Embed Size (px)
Citation preview

In this issue
From the ChairIn this edition of PalliativeProfileSA, we have tried to shine a spotlight on palliative care in the community. And that raises the question, what exactly is the community?
In the language of today’s health system, ‘community’ has come to mean all the sites of healthcare delivery that are outside the walls of our hospitals, except of course when the walls are temporarily removed to deliver ‘hospital in the home’. And this seems to me to create a very narrow view of the true meaning, or possible meanings of ‘community’.
The Shorter Oxford English Dictionary on historical principles, 1973, begins with 16th century meanings of ‘community’ which include common ownership, common liability and later common character, agreement, or identity. In the 18th century there is a shift to a broader concept of a body of people organised into a political, municipal and social unity, or a body of persons living together and practising communities of good.
If we try to look at what a community is in our vast, mobile, contemporary society, our ‘global village’, it is clear that there are many types of community
– geographic, professional, religious, other shared common interests such as the arts or sport and, for others, the shared common heritage of family. We could even include the new community of social media. And it is equally clear that there is great variation in how well these communities function in the face of terminal illness in one of their members.
Geography, proximity or distance, can mean many things to community. Living as so many of us do in suburban isolation, I have recently had the contrasting and enriching experience of seeing a country town and the widespread surrounding district, as a community, rally to support one of its members through terminal lung cancer. Just friends, yes, golfing buddies, yes, but in the gaps when family could not be there, they became family.
Palliative care rhetoric has been very much focused on ‘building community capacity’. If this comes from a position of building resilience in people in the face of the uncertainty and loss that comes with the death of someone we love, then this must be a good thing. But if it is simply code for inadequately funding community services to provide sufficient palliative care expertise to support care at home, then it is to be questioned.
An opportunity to talk about the Silver Chain model of care in Western Australia with Chief Operating Officer (Silver Chain Group), Stephen Carmody, revealed just how community capacity can be built. The provision of a comprehensive network of care, with 24 hour availability, has resulted in a greater than 60% home death rate for palliative care patients. McNamara and Rosenwax found in a 2007 study in WA that ‘people who accessed community-based specialist palliative care had a seven times higher chance of dying in their usual place of residence’1. But more than that, WA data on hospital and emergency department use by people with diagnoses for whom death was an expected or ‘predictable’ outcome revealed an average of 7.8 admissions in
the last year of life, most occurring in the last 3-4 months of life2, which compares with those people under the care of Silver Chain having on average only 1.2 admissions to hospital during their entire episode of care (approximately 80 days). And more than that again, the experience of family and carers is that ‘we did it, we took care of him/her’.
In the belief that building resilience must start early in life, and remembering that I had already attended too many funerals at my children’s school, I spent some time talking with Luke Thomson, Principal of Pembroke School, about the school as community and dealing with death. His view is that a school is a complex community, made up of all the many people engaged in the life of the school, students, teachers, parents, and the relationships involved are themselves complex and challenging.
Death, when it directly affects someone in the school community, inevitably connects the school to others in a much broader community – a wider circle of family, friends, colleagues. And the support generated within the school is able to reach outside the school to encompass others.
The position of school chaplain is a key one; an instant focus for practical things, as well as spiritual - school and family kept in constant dialogue. ‘The school is at their service’. Through the chaplain, information provided is clear and a consistent language around death and dying has developed, including suitable words for public statements.
• cont page 3
PalliativeProfile SAIssue 58 April, 2013
A Proud day 2
A Hat Trick of Thanks 2
Syringe drivers and
community care 3
CEO’s message 4
Di Roughton Community RN 5
A Palliative Care Emergency 6
Palliative care- everyone’s
business 7
Telehealth 8
Close the Gap Day 9
Behind the scenes – PCOC
and more 10
Calling for an indigenous artist 11
Conferences and coming events 12
Support from companies, corporations, foundations and philanthropic trusts who believe in our mission are integral to our success and it gives me much pleasure in thanking Rem Systems Pty Ltd who are supporting the 2013 annual palliative care forum series for the second year running. Founded in 1981 in Auckland NZ, Rem Systems is a privately owned distributor of high quality medical devices including the well known NIKI T34 syringe driver. Their customer base is wide ranging across many specialities, including veterinary practices but as a result of the NIKI T34’s success, organisations and facilities delivering Palliative Care have become one of their most important customers. “Supporting Palliative Care education and training makes perfect sense to us.” says REM Group Product Manager, (Medical) Ross Hardy. “It is an ideal partnership and link to our company motto, Caring For Lives”.
