Embed Size (px)
Citation preview

Overview of Myelodysplasia and New Harmonized CIBMTR Forms
Corey Cutler, MD MPH FRCPCAssistant Professor of Medicine
Harvard Medical SchoolDana-Farber Cancer Institute

Hematopoiesis
Hematopoiesis – the process by which blood cells are madePluripotent Hematopoietic Stem Cell – able to develop into any type of blood cell

Primary Myelodysplastic Syndromes
A group of hematopoietic disorders sharing an ineffective production of one or more myeloid cell lines
Ineffective hematopoiesis : Anemia, Thrombocytopenia and Neutropenia
Dysplastic hematopoiesis: Recurrent cytogenetic abnormalities arising from dysplastic clones
MDS encompasses several different, but related, conditions and in some instances may be mistaken for aplastic anemia or a myeloproliferativedisease
Median age is 70 and 30% progress to AML

Leukemia Stats: 2004/USA
Cell Type Child Adult Total AML 1,000 9,400 10,400 ALL 3,000 1,300 4,300 CML 120 4,400 4,520 CLL - 11,000 11,000 MDS 1,000 12,000 13,000 Totals 5,120 38,100 43,220
MDS Prevalence: 35 000 – 55 000 cases in USA

Age-Related Incidence of MDS
0 0 2 1 2 2 49
16
26
5259 61
34
10
10
10
20
30
40
50
60
70
20- 25- 30- 35- 40- 45- 50- 55- 60- 65- 70- 75- 80- 85- 90- 95-
Williamson PJ, et al. Br J Haematol. 1994 Aug;87(4):743-5.
Age
Age-specific incidence rates (per 100,000)
Less than 50 0.550-59 5.360-69 1570-79 4980 and over 89

Presenting Symptoms
Easy bruisability and bleeding, Spontaneous hemorrhage when severe.Thrombocytopenia
Susceptibility to infections increased; recurrent feversNeutropenia
Pallor, severe fatigue, shortness of breath; angina or heart attack
Severe anemia: Hct < 25%
Some fatigue, palpitations, shortness of breath, pallor
Mod. anemia: Hct 25-30%
Normal or slightly fatiguedMild anemia: Hct 30–35%
Anemia
• Patients with MDS present with signs and symptoms of bone marrowfailure –anemia, neutropenia and thrombocytopenia
• Nearly half of all patients with MDS may have no symptoms at all• Abnormal blood counts are noted on routine examination


Predisposition
Acquired:SenescenceMutagen/Genotoxic Stress
Therapeutic alkylators, Topo-II agents, β-emitters (32P), autoSCTEnvironmental/occupational (herbicides; pesticides; heavy petrochemical exposure) NQ01 polymorphismsTobacco
Aplastic anemiaPNH
List AF, et al. The Myelodysplastic Syndromes. In: Wintrobe’s Hematology 2003.
Heritable:Constitutional genetic disorders
Trisomy 8 mosaicismFamilial monosomy 7
Neurofibromatosis 1Embryonal dysgenesis (del12p)Congenital Neutropenia
Kostmann, Schwachman-DiamondDNA repair deficiencies
Fanconi anemia, AT, Bloom syndrome
Pharmacogenomic polymorphisms (GSTq1-null)

Exposures
Alkylating agentsRadiation
Long Latency80% with–5 (del 5) and/or MDS/AML–7 (del 7) + othersdel (3p), del (17p)
Topoisomerase II t(8;21)
(Etoposides, anthracyclines)t(15;17)
AML1 gene (21q22)
q11ALL (MLL genes)11q23
Short Latency


