Embed Size (px)
Citation preview

Padded SDine Board, Wafton et a!. 725 -
Louisiana Stare University, Sew Orleans. LA
Dcpartmcnt o f .Medicine, Section of Emergency Medicine (RW. JFDeS. AAE) Dcpartment of Biomctry and Genetics (AS)
Received: September 7. 1'34 Revision received: Dcccmber 1. 1004 Accepted: Dccemkr 2. 1994
Prior presentation: SAEM annual meeting. Washington, DC. M a y 1994.
Acknowledgments: Supported in part by Ferno-Washington of Wilmington. Ohio.
Addrcss for correspondence and reprints:
Jay DeSalvo. MD Louisiana State Lniversiry Department of Medicine Section of Ernergcncy Medicine Charity Hospital. 13th Floor 1532 Tulanr Avenue New Orleans. LA 70110
Key words: injury: spine: immobilization: back board: emergcncy medicil services
Padded vs Unpadded Spine Board for Cervical Spine Immobilization
Ross Walton, MD, Jay F. DeSalvo, MD, Amy A. E r s t , M D , Aditi Shahane
m ABSTRACT . , . . . , . . . , . . . . . . . . . , . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Objectives: To determine whether padding the long spine board im- proves patient comfort, affects cervical spine (c-spine) immobiliza- tion, or increases sacral transcutaneous O2 tension.
Methods: A prospective randomized, controlled crossover study of healthy volunteers was conducted over a two-week period. Partici- pants included 30 volunteers with no previous history of c-spine injury or disease. The subjects were randomized to either padded or un- padded long spine board immobilization with serial measurements of discomfort (using a visual analog scale) and transcutaneous tissue O2 tension obtained at zero and 30 minutes. Measurements of ability to flex, extend, rotate, and laterally bend the c-spine were made using a goniometer. The subjects then returned a minimum of three days later to complete the opposite half of the study (padded vs unpadded boards).
Results: Subject discomfort was significantly reduced in the padded group compared with the unpadded group (p = 0.024). There was no significant difference inflexion (p = 0.410), extension (p = 0.231), rotation (p = 0.891), or lateral bending (p = 0.230) for the two groups. There was no significant difference in the actual drop in sacral transcutaneous O2 tension from time zero to 30 minutes for the pad- ded and the unpadded groups (mean drop = 14.8% % 17.5% vs 12.2% r 16.8%, respectively; p = 0.906).
Conclusion: Adding closed-cell foam padding to a long spine board significantly improves comfort without compromising c-spine im- mobilization. Sacral tissue oxygenation does not appear affected by such padding for healthy volunteers.
Acad. Emcrg. Med. 1995; 21725-728.
I Spinal immobilization has become the out-of-hospital and ED standard of care in the treatment of patients with potential spinal injuries. The recommendations of the American College of Surgeons include a hard backboard, a rigid cervical collar, lateral support de- vices, and tape or straps.' These items are easily applied, allow ease of patient transport, and generally provide adequate immobilization. However, this immobilization technique can cause significant pain and discomfort, which may lead to further injury.2 There also is evidence that this technique may lead to pressure sore formation in the spinal cord-injured ~ a t i e n t . ~ Theoretically, minimizing the pain of immobilization may decrease voluntary movement and therefore decrease the likelihood of secondary injury.2
The current study was designed to assess the differences in dis- comfort, cervical spine (c-spine) immobilization, and sacral trans-

726 ACADEMIC EMERGENCY MEDICINE AUG 1995 VOL 21NO 8
cutaneous 0, tension for the two immobilization groups, i.e., those immobilized on a padded vs an unpadded long spine board.
I METHODS ...............................................................................................................
Study Design This was a prospective, nonblinded, randomized,
controlled crossover comparison trial of spinal immo- bilization with and without padding using a convenience sampling of 30 volunteers to assess the differences in discomfort, c-spine immobilization, and sacral trans- cutaneous O2 tension.
Population and Study Site The study was performed at the Louisiana State
University emergency medicine (EM) residency pro- gram using 30 healthy volunteers studied over a two- week period. Participants included men and women aged 23-60 years with no previous history of spinal injury or disease. Subjects were excluded if they had a history of spinal injury, if they had prior spine board immobilization, or if they were women who were preg- nant or lactating. Institutional human subject research committee approval and patient informed consent were obtained prior to the initiation of the study.
