Embed Size (px)
Citation preview
PAIN MANAGEMENT FUNDAMENTALS
Support for this program is provided by a
grant from the Reynolds Foundation
Learning Objectives
Systematically assess pain as a symptom
Select appropriate medication for individual patient
Describe the basic principles of opioid
pharmacotherapy
Perform simple opioid dose conversions
Recognize common opioid side effects
Pain in the elderly
Sources of pain in the elderly
• Degenerative joint disease
• Spinal stenosis
• Fractures
• Pressure ulcers
• Neuropathic pain
• Urinary retention
• Post-stroke syndrome
• Improper positioning
• Fibromyalgia
• Cancer pain
• Contractures
• Post herpetic neuralgia
• Oral/dental
• Constipation
3 TYPES OF PAIN SYNDROMES
• Nociceptive—pain due to activation of nociceptive
sensory receptors; often adequately treated with
common analgesics
Somatic—well localized in skin, soft tissue, bone
Visceral—due to cardiac, GI, or lung injury
• Neuropathic—from irritation of components of the CNS
or peripheral nervous system; may respond well to
nonopioid therapies; responds unpredictably to opioids
• Mixed or unspecified—has characteristics of both
nociceptive and neuropathic pain; common in older
adults
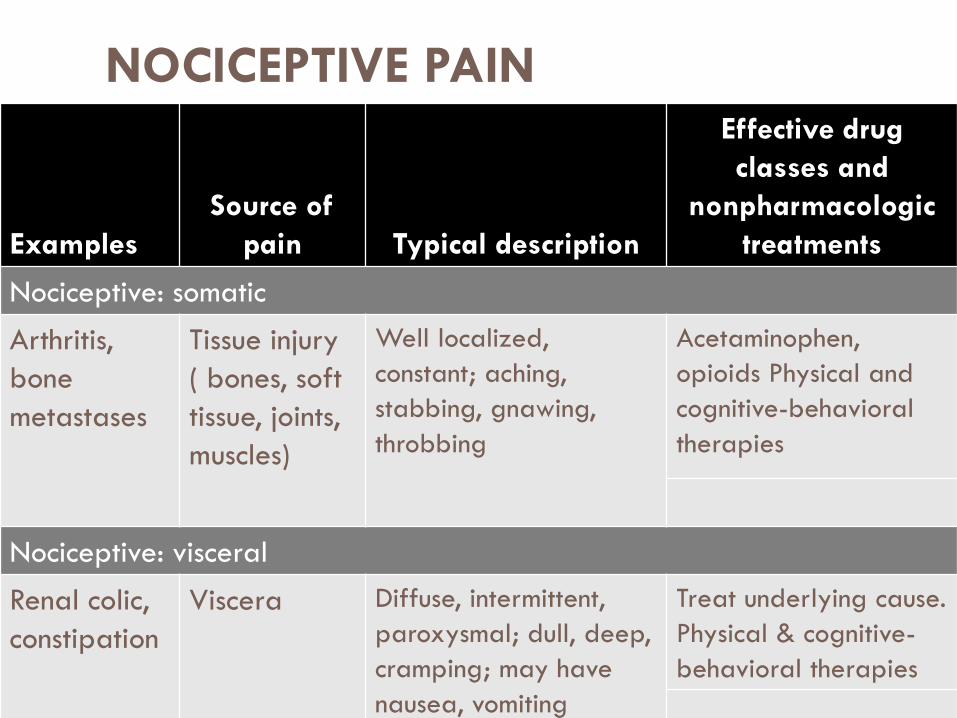
NOCICEPTIVE PAIN
Table 15.1 Examples
Source of
pain Typical description
Effective drug
classes and
nonpharmacologic
treatments
Nociceptive: somatic
Arthritis,
bone
metastases
Tissue injury
( bones, soft
tissue, joints,
muscles)
Well localized,
constant; aching,
stabbing, gnawing,
throbbing
Acetaminophen,
opioids Physical and
cognitive-behavioral
therapies
Nociceptive: visceral
Renal colic,
constipation
Viscera Diffuse, intermittent,
paroxysmal; dull, deep,
cramping; may have
nausea, vomiting
Treat underlying cause.
