Embed Size (px)
Citation preview

Pain Assessment ผู้��ช่�วยศาสตราจารย�แพทย�หญิ�งลั�กษมี� ช่าญิเวช่ช่�โรงพยาบาลัว�ฒโนสถ ศ�นย�การแพทย�โรงพยาบาลั
กร#งเทพ
งานประช่#มีโรงพยาบาลัพระจอมีเกลั�าฯ เพช่รบ#ร�
10 มี�นาคมี 2551

Objective
• Important of pain assessment
• Barriers in pain assessment• Standards of pain
management• Tools for pain
measurement

How is the assessment of pain
important?
• “… whatever the experiencing person says it is, existing whenever s/he says i
t does”• A subjective experience so we should
have self reporting as a reliable indicator
• McCaffery M. 1968
Pain

Pain
• An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage
• Pain is a complex experience that includes multiple dimensions (sensory, affective, cognitive)
International association for the study of pain® 1979
Pain Assessment: Goals
• Characterize the pain• Identify pain syndrome • Infer pathophysiology• Evaluate physical and
psychosocial comorbidities• Assess degree and nature of disability• Develop a therapeutic strategy

Characteristics of Nociceptive Pain

Characteristics of Neuropathic Pain
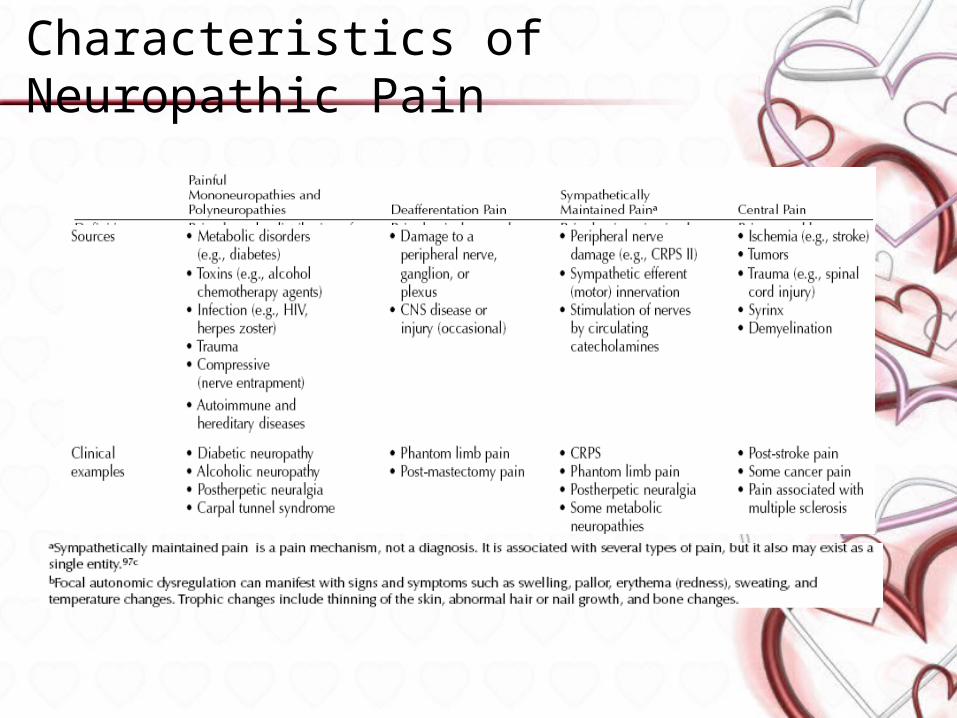
Characteristics of Neuropathic Pain

Pain Syndromes
• Acute pain
• Chronic pain
• Breakthrough pain
• Recent onset, transient, identifiable cause
• Persistent or recurrent pain, beyond usual course of acute illness or injury
• Transient pain, severe or excruciating, over baseline of moderate pain

