PowerPoint Presentation
Reza PramayudhaOxygen TherapyOxygen delivery to the periphery
determined by two major factors:Oxygen content of arterial blood
andBlood flow Oxygen deliveryOxygen delivery is calculated as the
product of cardiac output and arterial oxygen content. Total oxygen
delivery is calculated as: Oxygen delivery
Aerobic metabolism requires a balance between oxygen delivery
(Do2) and oxygen utilization (Vo2)A biphasic relationship between
Do2 and Vo2 has been observed during normal aerobic
metabolismOxygen transport and oxygen utilization are independent
variablesMechanisms of HypoxiaPada saat istirahat rata-rata
laki-laki dewasa membutuhkan kira-kira 225- 250 ml oksigen per
menit, dan meningkat sampai 10 kali saat beraktivitas. Jika aliran
oksigen ke jaringan berkurang, atau jika penggunaan berlebihan di
jaringan maka metabolisme akan berubah dari aerobik ke metabolisme
anaerobik untuk menyediakan energi yang cukup untuk metabolisme.
Apabila ada ketidakseimbangan, akan mengakibatkan produksi asam
laktat berlebihan, menimbulkan asidosis dengan cepat, metabolisme
selular terganggu dan mengakibatkan kematian sel.4Major causes
mechanistically divided into three broad categories:Arterial
hypoxemia, Reduced oxygen delivery, and Excessive or dysfunctional
tissue utilization.tissue hypoxiaBerdasarkan mekanismenya, penyebab
hipoksia jaringan dibagi dalam 3 kategori, yaitu: 1). Hipoksemia
arteri, 2). Berkurangnya aliran oksigen karena adanya kegagalan
transport tanpa adanya hipoksemia arteri, dan3). Penggunaan oksigen
yang berlebihan di jaringan.5
Causes of ARTerial HypoxemiaThe most common pathophysiological
causes of hypoxemia in lung disease:ventilation-perfusion
mismatchtrue shuntdiffusion barrierPathophysiologyCirculatory
hypoxia results when fully oxygenated blood is delivered to tissues
in insufficient quantity or at an inadequate level to support
tissue metabolic needsCirculatory causesClinical manifestations of
hypoxia are highly variable and nonspecific and depend on both
duration of the hypoxia (acute or chronic) and the individuals
fitness.Clinical ManifestationsManifestasi klinik hipoksia tidak
spesifik, sangat bervariasi, tergantung pada lamanya hipoksia (akut
atau kronik), kondisi kesehatan individu dan biasanya timbul pada
keadaan hipoksia yang sudah berat. 9
Symptoms and signs associated with acute hypoxiaManifestasi
klinik dapat berupa perubahan status mental/bersikap labil, pusing,
dispneu, takipneu, respiratory distress, dan aritmia. Sianosis
sering dianggap sebagai tanda hipoksia, namun hal ini hanya dapat
dibenarkan apabila tidak terdapat anemia.
10Short-Term Oxygen TherapyLong-Term Oxygen TherapyINDICATIONS
FOR OXYGEN THERAPY11Short-Term Oxygen Therapy
Terapi oksigen jangka pendek merupakan terapi yang dibutuhkan
pada pasien-pasien dengan keadaan hipoksemia akut, di antaranya
pneumonia, PPOK dengan eksaserbasi akut, asma bronkial, gangguan
kardiovaskular, emboli paru. Pada keadaan tersebut, oksigen harus
segera diberikan dengan adekuatPada kondisi ini, oksigen harus
diberikan dengan Fi02 60-100% dalam waktu petldek sampai kondisi
membaik dan terapi yang spesifik diberikan.12
Long-Term Oxygen Therapy (LTOT)- Pada pasien dengan PPOK dan kor
pulmonal, terapi oksigen jangka panjang (long-term oxygen therapy/
LTOT) dapat meningkatkan jangka hidup sekitar enam sampai tujuh
tahun. Angka kematian menurun pada pasien dengan hipoksemia kronis
apabila oksigen diberikan lebih dari 12 jam sehari- Berdasarkan
beberapa penelitian didapatkan bahwa terapi oksigen jangka panjang
dapat memperbaiki harapan hidup. Karena adanya perbaikan dengan
terapi oksigen jangka panjang, maka saat ini direkomendasikan untuk
pasien hipoksemia (Pa02 < 55 mmHg atau saturasi oksigen <
88%) oksigen diberikan secara terus menerus 24 jam dalam sehari.