You can find the program and register online for the 2013 Autumn and Spring forum series at www.pallcare.asn.au There are no costs to attend courtesy of the generous support of REM Systems. Don’t be disappointed, visit the website today.
We also thank National Palliative Care Week Partner for 2013, Alfred James & Sons Pty Ltd Funeral Directors whose support will help us reach as many people as possible during this week long campaign. Established in 1922 by Alfred James, the company is now a 3rd generation South Australian family business whose originating principles of kindness and deep understanding for those who have suffered the loss of someone they loved are still reflected in the business today.
Making the hat trick, it also gives me pleasure to thank Australian Hotel Association South Australia (AHA SA) for funding used to purchase our first vehicle. In any society, the response to health and illness is shaped by cultural traits, values and rules and they are learned
A Hat Trick of Thanks
through participation in that society. In Australia, there are significant cultural differences in the way disease and death are dealt with and understood by the dominant Anglo-Australian society and by Aboriginal peoples. The implications of such cultural differences are particularly poignant during the dying trajectory. In order to address this hiatus, Palliative Care Council South Australia has committed to the establishment of an Aboriginal Palliative Care Program. Core aspects of the program is the building and maintaining of relationships, respect for cultural difference and creating opportunities for Aboriginal people. We are confident these actions will have a significant effect and help us to bring about the changes that are required if we are to succeed in our aim of ensuring services are understood, are culturally safe and accessible.
Just as poor quality care can have a profound and lasting impact on those left behind, the effect of high quality end of life care can ripple across generations. The Australian Hotel Association (SA Branch) on behalf of the South Australian Hotel Industry has provided support by way of funding to purchase a vehicle in order to travel to communities is instrumental in enabling us to address the apprehension and fear about illness, dying, death and grief across contemporary Aboriginal communities.
It was a proud day for South Australia and indeed for Palliative Care when Emeritus Professor Ian Maddocks, who was elected first President of the Australian Association for Hospice and Palliative Care (now Palliative Care Australia) accepted the Award for 2013 Senior Australian of the Year.
The award was announced by Prime Minister Julia Gillard on Australia Day.
In his address Professor Maddocks said people who were near death were formerly isolated by regimes of hospital care. He said while care of the dying had come a long way in recent decades to include the positive involvement of the family and increased levels of care at home, more resources need to be devoted to palliative care to ensure that such services are available to all.
Professor Maddocks was appointed as Professor of Palliative Care in 1988, after promoting the development of palliative care treatment and services in southern Adelaide for some years.
Recognised also for his work in tropical and preventative medicine, his texts are used internationally, and he has received a number of international awards for his work.
A Proud Day for Palliative Care
Palliative Care Council is on the move ...
April 2013Page 2

Page 3April 2013
From the Chair • cont from page 1
Making a donation to the Palliative Care Council just got easier. You can donate directly using the following link www.givenow.com.au palliativecaresa
There is recognition that all families cope differently and an important acknowledgement of the power of words, or of no words.
But what of the students? And what of resilience? A programme to build a healthy but realistic appreciation of the world around them is underway. Bad stuff happens, but it may not be as bad as you think. Ups and downs are natural, happiness should be grasped and it may be fleeting. Expression of emotion is supported; Luke described boys (and girls) crying openly, talking, supporting one another. At another time, following the sudden death of a much loved young staff member, boys wrote letters and poems to express their feelings and love for him. And at the end of a very difficult year for that school community, exam results were better than they had ever been before. I think that is what we mean by resilience.
So when we talk about ‘care in the community’ we need to think beyond the ‘outside hospital walls’ paradigm. We need to truly understand all the many meanings and contexts, weaknesses and capacities that are encompassed in our different communities. And yes, we need to celebrate and honour their strengths, but fully support their vulnerabilities, and help build resilience to survive and perhaps to grow, in the face of death.
Dr Mary Brooksbank AM
References:
1 McNamara B &Rosenwax L; Factors affecting place of death in Western Australia. Health & Place 13 (2007) 356-367.
2 Rosenwax L et al; Hospital and emergency department use in the last year of life: a baseline for future modifications to end-of-life care. MJA Vol 194, 11, 570-573.
Syringe Drivers and their impact on community palliative care?