•Morphologic: FAB (1982)
•Prognostic: IPSS (1997)
•Combined (morphologic, cytogenetic and prognostic): WHO (2001)
Classification of MDS
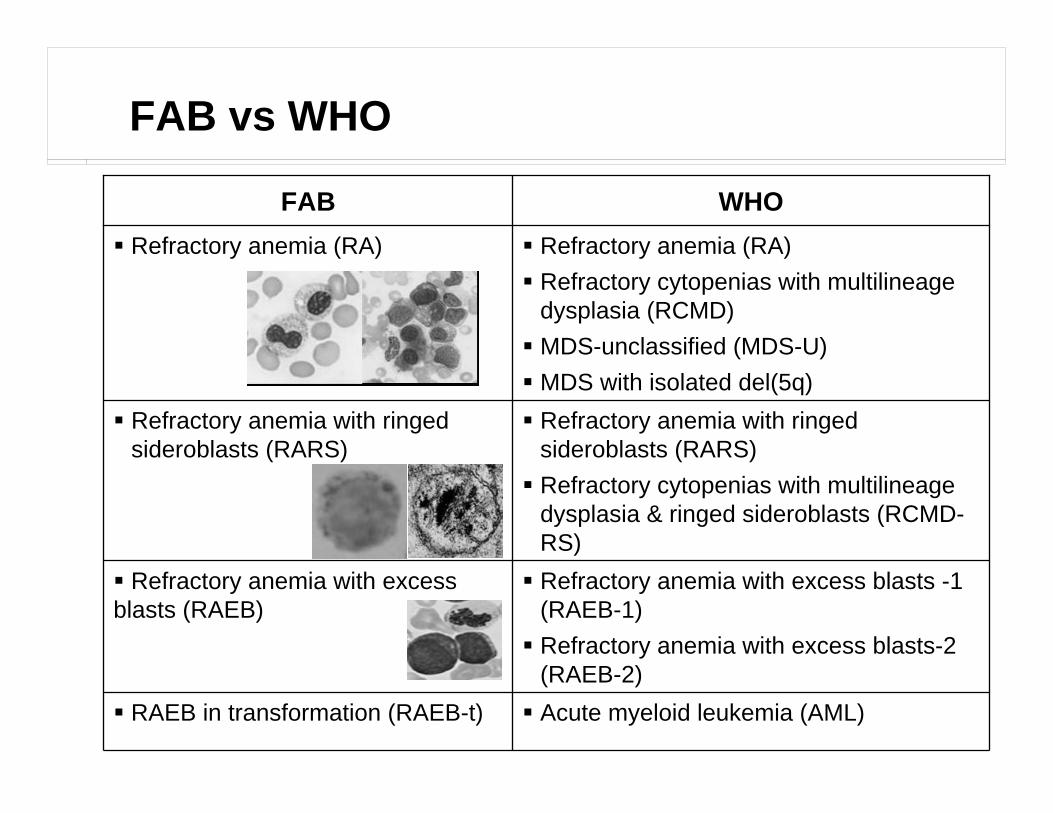
Acute myeloid leukemia (AML)RAEB in transformation (RAEB-t)
WHOFAB
Refractory anemia with excess blasts -1 (RAEB-1)Refractory anemia with excess blasts-2 (RAEB-2)
Refractory anemia with excess blasts (RAEB)
Refractory anemia with ringed sideroblasts (RARS)Refractory cytopenias with multilineagedysplasia & ringed sideroblasts (RCMD-RS)
Refractory anemia with ringed sideroblasts (RARS)
Refractory anemia (RA)Refractory cytopenias with multilineagedysplasia (RCMD) MDS-unclassified (MDS-U)MDS with isolated del(5q)
Refractory anemia (RA)
FAB vs WHO