Pasien dengan Pa02 56 -59 mmHg atau saturasi oksigen 89%, kor
pulmonal atau polisitemia jugamemerlukan terapi oksigen jangka
panjang.- Pasien yang menerima terapi oksigen jangka panjang harus
dievaluasi ulang dalam 2 bulan untuk menilai apakah hipoksemia
menetap atau ada perbaikan dan apakah masih dibutuhkan terapi
oksigen?13Choice of delivery system is based upon a variety of
criteria:The degree of hypoxemiaRequirement for precision of
deliveryPatient comfortCostTechnique of Oxygen
AdministrationClassification of Oxygen Delivery Systems
Provide a fraction of the patients minute ventilatory
requirement as pure oxygen, the remainder of the ventilatory
requirement is fullled by addition of another gas, usually
entrained room airFlows supplied through these devices are low
(less than 6 L/min)Cannot deliver constant inspired oxygen
concentrations variations in the amount of entrained room
airLow-flow Oxygen DeviceNasal cannulesimple, inexpensive,easy to
usewell-toleratedFio2 may vary greatlyOxygen masksachievable
fraction of inspired oxygen above 0.44Simple face masks require a
ow of inspired oxygen of 5 to 6 L/min to avoid accumulation of CO2
within the mask.
Low-flow Oxygen Devices
Fraction of Inspired OxygenLow-flow Oxygen DevicesNasal
CannulaSimpleCan use continuously with meals and activityFlow rates
in excess of 4L cause drying and irritationDepth and rate of
breathing affect amount of O2 reaching lungsadults 6
LPMinfants/toddlers 2 LPM children 3 LPMFIO2 is not affected by
mouth breathing
19Kateter nasal dan kanul nasal merupakan alat dengan sistem
arus rendah yang digunakan secara luas. Kanul nasal arus rendah
mengalirkan oksigen ke nasofaring dengan aliran 1-6 L/m, dengan
Fi02 antara 0,24 - 0,44 (24% - 44%). Aliran yang lebih tinggi tidak
meningkatkan Fi02 secara bermakna di atas 44% dan dapat
mengakibatkan mukosa membran menjadi kering.Simple MaskLow to
medium concentration of O2Client exhales through ports on sides of
maskShould not be used for controlled O2 levelsO2 flow rate 5 to
8LCan cause skin breakdown; must remove to eat.
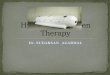
20Partial Rebreather MaskConsists of mask with exhalation ports
and reservoir bagReservoir bag must remain inflatedO2 flow rate - 6
to 10L FIO2=60%-80%Client can inhale gas from mask, bag, exhalation
portsPoorly fitting; must remove to eat
21Non-Rebreathing MaskConsists of mask, reservoir bag, 2 one-way
valves at exhalation ports and bagClient can only inhale from
reservoir bagBag must remain inflated at all timesO2 flow rate- 10
to 15L Fio2= 95-100%Poorly fitting; must remove to eat
22
Partial vs Non-rebreathing Masksclinical indications for use of
a high-flow oxygen delivery system:treatment of hypoxic patients
who depend on their hypoxic drive to breathe but who require
controlled increments in Fio2young, vigorous patients with
hypoxemia who have an abnormal ventilatory pattern and whose
ventilatory requirements may exceed the delivery capabilities of
low-ow systems.High-flow Oxygen Devices
Fraction of Inspired OxygenHigh-flow Oxygen DevicesVenturi
MaskMost reliable and accurate method for delivering a precise O2
concentrationConsists of a mask with a jetExcess gas leaves by
exhalation portsO2 flow rate 4 to 15L & Narrowed orificeFio2,
24%-60%Can cause skin breakdown; must remove to eat
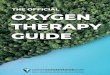
26Tracheostomy Collar/MaskO2 flow rate 8 to 10LProvides accurate
FIO2Provides good humidity; comfortable
27T-pieceUsed on end of ET tube when weaning from
ventilatorProvides accurate FIO2Provides good humidity
2829Goal of therapy is an SPO2 of >90% or for documented COPD
patients(Spo2 8892%)-(Pao2=55-60)As SPO2 normalizes the patients
vital signs should improveHeart rate should return to normal for
patientRespiratory rate should decrease to normal for patientBlood
pressure should normalize for patientGoal of Oxygen
Therapy29Pulmonary oxygen toxicity develops insidiously after a
variable lag period, during which the biochemical and cellular
changes occurDevelopment of chest pain, tachypnea, or cough in a
patient breathing elevated concentrations of oxygen alert to the
possibility of oxygen toxicityOxygen ToxicityThank YouMichael F.
Beers. Oxygen therapy and pulmonary oxygen toxicity.In: Fishman AP,
ed. 4th. Ed. Fishman' s pulmonary diseases anddisorders.
2008;2627-42.Reference: