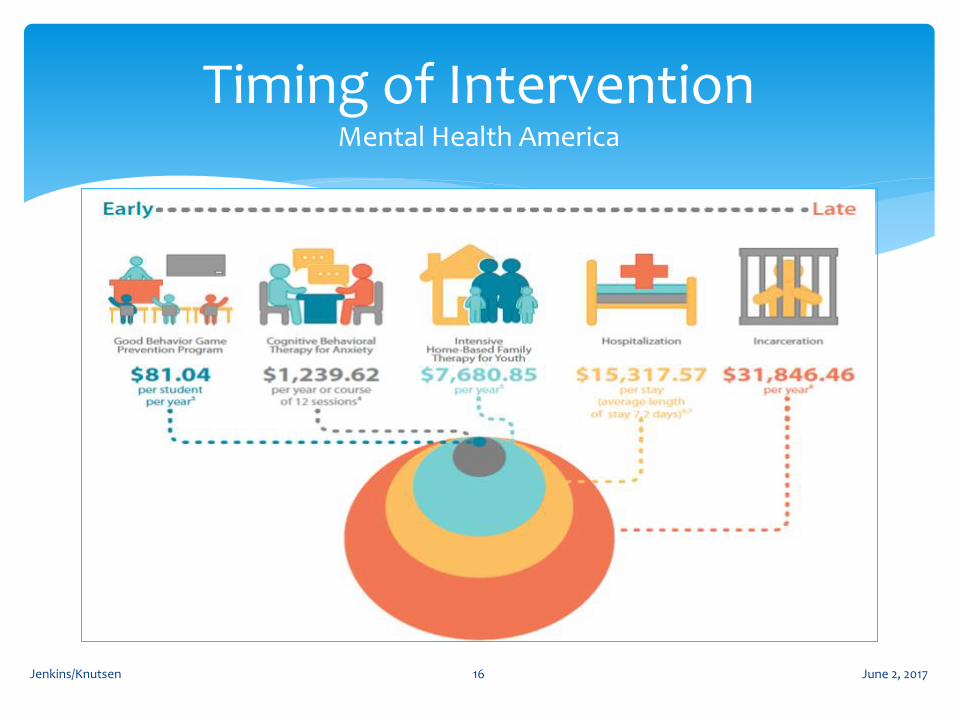
June 2, 2017Jenkins/Knutsen 16
Timing of InterventionMental Health America
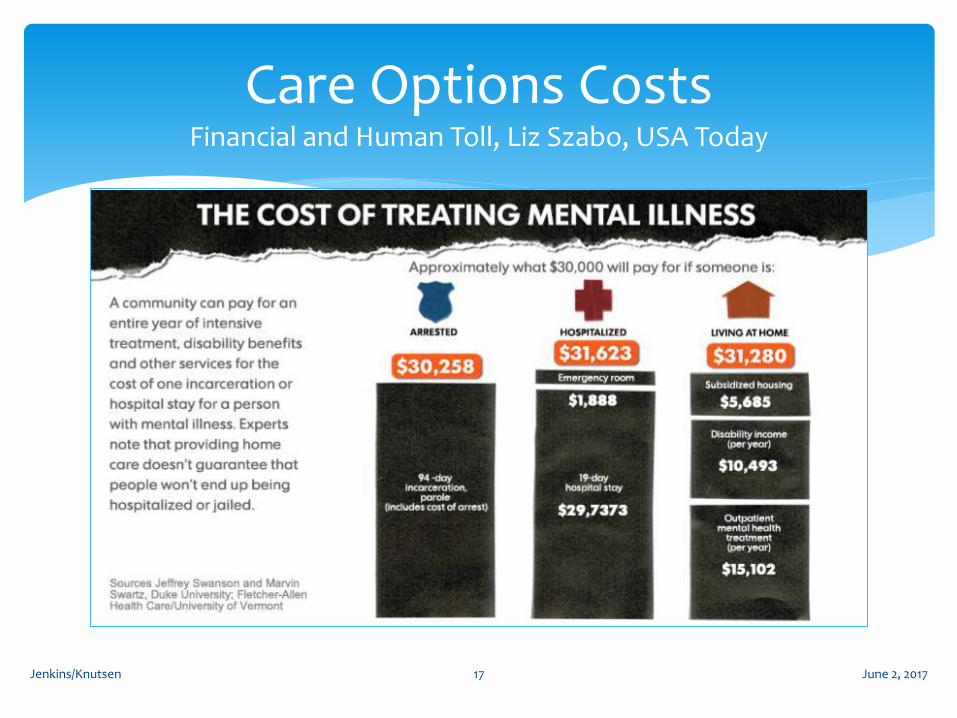
June 2, 2017Jenkins/Knutsen 17
Care Options CostsFinancial and Human Toll, Liz Szabo, USA Today
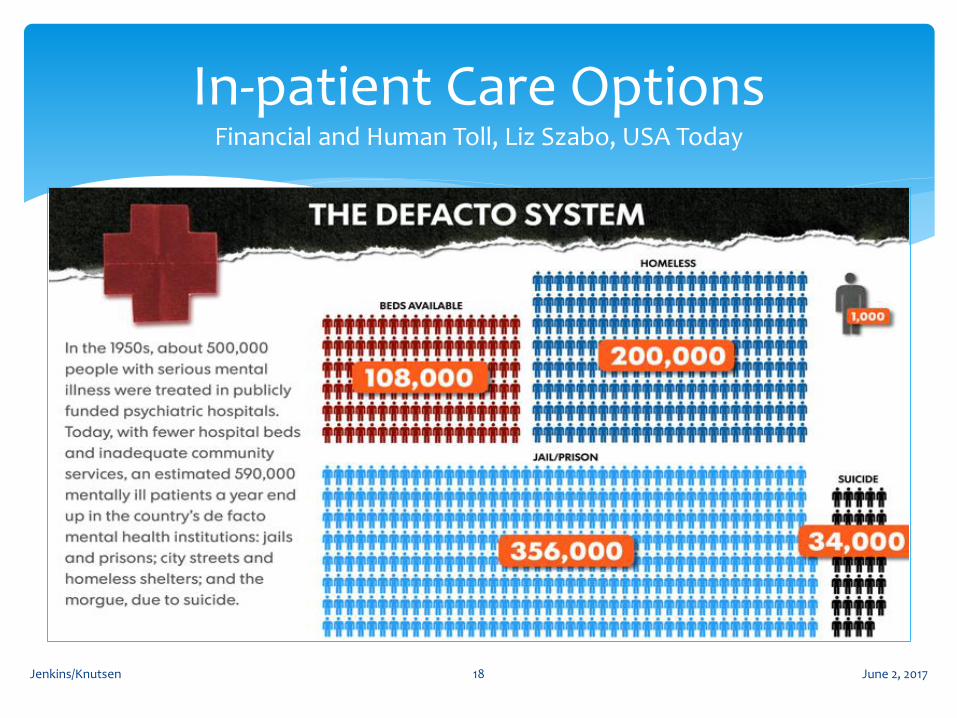
June 2, 2017Jenkins/Knutsen 18
In-patient Care OptionsFinancial and Human Toll, Liz Szabo, USA Today
Alaska Specific Information
June 2, 2017Jenkins/Knutsen 19
± $260 Million
(2013)
Federal
State
June 2, 2017Jenkins/Knutsen 20
Funding SourcesRelative Size ≈ Amount of Dollars
“Remember, we will pay for untreated mental illness and substance use disorders somewhere!”
So sayeth Jerry Jenkins – 2 June 2017
June 2, 2017Jenkins/Knutsen 21
Funding -What are we buying?
