Embed Size (px)
Citation preview

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
1/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
Official reprint from UpToDate®
www.uptodate.com ©2011 UpToDate®
AuthorsErrol R Norwitz, MD, PhDJoong Shin Park, MD, PhD
Section EditorCharles J Lockwood, MD
Deputy EditorVanessa A Barss, MD
Overview of the etiology and evaluation of vaginal bleeding inpregnant women
Disclosures
Last literature review version 19.3: September 2011 | This topic last updated: August 11,2010
INTRODUCTION — Vaginal bleeding is a common event at all stages of pregnancy. The sourceis virtually always maternal, rather than fetal. Bleeding may result from disruption of decidualblood vessels or from discrete cervical or vaginal lesions. The clinician typically makes aprovisional clinical diagnosis based upon the patient's gestational age and the character of herbleeding (light or heavy, associated with pain or painless, intermittent or constant). Laboratoryand imaging tests are then used to confirm or revise the initial diagnosis.
An overview of the etiology and evaluation of vaginal bleeding in pregnant women will bereviewed here. Specific causes of bleeding and their management are discussed in detailseparately. (See individual topic reviews on each subject).
FIRST TRIMESTER BLEEDING — Vaginal bleeding is common in the first trimester, occurringin 20 to 40 percent of pregnant women. It may be any combination of light or heavy,intermittent or constant, painless or painful. The four major sources of bleeding in earlypregnancy are:
Ectopic pregnancy
Miscarriage (threatened, inevitable, incomplete, complete)
Implantation of the pregnancy
Cervical, vaginal, or uterine pathology (eg, polyps, inflammation/infection, trophoblasticdisease)
Bleeding related to miscarriage is the most common cause of first trimester bleeding. Ectopicpregnancy is relatively common and the most serious etiology as rupture of the extrauterinepregnancy is a life threatening complication.
Evaluation — The exact etiology of uterine bleeding in the first trimester often cannot bedetermined; the goal of the evaluation is to make a definitive diagnosis when possible andexclude the presence of serious pathology in the remaining cases. Ectopic pregnancy isparticularly important to exclude since it can be life-threatening. Thus, the first step inevaluation is to determine whether the patient has had an ultrasound examination, as well asthe results of the test. Prior documentation that the pregnancy is intrauterine immediatelynarrows the differential diagnosis.
History — The extent of bleeding should be determined: is the woman passing blood clots or

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
2/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
is the blood soaking through her clothes? Does she feel lightheaded? Does she have significantpelvic pain or cramping? Has she passed any tissue? If she answers yes to these questions,then ectopic pregnancy and miscarriage are more likely diagnoses than implantation bleedingor cervicovaginal disease (eg, polyps, cervicitis, cancer). On the other hand, it is important toremember that the presence of only light, intermittent, painless bleeding does not exclude thepossibility of a life-threatening underlying disorder, such as ectopic pregnancy.
What is the patient's medical history? A past history of ectopic pregnancy or risk factors forectopic pregnancy (eg, history of pelvic inflammatory disease, presence of an intrauterinecontraceptive device, adnexal surgery) increases the probability of this disorder. (See"Incidence, risk factors, and pathology of ectopic pregnancy".)
A history of two or more consecutive miscarriages or a condition associated with miscarriage(eg, parental chromosomal translocation, maternal antiphospholipid syndrome, uterineanomaly) suggests bleeding may be related to impending pregnancy loss. (See "Spontaneousabortion: Risk factors, etiology, clinical manifestations, and diagnostic evaluation".)
Physical examination — Orthostatic changes in blood pressure or pulse are indicative ofsevere blood loss.
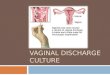
Any tissue the patient has passed should be examined. Patients may mistake blood clot for theproducts of conception. If the tissue represents a partial or complete miscarriage, the fetalmembranes, fronds indicative of placental villi, or an intact fetus should be visible upon carefulexamination. Visualization of villi can be facilitated by floating the products of conception inwater (picture 1A-B).