Physical & cognitive-
behavioral therapies
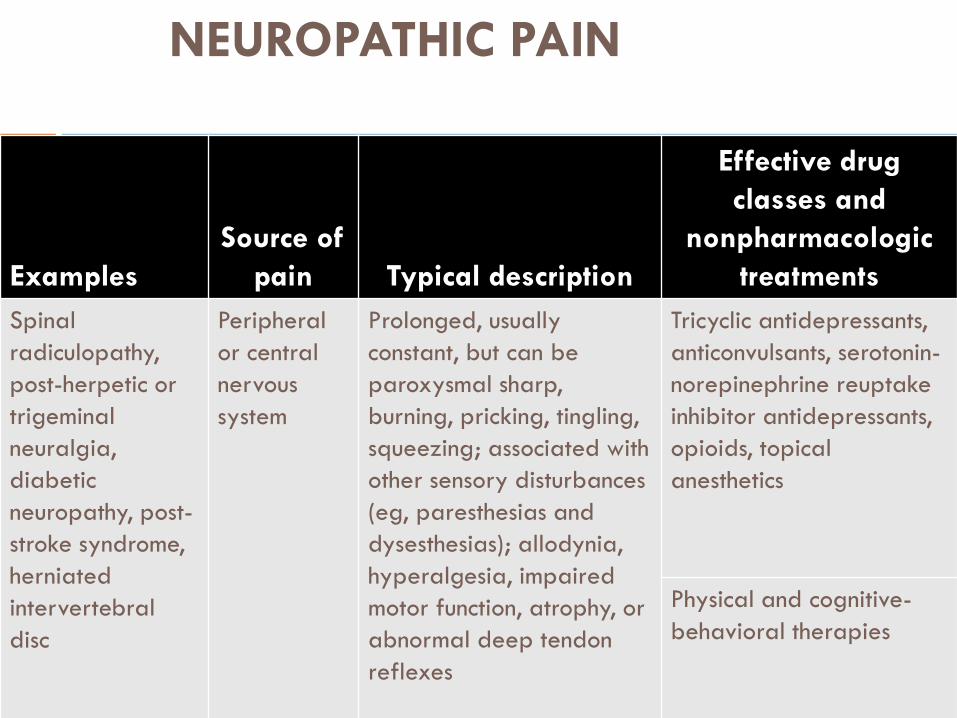
NEUROPATHIC PAIN
Table 15.1 Examples
Source of
pain Typical description
Effective drug
classes and
nonpharmacologic
treatments
Spinal
radiculopathy,
post-herpetic or
trigeminal
neuralgia,
diabetic
neuropathy, post-
stroke syndrome,
herniated
intervertebral
disc
Peripheral
or central
nervous
system
Prolonged, usually
constant, but can be
paroxysmal sharp,
burning, pricking, tingling,
squeezing; associated with
other sensory disturbances
(eg, paresthesias and
dysesthesias); allodynia,
hyperalgesia, impaired
motor function, atrophy, or
abnormal deep tendon
reflexes
Tricyclic antidepressants,
anticonvulsants, serotonin-
norepinephrine reuptake
inhibitor antidepressants,
opioids, topical
anesthetics
Physical and cognitive-
behavioral therapies
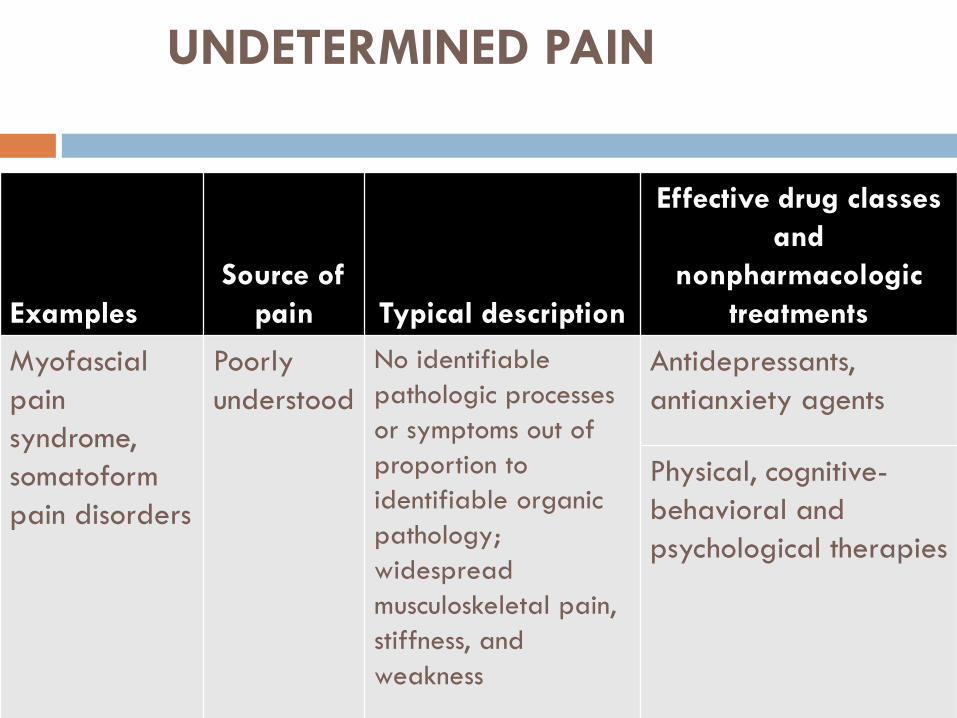
UNDETERMINED PAIN
Table 15.1
Examples
Source of
pain Typical description
Effective drug classes
and
nonpharmacologic
treatments
Myofascial
pain
syndrome,
somatoform
pain disorders
Poorly
understood
No identifiable
pathologic processes
or symptoms out of
proportion to
identifiable organic
pathology;
widespread
musculoskeletal pain,
stiffness, and
weakness
Antidepressants,
antianxiety agents
Physical, cognitive-
behavioral and
psychological therapies
Consequences of Untreated Pain
Acute pain:
increase metabolic rate and blood clotting,
impair immune function
induce negative emotions
Without intervention, pain receptors become
sensitive and may have long lasting changes in the
neurons
Consequences of Untreated Pain
Chronic pain may lead to:
fatigue,
anxiety,
depression,
confusion,
increased falls,
impaired sleep, and
decreased physical functioning/deconditioning
Why is pain control often not optimal?
• Clinician unfamiliarity with assessment and treatment
• Opiate misconceptions
• patients, families, and clinicians
• Fear of side effects
• Concern about addiction, regulatory reprimands, and
lawsuits
“I believe in traditional Western
medicine. Here, bite this bullet.”
Pain Management and the Law
Clinicians’ fear of regulatory scrutiny is a major
contributor to the problem of under treatment of pain.
An 85-year-old California man with metastatic lung
carcinoma spent the final week of his life in severe pain.
3 years later his children sued his doctor alleging that he
had failed to prescribe drugs powerful enough to relieve
their father's suffering.
This was one of the first U.S. cases in which a doctor has
gone on trial for allegedly under-treating a patient's
pain.
