Embed Size (px)
Citation preview

Injury, Int. J. Care Injured 45 (2014) 176–182
Paediatric extremity vascular injuries – Experience from a large urbantrauma centre in India
Jiten Jaipuria, Sushma Sagar *, Maneesh Singhal, Amit Bagdia, Amit Gupta, Subodh Kumar,Biplab Mishra
Department of Trauma Surgery, Jai Prakash Narayan Apex Trauma Centre, All India Institute of Medical Sciences, New Delhi, India
A R T I C L E I N F O
Article history:
Accepted 4 August 2013
Keywords:
Paediatric trauma
Non-iatrogenic vascular injury
Vascular repair
Extremity
Morbidity
Mortality
A B S T R A C T
Introduction: Paediatric extremity vascular injuries are infrequent, and management protocols draw
significantly from adult vascular trauma experience necessitating a continuous review of evidence.
Materials and methods: A retrospective registry review of all consecutive patients younger than 18 years
age treated for extremity vascular trauma from 2007 to 2012 was carried out. Diagnostic algorithm
relied little on measurement of pressure indices. Data was collected about demographics, time since
injury, pattern of injury, ISS, initial GCS and presence of shock, results of diagnostic modality and
treatment given with associated complications. Patients completing 2 years follow up were assessed for
functional disability and vascular patency. A multivariable regression model was used to evaluate effects
of – ISS, presence of orthopaedic injury, soft tissue injury, neural injury and arterial patency at the end of
2 years – on outcome of functional disability.
Results: Paediatric extremity vascular injuries accounted for 0.68% hospital admissions with a median
delay of 8 h from injury. 82 patients were included with 50 cases examined for long term outcome.
Patient cohort was overwhelmingly male, with ‘fall’, ‘road traffic injury’ and ‘glass cut’ being most
common injury mechanisms. CT angiography and duplex scan based diagnostic algorithm performed
satisfactorily further identifying missed injuries and aiding complex orthopaedic reconstruction.
Brachial and femoral vessels were most commonly injured. Lower extremity vascular injury was found
associated with significantly higher ISS and requirement for fasciotomy. Upper extremity vascular injury
was associated with higher odds of neural injury. Younger children were at higher risk of combined
radial and ulnar vessel injury. No patient satisfactorily complied with post-operative anticoagulant/
antithrombotic prophylaxis. 28 patients had good functional outcome with unsatisfactory functional
outcome found associated with significantly higher ISS, presence of orthopaedic and neural injury, along
with absence of arterial patency.
Conclusion: The epidemiology of paediatric peripheral vascular injury differs in India compared to west.
Certain traditional management principles of extremity vascular trauma may stand uniquely challenged
in the paediatric population.
� 2013 Elsevier Ltd. All rights reserved.
Contents lists available at ScienceDirect
Injury
jo ur n al ho m epag e: ww w.els evier . c om / lo cat e/ in ju r y
Introduction
Paediatric vascular injuries are fortunately infrequent; even inbusy dedicated paediatric trauma centres, with an overallestimated annual incidence of 0.6% among hospital admittedinjured children in United States of America based on records fromNTDB (National Trauma Data Bank) [1]. Population based (or evenhospital based) Indian data in this regard is scarce; a problemcompounded by the lack of a national trauma registry and
* Corresponding author at: Department of Surgical Discipline and Trauma Care,
Jai Prakash Narayan Apex Trauma Centre, All India Institute of Medical Sciences, Raj
Nagar, New Delhi 110029, India. Tel.: +91 11 9891510122; fax: +91 11 26589667.
E-mail addresses: [email protected], [email protected]
(S. Sagar).
0020–1383/$ – see front matter � 2013 Elsevier Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.injury.2013.08.002
organised trauma care being only in its infancy. Traditionally mostof diagnostic and therapeutic modalities used while treating suchinjuries in paediatric population has drawn from adult vascularinjury experience; necessitating a continuous review of data frompaediatric population [2].
Jai Prakash Narayan Apex Trauma Centre (JPNATC) is among thebusiest tertiary trauma care facilities in India with its emergencydepartment visited annually by more than 50,000 patients. Indialacks a dedicated paediatric trauma care centre and thus JPNATCalso extends its services to all paediatric trauma cases to acatchment area exceeding the boundaries of Delhi; to nearbyneighbouring states; thus serving a potential overall population ofmore than ten million people.
This study reviews our experience in dealing with paediatricperipheral vascular trauma from 2007 to 2012; with a special focus

Suspected peri pheral vasc ula r tra umabased on either har d* or so�# signs of vascular injury and s table vital si gns in
a child in wa rm surround ings
Pen etra�ng injury Blunt injury
Hard* si gns of vascular injury
Vascula r interven�on at the
earliest ∑
Op�onal Ω
CT angiography (consi der if C T s can nec essary for othe r
indica�ons α)
or
Dup lex scan
[for accurate localisa�on of
vascular injury if f elt nec essary by t he
surgeon]
So�# signs of vascular injury Har d* si gns of vascular injury
Eval uat e wit h ali gnment of possible culprit fractu res
Individ ual ise β
Observe
CT angiogra phy (consi der if C T
scan felt nec essary for other
indica� ons α)
OR
Duplex sca n
Vascula r inte rven� on a t the ear lies t ∑
Treat other injuries an d Observe with � mely
clinica l re-eval ua� on of vascular sta tus
Normal s tud y Abnormal stu dy
CT angiogra phypreferred (Duple x scan if CT scan felt
unnecessary or contrai ndica ted )
Inves �ga� on pre ferred prior to any surgica l
interven�on for accurat e local isa� on of
vascular injury Ω
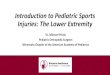
Fig. 1. JPNATC Algorithm followed for diagnosis and further management of
extremity vascular injuries in the paediatric population during the secondary
survey. *Hard signs of vascular injury include absent distal pulses or distal ischemia
(pulselessness, pallor, paraesthesia, pain, paralysis), bruit or thrill at injury site,
active pulsatile haemorrhage, large, pulsatile, or expanding hematoma. #Soft signs
of vascular injury include small or stable hematoma over an artery, neural deficit
originating in a nerve adjacent to a named peripheral artery, history of moderate
haemorrhage at scene, history of unexplained hypotension, diminished but
palpable pulse, and proximity of injury to major vessels.a
Indication for a CT
scan may include for example bullet injuries or associated skeletal injuries or other
organ system trauma qualifying independently as an indication for contrast
enhanced CT evaluation. CT angiography may also be considered when a duplex
scan cannot be done or if it is inadequate or unsatisfactory due to anatomical or
other constraints and vascular lesion localisation and characterisation is felt
necessary.b
Institutions with established protocols (and a clinically eligible patient
for accurate measurement) for ankle brachial pressure (ABPI) or Arm Pressure Index
measurements may choose to individualise decision based on criteria - if ABPI or
Arm Pressure Index is <0.9 or normal - with sometimes only observation for those
with normal values based on age adjusted nomograms. Observation may also be
appropriate upon consideration of number and/or combination and/or type of
individual soft signs present; more so in conjunction with exam findings of equally
palpable pulse in affected and contra lateral extremity.V
No undue delay waiting for
any radiological investigation should occur.S
Intraoperative (or even pre-operative)
catheter guided angiography may be considered as appropriate for gold standard
radiologic assessment of vascular status; more so if in case preoperative radiologic
evaluation was not done due to extreme circumstances.
J. Jaipuria et al. / Injury, Int. J. Care Injured 45 (2014) 176–182 177
on long term outcome for those patients who had completed 2years of follow up.
Materials and methods
A retrospective registry review of all consecutive cases from lessthan 1 year to 18 years of age, with at least one trauma ICD 9 codefor vascular injury involving upper or lower extremity (code 903-904), from November 2007 till July 2012 was carried out; approvedby the local hospital ethics review board. The patient treatmentrecords were individually reviewed and all those with iatrogenicinjury were excluded. Patients with injury distal to wrist and ankle,injuries to un-named vessels, and mangled extremities needingprimary amputation were also excluded. Patients primarily treatedelsewhere were also excluded along with patients presenting morethan 24 h after injury to the hospital as it may preclude attempt atrevascularisation. Patients assigned an ICD vascular injury code foronly a radiological diagnosis of vasospasm, but intact distal flow,were also excluded after review and confirmation of individualrecord for lack of any vascular intervention. Data was collectedabout age, gender, month of the year, time since injury, pattern ofinjury with associated injuries, ISS, initial GCS score and presenceof shock at admission, results of diagnostic modality and treatmentgiven with associated complications. Fig. 1 illustrates thediagnostic and management protocol followed for managementof such injuries in JPNATC. With a multi-disciplinary approach,after initial bone realignment (by external fixator or K wire, if feltnecessary); vascular intervention was performed in all cases withdefinitive orthopaedic reconstruction at the end. Isolated radio-logical finding of vasospasm in presence of intact distal flow wasmanaged conservatively. All vessels with ‘no immediate return offlow’ following orthopaedic stabilisation were explored. Finding ofany vasospasm during vascular exploration was managed by localirrigation and intra-arterial injection of papaverine (preferred) orlidocaine (along with other conservative measures like warming,hydration and relieving any extrinsic compression) followed byFogarty thrombectomy in case of non-return of flow within 10–15 min. All vascular anastomoses were performed by interruptednon-absorbable sutures by surgeons from plastic surgery and/ortrauma service. Both microscope and corneal loupe are availableand were used as per surgeon choice. Intra-operatively, a bolusdose of heparin (if other injuries permitted) as per patient weightwas used prior to vascular clamping and the local anastomotic sitewas also irrigated with dilute heparin (0.1%). Artificial grafts wereePolytetrafluoroethylene (ePTFE), and their use was restricted tofemoral vessels in patients approaching adulthood; unlessunavoidable in younger children. Practice of ‘on table completionangiography’ following vascular reconstruction is not followed inJPNATC due to lack of intra-operative angio-suite. Confirmation ofsuccessful revascularisation was done by a palpable pulse inconjunction with Doppler evaluation if necessary. The indicationsfor fasciotomy were palpably tense compartments, major veinligation, hypovolemic shock, ischaemia lasting more than 6 h, andany motor or sensory deficits. Objective compartment pressuremeasurements were not done. Post-operatively all patients whohad undergone reverse interposition vein grafting were prescribedvitamin K antagonist for 3 months with a target InternationalNormalised Ratio (INR) above 2, and all patients that underwentsynthetic graft bypass procedures were prescribed antiplatelettherapy (75 mg aspirin/day; with dose modification (1–5 mg/kg/day) for younger children] for a similar duration. Our institutionavoids endovascular procedures in paediatric population due tolack of convincing evidence on long term outcomes.
Patients completing 2 years follow up from initial date of injurywere telephonically contacted and called to JPNATC for indepen-dent examination by two trauma surgeons and review of follow up
records. Long term outcome was assessed by clinical examinationfor functional disability; supplemented by non-invasive duplexultrasound for arterial patency if felt necessary based on finding ofabsent or differentially weak pulse distal to vascular repair by anyof the two examiners. The functional outcome was assessed by asubjective ordinal scale of disability as none, mild, moderate,severe, amputation, or death (related to trauma episode under

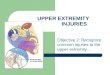
Fig. 2. Overall population characteristics and pattern of injury along with further
stratification based on gender.
J. Jaipuria et al. / Injury, Int. J. Care Injured 45 (2014) 176–182178
study) with score given from 0 to 5 for each ordinal outcome alongwith findings of a regular orthopaedic exam. Independent scoreswere given by each of the two examining trauma surgeons whileinterviewing the patient together; and final scores were created bypooling the results, with resolution of any difference in individualscores by mutual discussion with adoption of one final score foreach patient. The examiners primarily judged scores based onasking open ended questions in history regarding three broad areas– performance in daily activities/usual/unusual work, recreationand pain/discomfort – coupled with exam findings. The patientwas also asked to self-assign a score (where feasible based on ageand understanding of patient and/or guardians) and it was stronglyconsidered in arriving at the final score. For the purpose ofanalyses; the final functional outcome was converted to a binaryvariable; with all patients having a functional outcome score �1(subjective ‘none’ to ‘mild’ functional disability) assigned to the‘‘good functional outcome’’ category, and remaining assigned tothe ‘‘unsatisfactory functional outcome’’ category (functionaloutcome score �2; from ‘moderate’ functional disability to ‘severe’disability, amputation and death).
Quantitative data were compared with Mann Whitney U testand proportions compared using chi-squared test (with Yates’correction for continuity as appropriate) or the chi-squared trendtest (when looking for trends) when dealing with largercontingency tables; with odds ratios (OR) reported with 95%confidence intervals (CI) with appropriate corrections. Alpha errorwas set before-hand at 0.05 with two tailed distribution. Data areshown as numbers (%), mean [standard deviation (SD)] or median[interquartile range (IQR)]. A univariable analyses was done toevaluate the effect of – age, gender, ISS, extremity (upper or lower),mechanism of injury, time since injury, presence of shock atadmission, admission GCS, orthopaedic injury, soft tissue (muscle/tendon/ligament) injury, vascular patency at end of 2 years, andneural injury – on the variable of functional outcome at the end of 2years. All variables with a p value of <0.2 were then entered into amultivariable logistic regression model to determine final effectsize and odds ratios.
Results
During the study period more than 200,000 patients weretreated in JPNATC, with 20,456 hospital admissions. 136 paediatric
Table 1Details of pattern of injury in the entire study population divided into various age gro
Pattern of injury Age groups
<6 years (n = 18) 6–
Blunt, n (%) 14 15
Rail-track injury 0 0
Road traffic injury 4 4
Falls 7 9
Unknown 1 0
Crush under heavy object 2 2
Mortality 0 1
ISS (median, IQR) 11 (9–13) 9
Amputation 0 2
Penetrating, n (%) 4 13
Glass cut 0 5
Machinery 2 6
Rod impalement 1 0
Knife/sharp handheld instrument 0 0
Gunshot 0 0
Unknown 1 1
Mortality 0 0
ISS, median (IQR) 9 (8–9) 9
Amputation 1 2
n = number of patients.
patients with vascular injuries to the extremities were admitted,with 82 patients finally meeting the inclusion criteria for the study.Thus paediatric vascular injuries accounted for 0.68% of hospitaladmissions. The median time to arrival at hospital following injurywas 8 h (IQR 3–9 h).
