Embed Size (px)
Citation preview

PALLIATIVE IRRADIATION OF SCOTTISH FOLD
OSTEOCHONDRODYSPLASIA
MADELEINE HUBLER, DR. MED. VET., MATHIAS VOLKERT, DR. MED. VET.,BARBARA KASER-HOTZ, PROF. DR. MED. VET., SUSI ARNOLD, PD DR. MED. VET.
This report describes palliative irradiation as treatment for Scottish Fold osteochondrodysplasia. A 3-year-old
female spayed Scottish Fold cat suffering from osteochondrodysplasia was referred to the Veterinary Teaching
Hospital, University of Zurich. Based on the breed, history, clinical signs, radiographic findings, and the
histologic diagnosis of a biopsy specimen, Scottish Fold osteochondrodysplasia was confirmed. To control the
exostoses leading to inflammatory processes and pain, radiotherapy was initiated as palliative treatment. This
was successful in relieving the clinical signs within a few weeks. The short- and long-term results after ra-
diotherapy are presented and discussed with a comparable human disease, the plantar heel spur, which also
responds well to radiotherapy. Veterinary Radiology & Ultrasound, Vol. 45, No. 6, 2004, pp 582–585.
Key words: palliative treatment, radiotherapy, Scottish Fold osteochondrodysplasia.
Introduction
SCOTTISH FOLD OSTEOCHONDRODYSPLASIA is a hereditary
disease affecting bone growth and the formation of
articular cartilage and leads to progressive skeletal de-
formities at the distal extremities and tail. Initially it was
thought to affect only cats homozygous for the folded ear
(Fd) gene, which is inherited as an autosomal dominant
trait.1 Later, several reports described similar, but less se-
vere lesions occurring in heterozygous cats (Fd/fd), but
with a later onset and varying signs of skeletal disease such
as progressive lameness, stiff and stilted gait, reluctance to
jump or sometimes without ambulatory problems.2–5 Be-
cause the underlying disease is a genetic defect, the ther-
apies in use mainly aim at reducing the clinical signs and
accompanying pain. Pentosane polysulfates subcutaneous-
ly or complex glycosaminoglycans per os were used with a
reduction in lameness and discomfort in some cats.2 In one
cat a surgical approach, including staged bilateral os-
tectomies and pantarsal arthrodeses of both hindlegs, re-
solved the lameness.3 In the latest report the same result
was achieved with only the surgical removal of the tarsal
exostoses.5 The present report describes palliative radio-
therapy in a Scottish Fold cat affected by Scottish Fold
osteochondrodysplasia.
Case History
A 3-year-old neutered female cat with folded ears was
presented to the Veterinary Teaching Hospital, University
of Zurich, for evaluation of a progressive swelling of the
left and right tarsus. The cat had a slightly stiff gait in the
hindlegs for less than 1 month before presentation and
could no longer climb trees. The mother was a Scottish
Fold and the father a Chartreux. There were three litter-
mates, one with folded and two with straight ears.
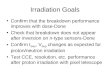
The cat was bright and alert and had grossly thickened
tarsi (Figs 1 and 2). By palpation, which caused no pain, the
right tarsus was more swollen and had a greater decrease in
range of motion. On the plantar aspect of the tarsus and
metatarsus of both hindlimbs new bone formation was
present, extending from the proximal calcaneus to the
proximal metatarsus. Along the dorsal, lateral, and medial
aspect of the tarsi no further swelling was noted. Radio-
Fig. 1. Three-year-old female spayed Scottish Fold cat at presentation.
Dr. Volkert’s current address is the private surgery of Dr. Med. Vet. G.Klaus, 4410 Liestal, Switzerland.
Address correspondence and reprint requests to Barbara Kaser-Hotz,Prof. Dr. Med. Vet., at the above address. E-mail: [email protected]
Received October 24, 2003; accepted for publication February 25, 2004.doi: 10.1111/j.1740-8261.2004.04101.x
From the Section of Small Animal Reproduction, (Hubler, Volkert,Arnold), and Section of Radiology and Radiation Oncology (Kaser-Hotz), Department of Small Animals, Faculty of Veterinary Medicine,Zurich University, Winterthurerstr. 260,8057 Zurich, Switzerland.
582

graphs were made of both distal hindlegs. On the dorsal
aspect of the right tarsus periosteal, new bone proliferations
were present, extending from the proximal os tali to the
proximal metatarsus. On the dorsal aspect of the talus and
at the intertarsal joints osteophytes were visible (Fig. 3). On
radiographs of the left tarsus there were similar, but milder
changes and on radiographs of both carpi no degenerative
changes were present. A biopsy taken from the bony pro-
liferation by the referring veterinarian was submitted for
histopathologic examination; results were compatible with
osteochondrodysplasia. The breed of the cat, history, clin-
ical signs, and radiographic findings were consistent with
the histological diagnosis of osteochondrodysplasia.