Identify Pain Syndromes
• Syndrome identification can direct assessment and predict treatment efficacy
• Cancer pain syndromes• Bone pain• Pathologic fracture• Cord compression• Bowel obstruction
• Noncancer-related pain syndromes • Atypical facial pain• Failed low-back syndrome• Chronic tension headache• Chronic pelvic pain of unknown etiology

Barriers to appropriate of pain assessment
• Clinician• Patient• System

Clinician-Related Barriers to Pain Assessment
• Lack of pain training in medical school
• Insufficient knowledge • Lack of pain-assessment skills• Rigidity or timidity in
prescribing practices• Fear of regulatory oversight

Patient-Related Barriers to Pain Assessment
• Reluctance to report pain• Reluctance to take opioid
drugs• Poor adherence

System-Related Barriers to Pain Assessment
• Low priority given to symptom control
• Unavailability of opioid analgesics
• Inaccessibility of specialized care
• Lack of insurance coverage for outpatient pain medication

• Pain as the fifth vital sign• Joint Commission on
Accreditation of Healthcare Organizations (JCAHO)
• Should be documented: flow sheet
Pain Assessment Standard

• 1996In , the American Pain iiiiiiiiii iii iiiiii ( ) iiiii iiiiii“ 5 . ”
• i ai n assessment i s as i mpor t ant as assessment of the standard four
vi t al si gns and t hat cl i ni ci ans need t o t ake act i on when pat i ent
s r epor t pai n• A concept for pain assessment• More or less frequent assessment may
be appropriate
The Pain as the 5th Vital Sign

Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
• 6 standards for pain management
• Apply to all patients in healthcare facilities
• Implementation of strategies required in 2001 to continue accreditation
– Comprehensive Accreditation Manual for Hospitals 1999: www.jcaho.org

• Recognition of the right of the individual to appropriate assessment and management of pain
• Assessment of pain, and also the nature and intensity of pain, in all patients
• Establishment of policies and procedures that support the appropriate prescribing of effective pain medications
JCAHO Standards… cont

JCAHO Standards… cont
• Education of patients and their families about effective pain management
• Addressing of the needs of the individual for symptom management in the discharge planning process
• Integration of pain management into the organization’s performance measurement and improvement program

As a patient in this hospital, you can expect:
• To receive information about pain and pain relief measures
• Treatment by concerned staff committed to pain prevention and management
• A quick response to your reports of pain• Your reports of pain will be believed• State-of-the-art pain management• Dedicated pain relief specialists
Patients Rights

As a patient in this hospital, you are expected to:
• Ask you health care providers what to expect regarding pain and its management
• Discuss pain relief option with doctors and nurses
• Work with healthcare providers to develop pain management plans
• Report pain when it first begins• Help healthcare providers measure
pain at all stages of your care• Tell healthcare providers if pain is
not relieved
Patient Responsibilities

Initial Assessment of Pain• Standard pain intensity tool
throughout the hospital (> 1 if pediatric and adult populations: Wong-Baker smile/frown, visual analogue, 1-10 scale)
• Displayed at bedside• Regular charting of pain as the 5th
vital sign• Standardized assessment sheets to
document effects and treatment of complications
• Develop trigger for review of pain management plan (e.g >4 pain or side effect such as respiratory depression)

Comprehensive Pain Assessment
• History
• Physical examination
• Appropriate laboratory and radiologic tests

Pain History
• Temporal features—onset, duration, course, pattern
• Intensity—average, least, worst, and current pain
• Location—focal, multifocal, generalized, referred, superficial, deep
• Quality—aching, throbbing, stabbing, burning• Exacerbating/alleviating factors—position,
activity, weight bearing, cutaneous stimulation