Injury pattern
Overall males constituted majority of total population and weresignificantly older than females (p value 0.0029, Fig. 2); however
ups.
13 years (n = 28) 14–18 years (n = 36) Total (n = 82)
17 46 (56%)
2 2
10 18
5 21
0 1
0 4
1 2
(5.25–9) 9 (9–16) 9 (9–13)
1 3
19 36 (44%)
12 17
2 10
2 3
3 3
1 1
0 2
0 0
(8–10) 9 (7.75–16) 9 (8.5–9.5)
0 3

0
2
4
6
8
10
12
14
16
Jan
Feb
Mar
Apr
May Jun Jul
Aug
Sep
Oct
Nov De
c
Numb er of pa�ents
month of the year
admissio n due vas cular injury
admissio n due to vas cular injury by farm mac hinery
Fig. 3. Monthly trend of hospital admissions due to vascular injury with
comparative trend of admissions with vascular injury due to farm machinery.
Fig. 4. Prevalence of musculoskeletal and peripheral nerve injury associated with
peripheral vascular trauma to upper and lower extremities (excluding patients with
complete or near total traumatic amputations with attempted re-implantation).
J. Jaipuria et al. / Injury, Int. J. Care Injured 45 (2014) 176–182 179
females constituted equal proportion among those between 1 and5 years. Blunt pattern of injury was more common overall butpenetrating injuries showed a progressively increasing trend(p = 0.043) till they became more common in the 14–18 years agegroup. Children less than 6 years old had higher odds of sufferingfrom blunt injury than the rest of the population closelyapproaching statistical significance (OR 3.5, CI 1.04–11.79). ‘Fall’,closely followed by ‘road traffic injuries’ constituted the mostcommon cause of blunt trauma and ‘glass cut’ was the mostcommon cause of penetrating injuries (Table 1). A high proportionof penetrating injuries were caused by machinery (n = 10, farmmachinery constituting majority, n = 9); seen most commonly inthe 6–13 years age group, and became infrequent as the childapproached adulthood. Overall victims of blunt trauma showed atrend for higher ISS values (as observed by the IQR) though notstatistically significant. Most admissions due to extremity vascularinjuries were seen in summer, and then again in the beginningmonths of winter season (Fig. 3). Farm machinery injuries werepredominantly seen from months of May to July and then again inOctober; coinciding with the harvest season of crops. Upper limbwas more commonly injured than the lower limb (prevalence ratio1.82) with brachial artery being the most common injured vesselfollowed by femoral artery (Table 2). Isolated venous injury was
Table 2Details of specific vessels injured in the entire study population divided into various a
Vessel injured Age groups
<6 years (n = 18)
Upper extremity, n (%) 9
Axillary artery 0
Brachial artery 5
Radial artery 0
Ulnar artery 0
Both radial and ulnar vessels 4
More than 2 arteries 0
Axillary vein 0
Brachial vein 0
ISS (median, IQR) 9 (5.25–9)
Amputation 1
Lower extremity, n (%) 9
Femoral artery 6
Popliteal artery 2
Anterior tibial/posterior tibial/peroneal artery 1
Femoral vein 1
Popliteal vein 0
ISS (median, IQR) 13 (13–14)
Amputation 0
n = number of patients.
not seen. With decreasing age the relative frequency of combinedradial and ulnar artery injury at the wrist increased as compared toinjury of either vessel alone. The median ISS with lower limbvascular injury was significantly higher than with vascular injuryto the upper limb (p < 0.0001). Upper limb vascular injuries hadsignificantly higher odds of being associated with motor nerveinjuries (OR 7.94, CI 2.10–29.98, p value 0.0019, Fig. 4). The odds oforthopaedic and soft tissue injury were not significantly differentbetween upper or lower extremity.
Diagnosis and management
51 CT angiograms and 8 duplex scans were performed as part ofdiagnostic algorithm outlined in Fig. 1. No adverse events werenoted attributable to the diagnostic modality; although this studylacks experience with children below 2 years age. Findings of CTangiogram correlated with operative findings in all cases, however
ge groups.
