Embed Size (px)
Citation preview

3/28/2016
1
PAIN MANAGEMENTKevin E Vorenkamp, MD
Director, Pain Medicine Fellowship
Virginia Mason Medical Center
Seattle, WAHEALTHCON 2016
April 13, 2016
11:15-12:30
ORLANDO, FL
OBJECTIVES
■ UNDERSTAND 2016 CPT CHANGES AND ADDITIONS FOR PAIN
MANAGEMENT
■ REVIEW PROPER CODING FOR PARAVERTEBRAL (FACET) JOINT BLOCKS
AND NEUROLYSIS PROCEDURES
■ IDENTIFY THE PAIN MANAGEMENT PROCEDURES WHICH ALREADY
HAVE IMAGING BUNDLED INTO THEM (AND WHICH DO NOT)
■ REVIEW THE MOST COMMONLY BILLED PAIN PROCEDURES AND HOW
TO ASSURE YOU ARE CODING ACCURATELY

3/28/2016
2
CPT Coding changes for 2016
CPT
Disclosure: Dr. Vorenkamp is a current member of the CPT
editorial panel and prior ASA advisor to CPT

3/28/2016
3
2015 Changes
NOTE that these codes (and following paravertebral codes) both include imaging guidance

3/28/2016
4
NOTE: These new codes 64461-64463 refer to the paravertebral space and NOT the paravertebral facet joint described in codes 64490-64495, 64633-64636, 0213T-0218T

3/28/2016
5
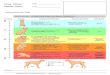
Paravertebral space ≠ paravertebral (facet) joint
Thoracic Paravertebral Space Lumbar Facet Joint
1 code deletion
■64412 Injection, spinal accessory
nerve

3/28/2016
6
Changes to spinal cord and peripheral nerve stimulator programming

3/28/2016
7
Case 1: A 54 year old man with neck pain undergoes bilateral cervical medial branch blocks at C4 and C5. How should these be coded?
■ Number of levels?
■ Additional fluoroscopy charge?
■ Modifiers?

3/28/2016
8
Case 1: A 54 year old man with neck pain undergoes bilateral cervical medial branch blocks at C4 and C5, with fluoroscopy. How should this procedure be coded?
A. 64490
B. 64490, mod 50
C. 64490 x 2
D. 64490, mod 50 and 64491, mod 50

3/28/2016
9
Case 1: A 54 year old man with neck pain undergoes bilateral cervical medial branch blocks at C4 and C5, with fluoroscopy. How should this procedure be coded?
A. 64490 (if 1 joint, unilateral)
B. 64490, mod 50 (YES! 2 nerves=1 joint, use bilateral
modifier)
C. 64490 x 2 (No, this is not a possible coding solution.
Should use either bilateral modifier or 64490 +64491)
D. 64490, mod 50 and 64491, mod 50 (No. This would be if
same bilateral procedure were performed at 3 levels [2
joints])
Codes pertaining to the cervical paravertebral (facet) joint

3/28/2016
10
What if the same procedure was performed with ultrasound rather than fluoroscopic (or CT) guidance?
A 54 year old man with neck pain undergoes
bilateral cervical medial branch blocks at C4
and C5, with ultrasound guidance. How should
this procedure be coded?
Imaging
guidance

3/28/2016
11
Other Narrative Changes to CPT 2016
A. 64633 x 2
B. 64633 + 64634
C. 64633 + 64634 x 2
D. 64633 + 64634 + 77003
Case 2: A 65-year-old woman with low back pain is scheduled for radiofrequency ablation of the medical branch nerves at L3, L4
and L5 with fluoroscopic guidance.
How would you code for this procedure?

3/28/2016
12
A. 64633 x 2
B. 64633 + 64634
C. 64633 + 64634 x 2
D. 64633 + 64634 + 77003
Case 2: A 65-year-old woman with low back pain is scheduled for radiofrequency ablation of the medical branch nerves at L3, L4
and L5 with fluoroscopic guidance.
How would you code for this procedure?
Does it matter if the ablation is performed at
60oC or 80oC?

