Embed Size (px)
Citation preview
Paediatric fractures
Differences
And
Paediatric pitfalls
Common things are common
• Fractures in upper limb > lower limb
On desktops in ED, “Paediatric fracture package” explaining fracture management and paediatric fracture quiz.
• Kids need generous analgesia– Physical – sling, POP– Medication – oral, IN, conscious sedation, GA
Fractures – kids differ
• Kids do daft things– Boys are more likely to sustain fractures
• “Plastic” skeleton– Greenstick, torus, bowing patterns– NB associated soft tissue injury
• 15% of # involve growth plates as point of weakness
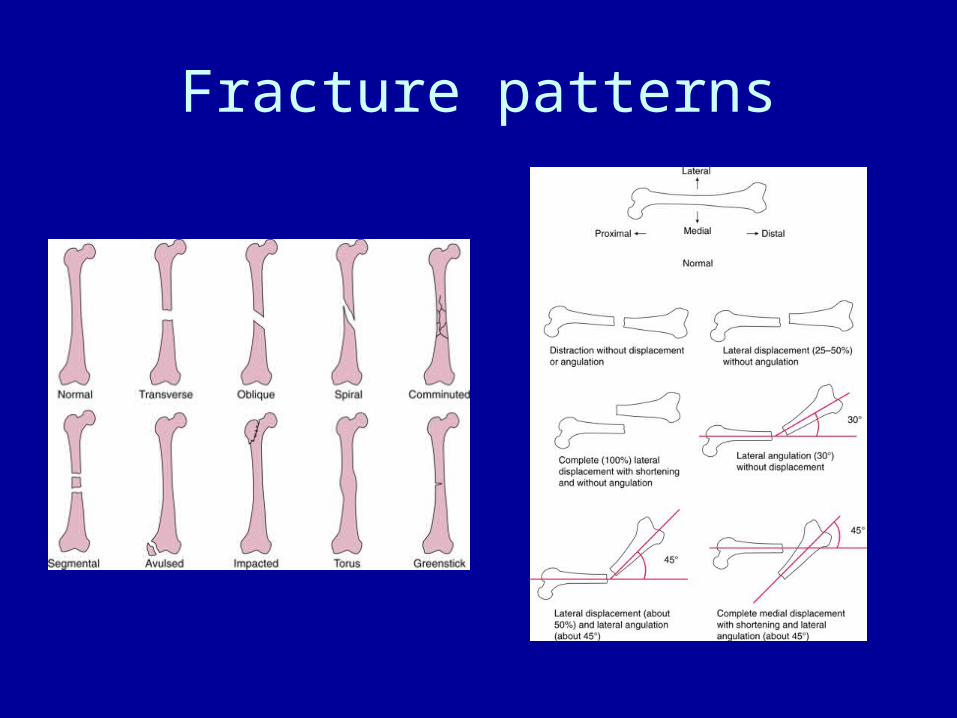
Fracture patterns
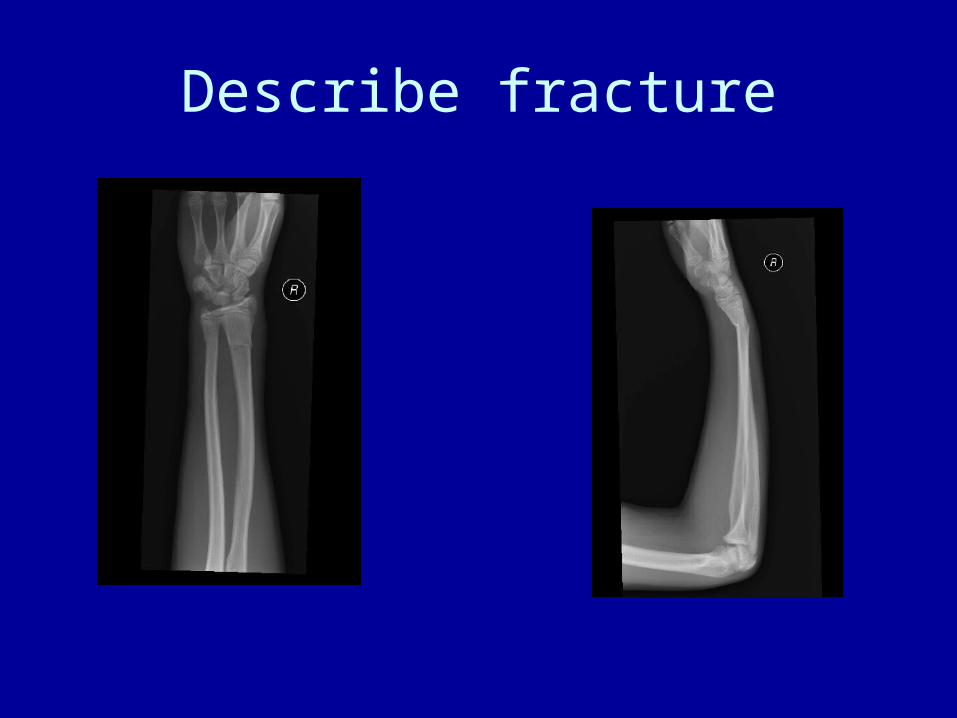
Describe fracture

4 year old falls off flying fox. Deformity and pain in left mid-forearm
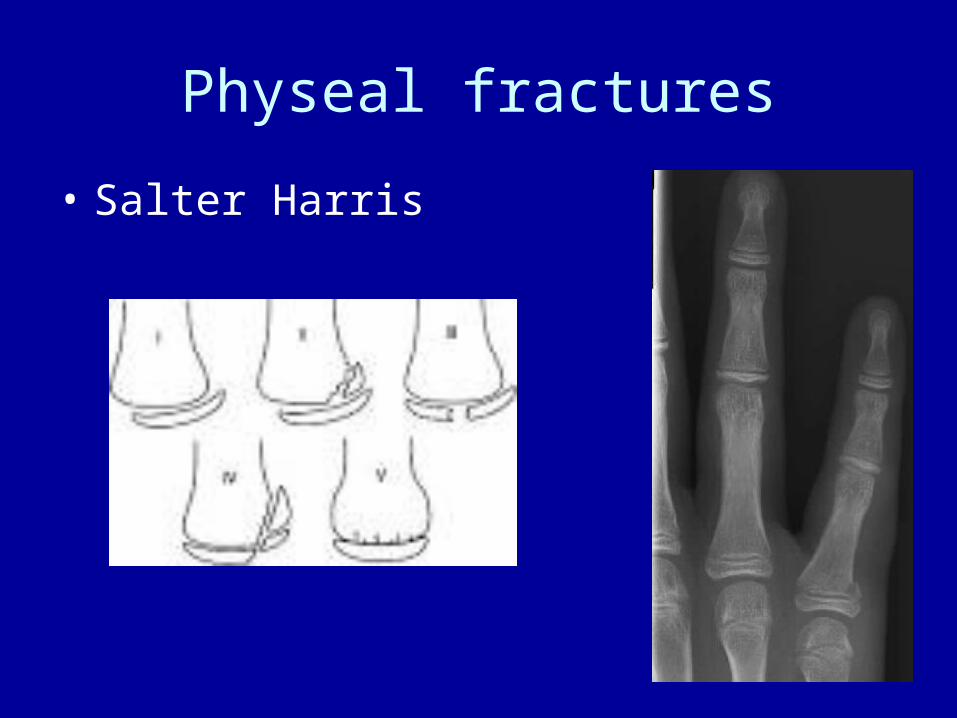
Physeal fractures
• Salter Harris
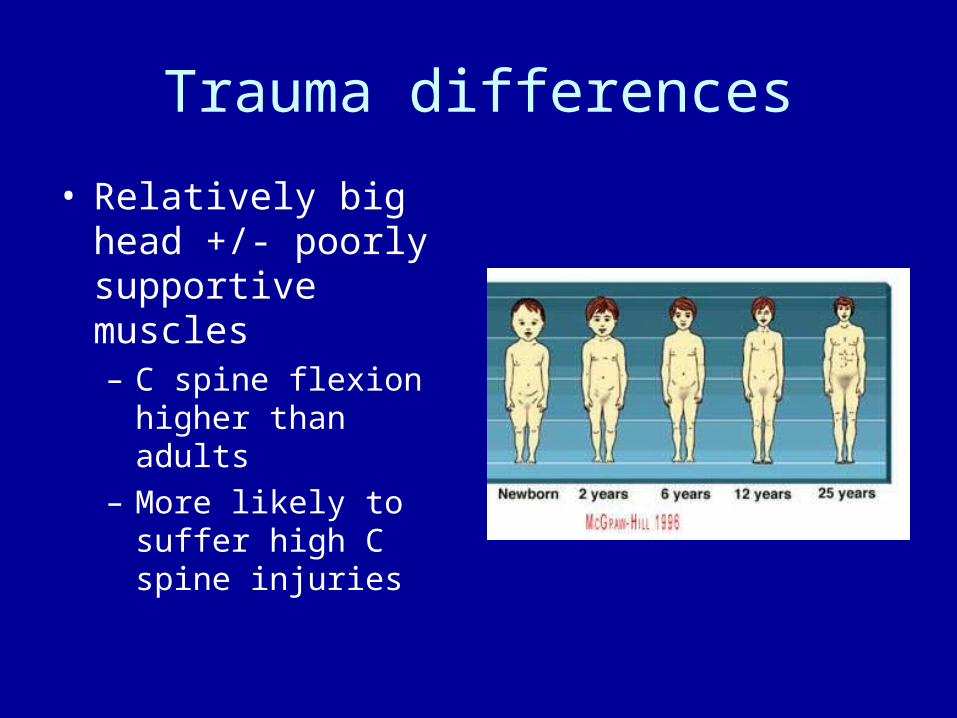