The patient's abdomen should be examined before performing an internal examination. It isbest to begin by examining the quadrant where the patient is experiencing the least pain.Gentle percussion is preferred to deep palpation since it causes less pain and guarding. Midlinepain is more consistent with miscarriage, while lateral pain is more consistent with ectopicpregnancy. Nongynecologic causes of pain also to be considered. (See "Approach to abdominalpain and the acute abdomen in pregnant and postpartum women".)
The clinician should determine whether uterine size is appropriate for the estimated gestationalage. The size - gestational age correlation is learned by experience and is often described interms of fruit (eg, 6 to 8 week size = small pear, 8 to 10 week size = orange, 10 to 12 weeksize = grapefruit). The uterus remains a pelvic organ until approximately 12 weeks ofgestation, when it becomes sufficiently large to palpate transabdominally just above thesymphysis pubis. The normal uterus is nontender, smooth, and firm.
If the pregnancy is at or beyond 10 to 12 weeks of gestation, a handheld Doppler device can beused to check the fetal heart beat. The fetal heart rate can be easily distinguished from thematernal heart rate since the fetal heart rate is typically in the range of 110 to 160 beats perminute [1]. Doppler confirmation of fetal cardiac activity is reassuring, as it indicates bleedingis not related to fetal demise and unlikely to be related to an ectopic pregnancy. On the otherhand, loss of a previously detected fetal heart beat should raise suspicion that fetal demise hasoccurred. However, inability to detect fetal heart motion by Doppler is subject to physicianerror, particularly in the first trimester.
After the abdominal examination, the patient is placed in the lithotomy position. The externalgenitalia are examined to assess the volume and source of bleeding and then a speculum isinserted into the vagina. If blood clots, products of conception, or both are present, they can beremoved with gauze sponges on a sponge forceps. This tissue is examined as described aboveand, by convention, sent for pathologic examination to confirm the presence of products ofconception and to exclude gestational trophoblastic disease. The utility of routine

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
3/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
histopathological examination is questionable, as it rarely suggests the underlying cause of thepregnancy failure or establishes a diagnosis of gestational trophoblastic disease [2]. However,pathologists can sometimes diagnose entities that are the probable cause of the loss orassociated with recurrence. These include massive chronic intervillositis, massive intervillousfibrin deposition, maternal vasculitis, findings suggestive of some chromosomal anomalies (eg,triploidy, some trisomies), and septic abortion.
Speculum examination may reveal a source of bleeding unrelated to pregnancy; in such cases,further evaluation depends upon the nature of the abnormality:
Vaginal laceration (see "Evaluation and management of lower genital tract trauma inwomen")
Vaginal neoplasm (see "Vaginal cancer")
Vaginal warts (see "Condylomata acuminata (anogenital warts)")
Vaginal discharge (see "Diagnostic approach to women with vaginal discharge")
Cervical polyps, fibroids, ectropion (see "Congenital cervical anomalies and benigncervical lesions")
Mucopurulent cervical discharge or friability at the endocervical os (see "Acute cervicitis")
Cervical neoplasm (see "Invasive cervical cancer: Epidemiology, risk factors, clinicalmanifestations, and diagnosis")
Visualization of the cervical os helps to distinguish between a threatened and animpending/inevitable miscarriage. Direct visualization of the gestational sac in a dilated cervixis generally sufficient to diagnose an impending/inevitable miscarriage clinically. The cervix willalso be open after a recent incomplete or complete miscarriage. Ultrasound can provideadditional information in these cases, such as whether or not there are retained products ofconception, or the unexpected presence of a twin pregnancy with a second viable gestationalsac.
A closed cervix is consistent with a threatened miscarriage, but not diagnostic. If the cervixappears closed and there are no obvious bleeding lesions, the speculum is removed and abimanual pelvic examination is performed. With an ectopic pregnancy, findings on pelvicexamination may include adnexal, cervical motion, or abdominal tenderness; an adnexal mass;and mild uterine enlargement. However, the physical examination is often unremarkable in awoman with a small, unruptured ectopic pregnancy. (See "Clinical manifestations, diagnosis,and management of ectopic pregnancy".)
Uterine size larger than expected for dates suggests a multiple gestation, possibly withmiscarriage of one of the multiples, gestational trophoblastic disease (molar pregnancy), orother uterine pathology (fibroids can cause an irregularly enlarged uterus). (See "Twinpregnancy: Prenatal issues" and "Gestational trophoblastic disease: Epidemiology, clinicalmanifestations and diagnosis" and "Epidemiology, clinical manifestations, diagnosis, and naturalhistory of uterine leiomyomas (fibroids)".)