3/28/2016
13
A. 64635
B. 64635 + 64999
C. 64640
D. 64635 + 64640
E. 64635 + 64640 x 2
F. 64999
A 44-year-old woman is scheduled for radiofrequency ablation of the left sacroiliac joint. How should this procedure be coded?
Does the
procedural
technique matter?
A. 64635
B. 64635 + 64999
C. 64640
D. 64635 + 64640
E. 64635 + 64640 x 2
F. 64999
A 44-year-old woman is scheduled for radiofrequency ablation of the left sacroiliac joint. How should this procedure be coded?
Does the
procedural
technique matter?
YES

3/28/2016
14
Bonus Feature: Surgery: Nervous System. Question: Should code 64640 x 4 be reported per lesion because it is a single percutaneous entry point or should the unlisted code 64999 be reported? What is the appropriate code to use for radiofrequency (eg, Simplicity IIIâ„¢ Radiofrequency Probe) for sacroiliac (SI) joint nerve destruction from a single percutaneous entry site in the following procedure?
-Answer: Since the documentation indicates insertion of a single electrode (having three contacts) at the sacroiliac (SI) joint "to lesion the lateral branches of S1, S2, S3, and S4," code 64999, Unlisted procedure, nervous system, is reported once. This "SI joint rhizotomy" would be reported once using the unlisted nervous system code 64999. The sacroiliac (SI) joint and sacral anatomy differs in that it is comprised of spine bone and pelvic bone wherein the exact innervation of the SI joint occurring more from contributing branches at adjoining nerve levels. Procedurally, the work of the described SI joint destruction differs from that described by code 64622*, Destruction by neurolytic agent, paravertebral facet joint nerve; lumbar or sacral, single level. Code 64622* may be reported for L5-S1 rhizotomy(nerve destruction since this joint lies between two spinal segments for which the anatomy and procedural work at L5-S1 is similar to that at other spinal segments (eg, L4-5). Therefore, the unlisted nervous system code 64999 would be reported once for SI joint or sacral rhizotomy (nerve destruction).
-To differentiate between the work when performing sacral nerve destruction of S1, S2, S3, and S4, each individually separate peripheral nerve root neurolytic block is reported as destruction of a peripheral nerve, using code 64640, Destruction by by neurolytic agent; other peripheral nerve or branch. In this instance, code 64640 is reported four times. It is suggested that Modifier 59, Distinct Procedural Service, be appended as well.
AMA CPT Assistant December 2009 page 11

3/28/2016
15
AMA CPT Assistant December 2009 page 11Bonus Feature:Surgery: Nervous System. Question: Should code 64640 x 4 be reported per lesion because it is a single percutaneous entry
point or should the unlisted code 64999 be reported? What is the appropriate code to use for radiofrequency (eg, Simplicity IIIâ„¢
Radiofrequency Probe) for sacroiliac (SI) joint nerve destruction from a single percutaneous entry site in the following procedure?
-The Simplicity III electrode was then advanced, maintaining continuous contact with the sacrum, on a cephalad and slightly lateral line,
staying lateral to the sacral foramen, medial to the sacroiliac joint, and ventral to the ilium, until contact with the sacral ala prevented further
advancement. Appropriate positioning was confirmed by changing the caudal/cephalad tilt of the C-arm to parallel the superior endplate of
S1; and verifying once again that the entire length of the Simplicity III electrode was advanced to the ipsilateral sacral ala and the three
independent, active contacts were positioned adjacent to the S1, S2, S3, and S4 lateral branch innervation pathways.... "Lesioning" was
then carried out using the Simplicity III preprogrammed protocol at 85 degrees centigrade for five minutes. Karen Glancy, CCS-P
-Answer: Since the documentation indicates insertion of a single electrode (having three contacts) at the sacroiliac (SI) joint "to lesion the
lateral branches of S1, S2, S3, and S4," code 64999, Unlisted procedure, nervous system, is reported once. This "SI joint rhizotomy" would
be reported once using the unlisted nervous system code 64999. The sacroiliac (SI) joint and sacral anatomy differs in that it is comprised
of spine bone and pelvic bone wherein the exact innervation of the SI joint occurring more from contributing branches at adjoining nerve
levels. Procedurally, the work of the described SI joint destruction differs from that described by code 64622, Destruction by neurolytic
agent, paravertebral facet joint nerve; lumbar or sacral, single level. Code 64622 may be reported for L5-S1 rhizotomy (nerve destruction
since this joint lies between two spinal segments for which the anatomy and procedural work at L5-S1 is similar to that at other spinal
segments (eg, L4-5). Therefore, the unlisted nervous system code 64999 would be reported once for SI joint or sacral rhizotomy (nerve
destruction).

