Embed Size (px)
Citation preview

SKULL BASE SURGERY/VOLUME 8, NUMBER 1 1998
CASE REPORT
Palatal Adenoid Cystic Carcinoma Presenting as
Perineural Spread to the Cavernous SinusLawrence E. Ginsberg, M.D., and
Franco DeMonte, M.D.
Adenoid cystic carcinoma of salivary gland originis an uncommon head and neck malignancy accountingfor 4-15% of salivary gland tumors and 25-37% of mi-nor salivary gland malignancies.'-3 The minor salivaryglands are distributed widely throughout the upperaerodigestive tract mucosa but are concentrated in theposterior hard and soft palate.1'24 The palate is the mostcommon site of both benign and malignant tumors ofminor salivary gland origin. Adenoid cystic carcinomasare notorious for their tendency to spread along smallcranial nerve branches, usually branches of the trigemi-nal nerve, a process known as perineural spread.2.5.6 Insome cases, disease at the site to which the tumorspreads becomes clinically evident prior to detection ofthe primary carcinoma.7,8 In such instances, the true di-agnosis may be obscure. Retrograde spread of adenoidcystic carcinoma along maxillary nerve (V2) branchesoften involves the pterygopalatine fossa, orbit, or cav-ernous sinus.9-13 This pattern of neoplastic spreadshould be kept in mind when evaluating patients withcavernous sinus masses in order to avoid undertreat-ment or nontreatment of the primary disease. We de-scribe three cases, one previously reported,8 in which acavernous sinus mass represented perineural spreadfrom a palatal adenoid cystic carcinoma. In all cases, the
primary tumor was not initially suspected or evidentclinically, and in two cases, disease that may have led tothe correct diagnosis was missed radiologically. In twocases, there was no evidence that the possibility of ahead and neck primary tumor was ever considered orpursued.
CASE REPORTS
Patient 1, a 35-year-old woman, noticed right-sided numbness and a small lump in the roof of themouth. Several months later, decreased visual acuity inthe right eye prompted her to seek medical attention.After a several month work-up, a magnetic resonanceimaging (MRI) and computed tomography (CT) studywere obtained. These demonstrated mass-like soft-tis-sue thickening in the right orbital apex and cavernoussinus (Fig. 1). This was interpreted as idiopathic inflam-matory orbital pseudotumor. Tumor in the right ptery-gopalatine fossa (Fig. 1) was not appreciated. A pteri-onal craniotomy was performed, and biopsy of materialfrom the right superior orbital fissure and parasellar/middle cranial fossa region was diagnostic for adenoidcystic carcinoma. According to the outside medical
Skull Base Surgery, Volume 8, Number 1, 1998. Departments of Diagnostic Radiology (L.E.G.), and Neurosurgery (F.D.), The University ofTexas M. D. Anderson Cancer Center, Houston, Texas. Reprint requests: Dr. Ginsberg, Diagnostic Radiology, Box 57, UT M. D. AndersonCancer Center, 1515 Holcombe Blvd., Houston, TX 77030. Copyright C 1998 by Thieme Medical Publishers, Inc., 333 Seventh Avenue, NewYork, NY 10001. All rights reserved.
39

SKULL BASE SURGERY/VOLUME 8, NUMBER 1 1998
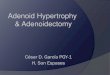
Figure 1. Patient 1. Initial outsidenoncontrast axial Ti -weighted MR imagesthrough the orbit and pterygopalatinefossa. Left: Soft-tissue infiltration is seen inthe right orbital apex, superior orbital fis-sure, and anterior cavernous sinus (arrow-heads). Right: There is tumor infiltrating theright pterygopalatine fossa (arrow) and ex-tending posteriorly along the foramen ro-tundum (small arrowheads). Normal fatsignal can be seen in the left pterygopala-tine fossa (large arrowhead).
record, a head and neck primary tumor was neversought, and the patient reported that her oral complaintshad been ignored. An MRI performed at the time ofbiopsy showed a subtle mass in the right hard palate andposterior maxillary alveolar ridge (Fig. 2) that was notappreciated. The patient received radiotherapy to her or-
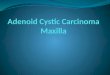
Figure 2. Patient 1. Coronal postcontrast, fat-sup-pressed, Ti-weighted MRI images through the posteriororbits and maxilla. Top: Image obtained at the time of cav-ernous sinus biopsy shows an enhancing mass in the righthard palate (*). Bottom: On image obtained 20 months af-ter biopsy, the right-sided hard palate tumor is still evidentand perhaps slightly larger (*. More tumor is now seen ex-tending posterolaterally into the retromolar and lateralgingival region (arrows).
bital apex/cavernous sinus region. Twenty months afterher initial surgery, the patient was evaluated at our insti-tution. The palatal mass, which had not been included inthe radiation field, had enlarged and become clinicallyevident (Fig. 2) and she had persistent disease in the or-bital apex/cavernous sinus and pterygopalatine fossa.Other images (not shown) demonstrated perineural tu-mor spread along the vidian nerve.
