Embed Size (px)
Citation preview
PAIN
PainCommon causes of oro-facial pain Local disorders
◦ Teeth & supporting tissues◦ Jaws◦ Maxillary antrum◦ Salivary glands◦ Pharynx◦ eyes
Neurological disorders◦ TN◦ Neoplasms involving the Trigeminal nerve◦ Glossopharyngeal neuralgia◦ Herpez Zoster◦ Multiple sclerosis◦ SUNCT sydrome
CausesVascular
◦Migraine◦Migrainous Neuralgia◦Giant cell arteritis◦Neuralgia induced cavitational
osteonecrosis (NICO)Psychogenic
◦Atypical facial pain◦Burning mouth syndrome◦TMPD
Referred pain
Analysis
Previous HistoryLocation
◦ Localized◦ Generalized◦ Focuses◦ Diffuse
Duration◦ Dentinal pain transient◦ Pulpitis longer◦ TN Brief lancinating◦ Migrainous Neuralgia 30-45 minutes◦ Migrain hours-days◦ Atypical facial pain persistent
AnalysisCharacter
◦Continuous◦Throbbing◦Severity
Ask the patient to scale it from 0-10
◦Dull◦Lancinating◦Burning sensation◦Interference with sleep
AnalysisFrequency & Periodicity:
◦ Pain on laying down/bowing Sinusitis◦ Disturbs sleep in the midnight (around 2am)
Migrainous neuralgia◦ Pain on waking TMPDS
Provoking or relieving factors:◦ Temperature dental pain◦ Trigger zone TN◦ Stress atypical facial pain◦ Alcohol migrainous neuralgia◦ Biting periapical pathology◦ Postural sinusitis?
Analysis
Other factors:◦Nausea/vomiting◦Facial swelling◦Nasal stuffiness◦Lacrimation◦Neurological signs & symptoms◦Relief by analgesics◦Weight loss◦TMJ click◦Trismus
Local Causes
Dental Pain
Dentinal:Sharp & deepEvoked by external stimulus i.e.
hot, cold, sweet, sour, salty foods/drinks
Subsides within few secondsPoorly localized
Dental Pain
PulpalPulp Vitality testPain may be
◦Sharp & intense, elicited by change in temp. remains for 5-10 minutes, remains diminished untill stimulated again Reversible Pulpitis
◦Spontaneous, dull, more than 20 minutes duration, difficult to localize, affected by body position Irreversible pulpitis
Pulpal
Diagnostic ToolsHistory, nature & duration of painReaction to thermal changesReaction to mild electrical
stimulusReaction to tooth percussionRadiographic examinationVisual clinical examinationPalpation of surrounding area
PeriodontalMore localized than pulpal painLess severeAssociated with
tenderness/pressureUsually not aggravated by
heat/cold
Acute peri-apicalSpontaneousModerate to severePersists for long periodsOn percussion/biting on toothExtruded tooth in severe casesUsually precisely located by
patientUsually associated with non-vital
toothSwelling of the face?
Other Oral CausesLateral periodontal abscessFood impactionCracked toothPericoronitisANUGMucosal
Other oro-facial painsJawsAcute infectionsMalignanciesPaget’s diseaseDirect traumaCystsRetianed rootsInfected impactionsRadiation therapy osteo-radio
necrosis osteomyelitis
Other oro-facial painsTMJDysfunctionAcute inflammationTraumaMalignanciesMuscularPain is usuallyDullPoorly localizedRadiatesIntensified by movement of mandible
Other oro-facial pains
Salivary glandsIn children mumpsIn adults calculi or mucous plugSevere pain in acute parotitisPain is
◦Localized to affected gland◦Quite severe◦Intensified by increased salivation

Other oro-facial pains
SinusesPreceding coldPain & tendernessRadio-opacity of sinusesUpper molars/premolars become
tender in maxillary sinusitisTumours of sinusesPressure on Mental nerve
Neurologic causesTrigeminal neuralgiaGlossopharyngeal neuralgiaPost-herpetic neuralgiaIdiopathic TNAny lesion affecting Trigeminal n.
◦Traumatic◦Cerebrovascular disease◦Multiple sclerosis◦ Infections such as HIV◦ Inflammation◦Neoplasia (Nasopharyngeal/antral ca.)