3/28/2016
16
AMA CPT Assistant December 2009 page 11 (continued)
-To differentiate between the work when performing sacral nerve destruction of S1,
S2, S3, and S4, each individually separate peripheral nerve root neurolytic block is
reported as destruction of a peripheral nerve, using code 64640, Destruction by by
neurolytic agent; other peripheral nerve or branch. In this instance, code 64640 is
reported four times. It is suggested that Modifier 59, Distinct Procedural Service, be
appended as well.
-It is very important that the service performed matches accurately with the descripton
in the CPT code. Therefore, for this very reason, it is important to remember that a
code that is "close" to the procedure performed is not selected in lieu of an unlisted
code. There are some who maintain that they are not allowed to use unlisted codes or
that the use of the unlisted codes is undesirable. While the use of an unlisted
procedure code does require a special report or documentation to describe the
service, correct coding demands that you use a code that is appropriate for the
service being provided (ie, a code that most accurately represents the services
rendered and performed).
Protect yourself

3/28/2016
17
Which spinal procedures DO have included imaging guidance?
■ Transforaminal epidural steroid injections/selective nerve root blocks (64479,
64480, 64483, 64484)
■ Paravertebral (facet) joint injections (64490-64495) and destructive procedures
(64633-64636)
■ Sacroiliac joint injection (27096)
■ Percutaneous lysis of adhesions (62263)
■ Celiac plexus block/neurolysis
A 65 year old man with pancreatic cancer and intractable abdominal pain undergoes injection of phenol around the area of the splanchnic nerves bilaterally.
How do you code for this?

3/28/2016
18
A 65 year old man with pancreatic cancer and intractable abdominal pain undergoes injection of phenol around the area of the
splanchnic nerves bilaterally.
How do you code for this?
[A splanchnic nerve block is also termed a retrocrural celiac plexus block]
CPT assistant (February 1999 page 10)
■ Coding Consultation
■ Surgery Nervous System, 64680 (Q&A)
■ Question: How do I report a procedure where the splanchnic nerve is
injected with phenol?
■ [A splanchnic nerve block is also termed a retrocrural celiac plexus
block]
■ AMA Comment:
– Since the splanchnic nerve is part of the celiac plexus, and
phenol is a neurolytic agent, you should report CPT code 64680,
Destruction by neurolytic agent, celiac plexus, with or without
radiologic monitoring.

3/28/2016
19
How do you interpret these? ■ Injection, celiac plexus (64530)
■ Destruction, celiac plexus (64680) and superior hypogastric plexus (64481)
If billing for fluoroscopy, which code to use?
*77003 should be used for spinal
sympathetic blocks

3/28/2016
20
The most commonly coded pain management procedures
Spine■ Epidural or subarachnoid injections
– Interlaminar (62310, 62311)
■ Continuous via indwelling catheter (62318, 62319)
– *Transforaminal (64479-80, 64483-4)
■ *Paravertebral (facet) joint injections
■ *Destruction, paravertebral (facet) joint
■ *Sacroiliac joint injection (27096)
■ Epidural blood patch (62273)
*Denotes procedes include imaging fuidance (fluoroscopy or CT)
The most commonly coded pain management procedures
Musculoskeletal■ 20552 Injection, single or multiple trigger point(s), 1 or 2 muscle(s)
– 20553 single or multiple trigger point(s), 3 or more muscles
■ Arthrocentesis, aspiration and/or injection
– Major joint/bursa (Shoulder, hip, knee, subacromial bursa)
■ With US (20611)
■ Without US (20610)
– Intermediate joint/bursa (TMJ, AC, wrist, elbow or ankle, olecranon)
■ With US (20606)
■ Without US (20605)
– Small joint or bursa (Fingers, toes)
■ With US (20604)
■ Without US (20600)

3/28/2016
21
The most commonly coded pain management procedures
The most commonly coded pain management proceduresNeuraxial Implants: SCS
For laminectomy (paddle) lead

3/28/2016
22

3/28/2016
23
The most commonly coded pain management proceduresPNS Implants
The most commonly coded pain management procedures
Neuraxial Implants: IDDS and tunneled catheters