Patient 2, a 47-year-old woman, developed right-sided sixth cranial nerve paresis. She reported "doublevision and a funny feeling in the right side of the face."MRI at an outside institution showed a mass in the rightcavernous sinus (Fig. 3). This was believed to be ameningioma or trigeminal neuroma. Neoplastic in-volvement of the pterygopalatine fossa and foramen ro-tundum was, in retrospect, present but was not appreci-ated at that time (Fig. 4). A small mass in the right hardpalate (Fig. 5) also was not appreciated. The cavernoussinus mass was resected and histologically confirmed tobe adenoid cystic carcinoma, for which the patient re-ceived radiotherapy. A search for a primary cancer wasfruitless because the palate primary was entirely submu-cosal and did not deform the oral surface of the palate(Fig. 5). Follow-up imaging showed regression of thecavernous sinus tumor, but again missed the disease inthe hard palate and pterygopalatine fossa, although inretrospect, disease was present at those locations.Thereafter, the patient developed right eyelid pain, pto-sis, right-sided blindness, and eventually right-sided fa-cial paralysis. Upon evaluation at our institution, MRIrevealed massive tumor involvement of the ptery-gopalatine fossa, V2 within the foramen rotundum, cav-ernous sinus, middle cranial fossa, and Meckel's cave(Fig. 6). There was posterior perineural tumor spreadalong the greater superficial petrosal nerve into and in-cluding the geniculate ganglion, accounting for the fa-cial nerve paresis (Fig. 6). There was also antegradeperineural tumor spread inferiorly along the mandibularnerve (V3) through foramen ovale and anteriorly alongthe infraorbital nerve (Fig. 5). The original palatal le-sion, never having received therapy, had enlarged con-siderably (Fig. 5).
40

PALATAL ADENOID CYSTIC CARCINOMA-GINSBERG, DEMONTE
noma, histologically identical to the initial cavernous si-nus specimen. By this time, the patient had a massiveskull-base tumor with perineural tumor spread alongmultiple cranial nerves, including the greater superficialpetrosal nerve. To our knowledge, the palate primarywas radiologically and clinically silent at first presenta-tion.
DISCUSSION
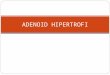
Figure 3. Patient 2. Initial outside coronal Tl-weighted MRI image showing a right-sided cavernous si-nus/parasellar/Meckel's cave mass (arrow).
Patient 3 was the subject of a previous report.8Briefly, the patient was a 49-year-old man who was ini-tially believed to have trigeminal neuralgia. MRI re-vealed a cavernous sinus mass, with biopsy diagnosticfor adenocarcinoma. The patient failed to respond to ra-diation and chemotherapy, developed multiple cranialneuropathies, and then failed to respond to gamma knifetherapy. His condition progressed to complete ophthal-moplegia. Ultimately, a mass was detected in the ipsilat-eral hard palate; biopsy showed adenoid cystic carci-
Figure 4. Patient 2. Initial outsidenoncontrast axial, Ti -weighted MR im-ages. Left: Tumor can be seen widening theright pterygopalatine fossa (arrow). Right:A slightly more cephalad image showstumor extending posteriorly through agrossly widened right foramen rotundum(arrows).
Perineural tumor spread is common in head andneck malignancies, particularly squamous cell carcino-mas of the skin and adenoid cystic carcinomas of themajor or minor salivary glands.'3'4 The second andthird divisions of the trigeminal nerve are among themost common nerves affected by perineural tumorspread." The descending portion of the seventh cranialnerve may also be affected," as may smaller cranialnerve branches.8'5 Perineural tumor spread is a poorprognostic indicator.'4 Perineural spread from palatalcarcinoma has been described in the head and neck liter-ature.19'2'6 Detection of the palatal primary tumor maybe difficult because these lesions are often submucosalin origin' and, as in Patient 2, may not be palpable.