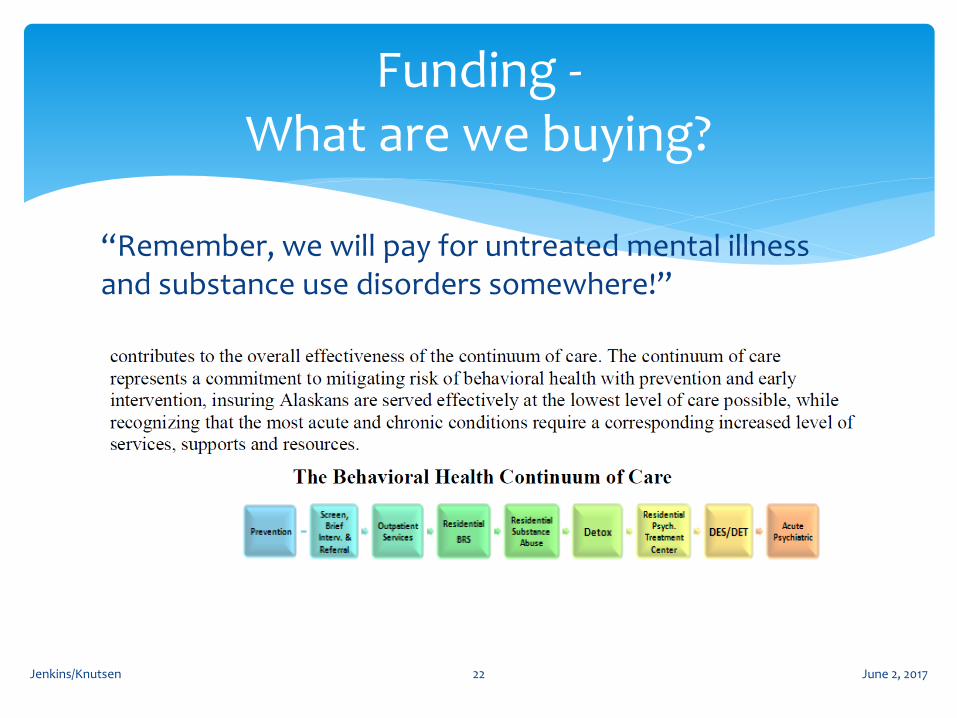
“Remember, we will pay for untreated mental illness and substance use disorders somewhere!”
So sayeth Jerry Jenkins – 2 June 2017
June 2, 2017Jenkins/Knutsen 22
Funding -What are we buying?
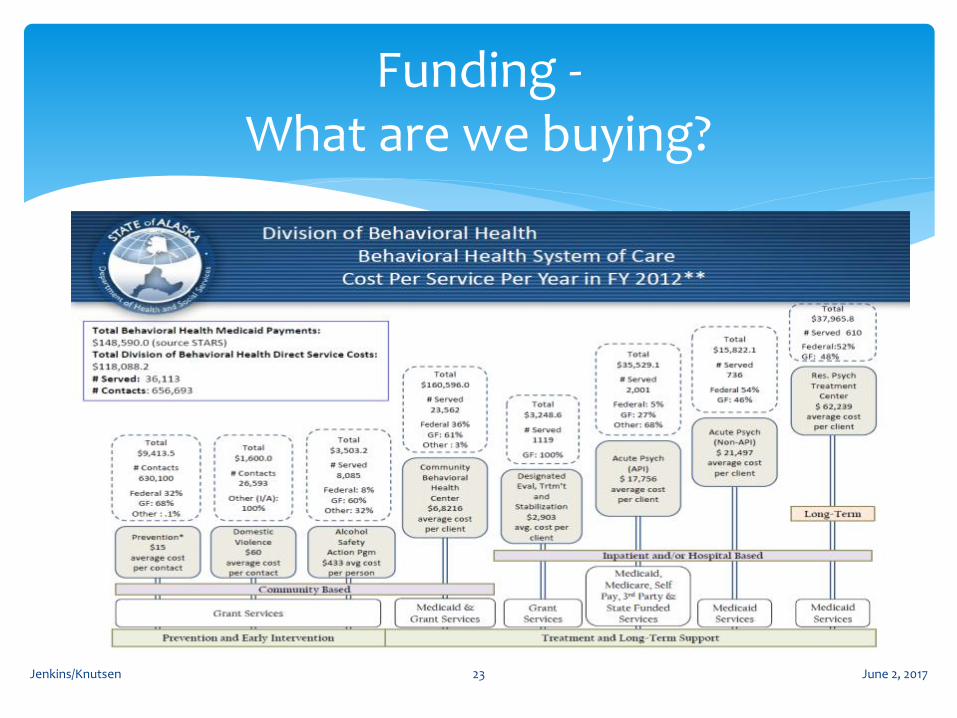
June 2, 2017Jenkins/Knutsen 23
Funding -What are we buying?
June 2, 2017Jenkins/Knutsen 24
Funding -What are we buying?
Gaps in system are resulting in additional utilization of more intense services.