Vascular causesMigraineMigrainous neuralgiaGiant Cell ArteritisNeuralgia Induced Cavitational
Osteonecrosis
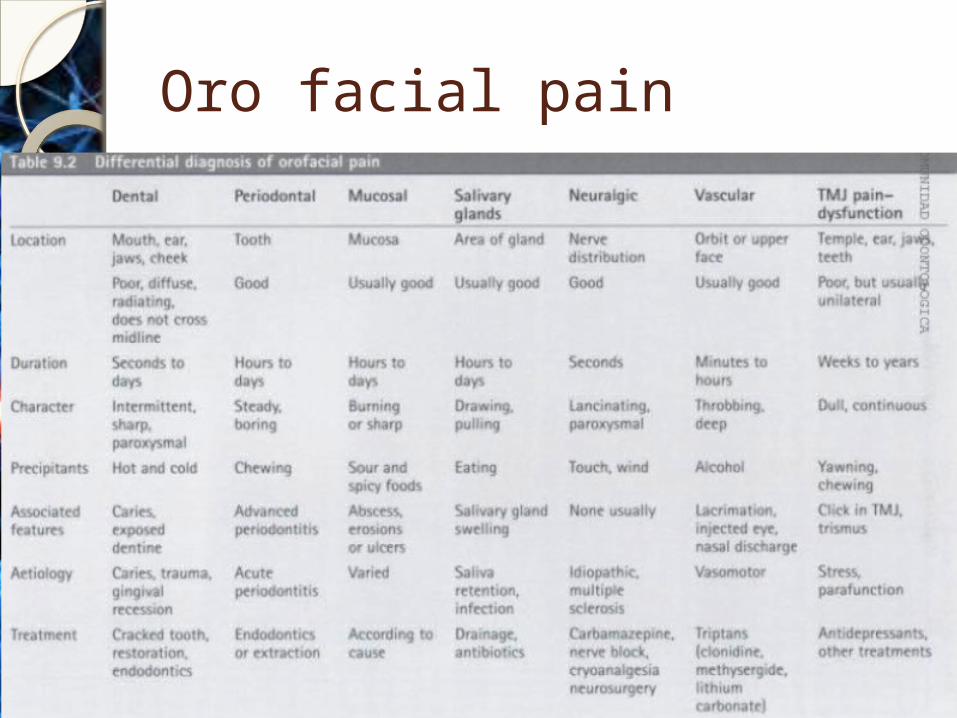
Oro facial pain
Neuralgias
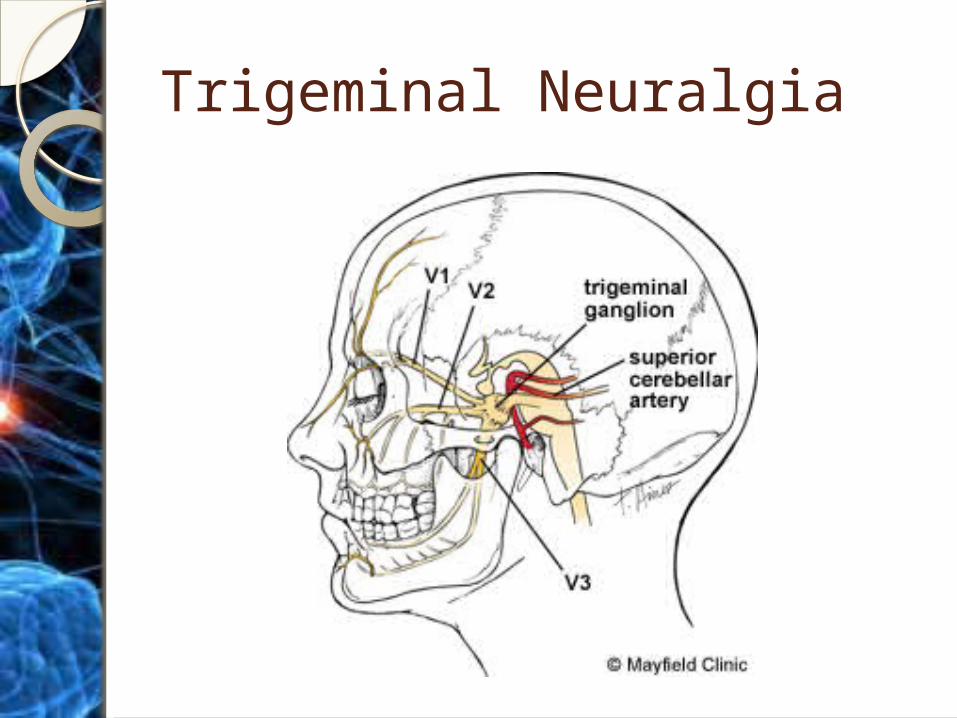
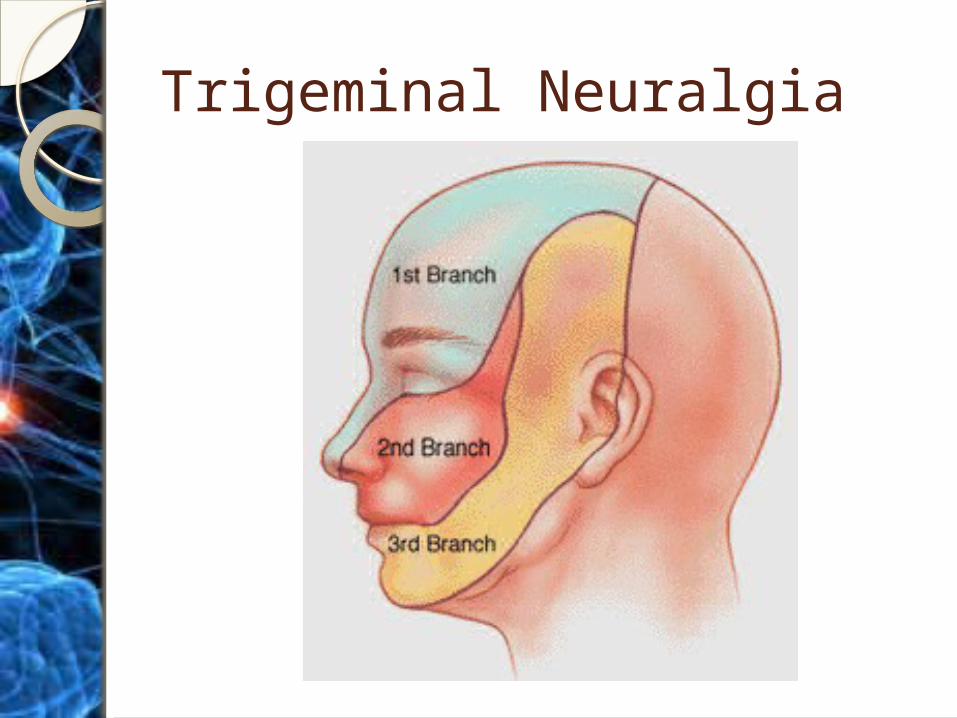
Trigeminal NeuralgiaA disorder of trigeminal nerve
that causes episodes of unilateral, intense, stabbing, electric shock like pain in the areas of face along the distribution of branches of this nerve
Areas effected may include lips, eyes, nose, scalp, forehead, upper/lower jaw
One of the most painful afflictions known
Trigeminal NeuralgiaTypes
◦Classical◦Symptomatic◦Idiopathic
Trigeminal NeuralgiaMost common neurological cause
of facial pain4 per 100000 patients50-70years age groupMore common in femalesNo specific predisposing factors