The neuroanatomy of the maxillary division of thetrigeminal nerve facilitates perineural tumor spreadfrom the palate as follows: from the hard and softpalate, sensory fibers of the greater and lesser palatinenerves, respectively, pass through the greater or lesserpalatine foramen and course upward along the descend-ing pterygoid canal to enter the pterygopalatine fossa.There, the fibers pass uninterrupted through thesphenopalatine (pterygopalatine) ganglion and join themain trunk of V2. The fibers then course posteriorlythrough the foramen rotundum, cavernous sinus, andMeckel's cave and finally into the brainstem. 17 Other ef-
41

SKULL BASE SURGERY/VOLUME 8, NUMBER 1 1998
Figure 5. Patient 2. Noncontrastcoronal, Ti -weighted MR images. Left: Ini-tial outside study obtained at the sametime as Figures 3 and 4 shows a small massin the right side of the hard palate (arrow).Note that the oral surface of the palate isnot deformed. This lesion would not havebeen palpable. Right: Image obtainedupon referral to M. D. Anderson CancerCenter shows considerable enlargement ofthe palate mass. Notice the enlargement ofthe right infraorbital canal/nerve indicatingantegrade perineural tumor spread (arrow).
ferent, postganglionic parasympathetic secretomotorfibers (branches of the seventh cranial nerve) alsocourse within the palatine nerves as follows: seventhnerve fibers originating in the nervus intermedius leave
Figure 6. Patient 2. Contrast-enhanced, fat-sup-pressed, axial Ti-weighted MRI images through the skullbase. Top: Enhancing tumor can be seen in the right ptery-gopalatine fossa (*), foramen rotundum (arrow), and cav-ernous sinus/Meckel's cave (arrowheads). Bottom: Imageslightly more caudal shows tumor infiltrating posterolater-ally along the course of the greater superficial petrosalnerve (small arrowheads). Abnormal enhancement andthickening indicate tumor involvement of the geniculateganglion (black dot), and the labyrinthine (large arrow-head) and proximal tympanic (arrows) segments of theright facial nerve.
the seventh nerve at the geniculate ganglion as thegreater superficial petrosal nerve.8,17'8 Exiting the supe-rior surface of the temporal bone through the facial hia-tus, the greater superficial petrosal nerve courses medi-ally and anteroinferiorly to the foramen lacerum andjoins the deep petrosal nerve of the sympathetic plexusto enter the vidian or pterygoid canal as the vidian nerveor nerve of the pterygoid canal.8"17'8 Arriving in thepterygopalatine fossa, these fibers synapse in thesphenopalatine ganglion, and some of the postgan-glionic fibers join the palatine nerves to course inferi-orly into the hard and soft palate. Other postganglionicparasympathetic fibers from the sphenopalatine gan-glion supply secretomotor innervation to the nasal cav-ity and lacrimal gland via other branches of V 8,1718Clearly, access to this neural pathway by carcinoma canresult in widespread extension and a variety of neuro-logic signs and symptoms.
Imaging evidence of perineural spread includesany of the following: widening and/or destruction ofneural foramina (in this case, the greater and lesser pala-tine foramen or foramen rotundum),2'613 replacementof normal fat density (CT) or signal intensity (Tl -
weighted MRI) with abnormal enhancement or widen-ing of the pterygopalatine fossa, widening or excessiveenhancement within the foramen rotundum (or foramenovale), or expansion or abnormal enhancement of thecavernous sinus or Meckel's cave. 0"I l 9 CT is more sen-sitive in the detection of bone destruction, and high-res-olution, fat-suppressed, contrast-enhanced MRI is betterfor detection of abnormal perineural enhancement.8,20Adenoid cystic carcinoma may also spread perineurallywith "skip" areas of normal-appearing intervening tis-sue.21,22 There is relatively little in the imaging literaturespecifically addressing perineural spread from thepalate.4
When a cavernous sinus mass is detected, the diag-nostic possibilities are many and include meningioma,trigeminal neuroma, granulomatous/inflammatory dis-eases, and hematogenous metastases. It is important toascertain that a cavernous sinus mass is truly limited to
42
.
b----

PALATAL ADENOID CYSTIC CARCINOMA-GINSBERG, DEMONTE
or has arisen primarily within the cavernous sinus, fornot to do so, as in the cases presented here, may haveadverse consequences. Careful radiologic and clinicalscrutiny of adjacent anatomic structures such as the or-bit, skull base foramina, and pterygopalatine fossa ismandatory. If disease is found or suspected at thesesites, the search for a head and neck primary tumor,such as palatal adenoid cystic carcinoma, should be ex-haustive. The entire head and neck region must be care-fully evaluated clinically and with dedicated imagingbecause of the possibility that tumor could have spreadperineurally to the cavernous sinus from a wide varietyof primary sites anywhere along the course of the threetrigeminal nerve divisions.