WHO Classification of MDS - Modifications
t(8;21) - AML1/ETO
t(15;17) - PML/RARα
inv(16) or t(16;16) -CBFβ/MYH11
11q23 (MLL)
Reclassification:
CMML MPD
RAEB-t
Irrespective of % Blasts are considered as AML:
Acute myeloidleukemia withmultilineagedysplasia
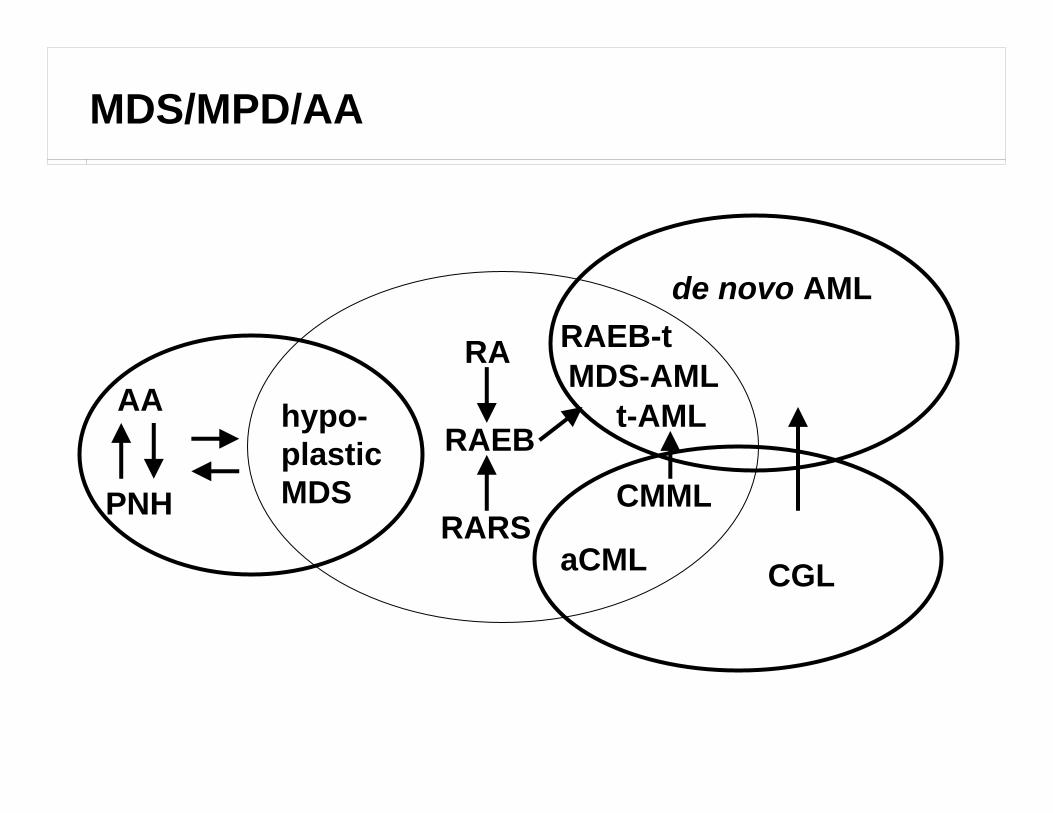
PNH
AA
CMML
aCML
MDS-AMLRA
RAEB
RARS
hypo-plasticMDS
de novo AML
CGL
RAEB-t
t-AML
MDS/MPD/AA

BONE MARROW BIOPSY:
Markedly hypercellular marrow (5% fat).Approximately 10-15% of the cellularity is comprised of intermediate sizedmononuclear cells with round nuclei, dispersed chromatin, distinct prominentnucleoli, consistent with blast forms as confirmed by immunoperoxidase studiesperformed on paraffin sections for CD34.Erythroid elements are mildly proportionally increased, exhibit maturation andinclude increased number of early forms.Myeloid elements are mildly proportionally decreased, exhibit maturation andinclude an increased number of early forms.Megakaryocytes are present in normal numbers and include occasional smallhypolobated forms.Scattered lymphocytes and plasma cells are seen.Bone trabeculae exhibit focal osteoblastic activity.Giemsa stain examined for final diagnosis of bone marrow biopsy.The aspirate smear findings are of a markedly hypercellular, spicular smearshowing maturing trilineage hematopoiesis, increased numbers of blasts,moderate dyserythropoiesis, and mild dysmyelopoiesis. Myeloid and erythroidelements are markedly left-shifted. Marked erythroid hyperplasia is present.
Overall, the findings are consistent with persistent involvement by thepatient's MYELODYSPLASTIC SYNDROME, best characterized as refractory anemiawith excess blasts (RAEB-2).