To decrease the new bone formation, which eventually
will lead to reactive inflammation and progressive ankylos-
ing arthropathy, radiotherapy was initiated as a palliative
treatment. Over 2 weeks the cat was irradiated in six frac-
tions of 1.5Gy each, on a Monday–Wednesday–Friday
schedule. The radiation used was 30-MeV electrons. The
radiation source was a Betatron.� For radiotherapy, the cat
was anesthetized with intravenously injected propofolw (in-
duction dose: 7mg/kg, maintenance: 0.5mg/kg/min). The
cat was positioned on its back with both hindlegs positioned
in the air and fixed to a rack. The irradiated field included
the whole tarsal area of both hindlegs and extended from
the tibia to the distal ends of the metatarsi. A single beam
was directed in a plantaro-dorsal direction and both tarsi
were irradiated in the same field. The Dmax was 100% at 1-
mm depth and no bolus was used. The entire depth and
circumference of both tarsi received 100% of the dose.
After six radiotherapy sessions the cat had no side effects
and went home in a good condition. The referring veterin-
arian re-examined the cat at regular intervals over the next
2 years and according to the owner the cat had no ambu-
latory problems and was now able to climb trees 1 month
after completion of radiotherapy. Twenty-eight months af-
ter therapy radiographs were repeated. On both hindlegs
there were no signs of further bone proliferation. The ex-
ostoses had strikingly smooth surfaces and a less opaque,
but more homogenous, structure. The talocrural joint
space of the more severely affected right hind limb was
narrowed and the proximal intertarsal joint was almost
completely fused. At the distal intertarsal and tarsometa-
tarsal joints ankylosis was almost complete with no effect
on the cat’s locomotion. Additionally, within the previous
Fig. 2. Right hindleg with pronounced swelling on the plantar aspect ofthe tarsus and metatarsus.
Fig. 3. Radiograph of the right tarsus (medio-lateral view) before radi-ation therapy.
�BBC, Switzerland.wDisoprivan, Fresenius Pharma (Schweiz) AG, 6370 Stans,
Switzerland (induction dose: 7mg/kg, maintenance: 0.5mg/kg/min).
583RadiationTherapy in a Scottish Fold CatVol. 45, No. 6

radiation treatment field a few new bony proliferations
were evident at the proximal plantar end of the metatarsal
bones (Fig. 4). On radiographs of the left leg there was only
minor new bone formation at the tarsal joint. The joint
spaces were still intact and without apparent changes.
Discussion
The trait for forward folded ears (Fd) originated as a
spontaneous mutation, in 1966, in a female British short-
hair, the founding cat of the Scottish Fold breed.1 Genetic
studies using breeding experiments revealed an autosomal
dominant inheritance.1 Additionally, it became evident
that cats homozygous for the gene (Fd/Fd) developed a
progressive skeletal disease, including a short thickened
and inflexible tail and deformities of the distal extremities
early in their lives. At the age of 7 weeks radiographic
changes are already apparent: there are distorted met-
aphyses and widened physes of the metacarpal and met-
atarsal bones. Similar but milder changes are seen at the
phalanges. This results in a reduced growth of the affected
bones, leading to shortened extremities and short, thick-
ened vertebrae of the tail with widened endplates.1 Histo-
logically the pathological changes of the affected bones are
mainly located at the growth plates and the neighboring
metaphyses. The growth plates have defective bone for-
mation with disordered chondroblast proliferation and ir-
regular groups of cells, which finally results in a disturbed
enchondral ossification with insufficient mineralization.
During growth the extremities become deformed and the
affected joints are abnormally stressed, resulting in degen-
erative joint diseases and periarticular new bone formation
at sites of ligamentous attachment to bone and joint cap-
sules.2 The extensive investigation of Scottish fold cats, in-
cluding pedigree analysis2 demonstrated clearly that not
only the homozygous, but also the heterozygous carriers
are affected to some degree by this osteochondrodysplasia.
The therapeutic approach in cats with clinical signs is solely
aimed at reducing the impaired locomotion and the ac-
companying pain. The use of pentosan and glyco-
saminoglycan preparations only helps in some cats2 and
surgical therapies3,5 indeed resolved the lameness, but they
are rather invasive procedures. It was therefore decided in
the presented cat to use a minimal invasive treatment, ra-
diotherapy, to stop the excessive bone formation and to
suppress the inflammatory process.
For this cat a low dose regimen of six fractions (1.5Gy)
was chosen. This fractionation schedule was arbitrarily
based on information for plantar heel spur radiation in
human medicine6–8 and was purely palliative with the aim
to stabilize the skeletal changes. The underlying problem
itself is incurable. In addition, we wanted to spare the
normal tissue. The achieved result, namely the suppression
of bony proliferation, and therefore a pronounced slowing
down of the osteochondrodysplasia, is promising, espe-
cially when compared with the more invasive surgical
methods.3,5 There was no posttreatment necessary and
long-term success was good. On radiographs made 28
months after radiotherapy there was just a minimal in-
crease of the exostoses.