The Verdict
The plaintiffs’ lawyers convinced the jury that
under-treatment of pain was ‘reckless
negligence.’ By a 9 to 3 vote the jury decided
that the physician’s lack of attention to pain
constituted elder abuse, awarding the family
$1.5 million (the amount was reduced to
$250,000).
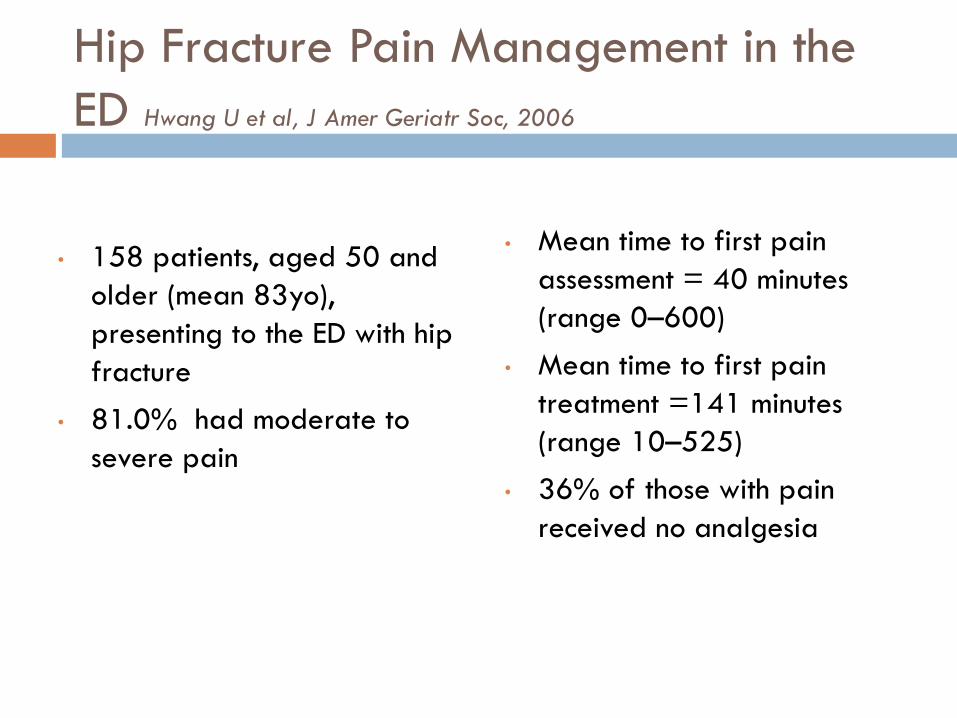
Hip Fracture Pain Management in the
ED Hwang U et al, J Amer Geriatr Soc, 2006
• 158 patients, aged 50 and
older (mean 83yo),
presenting to the ED with hip
fracture
• 81.0% had moderate to
severe pain
• Mean time to first pain
assessment = 40 minutes
(range 0–600)
• Mean time to first pain
treatment =141 minutes
(range 10–525)
• 36% of those with pain
received no analgesia
Case 1
You are rounding on an 83 y.o. NH patient admitted with pneumonia and a stage III sacral ulcer
She has advanced dementia, is bed- bound, and has limited verbalization
PMHx: DM, HTN,
Patient stopped eating and is combative with care
Bedside Assessment
ASK the patient about present pain
Identify preferred pain terminology
-hurting, aching, stabbing, discomfort, soreness
Use a pain scale that works for the individual
-Insure understanding of its use
-Modify sensory deficits
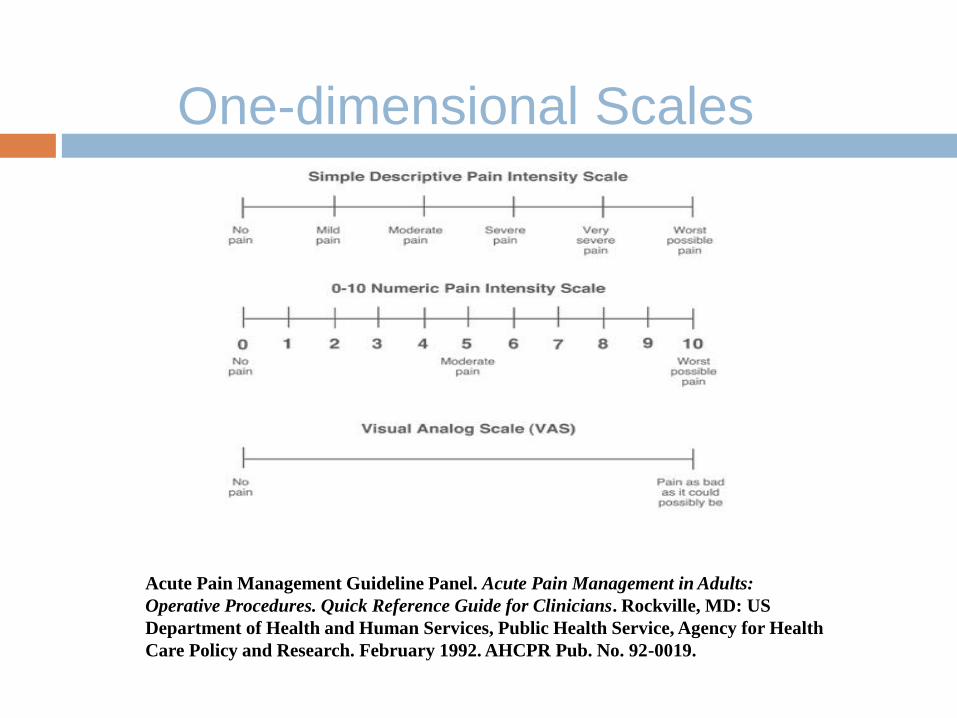
One-dimensional Scales
Acute Pain Management Guideline Panel. Acute Pain Management in Adults:
Operative Procedures. Quick Reference Guide for Clinicians. Rockville, MD: US
Department of Health and Human Services, Public Health Service, Agency for Health
Care Policy and Research. February 1992. AHCPR Pub. No. 92-0019.