One review of data from observational studies concluded that ultrasound examination andhuman chorionic gonadotropin (hCG) concentration (both discussed below) could replace pelvicexamination in the initial evaluation of patients with early pregnancy bleeding [3]. However,some diagnoses will be missed with this approach (eg, bleeding from cervical or vaginallesions), this combination of tests may not distinguish between a complete miscarriage and anectopic pregnancy (both will have an empty uterus and positive hCG), and the additional cost of

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
4/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
the tests can be avoided in some patients. For example, in bleeding patients in whomsonography has previously confirmed a viable singleton intrauterine pregnancy, anotherexamination is not necessary to exclude ectopic pregnancy or to confirm fetal viability if fetalheart motion can be detected by a handheld Doppler device. Additionally, there is no value inchecking human chorionic gonadotropin (hCG) concentration once the presence of anintrauterine pregnancy has been established sonographically.
Ultrasonography — Transvaginal ultrasonography is the cornerstone of the evaluation ofbleeding in early pregnancy. It is most useful in bleeding patients with a positive pregnancytest in whom an intrauterine pregnancy has not been previously confirmed by imaging studies.In these women, ultrasound examination is performed to determine whether the pregnancy isintrauterine or extrauterine (ectopic) and, if intrauterine, whether the pregnancy is viable (fetalcardiac activity present) or nonviable.
It is important to note that the absence of an intrauterine gestational sac is highly suggestive ofectopic pregnancy if more than 5.5 to 6 weeks have elapsed since the first day of the patient'slast menstrual period. At earlier gestational ages, however, an intrauterine pregnancy may bepresent, but not yet identifiable, by ultrasound. In these cases, sonographic findings arecorrelated with human chorionic gonadotropin (hCG) levels. The use of sonography and hCG inthe differential diagnosis of intrauterine versus extrauterine pregnancy and viable versusnonviable intrauterine pregnancy is described briefly below (see 'Laboratory tests' below) andin detail separately. (See "Spontaneous abortion: Risk factors, etiology, clinical manifestations,and diagnostic evaluation" and "Clinical manifestations, diagnosis, and management of ectopicpregnancy".)
Rarely, ultrasound examination reveals unusual causes of uterine bleeding, such as gestationaltrophoblastic disease or loss of one fetus from a multiple gestation. (See "Gestationaltrophoblastic disease: Epidemiology, clinical manifestations and diagnosis" and "Twinpregnancy: Prenatal issues", section on 'Early and late loss'.)
In bleeding patients in whom sonography has previously confirmed a viable singletonintrauterine pregnancy, another examination is not necessary to confirm fetal viability if fetalheart motion can be detected by a handheld Doppler device.
Laboratory tests — There is no role for monitoring human chorionic gonadotropin (hCG)concentration once the presence of an intrauterine pregnancy has been establishedsonographically. Serial measurements of hCG are helpful during the first six weeks ofpregnancy if ultrasonography is nondiagnostic, ie, the site and viability of the pregnancy arenot revealed. In this setting:
Falling beta-hCG concentrations are consistent with a nonviable intrauterine pregnancy orinvoluting ectopic pregnancy, but do not indicate whether the pregnancy is intrauterine orectopic.
Appropriately rising hCG levels are most consistent with a viable intrauterine pregnancy(85 percent of viable pregnancies display a rise in hCG greater than 66 percent over 48hours), but some ectopic pregnancies also display this pattern.
hCG levels that have plateaued or are rising slowly suggest an ectopic pregnancy.
The pattern of hCG change in normal and abnormal pregnancies and its correlation withultrasound findings are discussed in detail separately, and summarized below. (See "Clinicalmanifestations, diagnosis, and management of ectopic pregnancy", section on 'Human chorionicgonadotropin'.)

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
5/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
Other hormone assays (eg, progesterone, estrogen, inhibin A, PAPP-A) are less useful.