Trauma differences
• Relatively big head +/- poorly supportive muscles– C spine flexion higher
than adults– More likely to suffer
high C spine injuries
Trauma - differences
C spine
• Fracture
• Sublux/dislocate without fracture
• SCIWORA
• NB if there is a major distracting injury, children will not identify neck pain and the neck cannot be “cleared” clinically

12 yo female involved in high speed MVA

7 yo male involved in high speed MVA
Paediatric pitfalls of Musculoskeletal pain
• History / examination– Compliance decreases with pain
• Xrays – NB joint specific views– Backs– Joints
• Inflicted injuries
Assessment
History
• Mechanism of injury– Eg. Hurt ankle – exclude tibial fracture– Eversion – medial #: inversion – lateral #
• Referred pain– Xray - joint above and joint below
• Any fevers, rashes, medications?
Joint Examination• Look / Feel / MoveLook• Compare with normal side• Look for deformity / bruising• Can they weight bear? If so, assess gait.Feel• Point tenderness; joint line tenderness• Pulses + neurovascularMove• Active then passive ie/ watch what the kid does, then attempt to
move• Flexion/extension/abduction/adduction• Internal and external rotation
Neurovascular of handAny distracting injury limits compliance - Give analgesia!Movement• Stop – radial• Make an “L” – median• Make an “O” – ulnar• Make a fist (median), open it “make a star” (ulnar)
• Or hold piece of paper between fingers and do tug-of-war (ulnar)
Sensation• Thumb web space (radial)• Index finger (median)• Little finger (ulnar)
Limp
Acute v chronic• If pain present:
– Constant v intermittent– In same location– Worse at certain times of day
Examination• Abdomen• Spine• Lower limb• Feet
Back pain
Musculoskeletal causes commonest in adolescents.