Characteristics for the Pain Type
Location and distribution• Localized pain:
– pain confined to site of distribution origin (e.g., cut aneous pain, some visceral pain, arthritis)
• Referred pain:– pain that is referred to a distant structure (e.g., vis
ceral pain such as angina, appendicitis)• Projected (transmitted) pain:
– pain transferred along the course of a nerve with a segmental distribution (e.g., herpes zoster) or a pe
ripheral (e.g., trigeminal neuralgia)• Dermatomal patterns:
– peripheral neuropathic pain• Nondermatomal:
– central neuropathic pain, fibromyalgia• No recognizable pattern: CRPS
Characteristics for the Pain Type (cont.)
Duration and periodicity• Brief flash:
– quick pain such as a needle stick• Rhythmic pulses:
– pulsating pain such as a migraine or toothache• - Longer duration rhythmic phase:
– intestinal colic• Plateau pain:
– pain that rises gradually or suddenly to a plateau w here it remains for a prolonged period until resoluti
on (e.g., angina)• Paroxysmal:
– neuropathic pain• Continuously fluctuating pain:
– musculoskeletal pain

Characteristics for the Pain Type (cont.)
Quality• Superficial somatic (cutaneous) pain:
– sharp pricking or burning
• Deep somatic pain:– dull or aching
• Visceral pain:– dull aching or cramping
• Neuropathic pain:– - burning, shock like, lancinating, jabbing,
squeezing, aching

Characteristics for the Pain Type
Associated signs and symptoms• Visceral pain:
– “ sickening feeling,”nausea, vomiting, autonomic symptoms
• Neuropathic pain:– hyperalgesia, al l odyni a
• Complex regional pain syndrome:– hyperalgesia, hyperesthesia, allodynia, autonomicchanges, and t r ophi c

Physical Examination of a Patient With Pain

Physical Examination of a Patient With Pain

Physical Examination of a Patient With Pain

Diagnostic studies

Tools for pain measurement

•Unidimensional

Pain Intensity Rating

- 6From Wong DL, Hockenberry Eaton M, Wilson D, Winkelstein ML, Schwartz P: Wong’s Essentials of Pediatric Nursing, /e, St. Lou
, 2 0 0 1 , . 1 3 0 1 . , .is P Copyrighted by Mosby Inc
Pain Intensity Rating

Sample of Child’s FACES Pain Rating Scale
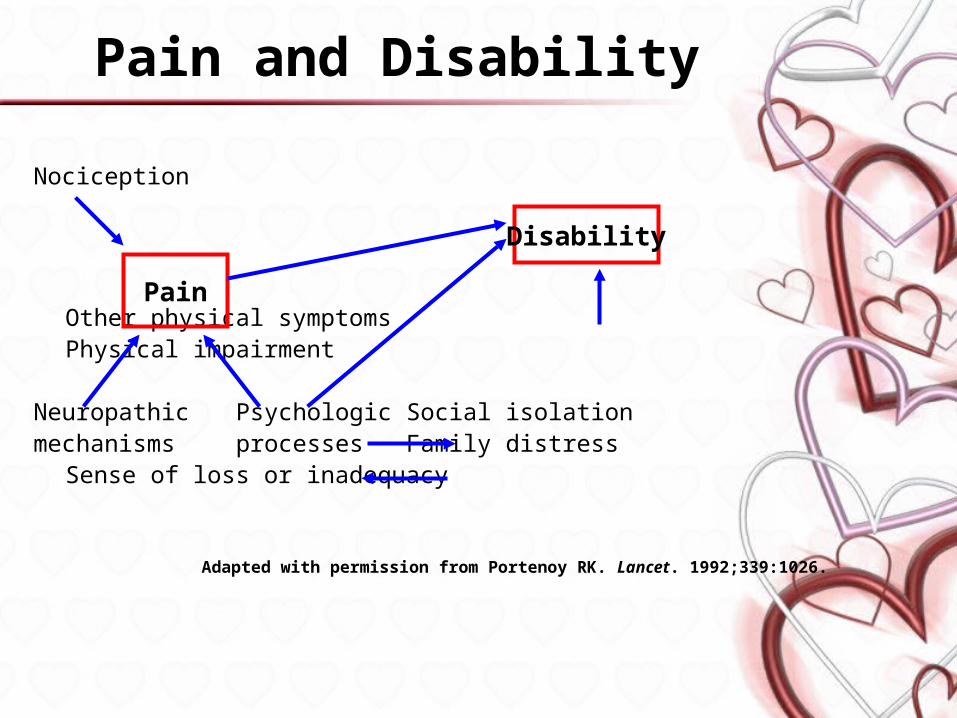
Pain and Disability
Nociception
Other physical symptomsPhysical impairment
Neuropathic Psychologic Social isolationmechanisms processes Family distress
Sense of loss or inadequacy
Adapted with permission from Portenoy RK. Lancet. 1992;339:1026.
Pain
Disability