Experimental Protocol Healthy volunteers were recruited from a popula-
tion of hospital employees and university residents; se- lection was by one of the authors of the study. After written informed consent was obtained, a transcuta- neous O2 tension (PtCo2) sensor was fmed to the sacral area. Subjects were randomized to either half-inch closed- cell foam- padded (Ferno-Washington, Wilmington, OH) or unpadded long spine board immobilization. Straps secured the chest, pelvis, and legs to the board. No attempt was made to blind the subjects or evaluators to the type of spine board used. Cervical immobilization for all patients consisted of a Philadelphia cervical collar with lateral support devices (sandbags) and regular ad- hesive tapes. The tapes were placed from one side of the board to the other across the forehead and chin. After completion of measurements (described below), the subjects were asked to return three to 14 days later to complete the other half of the study using the other type of long spine board.
Measurements The subjects were asked to exert maximum effort
while cervical flexion, extension, lateral rotation, and lateral bending were recorded. A hand-held bubble
goniometer was used by one of the investigators trained in the use of the instrument to measure flexion and extension according to the method described by Fisher et al.‘ Lateral rotation and lateral bending were mea- sured using an inclinometer.
Patient discomfort was determined using an unnum- bered lO-cm visual analog scale (VAS). The scale had no markings except “no pain” at one end (0 cm) and “worst pain” at the opposite end (10 cm). The subjects recorded their levels of pain or discomfort at the time of immobilization and again in 30 minutes. Sacral Ptco2 was measured using a Radiometer transcutaneous PO,/ PCO, monitoring system (Model Number TCM3, West Lake, OH). Values were measured immediately prior to immobilization and again at 30 minutes after im- mobilization. These values were recorded and used for comparison.
Data Analysis Statistical analyses were performed using Statistical
Ailalysis Software (SAS Institute, Inc., Cary, NC) Gen- eral Linear Models Procedure. Cervical ranges of mo- tion and drops in PIco2 values between the unpadded and padded groups were compared using analysis of covariance. The study had an 80% power to detect an absolute change in range of motion of 20% and to detect an absolute change in transcutaneous O2 tension of 50% in the padded vs unpadded groups. Patient discomfort differences at the 30-minute comparisons were deter- mined using the Wilcoxon signed-ranks method. An a- level of 0.05 was used throughout. Descriptive statistics for continuous variables are provided as mean f SD.
I RESULTS
The participants were aged 32.5 & 7.0 years. Four women and 26 men volunteered. The participants weighed 72 5 12 kg. Patient discomfort at 30 minutes was signif- icantly less with the padded board (mean 2.5 +. 2.1 cm) than it was with the unpadded board (mean 5.4 2 4.6 cm) using the VAS (p = 0.024). The baseline (time zero) discomfort levels also were lower with the padded board (mean 2.8 vs 5.3 cm) on the VAS.
The absolute drop in Ptco2 from time zero to 30 minutes with the padded board was 14.8 2 17.5 vs 12.2 2 16.8 percent with the unpadded board (p = 0.906). Baseline Ptco2 values were not significantly different for the padded vs the unpadded boards (mean 56.0% vs 67.3%).
There was no statistically significant difference in cervical range of motion between immobilization on the padded board and immobilization on the unpadded board (Table 1). The mean differences in range of motion with the two boards were 0.0” for cervical flexion (95%