Alarm bells for:• Child < 5 years• Night pain• Development of kyphosis or scoliosis• Altered gait eg limp• Early morning stiffness• Altered sensation +/- continence
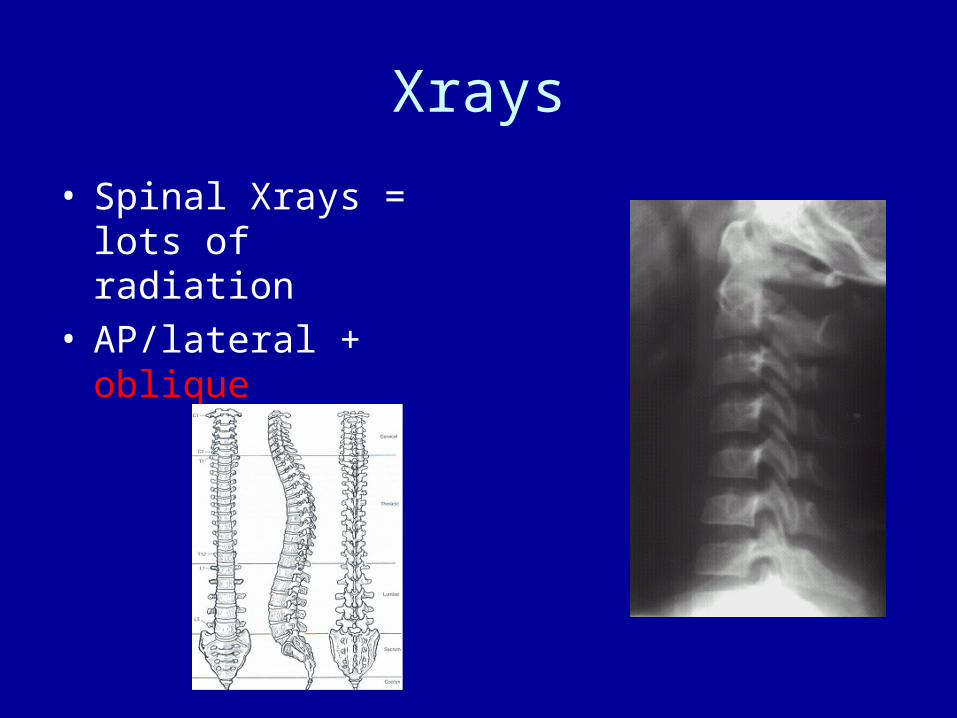
Xrays
• Spinal Xrays = lots of radiation
• AP/lateral + oblique

Spondylo-whatsit
SpondylolisthesisSpondylolysis
Hip pain
• Groin pain– Is it referred?
• Recent fevers?– Septic arthritis, osteomyelitis, transient synovitis
• Any trauma?– Avulsion of iliac crest
• Congenital defect?– Delayed presentation of hip dysplasia
• Rheumatological– Any meds?
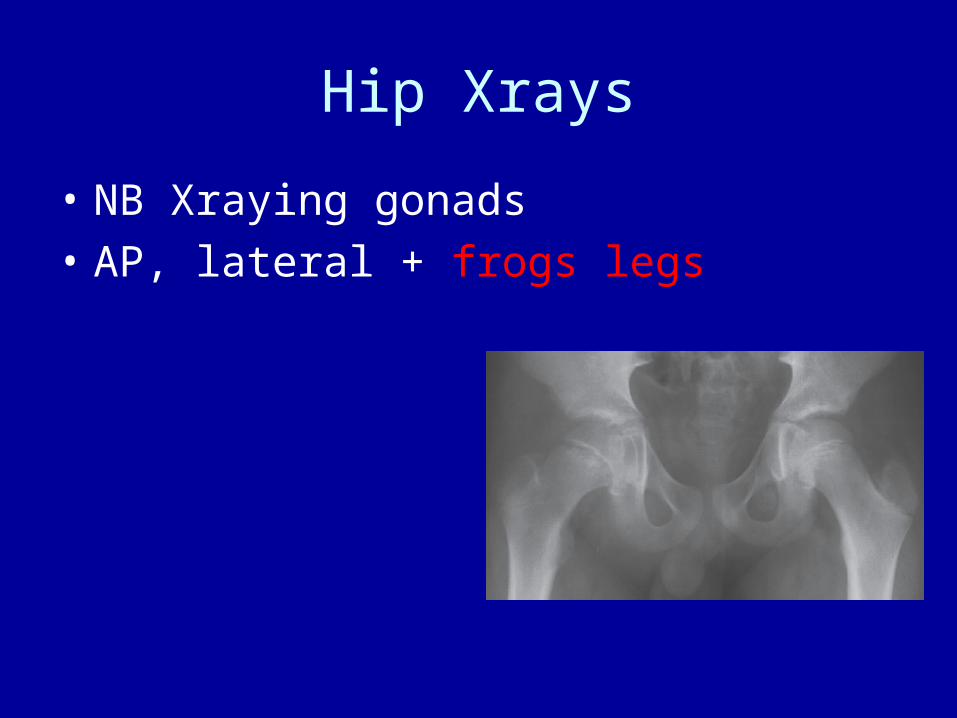
Hip Xrays
• NB Xraying gonads
• AP, lateral + frogs legs
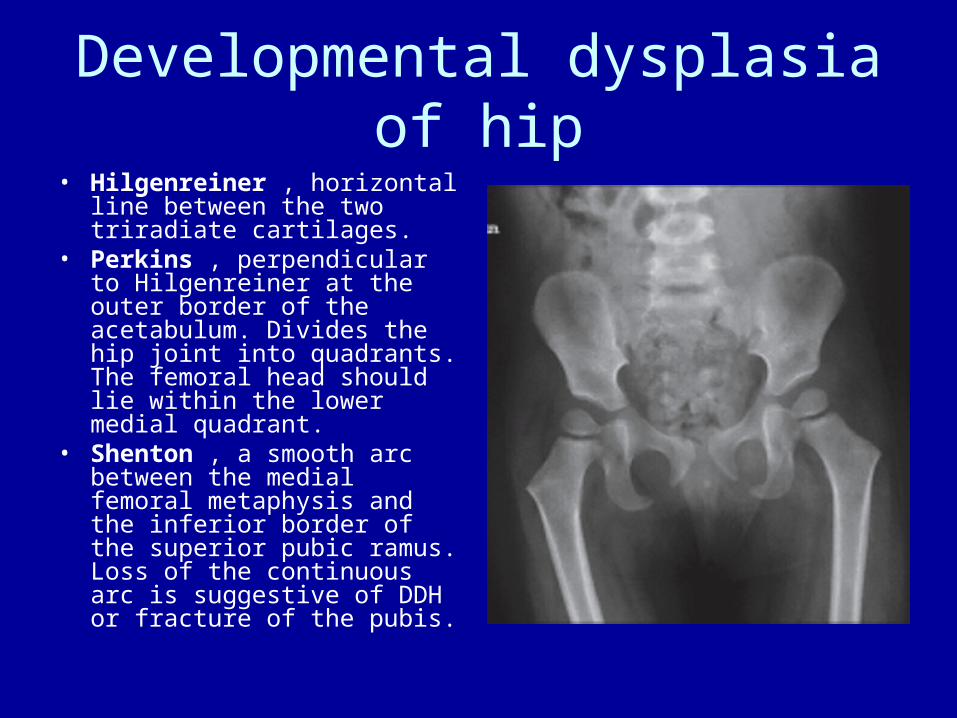