but emotional or physical stress, hypertension may be related
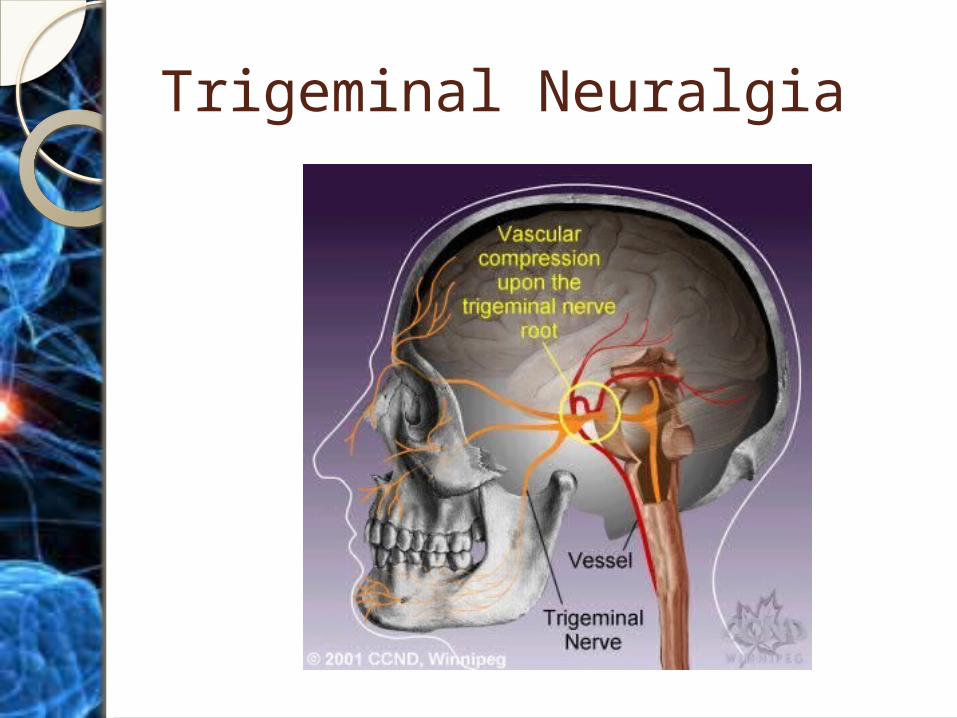
Trigeminal Neuralgia - PathophysiologyExact cause isn’t knownCompression around trigeminal root
due to atherosclerotic blood vessels is the hypothesized cause
Demyelination of trigeminal nerve causing ectopic pulses
Compression by tumourBony compressionAV malformationAmyloidPons infarct
Trigeminal Neuralgia
Trigeminal Neuralgia
Trigeminal Neuralgia – C/FMainly affects 2nd & 3rd divisions
of trigeminalParoxysmal attacks of facial painCan last from few seconds to 2
minutesOccurs mostly in the morningSpontaneous remission may be
possibleOr patients may have episodic
attacks over many years
Trigeminal Neuralgia – C/FPain has atleast four characteristics
◦A distribution along one or more divisions of trigeminal n.