...............................................................................................................
Padded Spine Board, Walton et al. 727
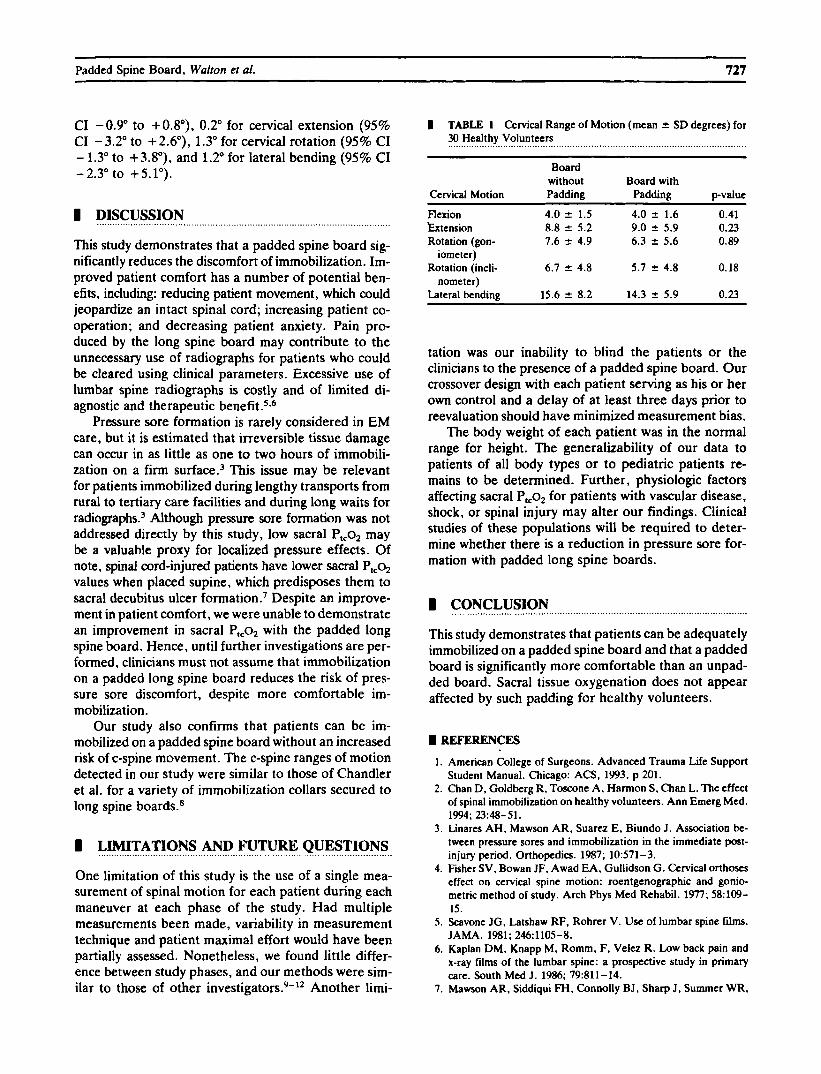
CI -0.9" to +0.8"), 0.2" for cervical extension (95% CI - 3.2" to + 2.6"), 1.3" for cervical rotation (95% CI - 1.3" to +3.8"), and 1.2" for lateral bending (95% CI -2.3" to +5.1").
I DISCUSSION
This study demonstrates that a padded spine board sig- nificantly reduces the discomfort of immobilization. Im- proved patient comfort has a number of potential ben- efits, including: reducing patient movement, which could jeopardize an intact spinal cord; increasing patient co- operation; and decreasing patient anxiety. Pain pro- duced by the long spine board may contribute to the unnecessary use of radiographs for patients who could be cleared using clinical parameters. Excessive use of lumbar spine radiographs is costly and of limited di- agnostic and therapeutic b e n e f i ~ ~ , ~
Pressure sore formation is rarely considered in EM care, but it is estimated that irreversible tissue damage can occur in as little as one to two hours of immobili- zation on a firm ~ u r f a c e . ~ This issue may be relevant for patients immobilized during lengthy transports from rural to tertiary care facilities and during long waits for radiograph^.^ Although pressure sore formation was not addressed directly by this study, low sacral PlCo2 may be a valuable proxy for localized pressure effects. Of note, spinal cord-injured patients have lower sacral P,$ values when placed supine, which predisposes them to sacral decubitus ulcer formation.' Despite an improve- ment in patient comfort, we were unable to demonstrate an improvement in sacral Plco2 with the padded long spine board. Hence, until further investigations are per- formed, clinicians must not assume that immobilization on a padded long spine board reduces the risk of pres- sure sore discomfort, despite more comfortable im- mobilization.
Our study also confirms that patients can be im- mobilized on a padded spine board without an increased risk of c-spine movement. The c-spine ranges of motion detected in our study were similar to those of Chandler et a]. for a variety of immobilization collars secured to long spine boards.8
I LIMITATIONS AND FUTURE QUESTIONS
One limitation of this study is the use of a single mea- surement of spinal motion for each patient during each maneuver at each phase of the study. Had multiple measurements been made, variability in measurement technique and patient maximal effort would have been partially assessed. Nonetheless, we found little differ- ence between study phases, and our methods were sim- ilar to those of other investigator^.^-'^ Another limi-
...............................................................................................................
I TABLE 1 Cervical Range of Motion (mean k SD degrees) for 30 Healthy Volunteers ................................................................................................................
Board without Board with
Cervical Motion Padding Padding pvalue
kxtension 8.8 2 5.2 9.0 k 5.9 0.23 Rotation (gon- 7.6 z 4.9 6.3 5.6 0.89
Flexion 4.0 2 1.5 4.0 & 1.6 0.41
iometcr)
nometer) Rotation (incli- 6.7 2 4.8 5.7 2 4.8 0.18
Lateral bending 15.6 -c 8.2 14.3 2 5.9 0.23
tation was our inability to blind the patients or the clinicians to the presence of a padded spine board. Our crossover design with each patient serving as his or her own control and a delay of at least three days prior to reevaluation should have minimized measurement bias.