KARYOTYPE: 44,XY,add(3)(p11),del(5)(q14),-7,inv(9)(p12q13),psudic(12)t(12;18) (p12-13;p12),der(16)t(3;16)(p11;q24)[cp12]/46,idem,-3,del(22)(q22),+2mar[cp8]
METAPHASES COUNTED: 20 ANALYZED: 10 SCORED: 10 BANDING: GTG
INTERPRETATION:All metaphases contained the clonal aberrations described above, includingdeletions of 5q and monosomy 7. Both these aberrations are characteristicfindings in MDS or AML. Similar aberrations were observed in a previous bonemarrow specimen from this patient, and here are consistent withpersistent/recurrent MDS or AML.


X
XXX
+3,inv(9),der(16)t(3;16)(p11;q24), -3
KARYOTYPE: 44,XY,add(3)(p11), del(5)(q14), -7, inv(9)(p12q13), psudic(12) t(12;18) (p12-13;p12), der(16)t(3;16)(p11;q24)[cp12]/46,idem,-3,del(22)(q22),+2mar[cp8]
X


*Good = normal, -Y, del(5q), del(20q); Intermediate = other karyotypic abnormalities; Poor = complex (≥3 abnormalities) or chromosome 7 abnormalities
**Hb <10 g/dL; ANC <1800/μL; platelet count <100,000/μL
Greenberg PL et al. Blood. 1997;89:2079
IPSS: International Prognostic Scoring System
All 3 prognostic variables required to generate IPSS score
Prognostic Variable 0 0.5 1 1.5 2
Bone marrow blasts (%) <5 5–10 - 11–20 21–30
Karyotype* Good Intermediate Poor -
Number of cytopenias** 0/1 2/3 - - -
Score Value
Risk Group: Low Int-1 Int-2 HighScore: 0 0.5-1.0 1.5–2.0 ≥2.5

Low Risk 31%
Int-1 Risk 39%
Int-2 Risk 22%
High8%
Greenberg PL et al. Blood. 1997;89:2079
IPSS Risk Categories Distribution


IPSS
1 2Years
100
90
80
70
60
50
40
30
20
10
00 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Perc
ent
A
Survival (<60 years old) Survival (≥60 years old)
1 2Years
100
90
80
70
60
50
40
30
20
10
00 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Perc
ent
BLow 60 ptsInt-1 87 ptsInt-2 49 ptsHigh 9 pts
Low 207 pts
Int-2 127 ptsHigh 50 pts
Int-1 227 pts
Source: Bennet, John M. MDS: Past, Present, Future. Presentation

Source: Bennet, John M. MDS: Past, Present, Future. Presentation
WHO MDS Subtypes5q- 3%
PRA8%RAEB-2
18%
RAEB-1 21%
PRA11%
RCMD 24%
RSAMD15%
Survival (months)
RAEB-2, 10
5q- , 116
RAEB-1 , 18
RSAMD, 32
PRA, 69
RCMD , 33
PSA, 69
Survival and WHO Subtypes

Therapy of MDS
Considerations:• IPSS, WHO/FAB Classification• Age / Performance Status• HLA-DR• Cytogenetics
Options:• General supportive care including transfusion, antibiotics• Cytokines – Erythropoeitin/G-CSF/Androgens• Immunosuppressive therapy: ATG, Steroids, Cyclosporine/FK506 • Single agent chemotherapy: Busulfan, Hydrea, Cytarabine• Multiple agents +/- BMT• Novel new drugs
• Hypomethylating agents (Dacogen, Vidaza)• IMIDs (Thalidomide, Revlimid)