June 2, 2017Jenkins/Knutsen 25
Funding Sources
Indian Health Services (IHS) 100% Federal Medicaid Assistance Percentage (FMAP) -Matching) Rates adjusted annually – encounter rate – D. Morgan is the resident expert. State regulated under auspices of Medicaid and state grants - “Self-determining” in
light of proposed administrative support organization (ASO) – aka managed care Grants: Federal and State including IHS funding. Third party insurance including Medicare; self pay
VA/DOD
Non-IHS (private for profit and non-profit; government; schools)
50% FMAP since 2010 88% Denali Kid Care (DKC) negotiated No regular rebasing of Alaska Medicaid rates. State regulated Grants: Federal and State Third party insurance including Medicare; self pay
June 2, 2017Jenkins/Knutsen 26
Funding Sources
Federal Sources: Indian Health Services
Federally Qualified Health Clinics
Medicaid (TEFRA, CHIP/DKC), Medicare, Tricare
Grant Funding for Specific Programs (HUD; HHS; USDA, DOJ, etc.)
State Sources: CAMA – Chronic and Acute Medical Assistance
Grants (GF, UGF, DGF)
SOA Employee Insurance
Private Sources – 3d party insurance, EAP
No insurance - out-of-pocket or charity care (EMTALA –Emergency Medical Treatment and Labor Act)
Southcentral Foundation– Indian Health Services (IHS)
Peninsula Community Health Services – Fed Qualified Health Clinic (FQHC)
Arc of Anchorage – Medicaid, multiple types (DD; MI), donations
Counseling Solutions of Alaska – Private Insurance, Out-of-pocket
Nugen’s Ranch – Grant Funded (IMD exclusion)
ACMHS/FCMHS – Various, Comprehensive Behavioral Health Treatment and Recovery (CBHTR) Grant – 50 funding streams.
Department of Corrections – State of Alaska – largest provider of mental health services in AK?
June 2, 2017Jenkins/Knutsen 27
60 + Service Providers: Samples
It is complicated trying to describe the Alaska behavioral healthcare system because it is complicated.
“Remember, we will pay for untreated mental illness and substance use disorders somewhere!”
So sayeth Jerry Jenkins – 2 June 2017
June 2, 2017Jenkins/Knutsen 28
June 2, 2017Jenkins/Knutsen 29
Walk-ins – Same day access – very limited in AK.
Referrals
Family and friends,
Employer,
Other providers like API, North Star, DOC
Civil Commitment
Criminal Justice System (DOC; Mental Health Court)
Emergency Medical Services – SB 74 – 5days for either primary care or behavioral health
June 2, 2017Jenkins/Knutsen 30
Access to Services
Stigma
Lack of ‘same day access’ or any access like detox
Lack of information about where to get services (211)
Transportation within local community
Geography and Weather
June 2, 2017Jenkins/Knutsen 31
Barriers to Services
Demand for Services Improving treatment:
Comorbidity is the norm – medically complicated
Resistance to effective clinical management (refuse meds, miss appointments due to limited transportation, don’t follow through on treatment plan) – just like other illnesses.
Acute/crisis focused often versus long-term support
System capacity:
Over capacity resulting in long waits for services and
Limited availability of services within communities
Limited or no same day services except ER
Workforce
June 2, 2017Jenkins/Knutsen 32
Challenges to the System
Workforce: Administrative and Clinical Talent
Recruiting and Retaining
Competitive compensation and benefits help.
High Stress due to nature of the work - It is not for everyone!
Documentation and Record Keeping demands-
Funding required documentation
Regulatory training and record keeping – highly audited
Turnover: train and then brain drain to private practice
Necessity to utilize locum tenens prescribers – migrant workers
Lack of routine rebasing for non-IHS providers.