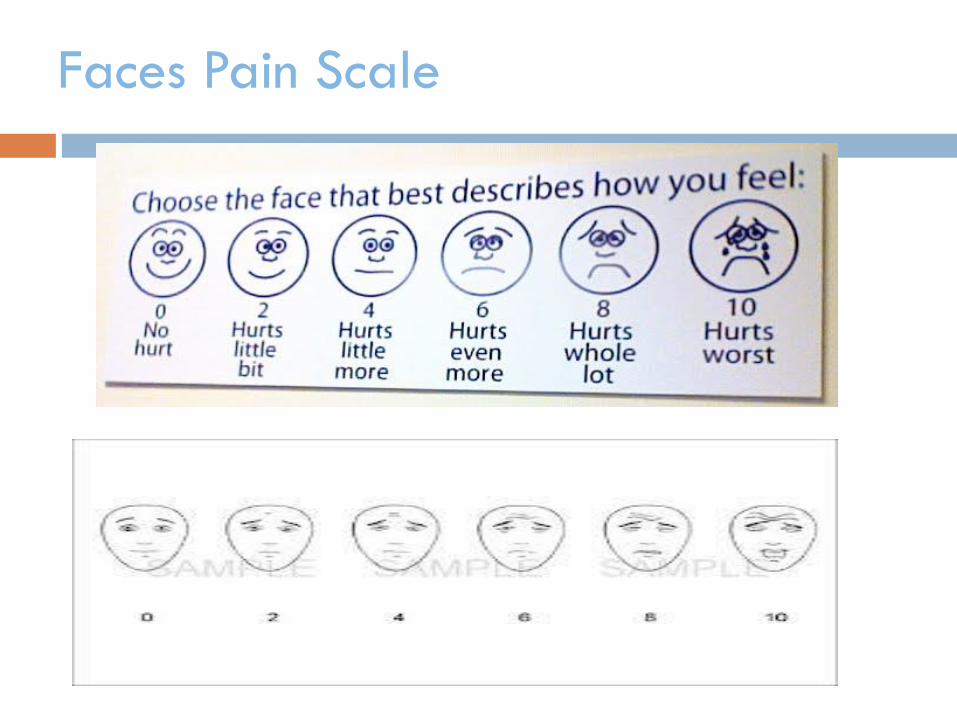
Faces Pain Scale
Assessing pain: Nonverbal, Moderate to Severe
Impairment
Formal assessment tools available but not
necessarily useful in routine clinical settings
PAINAD
FLACC
• Unique Pain Signature
• Nonverbal Pain Indicators
Nonverbal Pain Indicators
Facial expressions (grimacing)
-Less obvious: slight frown, rapid blinking, sad/frightened, any distortion
Vocalizations (crying, moaning, groaning)
-Less obvious: grunting, chanting, calling out, noisy breathing, asking for help
Body movements (guarding)
-Less obvious: rigid, tense posture, fidgeting, pacing, rocking, limping, resistance to moving
Nonverbal Pain Indicators
Changes in interpersonal interactions
-combative, disruptive, resisting care, decreased social interactions, withdrawn
Changes in mental status
-confusion, irritability, agitation, crying
Changes in usual activity
-refusing food/appetite change, increased wandering, change in sleep habits
Unique Pain Signature
How does the patient usually act?
What changes are seen when they are in pain?
family members
nursing staff
Communication across caregiver settings is key!
Assessing pain: Nonverbal, Moderate to Severe
Impairment (AGS Panel 2002)
1) Presence of non-verbal pain behaviors?
-assess at rest and with movement
2) Timely, thorough physical exam
3) Insure basic comfort needs are being met
(e.g. hunger, toileting, loneliness, fear)
4) Rule out other causative pathologies
(e.g. urinary retention, constipation, infection)
5) Consider empiric analgesic trial
Pain Assessment is NOT….
Relying on changes in vital signs
Deciding a patient does not “look in pain”
Knowing how much a procedure or disease “should
hurt”
Assuming a sleeping patient does not have pain
Assuming a patient will tell you they are in pain
Case 1
You are rounding on an 83 y.o. NH patient admitted with pneumonia and stage III sacral ulcer
She has advanced dementia, bed- bound, limited verbalization
PMHx: DM, HTN
Patient stopped eating and is combative with care
Recommended treatment- trial of empiric analgesic, such as acetaminophen 1000 mg or oxycodone 2.5-5mg 3 x day. Monitor for effect.
Case 2
You are rounding on a 75 y.o. male s/p fall
History of lumbar stenosis with new onset severe sharp pain down left leg
Xrays negative
Overnight patient was started on prn NSAIDs
Patient in severe pain at rounds
Question: How do we choose medication and dose in older adults?