Differential diagnosis and management — The information gleaned from the aboveevaluation is used to determine a diagnosis and plan of management. Women with significantfirst trimester vaginal bleeding (ie, menses-like) should have a red blood cell antibody screenchecked. Those who are Rh(D) negative are given anti-D immunoglobulin to protect againstRh(D) isoimmunization, unless the vaginal bleeding is clearly due to a nonplacental, nonfetalsource, such as a vaginal laceration. (See "Prevention of Rh(D) alloimmunization".)
Ectopic pregnancy — Women with a history of ectopic pregnancy and early pregnancybleeding and pain are assumed to have recurrent ectopic pregnancy until this diagnosis hasbeen excluded by laboratory and imaging studies.
In the hands of an experienced ultrasonographer, absence of an intrauterine pregnancy ontransvaginal ultrasound examination when the hCG concentration is greater than 1000 to 2000IU/L (greater than 6000 IU/L for transabdominal ultrasound) strongly suggests ectopicpregnancy (with less experienced sonographers the threshold may be higher, 2000 to 4000 IU/L). An adnexal mass may or may not be seen. The presence of hemodynamic instability and atender abdomen suggests the ectopic pregnancy has ruptured.
Diagnosis of intrauterine (viable or nonviable) versus extrauterine pregnancy at hCGconcentrations below 1500 IU/L is complicated and discussed in detail separately. (See "Clinicalmanifestations, diagnosis, and management of ectopic pregnancy".)
Management of ectopic pregnancy is generally medical (methotrexate therapy) or surgical.(See "Methotrexate treatment of tubal and interstitial ectopic pregnancy" and "Surgicaltreatment of ectopic pregnancy and prognosis for subsequent fertility".)
Expectant management can be dangerous for the mother, but may be possible in rare cases.(See "Expectant management of ectopic pregnancy".)
Even if an intrauterine pregnancy is diagnosed, the possibility of heterotopic pregnancy shouldbe kept in mind, even though rare. This is particularly important in women who underwent invitro fertilization since these patients are at increased risk of this pregnancy complication. (See"Abdominal pregnancy, cesarean scar pregnancy, and heterotopic pregnancy".)
Threatened miscarriage — Uterine bleeding in the presence of a closed cervix andsonographic visualization of an intrauterine pregnancy with detectable fetal cardiac activity isdiagnostic of threatened miscarriage. The term "threatened" is used to describe these casesbecause miscarriage does not always follow uterine bleeding in early pregnancy, even afterrepeated episodes or large amounts of bleeding. In fact, 90 to 96 percent of pregnancies withboth fetal cardiac activity and vaginal bleeding at 7 to 11 weeks of gestation do not miscarry;the higher success rate is associated with bleeding at the later end of the gestational age range[4,5].
Uterine bleeding in these cases is likely due to disruption of decidual vessels at the maternal-fetal interface. These separations generally cannot be visualized by ultrasound, but sometimesappear as a subchorionic hematoma. Management is expectant. The diagnosis and outcome ofsubchorionic hematoma are discussed in more detail separately. (See "Spontaneous abortion:Risk factors, etiology, clinical manifestations, and diagnostic evaluation", section on 'Findingspotentially predictive of pregnancy loss'.)
Inevitable miscarriage — When miscarriage is inevitable, the cervix is dilated, uterinebleeding is increasing, and painful uterine cramps/contractions are present. The gestationaltissue often can be felt or seen through the cervical os; passage of this tissue typically occurswithin a short time. Management may be expectant, or a medical or surgical intervention to

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
6/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
complete the miscarriage can be undertaken. (See "Spontaneous abortion: Risk factors,etiology, clinical manifestations, and diagnostic evaluation" and "Spontaneous abortion:Management".)
Complete and incomplete miscarriage
Complete miscarriage — When a miscarriage occurs before 12 weeks of gestation, it iscommon for the entire contents of the uterus to be expelled, thereby resulting in acomplete miscarriage. If this has occurred, the uterus is small on physical examinationand well contracted with an open or closed cervix, scant vaginal bleeding, and only mildcramping. Ultrasound will reveal an empty uterus and no extrauterine gestation.