Patients receiving palliative care are often transferred between hospital and community settings. Until the advent of the syringe driver, pain control was problematic outside of hospital/hospice settings. Historically, pain was relieved through administration of intramuscular or intravenous injections at timed intervals when patients became unable to take oral analgesia. Because of the short duration of action of most opioids, injections needed to be repeated at regular intervals with obvious drawbacks; injections became painful and the procedure was time-consuming and often difficult to maintain in the community.
The introduction of syringe drivers revolutionised pain control with added benefits for the patient and professionals. Continuous infusions helped maintain constant blood serum opioid levels providing improved pain relief. Many practitioners agree that syringe drivers facilitate patient independence in terms of the syringe driver being compact (Lee, 2006), and inconspicuous (Shaw and Meek, 2007), as well as negating the need for regular injections or suppositories which are deemed uncomfortable and inconvenient.
But do patients and families embrace the syringe driver with the same enthusiasm? Evidence of their use in end of life or palliative care has lead to patients and families regarding syringe drivers as an indicator of ‘near death’ and a consequent reluctance for their use (Copperfield, 1996). Blogs like the following found on many health sites indicate this stigma is still evident today.
“We were told that she would probably not last 2 weeks. She died at home 6 days after being admitted to hospital (3 days after coming home) and 36 hours after palliative care connected her to morphine pump. I feel
guilty for allowing Mum to be connected to a morphine pump. I am angry because I didn’t really understand what was happening”.
Even more alarming is that some professionals also wrongly associate the use of a syringe driver with imminent death (Dickman et al, 2005).
Given this misconception about syringe drivers, careful explanation to both patient and family about the reason for using a syringe driver is therefore important and although syringe drivers continue to be popular within palliative care settings (Graham and Clark, 2005), human error remains as a problem and there is, and needs to continue to be, education and training to help practitioners use these devices effectively.
In meeting this need, REM Systems Pty Ltd have developed a new DVD in-service training resource and will be making it freely available. The DVD is broken down into chapters and is presented as an in-service would be conducted. The DVD is going through a final Quality Assurance process, and when it is available REM Systems Pty Ltd will distribute it freely to anyone interested. Additionally websites including pallcare.asn.au will make the in-service power point presentation available for download.
Tracey Watters CEO PCCSA
Additional References
http://www.pharmacytoday.co.nz/resources/palliative-care/syringe-driver-use-in-palliative-care.aspx
The benefits and drawbacks of syringe drivers in palliative care (John Costello, Brian Nyatanga, Carole Mula, Jenny Hull) International Journal of Palliative Nursing, 2008 Vol 14, No. 3

Page 4
Chief Executive Officer’s Message
Welcome to 2013, and the year of the federal election. With the announcement that we are heading to the polls on 14 September the political parties are well and truly in election mode. PCCSA along with Palliative Care Australia and the other state and territory member organisations have identified the priorities for palliative care and submitted them in response to a call from the Federal Treasury, in the hope that it will deliver the best results for not only our collective membership but also those carers of some 140,000 patients who will die an expected death this year. In this election year should we remind ourselves of the power of the people? This makes for a lot of voters.
This PalliativeProfileSA edition focuses our attention on ‘community’ and the Federal Budget submission very clearly articulated our collective sentiment: community Palliative Care does not equate to reduced need or a less deserving response. If Governments believe community palliative care to be the golden key in addressing burgeoning demand it requires a different response and in doing so requires they invest differently.
What does it take to deliver great palliative care in the bed in which consumer’s choose to die? Are the essential elements of specialist palliative care truly available to all Australians at the end of life or does the current funding framework favour competitive sector behaviour?
More palliative care will ultimately fall into the realm of the generalist as we embrace the concept of palliative care being offered to not only those receiving palliative treatment for cancer, but also palliation of the non-malignant diseases and the fact that most people are living longer due to progress in medical management. Primary Care therefore is where the majority of longer term palliative care will be, outside hospital walls.
We know those who experience care in any one of our South Australian hospices are usually very, very satisfied with the care they and their loved one receive. It was only today when I purchased PCCSA’s first vehicle courtesy of funding provided to us by AHA SA Hotel Care, that I was reminded of an all too persistent comment by bereaved relatives..... “I wish I had known about palliative care sooner. Not only was [Pete] cared for so well, but they took care of me too!”
The challenge to current stakeholders is to
make the same level of care, compassion, technical brilliance and individual expertise available outside the walls of the LHN facilities whilst keeping specialist palliative care in the leadership role.