Medication Selection
Good pain history
Target to the type of pain
-e.g. neuropathic, nociceptive
Consider non-pharmacologic or non-systemic
therapies alone or as adjuvants
Use the WHO 3-Step ladder
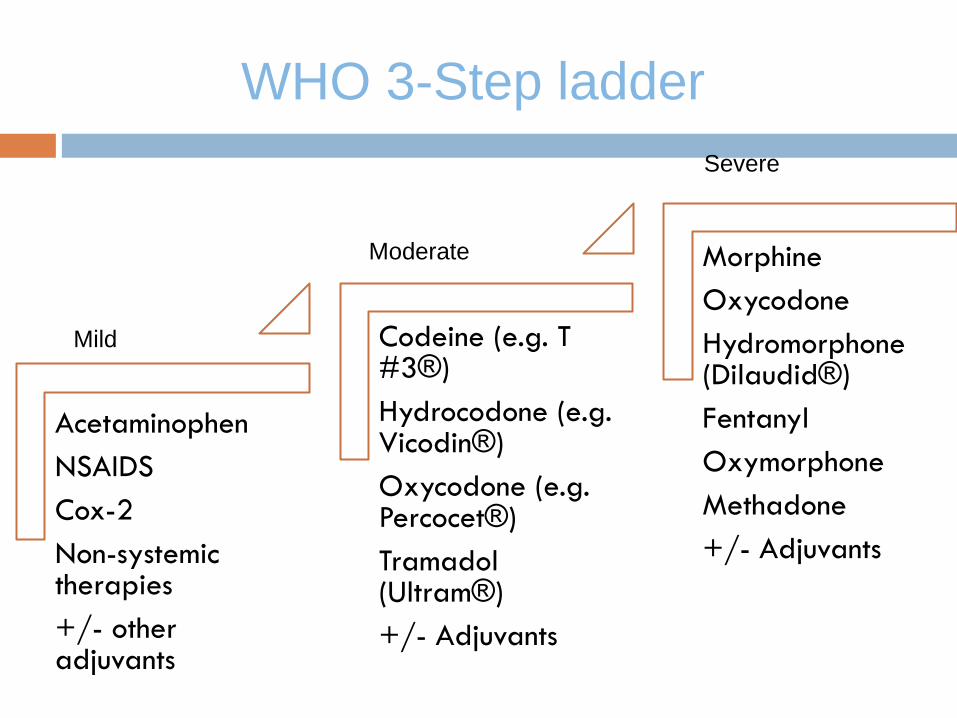
WHO 3-Step ladder
Acetaminophen
NSAIDS
Cox-2
Non-systemic therapies
+/- other adjuvants
Codeine (e.g. T #3®)
Hydrocodone (e.g. Vicodin®)
Oxycodone (e.g. Percocet®)
Tramadol (Ultram®)
+/- Adjuvants
Morphine
Oxycodone
Hydromorphone (Dilaudid®)
Fentanyl
Oxymorphone
Methadone
+/- Adjuvants
Mild
Moderate
Severe
Adjuvants
Topicals (lidocaine patch, capsaicin)
Acetaminophen
NSAIDS, celecoxib, steroids
Anticonvulsants
Antidepressants
Non-pharmacologic (TENS, PT/OT)
Multimodal Approach to Pain
Management
Physical Therapy Pharmacotherapy
Interventional
Approaches
Complementary Alternative
Psychological Support
Case 2
You are rounding on a 75 y.o. male s/p fall
History of lumbar stenosis with new onset severe sharp pain down left leg
Xrays negative
Overnight patient was started on prn NSAIDs
Patient in severe pain at rounds
Drugs to Avoid
Meperidine (Demerol®)
Mixed agonist-antagonist
-e.g. Pentazocine (Talwin®)
Codeine
Opioid Use in Renal Failure
Not rec’d: meperidine, codeine,
Use with caution: oxycodone, hydromorphone, morphine
Safest: fentanyl, methadone
Opioid dosing
CrCl
>50 mL/min normal
10 - 50 mL/min 75% of normal
<10 mL/min 50% of normal
Clearance Concerns: Dehydration, renal
failure, severe hepatic failure dosing interval (increase time between doses)
or
dosage
if oliguria or anuria: consider d/c around the clock
dosing
Opioids for Continuous Pain
Dose find, opioid naive:
-begin with short-acting opioid ATC
-allow breakthrough based on Cmax and patients metabolism
Cmax (peak) after
-po, pr 1 h
-SC, IM 30 min
-IV 6 – 15 min
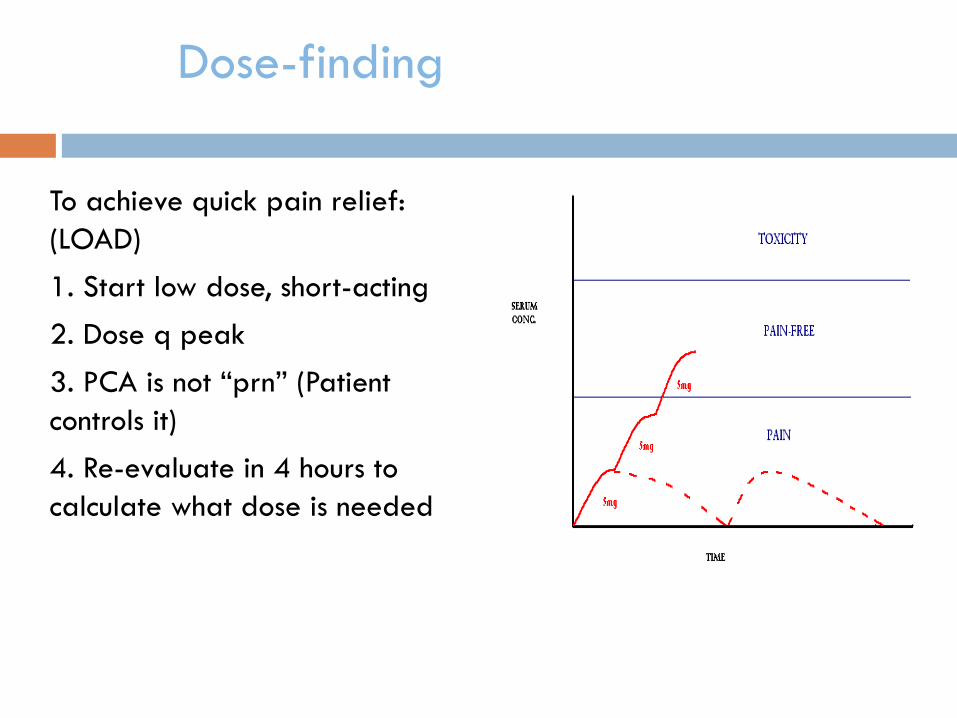
Dose-finding