A complete miscarriage can be distinguished from an ectopic pregnancy by examining thetissue that was passed to confirm products of conception, by demonstrating falling rather thanrising or plateaued hCG levels, and by patient description of diminishing bleeding and pain. Nofurther intervention is needed for complete miscarriage if chorionic villi are identified bypathologic examination of the products of conception. However, if no villi are identified or nospecimens are available for pathologic examination, then serum hCG levels should be followedserially until the level is undetectable. (See "Spontaneous abortion: Risk factors, etiology,clinical manifestations, and diagnostic evaluation" and "Spontaneous abortion: Management".)
Incomplete miscarriage — After 12 weeks of gestation, the membranes may rupture andthe fetus may be passed, but significant amounts of placental tissue can be retained,resulting in an incomplete miscarriage. On examination, the cervical os is open,gestational tissue may be observed in the cervix, and the uterine size is smaller thanexpected for gestational age, but not well contracted. The amount of bleeding varies, butcan be severe enough to cause hypovolemic shock. Painful cramps/contractions are oftenpresent. Ultrasound reveals tissue in the uterus. Medical or surgical evacuation isgenerally performed.
Missed abortion — A missed abortion (also called a delayed miscarriage) refers to in-uterodeath of the embryo or fetus prior to the 20th week of gestation, with retention of thepregnancy for a prolonged period of time. Women may notice that symptoms associated withearly pregnancy (eg, nausea, breast tenderness) have abated and they don't "feel pregnant"anymore. Vaginal bleeding may occur. The cervix usually remains closed. Ultrasound revealsan intrauterine gestational sac with or without a fetal pole, but no fetal cardiac activity.Management may be expectant or a medical or surgical intervention to complete themiscarriage can be undertaken. (See "Spontaneous abortion: Risk factors, etiology, clinicalmanifestations, and diagnostic evaluation".)
Vanishing twin — The term "vanishing twin" has been used to describe a singletonpregnancy which results from very early loss of one member of a multiple gestation. Vanishingtwins are often the product of assisted reproduction techniques and can be associated withvaginal bleeding [6]. (See "Pregnancy outcome after assisted reproductive technology", sectionon 'Early loss' and "Twin pregnancy: Prenatal issues", section on 'Early and late loss'.)
Vaginitis, trauma, cancer, warts, polyps, fibroids — These conditions are diagnosed byvisual inspection, with ancillary tests as indicated (eg, wet mount and pH of vaginal discharge,cervical cytology and/or biopsy of mass lesions, ultrasound examination of fibroids).
Management of bleeding related to these conditions depends upon the specific condition. (Seeindividual topic reviews on each subject).
Ectropion — Cervical ectropion (columnar epithelium exposed to the vaginal milieu byeversion of the endocervix) is a common and normal finding in pregnancy. The exposed

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
7/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
columnar epithelium is prone to light bleeding when touched, such as during coitus, insertion ofa speculum, bimanual examination, or when a cervical specimen is obtained for cytology orculture. Therapy is unnecessary. (See "Congenital cervical anomalies and benign cervicallesions", section on 'Ectropion'.)
Physiologic or implantation bleeding — This is a diagnosis of exclusion. It is characterizedby a small amount of spotting or bleeding approximately 10 to 14 days after fertilization (at thetime of the missed menstrual period), and is presumed to be related to implantation of thefertilized egg in the decidua (ie, lining of the uterus) [7], although this hypothesis has beenquestioned [8]. No intervention is indicated.
Prognosis — Studies consistently show an association between first trimester bleeding andadverse outcome (eg, miscarriage, preterm birth, premature rupture of membranes, fetalgrowth restriction) later in pregnancy [8-18]. The prognosis is best when bleeding is light andlimited to early pregnancy, ie, less than 6 weeks of gestation [8,17]. The prognosis worsenswhen bleeding is heavy or extends into the second trimester [12-16]. These relationships areillustrated by the following examples:
In a series of 550 women followed prospectively from the time of their positivepregnancy test, 117 (21 percent) had bleeding prior to 20 weeks of gestation and 67miscarried (12 percent, or about one-half of those with bleeding) [19]. Fourteen of 18pregnancies with heavy bleeding (eg, clots) and moderate pain miscarried (78 percent).
