Embed Size (px)
Citation preview


PACHC
2015 Annual Conference & Clinical Summit
The Cost of Care: Determining the True Cost of Providing Care to your Patients
Jennifer Nolty
Director, Innovative Primary Care
October 8, 2015

Determining the True Cost of Care
You can’t do today’s job with yesterday’s methods and be in business tomorrow.
Anonymous

Determining the True Cost of Care
I. Where are we today?
II. Cost vs Reimbursement
III. Preparing and Positioning for the Future

Health Center Lines of Business
Uninsured
– Nationwide accounts for about 35% of total Health Center Patients
– Care paid for by federal grant, local funding and patient fees (sliding fee scale)
– Health Centers MUST be ran as a sustainable business (PIN 2007-09 “Service Area
Overlap: Policy and Process”)
Medicaid
– Accounts for 41% of Health Center patients nationwide
– Highest payment rates and usually the quickest payer
Commercial
– Accounts for 16% of Health Center patients nationwide
– Typically lowest payment rates
Medicare
– Accounts for 8% of Health Center patients nationwide

Determining the True Cost of Care
ACA / Medicaid Managed Care / ACOs allow patients to have:
• Catastrophic coverage (inpatient, surgery, ER)
• Also gives patients ‘choices’:– Keep the HC / PCP / Care Team– Access to a network of providers – Additional services not previously covered (vision, adult
dental, etc.)
• ‘Risk’ is transferred from the State / CMS / Federal Government to Insurer / payer

Determining the True Cost of Care
‘Patient Landscape’ is changing for everyone
- Is it the same as it was 5, 10 years ago?
- What has impacted this?- Payer mix changing
- # of uninsured decreasing- # of insured increasing
- Retention of patients
- Demographics (aging population)
- Definition of who our patient is – movement to Population Health Management

Common Denominator - PATIENT
Health Center identifies a patient as:
• person who comes into the Health Center and received some type of service (physician, nurse practitioner, dentist, behavioral health, pharmacy, lab, x-ray)
• the Health Center bills some one (patient, managed care company, state Medicaid agency, etc) for payment of these services
• having a medical record on them
• reported on UDS

Is anyone else a Health Center patient?
Managed care / Accountable Care organizations define the Health Center patient is:
• the Health Center’s definition PLUS
• people who are now covered by an insurance plan AND have never been seen by the Health Center before
• Under managed care, everyone is assigned to or has to pick a primary care physician
• Day 1 at risk for patient’s cost of care
• Understand the definition of a New versus Established patient

Goals of Managed Care Organizations is to ensure:
• Providers deliver high-quality care in an environment that
manages or controls costs
• Care delivered is medically necessary and appropriate for the
patient’s condition
• Care is rendered by the most appropriate provider
• Care is rendered in the most appropriate, least restrictive
setting
Determining the True Cost of Care

Determining the True Cost of Care
• Increase number of patients in the plan
• Keep patients out of the hospital– Inpatient stay
– ER visits
• Receive accurate and detailed billing information – Services rendered AND diagnosis coding – includes $0 reimbursement
• Shift more services and payments to primary care physician (clinically appropriate)
*differs from the total cost of care for their patient

Determining the True Cost of Care
Very few instances where physician patient service revenue has been or is reduced due to:
- Patient noncompliance / Poor quality outcomes
- Unnecessary utilization
- Excessive total cost of care
- Poor customer service / patient satisfaction
- Not seeing the patient @ least annually
- Movement from patient volume to demonstrating the management of patient populations effectively and efficiently (value) for reimbursement

Determining the True Cost of CareWe know the environment is shifting to a payment model where a greater portion of patient revenue is based on the:
- Examples of this shift - Financial incentives (P4P, shared savings, etc.)
- Hospital readmission nonpayment
- Bundled payments for a procedure or condition
- Larger piece of reimbursement from payer to PCP is capitation

The money flow in Managed Care Payments
Pre-payment to payer of patients covered

Determining the True Cost of Care
Under managed care, everyone is assigned to or has to pick a primary care physician
Patient Attribution:
- Claims- Patient choice- Auto assignment - Combination of any above
*Patients are linked to Primary Care Providers and are not able to be ‘removed’ from the panel
–Day 1 at risk for patient’s cost of care

Influence premium dollars:
• Payers are the ‘stewards’ of premium dollars • rely on accurate and detailed claims submission• evaluated on outcomes (HEDIS, STARs, financial, etc)• impacts how dollars are spent on patients (ex. benefits) and providers
• Payers are willing to pay dollars to positively influence population outcomes • Clinical Outcomes and Cost measures: P4P, shared savings • Evaluation and documentation of patients to receive the highest reimbursement /
premium allowed (Risk adjustment) • services not claims driven but impact patient outcomes (ex: soft costs - care
management, PCMH, coordinator, etc)
• Payers develop and rely on strong partnerships with Primary Care providers – including Health Centers – especially those who can tell a Quality Story with data
Determining the True Cost of Care

Determining the True Cost of Care
Payer is responsible for demonstrating the following:
“What am I (CMS/employer/State/HHS),
the purchaser, getting for my money?”