Developmental dysplasia of hip• Hilgenreiner , horizontal line
between the two triradiate cartilages.
• Perkins , perpendicular to Hilgenreiner at the outer border of the acetabulum. Divides the hip joint into quadrants. The femoral head should lie within the lower medial quadrant.
• Shenton , a smooth arc between the medial femoral metaphysis and the inferior border of the superior pubic ramus. Loss of the continuous arc is suggestive of DDH or fracture of the pubis.
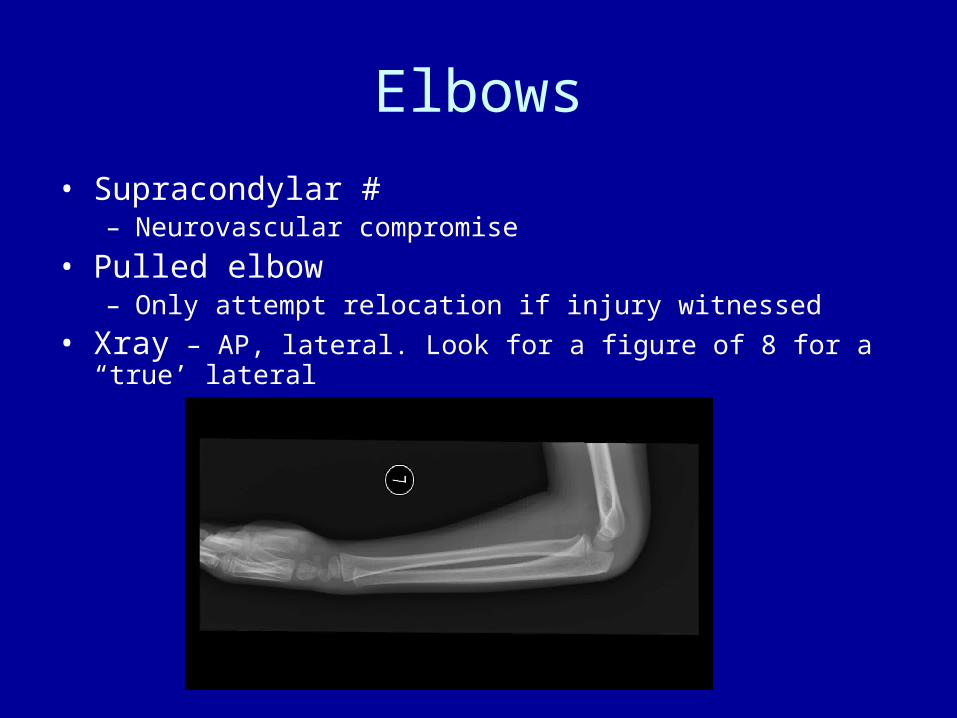
Elbows
• Supracondylar #– Neurovascular compromise
• Pulled elbow– Only attempt relocation if injury witnessed
• Xray – AP, lateral. Look for a figure of 8 for a “true’ lateral
Injuries – inflicted?