◦A sudden, intense, sharp, superficial, stabbing or burning pain
◦Intensely severe◦Precipitation from trigger areas or certain
daily activities such as eating, talking, washing the face, shaving or cleaning teeth
◦Usually asymptomatic between paroxysms but some patients report a dull ache
Trigeminal Neuralgia
Trigeminal Neuralgia – C/FNo neurological deficitAttacks are stereotyped in
individual patientsAtypical TNLess intense, constant, dull
burning or aching pain with occasional electric shock like stabs
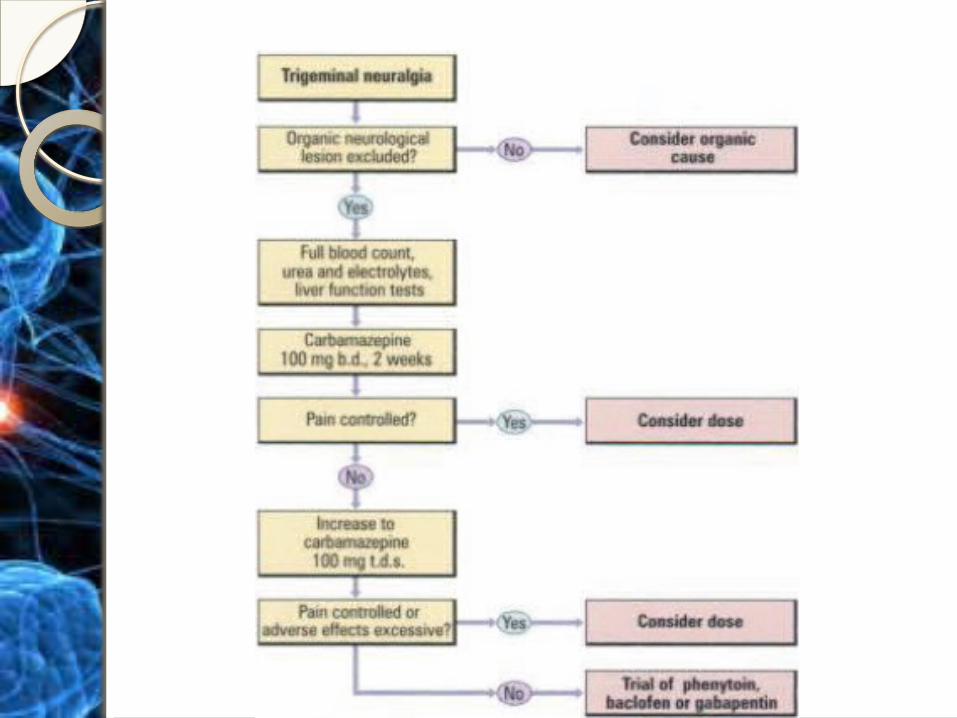
DiagnosisExclusion of other causes of pain
by history, physical examination & further evaluation necessary
Exclusion of physical signs such as facial sensory or motor impairment, CVA, Multiple sclerosis, infections (HIV) or neoplasms
ManagementAnticonvulsants