REFERENCES
1. Beckhardt RN, Weber RS, Zane R, et al: Minor salivary gland tu-mors of the palate: clinical and pathologic correlates of out-come. Laryngoscope 105:1155-1160, 1995
2. Dodd GD, Jing BS: Radiographic findings in adenoid cystic car-cinoma of the head and neck. Ann Otol Rhinol Laryngol81:591-598, 1972
3. Som PN, Brandwein M: Salivary glands. In: Som PM, CurtainHD, eds. Head and Neck Imaging. St. Louis: Mosby, 1996
4. Curtin HD, Som PM, Braun IF, Nadel L: Skull base. In: SomPM, Curtain HD, eds. Head and Neck Imaging. St. Louis:Mosby, 1996
5. Ballantyne AJ, McCarten AB, Inaez ML: The extension of can-cer of the head and neck through peripheral nerves. Am J Surg106:651-667, 1963
6. Dodd GD, Dolan PA, Ballantyne AJ, Ibanez ML, Chau P: Thedissemination of the tumors of the head and neck via the cra-nial nerves. Radiol Clin North Am 8:445-461, 1970
7. Bumpous JM, Maves MD, Gomez SM, Levy BK, Johnson F:Cavernous sinus involvement in head and neck cancer. HeadNeck 15:62-66, 1993
8. Ginsberg LE, DeMonte F, Gillenwater AM: Greater superficialpetrosal nerve: Anatomy and MR findings in perineural tumorspread. Am J Neuroradiol 17:389-393, 1996
9. Baker SR: Malignant neoplasms of the oral cavity. In: Cum-mings CW, ed. Otolaryngology-Head and Neck Surgery, 2nded, vol 2. St. Louis: Mosby, 1993
10. Curtin HD, Williams R, Johnson J: CT of perineural tumor ex-tension: pterygopalatine fossa. Am J Neuroradiol 5:731-737,1984
11. Parker GD, Harmsberger HR: Clinical-radiologic issues in peri-neural tumor spread of malignant diseases of the extracranialhead and neck. RadioGraphics 11:383-399, 1991
12. Thawley SE, O'Leary M: Malignant neoplasms of the orophar-ynx. In: Cummings CW, ed. Otolaryngology-Head and NeckSurgery, 2nd ed, vol 2. St. Louis: Mosby, 1993
13. Woodruff WW, Yeates AE, McLendon RE: Perineural tumor ex-tension to the cavernous sinus from superficial facial carci-noma: CT manifestations. Radiology 161:395-399, 1986
14. Goepfert H, Dichtel WJ, Medina JE, Lindberg RD, Luna MD:Perineural invasion in squamous cell skin carcinoma of thehead and neck. Am J Surg 148:542-547, 1984
15. Pandolfo I, Gaeta M, Blandino A, Salvi L, Longo M: MR imag-ing of perineural metastasis along the vidian nerve. J ComputAssist Tomogr 13:498-500, 1989
16. Laccourreye 0, Bely N, Guimaraes R, Halimi P, Brasnu D: Cav-ernous sinus involvement from recurrent adenoid cystic carci-noma. Ann Otol Rhinol Laryngol 103:822-825, 1994
17. Graney DO, Baker SR: Anatomy. In: Cummings CW, ed. Oto-laryngology-Head and Neck Surgery, 2nd ed, Vol 1. St. Louis:Mosby, 1993
18. Williams PL, Warwick R, Dyson M, Bannister LH: Gray'sAnatomy of the Human Body, 3th ed. New York: ChurchillLivingstone, 1989
19. Laine FJ, Braun IF, Jensen ME, Nadel L, Som PM: Perineural tu-mor extension through the foramen ovale: evaluation with MRimaging. Radiology 174:65-71, 1990
20. Barakos JA, Dillon WP, Chew WM: Orbit, skull base and phar-ynx: contrast-enhanced fat suppression MR imaging. Radiol-ogy 179:191-198, 1991
21. Lee YY, Castillo M, Nauert C: Intracranial perineural metastasisof adenoid cystic carcinoma of head and neck. J Comput As-sist Tomogr 9:219-223, 1985
22. Tang T, Lee Y: CT and MRI imaging evaluation of adenoid cys-tic carcinoma of the head and neck: Emphasis on its perineuralextension. Radiology 197(Suppl. P):173, 1995 (abstr).
43