In one large prospective series in which all subjects had a viable pregnancy at enrollmentat 10 to 14 weeks, the frequency of preterm delivery with no, light, or heavy firsttrimester bleeding was about 6, 9, and 14 percent, respectively, and the frequency ofspontaneous loss before 24 weeks of gestation was 0.4, 1, and 2 percent, respectively[12]. Because these subjects were enrolled late in the first trimester and withsonographically confirmed fetal viability, women with very early bleeding andmiscarriage had already been excluded.
In a third series, vaginal bleeding occurring in more than one trimester was associatedwith a greater than seven-fold increased risk of preterm premature rupture ofmembranes (OR 7.4; 95% CI 2.2-25.6) [16].
A retrospective registry-based study including over one million women found that,compared to women without bleeding, first trimester bleeding significantly increased therisk of preterm birth at 28 to 31 weeks (0.9 versus 0.3 percent; OR 2.98, 95% CI 2.50-3.54) and at 32 to 36 weeks (6.1 versus 3.6 percent; OR 1.65, 95% CI 1.57-1.77) [18].First trimester bleeding was also associated with a significant increase in risk of bleedingand preterm birth in the subsequent pregnancy. A history of first trimester bleeding in thefirst pregnancy increased the incidence of bleeding in the second pregnancy from 2.2percent to 8.2 percent (OR 4.05; 95% CI 3.78-4.34) and increased the incidence ofpreterm delivery from 2.7 percent to 4.8 percent (OR 1.83; 95% CI 1.67-2.00).
No change in pregnancy management is indicated for women with first trimester bleeding.There are no effective interventions, but women can be reassured of the low likelihood ofadverse outcome. In particular, bedrest is unnecessary and will not affect outcome. (See "Riskfactors for preterm labor and delivery", section on 'Vaginal bleeding'.)
SECOND AND THIRD TRIMESTER BLEEDING — Vaginal bleeding is less common in thesecond and third trimesters. The major causes of bleeding at these times are:
Bloody show associated with cervical insufficiency or laborPlacenta previa

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
8/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
Abruptio placentaUterine ruptureVasa previa
Prior to 20 weeks of gestation
Evaluation — The evaluation of pregnant women with vaginal bleeding prior to 20 weeks issimilar to that in the first trimester (see above); however, ectopic pregnancy is less of aconcern because over 95 percent of ectopic pregnancies occur in the fallopian tube and virtuallyall tubal ectopic pregnancies will have been diagnosed by this time. Although abdominal,heterotopic, cervical, cornual, and cesarean scar ectopic pregnancies often present at moreadvanced gestations than tubal ectopics, these types of ectopic pregnancy are rare.
The first step in the evaluation is to determine the extent of bleeding and whether bleeding isaccompanied by pain. The presence of only light, intermittent, painless bleeding suggestsbloody show from cervical insufficiency, a small marginal placental separation, or a cervical orvaginal lesion (eg, polyp, infection, cancer). Heavier bleeding, particularly when associatedwith pain, is more consistent with impending miscarriage or a larger placental separation (ie,abruption).
As discussed above, loss of a previously detected fetal heart beat should raise suspicion thatfetal demise has occurred, but inability to detect the fetal heart by Doppler is subject tophysician error and should always be confirmed by ultrasound examination. On the other hand,Doppler confirmation of fetal cardiac activity is reassuring.
An abdominal examination is performed to assess for pain or other abnormalities and uterinesize. At 16 weeks of gestation, the uterine fundus is palpable about midway between thesymphysis pubis and umbilicus, while at 20 weeks it is palpable at about the level of theumbilicus. After the abdominal examination, the patient is placed in the lithotomy position. Theexternal genitalia are examined and then a speculum is inserted into the vagina. As discussedabove, physical examination may reveal a nonpregnancy-related source of bleeding, such ascervical ectropion, an abnormal growth, a laceration, or sanguinous-purulent discharge.
Direct visualization of a dilated cervix or fetal membranes may be sufficient to diagnoseimpending miscarriage if contractions are present, or cervical insufficiency in the absence ofcontractions.