CarbamazepineIt is the main drug of choicePrevents attacks in 60% of
patientsGiven continuousely &
prophylactically for long periodsUsed carefully & under strict
medical surveillanceContra-indicated in pregnancy
Dose regime100mg B.D for 2 weeksCan be increased by 100mg daily every 3 days
to a maximum dose of 1000mg/dailyBlood monitoring mandatoryAdverse effects
◦ Ataxia◦ Drowsiness◦ Visual disturbances◦ Headache◦ GIT effects◦ Folate deficiency◦ Hypertension◦ Pancytopenia or leukopenia◦ Interaction with cimetidine, isoniazid, interferes
with oral contraceptives
Monitoring B.P: first 3 months..then 6
monthlyBlood tests:
◦Electrolytes (for hyponatraemia)◦LFTs◦RBC, WBC & Platelet counts
Surgical interventionPeripheral surgery
◦Local cryosurgery◦Injections of glycerol or streptomycin
around mandibular or infra-orbital foramen
◦Peripheral neurectomy◦Radiofrequency thermocoagulation
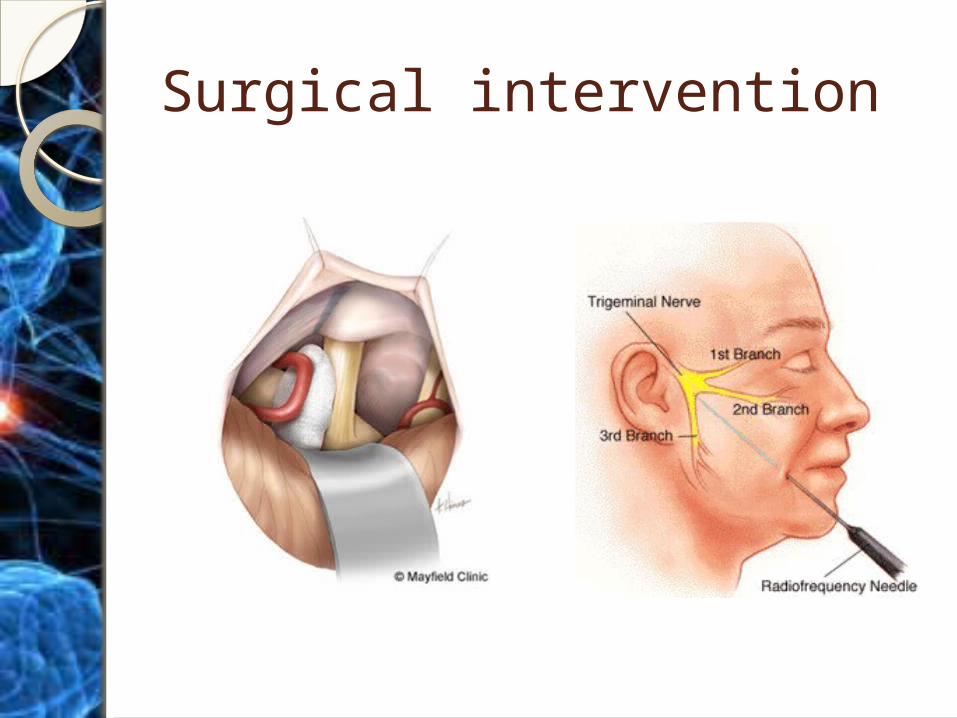
Surgical interventionCentral neurosurgery
◦Micro-vascular decompression◦Gasserian ganglion operations
Injections around trigeminal ganglion Radiofrequency thermocoagulation
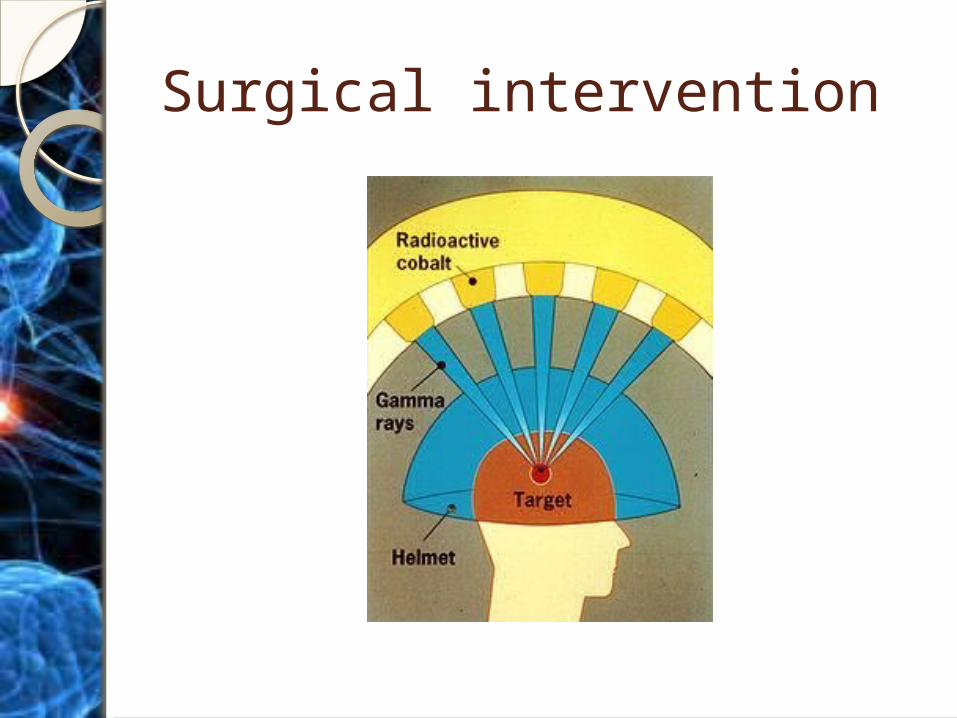
ganglionolysis Gamma knife Trigeminal ganglion microcompression
using Fogarty ballon catheter
◦Posterior cranial fossa procedures
Surgical intervention
Surgical intervention
Differential DiagnosisGlossopharyngeal neuralgiaGiant cell arteritisCluster HeadacheIntracranial tumourPost-herpetic neuralgiaMultiple sclerosisMigrainDental painTMPDS
Glossopharyngeal Neuralgia
Glossopharyngeal NeuralgiaA pain syndrome characterized
by unilateral, sharp pain along the sensory distribution of ninth cranial nerve (glossopharyngeal n.)