6–13 years (n = 28) 14–18 years (n = 36) Total (n = 82)
24 20 53 (65%)
2 2 4
15 6 26
0 3 3
2 5 7
4 3 11
1 1 2
1 0 1
2 0 2
9 (8.5–9.5) 9 (5–9) 9 (6–9)
3 0 4
4 16 29 (35%)
2 10 18
0 3 5
2 4 7
0 3 4
0 1 1
9 (5.25–14.25) 16 (10.75–16) 15 (9–16)
1 1 2

Table 3Type of vascular injury encountered in the entire population (includes 83 arterial
and 8 venous injuries).
Type of vascular injury Extremity
Upper extremity Lower extremity
Occlusion/thrombus, n (%) 6 (11%) 9 (26%)
Transection, n (%) 32 (57%) 13 (37%)
Laceration, n (%) 9 (16%) 8 (23%)
Spasm, n (%)a 6 (11%) 2 (6%)
Pseudoaneurysm, n (%) 0 1 (3%)
Entrapment, n (%) 3 (5%) 2 (6%)
Total vascular injury burden 56 35
There were 53 patients with upper extremity vascular injury and 29 patients with
lower extremity vascular injury.a Includes only those cases which underwent operative exploration and
additional intervention directed towards either vessel or soft/hard tissues to
relieve the spasm.
J. Jaipuria et al. / Injury, Int. J. Care Injured 45 (2014) 176–182180
3 cases diagnosed with arterial spasm were found to contain anassociated thrombus and flow was restored with Fogartythrombectomy. On the contrary none of the 12 cases assigned atrauma vascular injury ICD 9 code for radiological confirmedvasospasm, with intact distal flow, required vascular intervention(subjects excluded from the study).
Duplex scans were performed only in patients with soft signs ofinjury and 3 cases were explored based on positive findings with100% correlation with scan results; no case required unplannedoperative intervention. One 17 year old referred patient with gun-shot injury in vicinity to popliteal artery and initial normal vascularexam and CT angiogram; developed pseudoaneurysm withinhospital stay with increasing pain, limitation of movement andswelling in the popliteal fossa. Repeat CT angiogram confirmed thesame, and he was managed surgically. No other patient chosen forconservative management based on CT angiogram requiredsubsequent vascular operative intervention. Importantly, CT scanidentified skeletal injuries missed on plain radiographs in 14patients (12 of which had suffered from blunt trauma) and aided inplanning orthopaedic management of complex bone and jointinjuries in 6 cases (mainly involving the physes). There was nosignificant difference in the type of vascular injury encounteredbetween the two extremities (Table 3); with ‘transection’ observedmost commonly. Most injuries could be dealt by simple procedures;with end to end repair being the commonest intervention performed(Table 4). Temporary vascular shunt was not used in any case.Fasciotomy was performed more often in the management of lowerextremity injuries than the upper extremity (OR 8.77 CI 2.17–35.37,p value 0.0019). Artificial ePTFE grafts were used in 4 patientsapproaching adulthood for femoral artery bypass.
10 patients were eligible for postoperative anticoagulant/antithrombotic prophylaxis; however their follow up records
Table 4Type of vascular intervention along with related procedures performed in the entire p
Type of vascular intervention (% among total vascular injury burden)
Thrombectomy alone, n (%)
Primary repair, n (%)
End to end anastomosis, n (%)
Reverse interposition vein grafting, n (%)
Artificial graft, n (%)
Ligation, n (%)
No vascular intervention,a n (%)
Total vascular injury burden
Fasciotomy, n (% among number of patients)
n = number of instances.
Overall significantly different values highlighted with bold text.a Includes cases with surgical release of vessel from entrapment, fasciotomy alone for
arterial irrigation of papaverine or lidocaine, and observation of certain other injuries
showed inadequate compliance in every case, although no adverseeffects related to anti thrombotic therapy were documented.
Complications and outcome
Two deaths were seen among patients with blunt mechanism ofinjury caused by multi organ failure as a consequence of poly-trauma, with no mortality seen among patients with penetratingmechanism of injury. Overall limb salvage rate was 93%, with 6patients needing subsequent limb amputation following initialvascular reconstruction involving 4 upper and 2 lower extremities.Three cases needing subsequent upper extremity amputation hadtraumatic hand amputation following machinery injury aspresenting profile, while one patient had brachial artery injurywith haemorrhage in the post-operative period following initialreverse interposition vein grafting. Overall 7 hand re-plantationswere attempted with success in 4 cases. Both cases of subsequentlower extremity amputation had failed reconstruction withreverse saphenous vein graft following injury to femoral andpopliteal artery respectively. Limb was salvaged in all patientswith ePTFE grafts (n = 4); however 2 patients developed infectionin soft tissues in the vicinity of the graft, and graft was rejected, 6and 12 months following initial surgery. Skin and soft tissue coverwas mostly provided with split skin grafts (n = 36), however 13cases required local/pedicle flap coverage and 5 cases required freetissue transfer.