Transvaginal ultrasonography is also the cornerstone in the evaluation of bleeding in the secondtrimester. The primary goals are to determine whether the placenta is covering the cervical os(placenta previa), whether there is evidence of decidual hemorrhage causing placentalseparation (ie, abruptio placenta), and whether the cervix shows signs suggestive of cervicalinsufficiency (short length, dilated internal os, funneling of the fetal membranes). (See"Prediction of prematurity by transvaginal ultrasound assessment of the cervix" and "Cervicalinsufficiency".)
Differential diagnosis
Miscarriage (see 'Threatened miscarriage' above and 'Inevitable miscarriage' above and'Complete and incomplete miscarriage' above and 'Missed abortion' above)
Cervical, vaginal, or uterine pathology (see 'Vaginitis, trauma, cancer, warts, polyps,fibroids' above)
Cervical insufficiency — The diagnosis of cervical insufficiency is clinical; the classicpresentation is cervical dilatation and effacement in the second trimester with fetalmembranes visible at or beyond the external os in the absence of contractions. It may be

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
9/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
asymptomatic or associated with one or more of the following: vaginal fullness orpressure; vaginal spotting or bleeding; an increased volume of watery, mucousy, orbrown vaginal discharge; and vague discomfort in the lower abdomen or back.Sonographic findings of a short cervix, dilated internal cervical os, and/or funnelingsupport the diagnosis. (See "Cervical insufficiency".)
Abruption — Bleeding and cramping are the signs and symptoms of placental separationdue to hemorrhage into the decidual basalis. The diagnosis is one of exclusion sinceplacental separation usually cannot be visualized on ultrasound examination. Thepresence of a subchorionic hematoma or placenta that covers the internal cervical ossupports the diagnosis. (See "Spontaneous abortion: Risk factors, etiology, clinicalmanifestations, and diagnostic evaluation", section on 'Ultrasonography'.)
Ectopic pregnancy — Ectopic pregnancy is rare at this gestational age. When an ectopicpregnancy is diagnosed after the first trimester, the location is likely to be nontubal(abdominal, cervical, cesarean scar, or cornual) or heterotopic (ie, coexistent intrauterineand extrauterine pregnancies). (See "Abdominal pregnancy, cesarean scar pregnancy,and heterotopic pregnancy" and "Cervical pregnancy".)
Bleeding after 20 weeks of gestation — The term antepartum hemorrhage typically refers touterine bleeding after 20 weeks of gestation that is unrelated to labor and delivery. Antepartumhemorrhage complicates 4 to 5 percent of pregnancies. The major causes are:
Placenta previa (20 percent)Abruptio placenta (30 percent)Uterine rupture (rare)Vasa previa (rare)
In the remaining cases, the exact etiology of the antepartum bleeding cannot be determinedand is frequently attributed to marginal separation of the placenta.
Evaluation — In contrast to bleeding in the first half of pregnancy, digital examination ofthe cervix SHOULD BE AVOIDED in women presenting with bleeding in the second half ofpregnancy until placenta previa has been excluded. Digital examination of a placenta previa cancause immediate, severe hemorrhage.
Differential diagnosis
Placenta previa — Placenta previa should be suspected in any woman who presents withvaginal bleeding in the second half of pregnancy. Classically, the absence of abdominalpain and uterine contractions was considered the clinical feature that distinguishedbetween placenta previa and abruptio placenta, which is the other major cause of vaginalbleeding at this time. However, some women with placenta previa have uterinecontractions in addition to bleeding; thus, the diagnosis of placenta previa must bedetermined by sonographic examination. (See "Clinical manifestations and diagnosis ofplacenta previa".)
Abruptio placenta — Abruptio placenta refers to premature separation of a normallyimplanted placenta prior to delivery of the infant. The most common risk factors includeprior placental abruption, trauma, smoking, cocaine use, hypertension, and pretermpremature rupture of the membranes.
Clinically, placental abruption typically presents with vaginal bleeding (80 percent), uterinetenderness (70 percent), and uterine contractions (35 percent), with or without nonreassuringfetal testing. Uterine tenderness is caused by extravasation of blood into the myometrium

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
10/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
(called a Couvelaire uterus when the blood penetrates all the way through the myometrium tothe peritoneal cavity). The amount of vaginal bleeding may not be a reliable indicator of theseverity of the hemorrhage since bleeding may be concealed (retained in the uterine cavity).Ultrasound may show placental separation, but this is uncommon (only 2 percent of abruptionscan be visualized on ultrasound); the major purpose of ultrasound examination is to excludeplacenta previa. Abruption ranges from mild to severe (life threatening) and may be acute orchronic. (See "Clinical features and diagnosis of placental abruption".)