•Multidimensional

BPI




Neuropathic Pain Scales

Neuropathic Pain Scales (cont.)
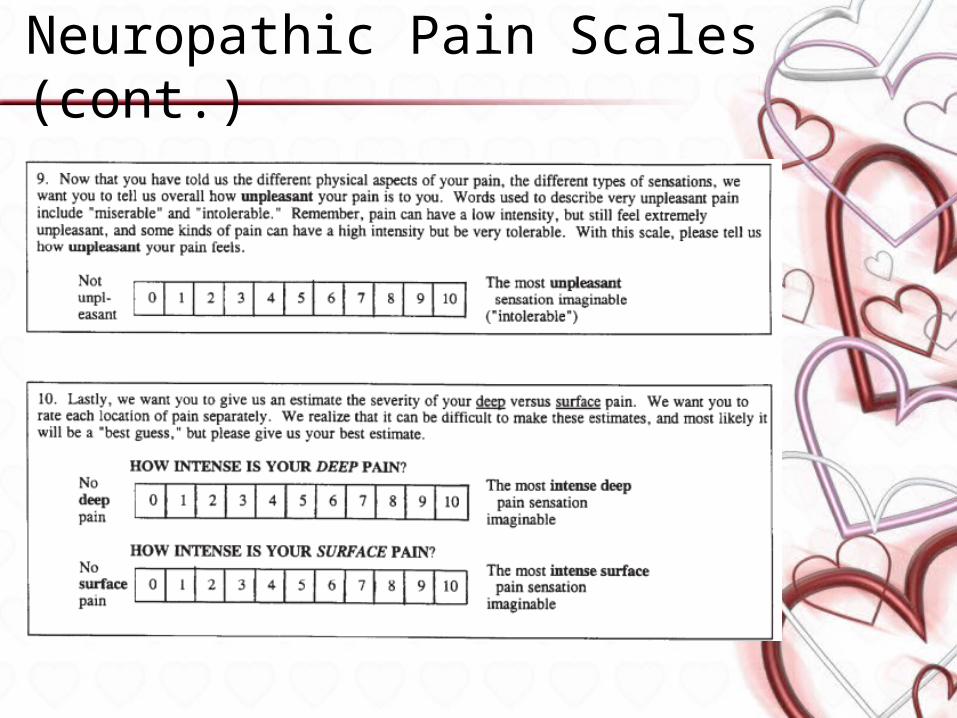
Neuropathic Pain Scales (cont.)

Cries score



Pain Assessment Techniques• In infants, behavior must be
interpreted by using physiological and behavioral measures
• CRIES is useful for neonates from 32 weeks to infants of up to 1 year
• FLACC (full term neonate – 7 years)
• Preschool children (ages 3 to 7) are in a transition group in which v
erbal abilities are developing.

Frequency of re-assessmentAcute setting of pain
1 30) within minutes of parenteral iii iiiiiiiiiiii, 2 ) within one hour of oral drug
administration, 3) with each report of new or
changed pain

Conclusions• Important of pain assessment
– Effective pain management
• Standards of pain management– Patient rights– Hospital accreditaion
• Tools for pain measurement– Simple and appropriate– Documentation
Thank you