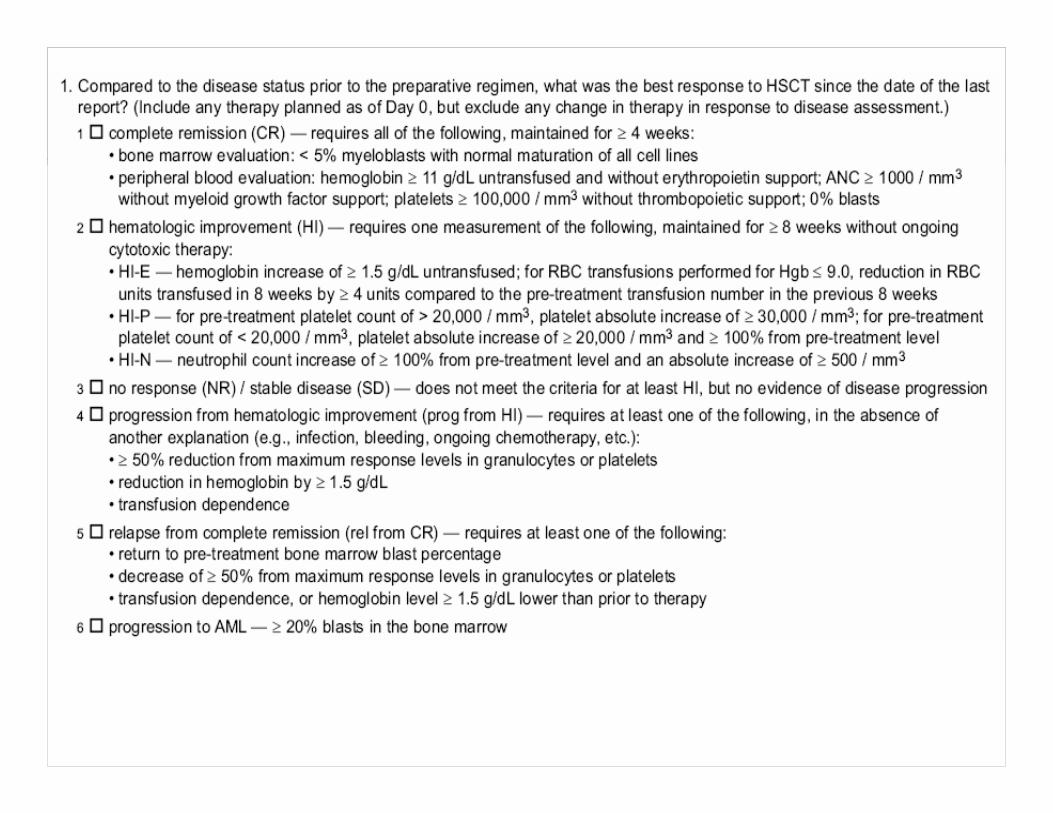
IWG Response Criteria in MDS
Cheson BD, et al. Blood 2000. 96:3671-4.
RBC (HI-E): Major: Treatment-indepen. or >2g/dl ↑ in Hgb; Minor: 50% ↓ in tx req or 1-2 g/dl ↑ in Hgb.PLT (HI-P):Major: PLT tx indep or ↑ by 30K if < than 100K at baseline;Minor: 50% ↑ in PLT count (of at least 10K) if baseline <100K.PMN (HI-N):Major: if ANC <1500, a 100% ↑ or 500/ μl, ↑ whichever greater; Minor: if ANC <1500, ANC ↑ by 100%, but < than 500/ μl.
HematologicImprovement
Same as CR; ↓ blasts by 50%Partial Remission
<5% BM blasts, No dysplasia; Hgb>11; PMN>1.5, PLT>100KComplete Remission



Transplantation for MDS
Only curative therapy available
0
500
1,000
1,500
2,000
2,500
AMLALL NHL MDS
Non-Malignant Diseases
CMLCLL Myeloma
Other Malignancies
Hodgkin's
Neuroblastoma
Tran
spla
nts
Source: CIBMTR 2005 slideset

Adapted from Deeg et al, Blood 2002
Related vs. Unrelated Donors

Castro-Malaspina et al, Blood 2002
NMDP Experience



Thanks for your attention
Good luck with the new forms!!!
















![Harmonized Tarriffs[1]](https://img.pdfslide.net/doc/110x75/577d2cbd1a28ab4e1eacc307/harmonized-tarriffs1.jpg)