• 1-10% of ED presentations
Risk factors
• Kids under 18 months of age
• Socio-economic– poor, recent migrants, recently adopted from
other countries
• Developmentally delayed
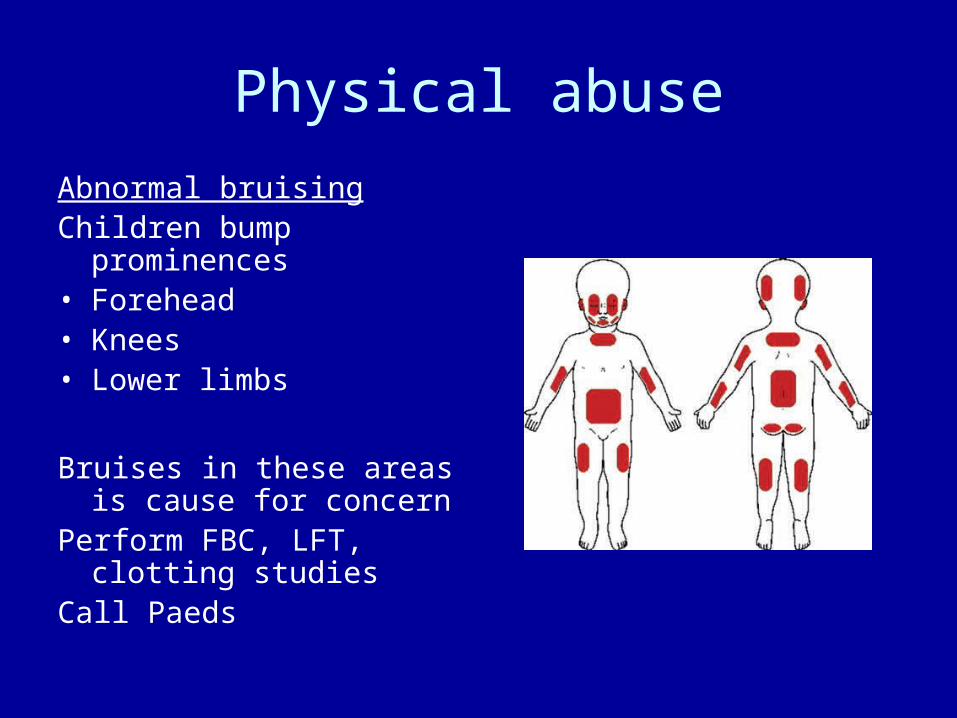
Physical abuse
Abnormal bruisingChildren bump prominences• Forehead• Knees• Lower limbs
Bruises in these areas is cause for concern
Perform FBC, LFT, clotting studies
Call Paeds
Other signs
Inflicted burns
• Scalds when toilet training
• Glove and stocking after immersion
Bites
• Intercanine distance >3cm
Bones
• Alarming fractures– Any fracture in child < 1 year– Spiral fracture– “Chip” fractures of radius and ulna– Transverse fractures of midshaft radius, ulna,
femur– Skull fracture associated with apnoea
Summary of Paediatric Fractures
• Is the story consistent with injury?
• Force dissipation– Growth plates– Soft tissue
• Good analgesia– Physical – sling, POP– Medication – oral, IN, conscious sedation, GA