62 patients had completed 2 years following initial injury andwere sought for follow up, of which 49 patients responded;remaining 9 cases were lost permanently to follow up, 3 refused tocome for examination due to convenience issues and 1 death wasassigned unsatisfactory functional outcome by default. None of the49 cases had any component of head injury.
Other than amputation; limb length discrepancy was noted in 5cases (3 lower and 2 upper extremities) with contractures and/orbone length shortening as contributing factors. No patient gavehistory suggestive of claudication although functional limitationwas noted in 22 patients. 10 patients gave history and/or showedphysical signs of sensory and/or motor neuropathy.
Table 5 shows the comparison of various factors in relation togood versus unsatisfactory functional outcome and only soft tissueand neural injury were found significantly different in theunivariable analyses. Interestingly, in the final model soft tissueinjury emerged no longer significant (OR 0.42, CI 0.04–3.91, p value0.44), while all other variables assumed significance with overallarea under ROC curve of 0.847. Patients with unsatisfactoryfunctional outcome had significantly higher adjusted odds ofhaving – neural injury (OR 37.33, CI 2.33–597.5, p value 0.01);orthopaedic injury (OR 7.66, CI 1.14–51.25, p value 0.035); absence
opulation (includes 83 arterial and 8 venous injuries).
Extremity
Upper extremity (n = 53) Lower extremity (n = 29)
9 (16%) 4 (11%)
9 (16%) 5 (14%)
18 (32%) 8 (23%)
12 (21%) 5 (14%)
0 4 (11%)
3 (5%) 2 (6%)
5 (9%) 7 (20%)
56 35
3 (6%) 10 (34%)
restoration of blood flow, relief of vascular spasm with local infiltration and intra-

Table 5Comparison of various factors and good versus unsatisfactory functional outcome.
Variable Functional outcome (n = 50) p-Value
Good (functional outcome score � 1), n = 28 Unsatisfactory (functional outcome score � 2), n = 22
Age, median (IQR) 9.5 (6–16) 12 (7–17) 0.42
Gender, male, n (%) 22 (79%) 18 (82%) 0.77
Extremity, lower, n (%) 10 (36%) 7 (32%) 0.77
Time since injury, hours, median (IQR) 7 (3–8) 8 (4–8) 0.30
ISS,a mean (SD) 9.07 (4.08) 10.91 (3.94) 0.11
Presence of shock at admission, n (%) 4 (14%) 6 (27%) 0.43
Admission GCS, mean (SD) 14.1 (2.8) 13.2 (3.7) 0.31
Mechanism of injury, blunt, n (%) 18 (64%) 11 (50%) 0.47
Orthopaedic injury,a n (%) 14 (50%) 16 (72%) 0.18
Soft tissue injury,a n (%) 6 (21%) 11 (50%) 0.069Neural injury,a n (%) 4 (14%) 11 (50%) 0.015Long term arterial patency,a n (%) 25 (89%) 15 (68%) 0.13
Significant p values are marked with bold text.
n = number of patientsa Variables considered for inclusion in the multivariable logistic regression model based on p value cut off.
J. Jaipuria et al. / Injury, Int. J. Care Injured 45 (2014) 176–182 181
of long term arterial patency (OR 9.68, CI 1.05–89.47) and possiblyhigher ISS scores (OR 1.21, CI 0.99–1.48, p value 0.059).
Discussion
This study highlights aspects on epidemiology of an importantproblem about which little literature exists from the Indiansubcontinent. Surprisingly, while paediatric vascular injuriesaccount for average 0.6% admissions among all paediatric traumavictims in United States; this figure stands at 0.68% of all hospitaladmissions (including adults) in JPNATC [1,3]. Interestingly, thecause of injuries differ markedly from the west too; where ‘motorvehicle crash’, followed by ‘gun-shot’ and ‘stab’ are the three maincauses of vascular injury; while we found ‘falls’ followed by ‘roadtraffic injuries’ and ‘glass cut’ to be the three most common causesof vascular trauma in our scenario [1]. High proportion ofmachinery injuries in younger children are a cause of concern.The finding of relative higher frequency of combined radial andulnar artery injury at the wrist in younger age group childrenhighlights the immediate gravity that such injuries may pose to thetreating team.