I don’t believe it is rocket science but it does require people to work differently. We must start to build service growth around the consumer, not those delivering the services. Community palliative care is a tapestry woven from countless threads. It requires that specialist palliative care be more than just consultants to meet the needs of patients and families in their communities. There also must be strong links with GPs who form part of the team and who are adequately remunerated for their care.
PCCSA’s role in this challenge is to create the space for networking between consumers and the sector. There is never better opportunity than in an election year to engage with and turn into ambassadors those surviving relatives for whom the application of palliative care served them and their loved one well.
This year PCCSA’s strategic objectives are to consolidate upon the gains made in the past two years; incremental as opposed to transformational.
Advocacy
Last year PCCSA successfully advocated members and interested South Australian stakeholder concerns in Canberra through the Senate Inquiry into Palliative Care in Australia. Election year provides us the opportunity to clearly articulate why future investment in palliative care must be targeted to ensure true connectedness between specialist and generalist palliative care.
This year we partner with REM Systems Pty Ltd again to present internationally and nationally recognised speakers and leaders. The Hawke Institute Palliative Care Lecture this year will be delivered by Professor Roderick Macleod who will touch on the subject of health promoting palliative care. We kicked off the year’s Autumn Forum series in February with the ‘Letting Go’ forum and you can see a full list of topics planned for the rest of the year in ‘coming events’ later in this edition.
To mark World Hospice and Palliative Care Day in October, the Adelaide Symphony Orchestra has generously donated their concert A Night in Vienna to the cause and we will be providing more information soon about how you can support this event.
Given the growing use of social media by ‘community’, PCCSA is working with a consultant on two levels; to develop social media and mobile strategies to help raise awareness of our work and palliative care generally and to encourage donations and financial support for PCCSA programs. We will also look to present a forum about Social Media – its meaning for the palliative care sector, protection for health care professionals, policies regarding non engagement of staff with patients and the issue of virtual friends.
Progressing our Strategy
We will continue to work towards the successful completion of priority goals including:-
• Biculturalgovernanceandachievementof PCCSA ‘s Reconciliation Action Plan
• Productionofthreehighqualityeditionsof PalliativeProfileSA (the newsletter of the South Australian Palliative Care sector)
• AmorevisibleNationalPalliativeCareWeek campaign
• Continueddisseminationofinformationand resources
• Wewillcontinuetoassistcallersseekinginformation about access, direct contact information and processes for referral and resources.
Our goals and objectives remain the same: raising awareness and understanding of palliative care in the public; increasing the understanding of what palliative care can offer; advocating to the Government for improved services; and building relationships to provide a platform for networking in palliative care.
You will soon start seeing a number of activities in the media to help us get the message across to politicians and decision makers. Members will also be kept up-to-date through future editions of PalliativeProfileSA, our website and through social media.
Tracey WattersChief Executive Officer
April 2013

page 5
I was a little early when I first arrived at RDNS Mawson Lakes to interview Community Palliative Care RN Di Roughton or Dianne as she now introduces herself…I will tell you about that a bit later. Having never been there before I took a stroll up the Main Street returning to see Di at the corner with the day’s diary and associated papers, notes and reminders under one arm and the mobile device to her ear. In the time she walked the 300 metres from the corner to the office door, two patients had called and she and a colleague on the way out the door shared a quick exchange of information. She had not even made it in the door yet.
Having attended quickly to the early enquiries, Di and I settled down with a coffee to talk about her career of over 26 years as a community nurse, the last 16 as a community palliative care nurse. I wanted to ask her about how and why nurses enter the world of palliative care and what a typical day at work involves. What is the essence of being a community RN, what are the challenges and how it has changed in her 26 years and importantly what she draws on when the going gets tough.
Well, first of all she said, for almost all the 26 years I have been known as Di Roughton, community nurse and it was only just a short while ago, after a patient I visited for the first time since stopping active treatment, opened the door and said despondently, “well, that’s appropriate isn’t it” looking at my name badge. Until then, although it had occurred to me, no one had said it. “I guess this kind of reflects the essence you asked about”, says Di. “It’s about honesty and trust”.
“When I started working for RDNS I was a ‘round nurse’. I enjoyed the palliative care visits and applied for the next palliative care specific position, progressing from there with post graduate study. RDNS Palliative Care is hands-on, nurse-led specialist palliative care. Notwithstanding the increasing complexity and acuity of patients who are dying, RDNS palliative care nurses deliver (care)to exacting and multiple standards. The role of the RDNS Palliative Care nurse is also to support, advise and educate ‘round nurses’ in the principles of palliative care. Given their very big role in caring for the chronic illness population, this will be an
important strategy in meeting burgeoning demand”.