To achieve quick pain relief:
(LOAD)
1. Start low dose, short-acting
2. Dose q peak
3. PCA is not “prn” (Patient
controls it)
4. Re-evaluate in 4 hours to
calculate what dose is needed
Starting doses and half-life
For thin, frail elderly suggest 2-5 mg po MSO4 or an
equivalent (e.g. 1/2-1 percocet q 4h)
Half-life at steady state
po / po / SC / IM / IV 3-4 h
4-5 half-lives to reach steady state
Opioid Dose Escalation
• Should be done on percentage increase irrespective of starting dose
• mild / moderate pain 25%–50%
• severe / uncontrolled pain 50%–100%
• How frequently? Depends on t1/2
• Short-acting single-agent every 2 hrs
• Long-acting every 24 hours
• Fentanyl transdermal 72 hours
• Methadone 4-7 days
Breakthrough dosing
Use immediate-release opioids
10% of 24-h dose or 1/3 of one ER dose
offer after Cmax reached
po / pr q 1 h
SC, IM q 30 min
IV q 10–15 min
Do NOT use extended-release opioids for
breakthrough
Transdermal Fentanyl
Duration 24-72 hours
12-24 hours to reach full analgesic effect
Has caused fatal respiratory depression in opiate naïve patients (at least 1 week use of 60mg/day of oral morphine required before starting)
Lipophilic
Simple Conversion rule:
-1 mg po morphine = ½ mcg fentanyl
-(60 mg morphine roughly 25 mcg patch)
Case 3
You are rounding on a 70 y.o. male admitted with pleuritic
chest pain
New pulm mass found on chest CT
Severe pleuritic pain well-controlled on hydromorphone 4
mg IV q 3 hours
You want to convert him to something he can take at home
Question: How do convert from one opiate to another route
or drug?
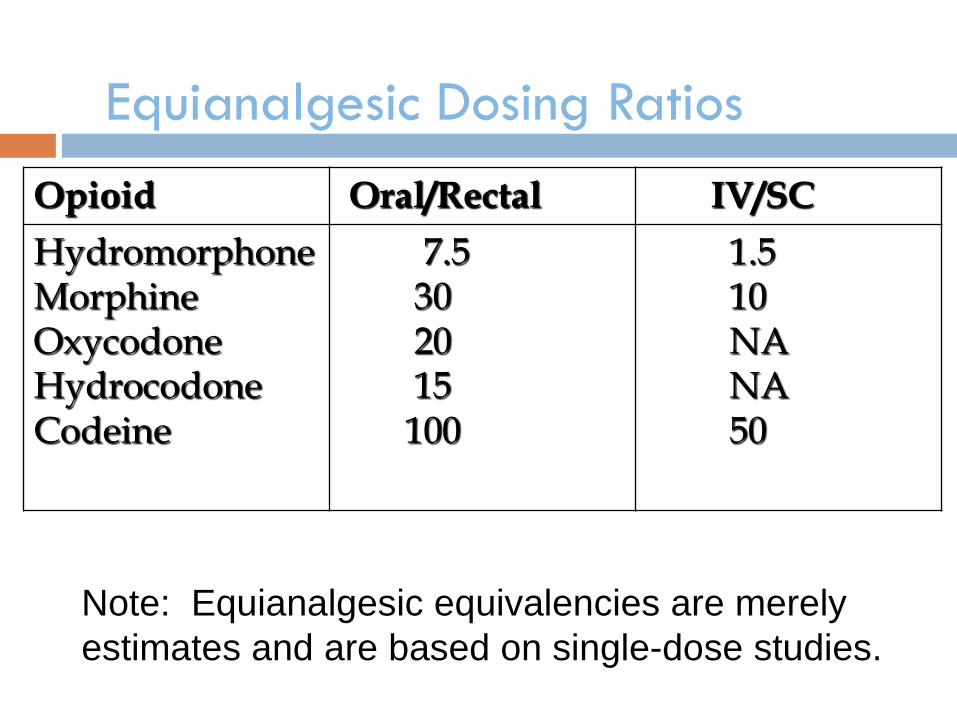
Equianalgesic Dosing Ratios
Opioid Oral/Rectal IV/SC
Hydromorphone
Morphine
Oxycodone
Hydrocodone Codeine
7.5
30
20
15 100
1.5
10
NA
NA 50
Note: Equianalgesic equivalencies are merely
estimates and are based on single-dose studies.