A diagnostic algorithm, similar in elements to adult vasculartrauma; with emphasis on ankle brachial pressure index (ABPI)measurements (cut off 0.9), has been recently proposed forpaediatric population [3]. Our experience and a critical scrutiny ofavailable evidence highlight many areas of theoretical andpractical concern. There may be cases where it may be simplyunfeasible to obtain ABPI values due to anatomical constraints ofinjury (soft tissue swelling/raw area/fractures). Moreover, the useof correct cuff size cannot be overemphasised, and the method tomeasure ABPI must be standardised as per current guidelines, asotherwise significant errors may creep in primary measurement, aswell intra- and inter-observer repeat measurements [4]. NormalABPI values may also differ in children less than 2 years age [5]. Wecould not come across any publication on paediatric vasculartrauma in English literature which documented specific details ofthe ABPI measurement method, or protocol, or evaluated itsperformance in clinical context. All these concerns, coupled withthe scarcity of regular experience with these injuries amongresidents compelled us to adopt a management algorithm, whichrelied little on ABPI. There is similar literature among adultextremity vascular injuries, which does not emphasise on pressureindex measurements in the diagnostic algorithm [6,7]. Experiencewith the performance of duplex scan and CT angiography inpaediatric population is increasing, and duplex scan has beensuccessfully used in managing vascular trauma even in pre-term
infants [8]. However, if pressure index measurements are utilised,then physicians may also find utility in the less discussed InjuredExtremity Index for diagnosing vascular injury to the upper limb,which compares Doppler occlusion pressure between both upperextremities [9].
Anticoagulant/antithrombotic prophylaxis following vascularreconstruction with autologous vein or artificial grafts in trauma isalso controversial. Authorities are divided with opinion favouringeach of – ‘not necessary in every case’ [10]; ‘in favour’ [6,7,11];while others are ‘equivocal’ [12]. Intra-operative anticoagulationduring vascular reconstruction appears more acceptable [13,14].While meta-analyses of infra inguinal arterial reconstruction inpatients with peripheral artery disease favours use of vitamin Kantagonists with autologous vein reconstruction and plateletinhibitors with artificial graft reconstruction; its findings cannot begeneralised to paediatric trauma [15]. Practically, presence of otherinjuries may also preclude anticoagulant/antithrombotic use. Ourstudy highlights another layer in complexity to this problem – theissue of ‘compliance’. The finding of universal unsatisfactorycompliance made us reassess the external validity to actual clinicalpractice of questionable benefit (if any) of anticoagulant/antith-rombotic prophylaxis.
Another vexing aspect in paediatric vascular trauma deals withassessment of long term functional outcomes. It is difficult toimagine a traditional functional outcome scale; with a fixed set ofquestions; which can evaluate functional ability of children fromless than one to18 year age. Our study humbly highlights thesobering fact that more than a successful vascular result; theultimate functional outcome depends on elements of each –vascular, neural and orthopaedic injury, superposed by globalanatomical impact of trauma on the complete individual – as seenby good functional outcomes in only 56% of victims, despitereasonable vascular patency rates. Similar findings of decreasedresidual function in 25% paediatric extremity vascular traumavictims were noted by Harris and colleagues in a cohort of 19patients with major extremity vascular trauma requiring bypass[16]. We resorted to use of multiple logistic regression; howeversimilar/improvised model on larger data stratified by pattern/typeof injury and extremity/individual vessel may be needed to form amore accurate opinion; as large confidence intervals due to smallsample size in our study testify. Moreover, human effort can onlyremain humble if one looks at the large number of hidden factorsthat may have bearing on final success or failure such as – type ofpre-hospital care and intervention, delay in operative intervention,variation in individual skill of surgeon, compliance with treatment,and possibly many more determinants.

J. Jaipuria et al. / Injury, Int. J. Care Injured 45 (2014) 176–182182
Lastly, a median delay of 8 h from time of injury to hospitalpresentation is an unhealthy trend and may adversely affectoutcomes; over which we have little control. Evidence exists thatwarm ischaemia time for skeletal muscle may be 4–8 h (may beeven lower for nerve) and forms the rationale for 6 h golden periodfor early intervention [17]. However, it must be understood that‘time since injury’ may not be the same as ‘time from completeischaemia’ and also that ischaemia may have degrees of severityinfluenced by level of arterial injury, extent of soft tissue damage,and the efficiency of collateral circulation; and thus it may not beprudent to assume that reasonable limb salvage rates are notpossible even in the 12–24 h period from the time of injury [18].Clinical examination findings at presentation must take prece-dence over absolute consideration of time from injury andsometimes it may be necessary to expose all compartments inan affected extremity to assess response to physical stimulus asmuscles may be unviable in only one compartment justifyingattempt at revascularisation [19].
Conclusion
The epidemiology and pattern of paediatric peripheral vascularinjury differ in India compared to west. Appropriately utilisedradiological investigations may prove a valuable adjunct tophysical findings in the diagnostic algorithm as well as planningmanagement. Despite a relative delay in presentation, reasonablelimb salvage and long term vascular patency rates may beachieved. Long term functional outcome however depends notonly on long term vascular patency, but also on elements oforthopaedic and neural injury, and the overall impact of trauma onthe whole individual. Certain traditional management principlesstand uniquely challenged upon closer scrutiny.