Glossopharyngeal NeuralgiaPain characterAcute pain that lasts from seconds to
few minutesLancinating, stabbing, shooting &
electric shock likeFelt in the ear, throat, posterior part
of tongue, soft palate & lower lateral & posterior parts of pharynx
Triggered by swallowing & speech resulting in weight loss
Glossopharyngeal NeuralgiaBetween the attacks, patient may remain
pain free or may have feeling of pressure & burning lasting for several minutes
In some patients, attack may be associated with vasomotor changes (syncope, bradycardia, hypotension or even asystole) making it potentially fatal
Differentiated from TN by distribution & triggering movements (swallowing, talking, coughing)
In 15% patients, both conditions are present & symptoms overlap
Glossopharyngeal NeuralgiaIncidenceLess common than TNA population bases study showed
an incidence of 0.7 in 100,000More common in menIncidence increases with age (>
50 years)
Glossopharyngeal NeuralgiaEtiologyTwo typesWithout discernable cause
idiopathic or essential GPNWith underlying pathology
secondary GPN
Glossopharyngeal NeuralgiaIdiopathic or Essential GPNBelieved to be caused by
vascular compression of ninth cranial n. (theory supported by success of MVC in elimination of symptoms)
Or central (pontine) dysfunction
Glossopharyngeal NeuralgiaSecondary GPNNeoplasmsVascular malformationsInfectionsDemyelinationTraumaElongated styloid process (eagle’s
syndrome)Other causes
Eagle’s syndromeA painful condition first described
in 1937 caused by elongated styloid process
Pain in Eagle’s syndrome resembles that of GPN
Pain is more constant & dullTwo types
◦Classic◦Carotid artery syndrome
Eagle’s syndrome
ClassicSpasmatic, nagging painSeen in patients with elongated
styloid process (> 3-3.5cm) or ossification of stylohyoid
ligamentSometimes seen in
tonsillectomized patients
Eagle’s syndrome
Carotid artery syndromePain of pharyngeal distributionBecomes prominent on head
turningNot related to previous surgeryCaused by pressure exerted by
elongated styloid process on carotid artery when the head is turned
Glossopharyngeal Neuralgia
Association with syncope & hypotention
GPN is known to be associated with cardiac syncope, arrhythmias (bradycardia) & hypotension
Cardiovascular abnormality is seen during the pain attack or immediately following it
Glossopharyngeal NeuralgiaAssociation with syncope &
hypotentionTwo theories1. Intense neuralgic pain activates
glossopharyngeal-vagal reflex arc
2. Direct inhibition of vasomotor center peripheral vasodilation hypotention
ManagementCarbamazepine is the drug of
choiceMay partially effective in some
patientsMay cause drowsiness, dizziness
or itchingMay develop gradual tolerance
with persistent high dose necessitating surgical intervention
Management Other medications
◦Baclofen◦Ketamine◦Various analgensics◦Lamotrigine◦Local anaesthesia blocks for
therapeutic & diagnostic purpose Infilteration of pharyngeal area Glossopharyngeal nerve block at jugular
foramen Or local application of cocaine to throat
Management Injection of neurolytic substances
such as phenol in glycerine21 guage needle 0.5cm lateral to
margin of anterior pillar at its lower end
0.7ml of 5% solution of phenol in glycerine
Lateral margin of tongue near anterior pillar directed to its base
ManagementPercutaneous rhizotomyExtracranial
neurotomy/neurectomyIntracranial rhizotomyMicrovascular decompression