June 2, 2017Jenkins/Knutsen 33
Challenges to the System (Continued)
Cost of Services
June 2, 2017Jenkins/Knutsen 34
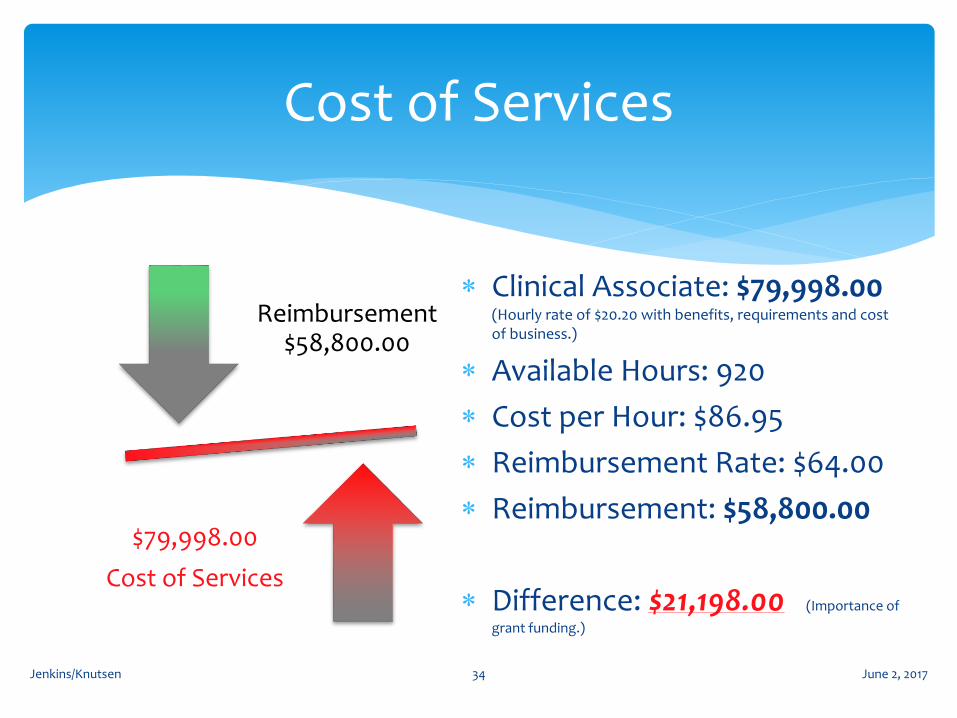
Reimbursement $58,800.00
$79,998.00
Cost of Services
Clinical Associate: $79,998.00 (Hourly rate of $20.20 with benefits, requirements and cost of business.)
Available Hours: 920
Cost per Hour: $86.95
Reimbursement Rate: $64.00
Reimbursement: $58,800.00
Difference: $21,198.00 (Importance of
grant funding.)
Summary
June 2, 2017Jenkins/Knutsen 35
June 2, 2017Jenkins/Knutsen 36
It is complicated trying to describe the system because it is complicated.
And, “Remember, we will pay for untreated mental illness and substance use disorders somewhere!”
So sayeth Jerry Jenkins – 2 June 2017 So sayeth Jerry Jenkins – 2 June 2017
Gaps in system result in additional utilization of more
intense/higher costing services.
Fill gaps and use telephone/technology triage.
Use 211 for steerage.
Supporting Office of Children’s Services
Identifying mentally ill departing Department of Corrections
and linking to services.
Identifying and connecting Division of Juvenile Justice
releases to community services.