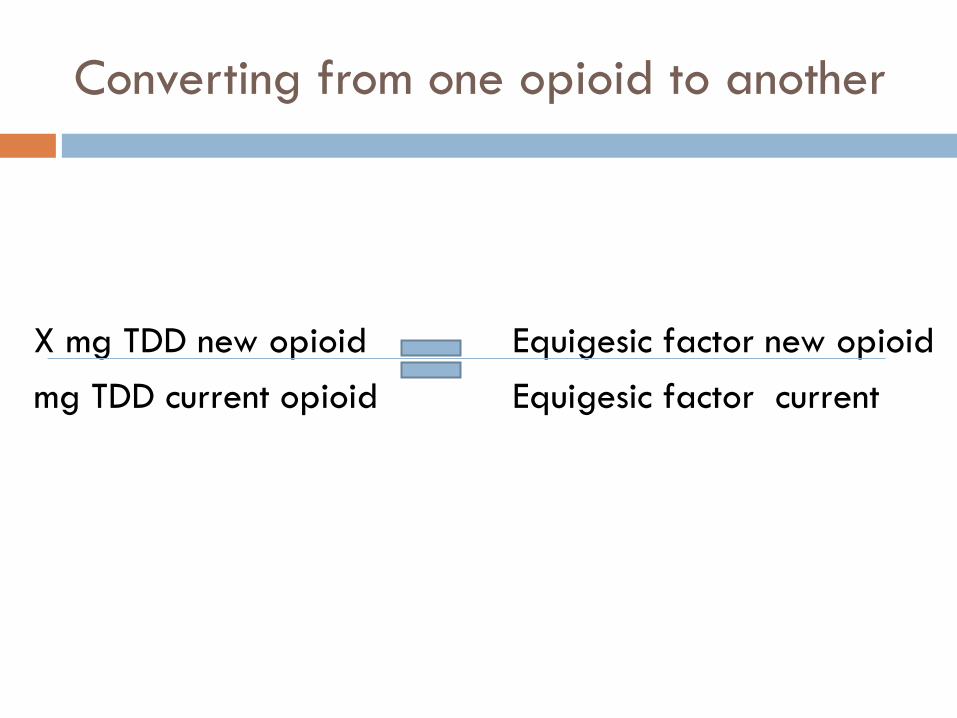
Converting from one opioid to another
X mg TDD new opioid Equigesic factor new opioid
mg TDD current opioid Equigesic factor current
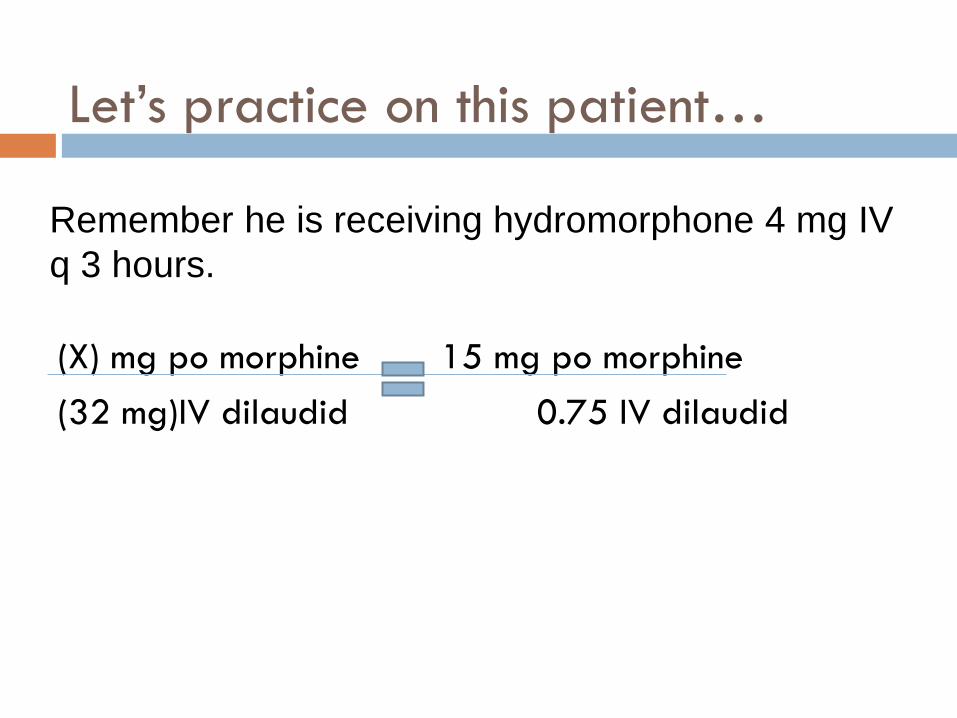
Let’s practice on this patient…
(X) mg po morphine 15 mg po morphine
(32 mg)IV dilaudid 0.75 IV dilaudid
Remember he is receiving hydromorphone 4 mg IV
q 3 hours.
Incomplete cross tolerance
When changing from 1 opiate to another ALWAYS
decrease the dose of the new opiate by 50% of the
equianalgesic dose.
So our patient would need 320mg/day of sustained
release oral morphine
Don’t forget to give immediate release
medication for breakthrough (5-15% of
TDD)
Opiate adverse effects
Constipation
Dry mouth
Nausea / vomiting
Sedation
Sweats
Delirium
Bad dreams / hallucinations
Dysphoria / delirium
Myoclonus / seizures
Pruritus / urticaria
Respiratory depression
Urinary retention
Hypogonadism
SIADH
Common Uncommon
Managing GI Side Effects
• NEVER resolves!