Conflict of interest statement
All authors hereby declare that there is no conflict of interest inthe publication of this paper.
Acknowledgements
Many people helped in individual and collective capacity whiledoing this study. We acknowledge the support provided by ProfMC Misra, Chief, JPNATC; Co-faculty members from EmergencyMedicine, Anaesthesia, Radiology, Orthopaedics and Lab Medicine;and not the least – the residents and nursing staff of Department ofTrauma Surgery, JPNATC. We also thank the three unknown peer
reviewers for suggestions leading to substantial improvement inthe manuscript.
References
[1] Barmparas G, Inaba K, Talving P, David JS, Lama L, Plurad D, et al. Pediatric vsadult vascular trauma: a National Trauma Databank review. Journal of Pedi-atric Surgery 2010;45:1404–12.
[2] De Virgilio C, Mercado PD. Noniatrogenic pediatric vascular trauma: a ten yearexperience at a level I trauma center. American Surgeon 1997;63:781–4.
[3] Shah SR, Wearden PD, Gaines BA. Pediatric peripheral vascular injuries: areview of our experience. Journal of Surgical Research 2009;153:162–6.
[4] Aboyans V, Criqui MH, Abraham P, Allison MA, Creager MA, Diehm C, et al.Measurement and interpretation of the ankle-brachial index: a scientificstatement from the American Heart Association. Circulation 2012;126.http://dx.doi.org/10.1161/CIR.0b013e318276fbcb.
[5] Katz S, Globerman A, Avitzour M, Dolfin T. The ankle-brachial index in normalneonates and infants is significantly lower than in older children and adults.Journal of Pediatric Surgery 1997;32:269–71.
[6] Franz RW, Shah KJ, Halaharvi D, Franz ET, Hartman JF, Wright ML. A 5-yearreview of management of lower extremity arterial injuries at an urban level Itrauma center. Journal of Vascular Surgery 2011;53:1604–10.
[7] Franz RW, Skytta CK, Shah KJ, Hartman JF, Wright ML. A five-year review ofmanagement of upper-extremity arterial injuries at an urban level I traumacenter. Annals of Vascular Surgery 2012;26:655–64.
[8] Downey C, Aliu O, Nemir S, Mathuria BN, Hatef DA, Bullocks JM, et al. Analgorithmic approach to the management of limb ischemia in infants andyoung children. Plastic and Reconstructive Surgery 2013;131:573–81.
[9] Peck MA, Rasmussen TE. Management of blunt peripheral arterial injury.Perspectives in Vascular Surgery and Endovascular Therapy 2006;18:159–73.
10. King DR. Anticoagulation in penetrating trauma. In: Velmahos GC, Degiannis E,Doll D, editors. Penetrating trauma, a practical guide on operative techniqueand peri-operative management. 1st ed., Berlin, Heidelberg: Springer-Verlag;2012. p. 537–9.
[11] Wahlberg E, Olofsson P, Goldstone J. Emergency vascular surgery, a practicalguide. Berlin, Heidelberg: Springer-Verlag; 2007.
[12] Budd ME, Evans GRD. Postoperative care. In: Wei FC, Mardini S, editors. Flapsand reconstructive surgery. 1st ed., Elsevier; 2009. p. 137–43.
[13] Frykberg ER. Popliteal vascular injuries. Surgical Clinics of North America2002;82:67–89.
[14] Huynh TT, Pham M, Griffin LW, Villa MA, Przybyla JA, Torres RH, et al.Management of distal femoral and popliteal arterial injuries: an update.American Journal of Surgery 2006;192:773–8.
[15] Geraghty AJ, Welch K. Antithrombotic agents for preventing thrombosis afterinfrainguinal arterial bypass surgery. CDS Review 2011;6:CD000536. http://dx.doi.org/10.1002/14651858.CD000536.pub2.
[16] Harris LM, Hordines J. Major vascular injuries in the pediatric population.Annals of Vascular Surgery 2003;17:266–9.
[17] Malan E, Tattoni G. Physio- and anatomo-pathology of acute ischemia of theextremities. The Journal of Cardiovascular Surgery 1963;4:214–21.
[18] Hafez HM, Woolgar J, Robbs JV. Lower extremity arterial injury: results of 550cases and review of risk factors associated with limb loss. Journal of VascularSurgery 2001;33:1212–9.
[19] de Silva WDD, Ubayasiri RA, Weerasinghe CW, Wijeyaratne SM. Challenges inthe management of extremity vascular injuries: a wartime experience from atertiary centre in Sri Lanka. World Journal of Emergency Surgery 2011;6:24.http://dx.doi.org/10.1186/1749-7922-6-24.