(BTW, they normally do a good job.)
Opportunities
This need in Alaska continues to grow
Behavior/Mental Health services cannot fix all of the
“Inputs”; can mitigate and treat
Can positively affect the Outcomes: interrupt the cycle
Universal Concern: the inner drama of being Human
More investment in behavior/mental health services
Saves lives, families, and communities
Improves over-all health and well being – avoids other costs
June 2, 2017Jenkins/Knutsen 38
Summary
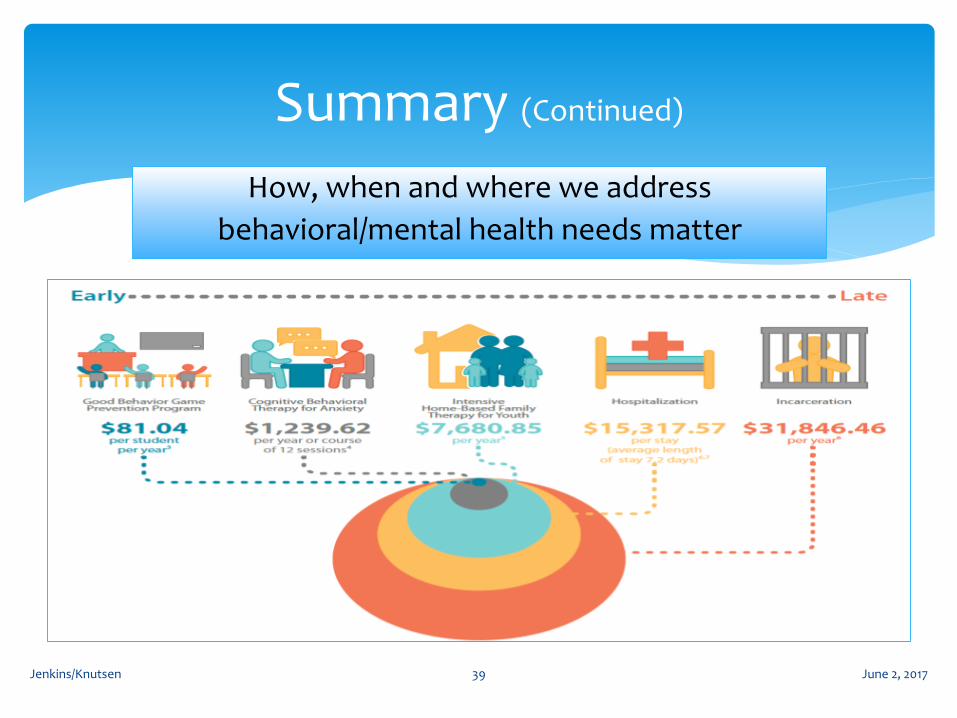
How, when and where we address
behavioral/mental health needs matter
June 2, 2017Jenkins/Knutsen 39
Summary (Continued)
June 2, 2017Jenkins/Knutsen 40
Summary (Continued)
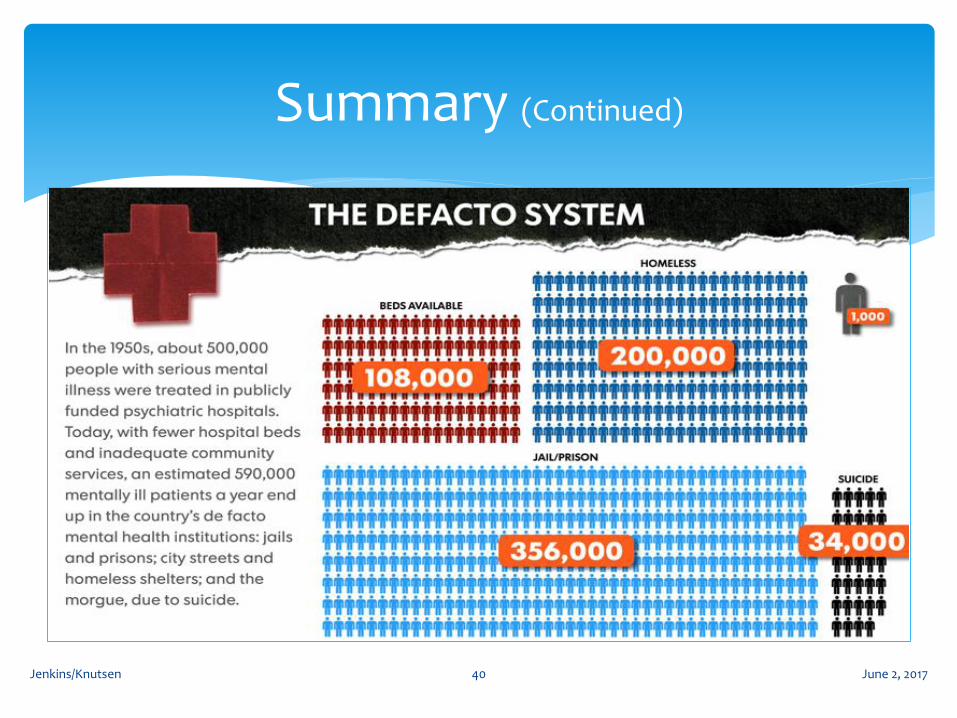
To save money – change the De Facto system
Continue to educate and inform Alaskans about the dynamics of behavioral and mental health issues
All service segments are inextricably linked
Swim against the tide and increase funding for all service providers
There are real and measurable economic and financial benefits to gain with improved services
June 2, 2017Jenkins/Knutsen 41
Summary (Continued)





