• Prevent with
scheduled softeners
PLUS stimulants
• Avoid bulking agents
(e.g. Metamucil®)
Frequent, small meals
Antiemetic agents
Promotility agents
(metoclopramide)
serotonergic blocking agents (odansetron)
dopaminergic blocking agents (haloperidol, metoclopramide, prochlorperazine)
Constipation
Nausea/Vomiting
The Evidence: Pain, Opioids, and Delirium
Two studies* have reported a significant association between opioid use and delirium
Neither study controlled for pain
All patients received meperidine
*Marcontonio et al, JAMA 1994, Schor et al, JAMA 1992
†Egbert et al, Arch Intern Med 1990 ,
Duggleby & Lander, JPSM 1994,
Lynch et al, Anesth Analg 1998;
Morrison et al, J of Gerontology: Medical Sciences, 2004
Five studies† have reported a significant association between uncontrolled pain and delirium
No relationship found between opioid use/dose and delirium in 4 studies
Opioids found to reduce the risk of delirium in 2 studies
Respiratory Depression
Does not occur in patients on chronic opioids
Can occur in opioid-naïve patients whose opioid dose is rapidly escalated
Is always preceded by slowly progressive somnolence
If you must treat:
-Dilute naloxone (10:1) in saline and infuse 1 mL until breathing pattern returns to normal
Case 4
You are rounding on a 90 year old female with severe osteoporosis admitted for sudden severe back pain
New vertebral compression fracture
Pain controlled on morphine 4 mg IV q 4 hours
Patient very sedated, family concerned
Sedation and Delirium
Consider trying one of the following:
1. If pain control is adequate, decrease dose by 25%
2. Rotate to a different opioid preparation
3. Use small doses of psychostimulants (2.5 to 5 mg methylphenidate or dextroamphetamine) for excessive somnolence
Use nonsedating antipsychotics (haloperidol, risperidone) for delirium
Case 5
Ms. GG is a 67 year-old female with history of
osteoarthritis, coronary artery disease, chronic
kidney disease, and new diagnosis of metastatic
breast cancer, who presents to clinic for follow after
RT to her hip.
She says, “I am taking 10 pills of morphine (600mg
q 12 hours) twice a day; I want to stop it. The
radiation therapy worked and the pain is gone. What
should I do?”
Case 5 continued
Keep in mind the physical dependence properties of
opioids.
Decreased by 50% every 4-5 half lives.
If the dose is lowered too quickly and abstinence signs
appear, you can: increase the opioid transiently, treat
symptoms with clonidine or small amounts of lorazepam.
On average, XRT can take anywhere from 1-4 weeks to
begin having pain relief effects. XRT can cause initially
cause increase in pain due to inflammatory effects and
release of cytokines.
Case 6
AA is a 65-year-old woman with breast cancer
taking long acting morphine who developed a
pathologic fracture of the femur and was started on
Morphine 40mg IV Q4h and the new rescue dose of
24mg IV every 1 hour prn.
The next morning, you come in to see Ms. Amidiaz
but she seems very lethargic. Her respiratory rate is
6 and she is only responsive to painful stimuli.
What should you do?
Opioid Overdose
Provide ventilatory assistance with bag-valve mask
Naloxone should only be used for life threatening opioid induced respiratory depression.
To avoid withdrawal:
Dilute 0.4mg (1 ml) with NS 9ml for a total volume of 10ml and administer 1-2 ml IV q2-3 min until response
Half life: 30-81minutes (mean 64 min)
Naloxone’s half-life is less than most opioid agents so respiratory depression may recur
Common pitfalls to avoid
Changing meds/route on discharge
Writing the prescription
Medication cost
Educating patient/family
Appropriate follow-up
References
Levy M. Drug therapy: Pharmacologic treatment of cancer pain. NEJM 1996;335(15):1124-1132.
EPEC Project, The Robert Wood Johnson Foundation, 1999.
Storey P and Knight CF. UNIPAC 3: Assessment and Treatment of Pain in the Terminally Ill. AAHPM 2003.
Gazelle. Methadone for the treatment of pain. J Pall Med. 2003;6(4):620
AGS Panel on Persistent Pain in Older Persons. JAGS. 2002;50:S205-S224.
American Pain Society. APS Glossary of Pain Terminology. http://www.ampainsoc.org/links/pain_glossary.htm.
Bruera E and Portenoy R. Cancer Pain Assessment and Management. Cambridge University Press, 2003.
Cherny N, Ripamonti C, Pereira J, et al. Strategies to manage the adverse effects of oral morphine: an evidence-based report. J Cli Oncol. 2001;19:2542-2554.
References
Dean M. Opioids in renal failure and dialysis patients. J Pian Symptom Manage 2004;28(5):497-504.
EPERC 063 The Legal Liability of Under-Treatment of Pain, 2nd ed. E Warm, D Weissman.
Gordon DB, Stevenson KK, Griffie J, et al. Opioid equianalgesic calculations. J Palliat Med. 1999;2(2):209-218.
Herr K, Bjoro K, Decker S. Tools for assessment of pain in nonverbal older adults with dementia: A state-of-the-science review. J Pain Symptom Manage 2006;31(2):170-192.
Hewitt DJ, Portenoy RK. Adjuvant drugs for neuropathic cancer pain. Topics in Palliative Care. New York: Oxford University Press 1998:31-62.
Kirsh KL, Passik SD. Palliative care of the terminally ill drug addict. Cancer Invest 2006;24:425-431.
References
Klaschik E, Nauck F, Ostgathe C. Constipation – modern laxative therapy.
Support Care Cancer 2003;11:679-685.
Mercadante S and Bruera E. Opioid switching: A systematic and critical
review. Cancer Treatment Reviews 2006;32:304-315.
Meuser T, Pietruck C, Radbruch L, et al. Symptoms during cancer pain
treatment following WHO guidelines: a longitudinal follow-up study of
symptom prevalence, severity, and etiology. Pain 2001;93:247-257.
Skaer TL. Transdermal opioids for cancer pain. Health and Quality of Life
Outcomes 206;4(24):1-9.
Swegle JM and Logemann C. Management of common opioid-induced
adverse effects. Am Fam Physician 2006;74:1347-1354.
WHO ladder:Cancer Pain Relief and Palliative Care. Technical Report Series
804. Geneva: World Health Organization; 1990.