The body weight of each patient was in the normal range for height. The generalizability of our data to patients of all body types or to pediatric patients re- mains to be determined. Further, physiologic factors affecting sacral Ptco2 for patients with vascular disease, shock, or spinal injury may alter our findings. Clinical studies of these populations will be required to deter- mine whether there is a reduction in pressure sore for- mation with padded long spine boards.
I CONCLUSION
This study demonstrates that patients can be adequately immobilized on a padded spine board and that a padded board is significantly more comfortable than an unpad- ded board. Sacral tissue oxygenation does not appear affected by such padding for healthy volunteers.
...............................................................................................................
I REFERENCES
1.
2.
3.
4.
5.
6.
7.
American College of Surgeons. Advanced Trauma Life Support Student Manual. Chicago: ACS. 1993, p 201. Chan D. Goldberg R, Toscone A , Harmon S, Chan L. The effect of spinal immobilization on healthy volunteers. Ann Emerg Med.
Linares AH, Mawson AR, Suarez E, Biundo J . Association be- tween prcssure sores and immobilization in the immediate post- injury period. Orthopedics. 1987; 10571-3. Fisher SV. Bowan JF, Awad EA. Gullidson G . Cervical orthoscs effect on cervical spine motion: roentgenographic and gonio- metric method of study. Arch Phys Med Rehabil. 1977; 58:109- 15. Scavone JG. Latshaw RF, Rohrer V. Use of lumbar spine films.
Kaplan DM, Knapp M, Romm, F, Velez R. Low back pain and x-ray films of the lumbar spine: a prospective study in primary care. South Med J . 1986; 79:811-14. Mawson AR, Siddiqui FH, Connolly BJ, Sharp J , Summer WR,
1994; 23~48-51.
JAMA. 1981; 246:1105-8.
7211 ACADEMIC EMERGENCY MEDICINE AUG 1995 VOL 2/NO 8
Biundo JJ . Sacral transcutaneous oxygen tension levels in the spinal cord injured: risk factors for pressure ulcers? Arch Med Rehabil. 1993; 74:745-51.
8. Chandler DR, Nemeji C, Adkins RH, Waters RL. Emergency cervical spine immobilization. Ann Emerg Med. 1992; 21:1185- 8.
9. Howell J , Burrow R, Dumontier C, Hillyard A. A practical ra- diographic comparison of short board technique and Kendrick extrication device. Ann Emerg Med. 1989; 18:943-6.
10. Graziano AF, Scheidel EA, Cline JR, Baer U. A radiographic
comparison of prehospital cervical immobilization methods. Ann Emerg Med. 1987; 16:1127-31.
11. Podolsky S. Baraff U, Simor RR, Hoffman JR. Larmon B, Ablon W. Efficacy of cervical spine immobilization collars. J Trauma. 1983; 23:461-5.
12. Rosen PB, McSwain NE, Arata M, Stahl S, Mercer D. Com- parison of two new immobilization collars. Ann Emerg Med. 1992; 21:1189-95.
CALL FOR ABSTRACTS 1996 Annual Meeting
May 6-9 Adams Mark Hotel - Denver, Colorado M
The Program Committee is accepting abstracts for review for oral and poster presentation. Authors are urged to submit original work in all aspects of Emergency Medicine including cerebral resuscitation, pediatrics, cardiopulmonary resuscitation, medical toxicology, administration, trauma, EMS, shock, basic science, injury prevention, health policy research, education, infectious disease, neurologic trauma, and methodology. Abstract submission forms are available upon request to the SAEM office and will be published in the November 1995 issue of the SAEM newsletter. Abstracts not submitted on the official abstract form or not conforming to the instructions will not be considered. Call (5 17) 485-5484 to request an abstract form or obtain further information. Abstracts submitted or the resultant manuscripts must not appear in a refereed journal prior to publication of the Annual Meeting abstracts in the May 1996 issue of Academic Emergency.Medicine. Abstracts presented at other national meetings within 30 days of the 1996 S A E M Annual Meeting will be considered for presentation. SAEM strongly recommends that authors submit their manuscripts to Academic Emergency Medicine. Academic Emergency Medicine will notify authors of a decision regarding publication within 60 days of receipt. AU abstracts must be submltted on the official abstract form, and must be received no later than January 10,1996. Abstracts and correspondence should be sent to:
SAEM Annual Meeting Abstracts 90 1 North Washington Avenue
Lansing. MI 48906 Awards will be given for the best abstracts in the following categories: Clinical Oral (Human Subjects), Basic Science Oral, Education, ResidentFellow Oral, Poster, Innovation in Medical Education Exhibit, ResidenVFellow Poster, Medical Student, Technology, and Pediatric Emergency & Critical Care. Awards will be presented at the 1997 Annual Meeting.