The possibility of abruption should always be considered in women who are being evaluated fortrauma (eg, motor vehicle crash, fall, domestic violence). (See "Trauma in pregnancy", sectionon 'Abruptio placentae'.)
Uterine rupture and vasa previa — Uterine rupture and vasa previa are rare causes ofvaginal bleeding, and occur more often intrapartum than antepartum. Both may lead tofetal death. (See "Vasa previa and velamentous umbilical cord" and "Choosing the routeof delivery after cesarean birth", section on 'Uterine rupture'.)
Cervical, vaginal, or uterine pathology (see 'Vaginitis, trauma, cancer, warts, polyps,fibroids' above)
Prognosis — As with first trimester bleeding, episodes of second and third trimester bleedingare also associated with adverse pregnancy outcome, primarily preterm birth [20-22]. (See"Risk factors for preterm labor and delivery", section on 'Vaginal bleeding'.)
The risk of adverse outcome appears to depend on the degree of bleeding (worse outcome withheavier bleeding) and the cause (worse outcome with bleeding from nonprevia source) [23].
MANAGEMENT — The management of pregnant women with vaginal bleeding depends on thenumerous factors, including the gestational age, the cause of bleeding, the severity of bleeding,and fetal status. Management is discussed in the individual topic reviews on the specific causesof vaginal bleeding.
SUMMARY AND RECOMMENDATIONS
The clinician typically makes a provisional clinical diagnosis of the cause of vaginalbleeding based upon the patient's gestational age and the character of her bleeding (lightor heavy, associated with pain or painless, intermittent or constant). Laboratory andimaging tests are then used to confirm or revise the initial diagnosis. (See'Introduction' above.)
The four major causes of bleeding in early pregnancy are: ectopic pregnancy; threatenedor impending miscarriage; physiologic (ie, related to implantation of the pregnancy), andcervical, vaginal, or uterine pathology. Transvaginal ultrasonography is the cornerstoneof the evaluation of bleeding in early pregnancy. (See 'First trimester bleeding' above.)
An important goal in the evaluation of women with bleeding in early pregnancy is toexclude the possibility of ectopic pregnancy, since ruptured ectopic pregnancies can resultin severe hemorrhage and death. (See 'Ectopic pregnancy' above.)
The major causes of bleeding in the second and third trimesters are: bloody showassociated with cervical insufficiency or labor; placenta previa; abruptio placenta; andrarely uterine rupture or vasa previa. (See 'Second and third trimester bleeding' above.)
Digital examination of the cervix should be avoided in women presenting with bleedingin the second half of pregnancy until placenta previa has been excluded because digitalexamination of a placenta previa can cause immediate, severe hemorrhage. (See

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
11/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
'Bleeding after 20 weeks of gestation' above.)
For women with uterine bleeding who are Rh(D)-negative, we recommend anti-D immuneglobulin to protect against Rh(D) alloimmunization (Grade 1B). (See "Prevention of Rh(D)alloimmunization".)
Use of UpToDate is subject to the Subscription and License Agreement.

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
12/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
GRAPHICS
Chorionic villi
One method of distinguishing placenta from organized clot isto rinse with water and then float the tissue in a dish of water,preferably with a good light source underneath. Villi have afrond-like appearance, which has been described as similar toseaweed floating in the ocean Courtesy of Errol R Norwitz, MD, PhD.

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
13/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
Chorionic villi2
Courtesy of Errol R Norwitz, MD, PhD.

11/28/11 Overview of the etiology and evaluation of vaginal bleeding in pregnant women
14/14uptodate.com/…/overview-of-the-etiology-and-evaluation-of-vaginal-bleeding-in-pregnant-women?v…
© 2011 UpToDate, Inc. All rights reserved. | Subscription and License Agreement | Support Tag:[ecapp1005p.utd.com-218.186.18.251-AAA4B2E8D9-1218.14]Licensed to: Fundacion Marques de Valdicilla