Atypical Facial Pain
Atypical Facial PainConstant chronic oro-facial pain
defined as a “facial pain not fulfilling other criteria”
Falls under the category of Medically Unexplained Symptoms (MUS)
Atypical Facial Pain
CharacteristicsConstant chronic orofacial
discomfort/painDull, boring or burning typeIll-defined locationTotal lack of objective signsAll investigations negativeNo cause detectedPoor response to treatment
Atypical Facial Pain1-2% of population suffers from itMiddle aged – older adults> 70% womenThere may be history of adverse
life events, family illness, dental or oral procedures
Aetiology & PathogenesisPositron Emission Tomography in
patients with AFP shows enhanced cerebral activity enhanced alerting mechanism in response to peripheral stimuli release of neuropeptides production of free radicals cell damage release of prostaglandins pain
Atypical Facial Pain – C/FCheek, nose, upper lip or sometimes lower
jawLocation of pain is unrelated to anatomical
distribution of trigeminal nerveMay last for hours days or weeksPoorly localizedMay cross the midline, change its location,
usually bilateralDoes NOT awaken the patient from sleepDeep, dull, boring/burning sensation, may
cause lacrimation & watering of nose
Atypical Facial Pain – C/FMay have other related problems such
as◦Dry mouth◦Bad taste◦Headaches◦Chronic back pain◦Irritable bowl syndrome◦Dysmenorrhoea
History of multiple consultations & attempts at treatment
Pain accompanied by altered behaviour, anxiety, depression & hypochondriasis
Atypical Facial PainExaminationNo erythema, tenderness or swellingNo odontogenic or other cause of painLack of objective physical signsAll investigations are negativeDxDiagnosis is clinicalCareful examination of oral, perioral
structures, all radiographs to rule out othe causes
ManagementCognitive behaviour therapy
(CBT)Specialist referral for
psychogenic treatment
Burning mouth syndrome
Burning mouth syndrome
Also known as glossopyrosis, glossodynia or stomatodynia
Is defined as a burning sensation in the absence of identifieable organic etiology
Also comes under MUS
Burning mouth syndrome5 persons/100,000Middle aged-older adultsFemale predilectionNo precipitating cause detected in 50%
patientsIn 20% cases, psychogenic cause can
be identifiedIn others it follow:
◦Dental intervention◦Upper respiratory tract infection◦Drugs such as ACE or protease inhibitors
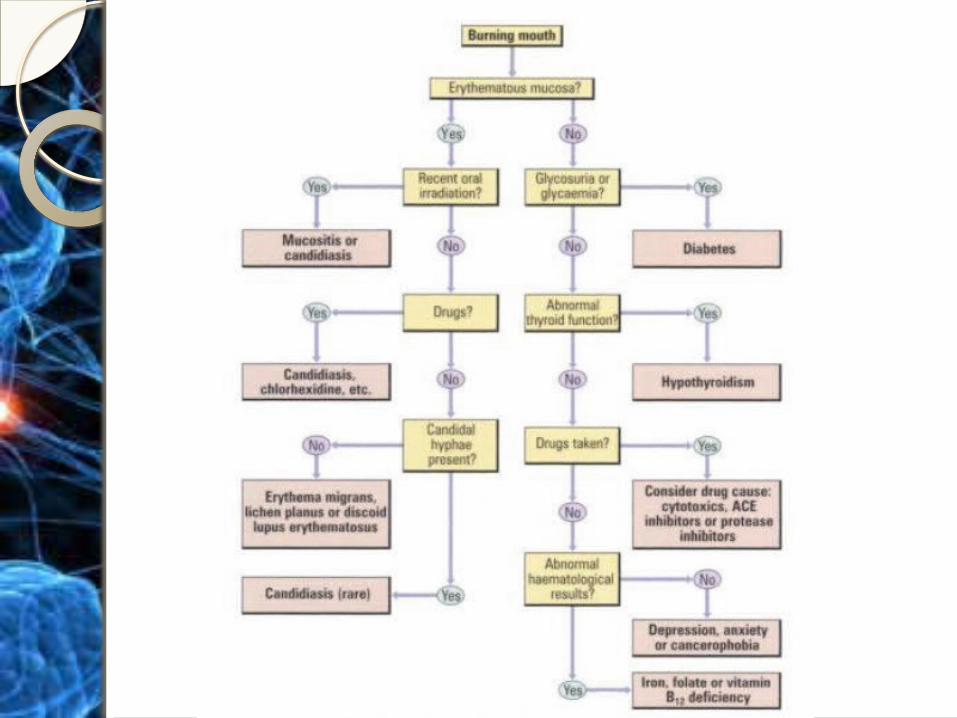
Burning mouth syndromeDiagnosis depends on exclusion
of other causes of burning sensation◦Erythema migrans◦Lichen planus◦Dry mouth◦Candidiasis◦Glossitis following nutritional
deficiency◦Diabetes
Burning mouth syndromeExclusion of organic causes such
as◦Haematological deficiency (iron, folic
acid, vit B)◦Restricted tongue space due to
denture◦Para-function such as bruxism,
tongue thrusting◦Neuropathy◦Thyroid dysfunction◦Drugs
Burning mouth syndrome – C/FMostly affects tongueMay affect palate, lips or lower alveolusBurning sensation is chronic, bilateralOften relieved by eating/drinkingMay accompany
◦Dry mouth◦Altered taste◦Thirst◦Headaches◦Chronic back pain◦ Irritable bowl syndrome◦dysmenorrhoea
Burning mouth syndrome
DiagnosisExamination to rule out other
causesAll investigations are negative
Management Avoid anything that aggravates
symptomsAvoid active dental or surgical
treatmentCognitive behavioural therapy &
referral to specialist