Determining the True Cost of Care
Total Cost of Providing Health Care
Expectation is $0.85 of every dollar paid to payer is spent on utilization and quality
Evaluate the Who, What, When, Where, Why and How
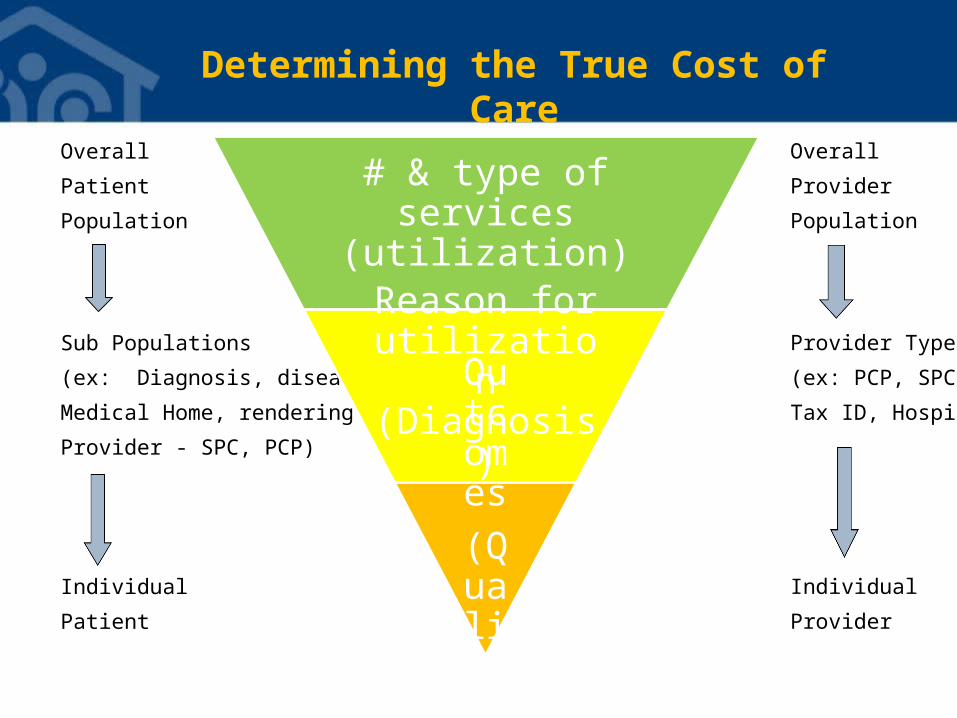
Overall
Patient
Population
Sub Populations
(ex: Diagnosis, disease,
Medical Home, rendering
Provider - SPC, PCP)
Individual
Patient
Determining the True Cost of Care
# & type of services (utilization)
Reason for utilization
(Diagnosis)
Outcomes
(Quality)
Overall
Provider
Population
Provider Type
(ex: PCP, SPC,
Tax ID, Hospital)
Individual
Provider

Determining the True Cost of Care
• When do patients usually go to the primary care doctor?– Sick or hurt
– Need refill of Medication
• When does the Managed Care/ACOs want patients to go to
the primary care doctor?– Same reasons above
– At least once a year for a check-up (when we are not sick)
– Preventative items (colonoscopy, mammogram, vaccinations, lab tests)
– After being treated in the ER or have been in the hospital

Determining the True Cost of Care
• Why do managed care companies want patients to see their primary care doctor?
– they are who the patient trusts (medical home)
– can treat most conditions
– connections to other providers in the community
– easy to work with
–better use of services leads to better health
outcomes and keeps costs down
* Increase in Primary Care Services is expected – over time this
should result in a decrease in other utilization and costs

Determining the True Cost of Care
Need to answer one of the following:
“Why should a payer pay the HC more for the
same service they can get from another PCP
at a much lower amount?”
or
“What is the cost of not being in, or having the HC, in the payer’s network?”

Determining the True Cost of Care
• Need to tell your story:

Determining the True Cost of Care
Demonstrate the value of having the HC in the network / Cost of not having them in the network
• Using data to show what the payer’s money pays for and what they are not getting from another PCP?
• One stop shop / attractive to patients and payers• F2F, Lab, Xray, Enabling services, specialists, access to BH, dental, vision (if covered by MCO/CMS/ACO) etc
• Share data (unblinded) among all providers / care team
within the HC• How this is used to influence P&Ps, patient outcomes, etc
• Patient engagement and outcomes
• Patient Education (aka Outreach & Enrollment)

Determining the True Cost of Care
Educate and Use the Tools Specific to Health Centers to demonstrate VALUE
• Annual reporting UDS data
• Board Oversight
• Strong Community based relationships / MOUs
• Data on patients previously uninsured
• Enabling Services / Social Determinants of Health data being captured
• Patient retention rates – especially as we expand PCMH to Population Health

Need to evaluate the same things Payers are:
• ID Patients:• ALL responsible for• where they receive ALL care from • Retention • Demographics
• Costs• Hard costs (billable)• Soft costs (captured but unable to bill)• Quality Programs / Outreach
Determining the True Cost of Care

Need to evaluate the same things Payers are:
• Reimbursement • Overall vs payer• does it cover the costs• Ways to maximize reimbursement• ID items not reimbursed for today but
impact outcomes and cost
• Outcomes• Compliance / ‘in control’• Annual visits / # of PCP visits
Determining the True Cost of Care

Overall
Patient
Population
Sub Populations
(ex: Diagnosis, disease,
Medical Home, rendering
Provider - SPC, PCP)
Individual
Patient
Determining the True Cost of Care
# & type of services (utilization)
Reason for utilization
(Diagnosis)
Outcomes
(Quality)
Overall
Provider
Population
Provider Type
(ex: PCP, SPC,
Tax ID, Hospital)
Individual
Provider

Additional Items:
• Patient retention and growth• Need to be better at documenting, coding, and
billing• Understand HIT (EMR / practice management)
capabilities• Understand where our patients access health care• Need data from payers and other HC providers
• develop / deepen these relationships • Share resources
• Understand your data to demonstrate your value
Determining the True Cost of Care

Thank you

For More Information
Jennifer NoltyDirector, Innovative Primary Care
National Association of Community Health CentersEmail: [email protected]
Phone: (301) 347-0437





