A comparable and well-known disease in humans is the
plantar heel spur, an original disease of the ‘‘Calcaneodynie
syndrome,’’ which irritates the whole osseous and tend-
inous system of the heel in its function. Because the etio-
logy of the plantar heel spur is still controversial, the aim of
treatment is primarily to eliminate the accompanying irri-
tations.8 Beside local and systemical medical treatment
with antiphlogistic and analgetic substances, physical ther-
apy and inner soles are the preferred therapeutic approach-
es for the plantar heel spur. It is often refractory to medical
therapy, but has responded well to radiotherapy which is
well established in European countries.6–8 The primary
goal of radiotherapy in affected people is the control of
inflammation, which is responsible for the subjective pain
of the patient. In one prospective study8 three different
dose concepts were compared with a variable number of
fractions and different total radiation dose. Group A
(n¼ 72 heels) received 12-Gy total radiation in three frac-
tions per week and two series (6� 1Gy/series) separated
by 6 weeks; group B (n¼ 98 heels) received 3-Gy total ra-
diation in ten fractions of 0.3 -Gy (n¼ 50) or 5Gy
(10� 0.5Gy) (n¼ 48) with conventional fractionations in
one series. At the end of therapy 75% of group A and 77%
of group B had a subjective pain relief of 80–100%. A
delayed response after 4 weeks or subjective pain relief of
less than 80% was observed in 25% (group A) and 24%
(group B), respectively. On long-term evaluation complete
pain relief was achieved in 67% (group A) to 71% (group
B) of the treated patients, with no significant difference
between the three radiation protocols. However, prognos-
Fig. 4. Radiograph of the right tarsus (medio-lateral view) 28 monthsafter radiation therapy.
584 Hubler et al. 2004

tic factors for complete pain relief were short duration of
pain symptoms prior to therapy and acute pain symptoms
prior to radiotherapy.
The clinical presentation of the Scottish Fold osteo-
chondrodysplasia and the onset of clinical signs in our cat,
as well as the good response to radiotherapy, are somewhat
similar to the human heel spur problem.6–8 Because os-
teochondrodysplasia results in degenerative joint disease and
periarticular new bone formation leading to inflammatory
processes, it explains the good response to radiotherapy in
our cat. Therefore, the palliative radiotherapy offered an ef-
fective and minimally invasive treatment for this Scottish
Fold osteochondrodysplasia, if the degree of the skeletal
changes, including degenerative joint diseases, is not too ad-
vanced. Because in cats heterozygous for the folded ear (Fd)
gene, the age at onset of clinical signs (6 months–6 years), as
well as the severity of changes and rate of progression, is
considerably variable, palliative radiotherapy should be eval-
uated individually for each case. When the skeletal changes
are not too advanced, and there is a good clinical response to
radiotherapy, a second irradiation could be considered if
clinical signs reoccur. Although the result of palliative radi-
otherapy was quite promising in this Scottish Fold cat, the
maintenance of this breed should be discouraged2 as cats
heterozygous for the folded ear gene are also affected by this
osteochondrodysplasia sometime during their lifetime.
REFERENCES
1. Jackson OF. Congenital bone lesions in cats with fold-ears. Bull FelAdvis Bur 1975;14:2–4.
2. Malik R, Allan GS, Howlett CR, et al. Osteochondrodysplasia inScottish Fold cats. Aust Vet J 1999;77:85–92.
3. Mathews KG, Koblik PD, Knoeckel MJ, Pool RR, Fyfe JC. Res-olution of lameness associated with Scottish Fold osteodystrophy followingbilateral ostectomies and pantarsal arthrodeses: a case report. J Am AnimHosp Assoc 1995;31:280–288.
4. Partington BP, Williams JF, Pechman RD, Beach RT. What is yourdiagnosis? Scottish Fold osteodystrophy. J Am Vet Med Assoc1996;209:1235–1236.
5. Simon D. Osteochondrodysplasie bei einer Scottish-Fold Katze.Tierarztl Prax 2000;28:107–110.
6. Basche ST, Drescher W, Mohr K. Ergebnisse der Rontgenstrahlen-therapie bei Fersensporn. Radiobiol Radiother 1980;21:233–236.
7. Schafer U, Micke O, Glashorster M, Rube C, Prott F-J, Willich N.Strahlentherapeutische Behandlung des schmerzhaften Fersenbeinsporns.Strahlenther Onkol 1995;171:202–206.
8. Seegenschmiedt MH, Keilholz L, Stecken A, Katalinic A, Sauer R.Radiotherapie beim plantaren Fersensporn. Indikation, Technik, klinischeErgebnisse bei unterschiedlichen Dosiskonzepten. Strahlenther Onkol1996;172:376–383.
585RadiationTherapy in a Scottish Fold CatVol. 45, No. 6