A typical day in the life of an RDNS Palliative Care nurse involves making scheduled visits to patients living with the sometimes difficult symptoms associated with dying. It means being responsible for receiving and admitting new patients to RDNS care. This usually requires a visit and a full and comprehensive assessment of the physical, social, and emotional aspects of the situation and preparation and agreement of a care plan with identified goals of care. Additionally the family or persons caring for the patient at home are canvassed in terms of their need for support. Obviously liaising back and forth with ‘round nurses’, and problem solving with GPs and others involved in the patient’s care are also important aspects of the role.
Although unsure that hospital avoidance budget measures should be the impetus for developing community care, community care now involves more complex clinical procedures at home, like blood transfusions, pleural and ascites drain management and intrathecal pumps; all this has strengthened the ability and confidence of communities to care for a dying relative at home and simultaneously raised the bar in terms of the clinical knowledge and skill required. “It really is the simultaneous application of evidence based knowledge and skill delivered with compassion and empathy that is the essence of the community palliative care nurse” Di replies to my question. “By that I mean the ability to put patients and their families at ease so they are comfortable to discuss very difficult and sometimes confronting issues at an emotional time”.
I ask Di about just that, the emotion of palliative care and being constantly exposed to it. What do you draw on when the going gets tough I ask?
Although part of the learning process and not something you immediately understand, requirements of the job include emotional stability, in other words the ability to be able to deal with anything, without surprise or angst. Time for debriefing is essential in the bigger scheme of things. “If you don’t you will end up burying yourself in it. The RDNS team at Mawson Lakes is quite widespread but we make an effort to keep
in touch and meet regularly to debrief and discuss concerns and provide support”.
I ask Di what is your approach, how do you go about this business of death and dying? “I try to be very open, discuss the issues, options and choices that are available for people facing this situation. I am positive about the need for advance directives and encourage discussions with families to put measures in place well before they are needed. I am definitely an advocate for home care if it can be managed. My experience tells me the person who is dying and the family has a better environment and overall outcome if they can manage at home”.
Is Palliative Care health promoting? “Given most of my clients are terminal it is difficult to quantify what health promotion might look like with them, but because we are in the community, because we are out there doing it, we are becoming more recognised as being able to do so. I really think over recent years dying at home has become more accepted. As a general rule I think people are more open to palliative care and have a better understanding of what it involves than say 10 years ago, but many are still very reserved”.
In bringing our talk to an end, I asked Di about the state of palliative care, and if she felt there were changes that should be made? “Oh, that’s far too political a question for me to answer,” and we laughed a little. “Some families will always need intensive care and support while other families manage with less”.
In 2012, RDNS support enabled 1660 patients with a terminal illness to be cared for and die in their own homes.
Tracey Watters Interviewer/Author
Di Roughton Community RN
April 2013

Page 6
A Palliative Care Emergency
Traditionally, we have thought about emergency medical care and palliative care as two separate silos in our very complex health system. Palliative care is all about the quality of remaining life whereas the emergency medical response is focused on prevention of death and morbidity.
A patient in a palliative care setting can still have an emergency and need urgent and skilful treatment. The emergency may be a breakthrough pain issue; it may be a new and worrying symptom or a dramatic and confronting complication. Inevitably the emergency is going to have many complex facets including the psychological state of the patient, their family and carers and the ability of the system to support them.
A truly patient centred approach to care will not respect traditional medical silos but is focused on an immediate and urgent need of a patient for management in the broadest sense and support in the broadest sense.
Recently, palliative care services have evolved a relationship with extended care paramedics working for the ambulance service. The extended care paramedics are there to provide care to complex patients who may need quite involved intervention. The aim is to provide the patient with the necessary care in their own surroundings and on their own terms if it is safe and appropriate to do so.
Extended care paramedics have been created to meet a need for more extensive patient care in the community in an emergency without necessarily resorting to hospitalisation. In South Australia, the extended care paramedic program is staffed by very senior intensive care paramedics who have considerable clinical experience of emergency medical response over a number of years and a comprehensive understanding of complex emergency clinical care in the community. These extended care paramedics routinely form the acute part of a health team that may be centred upon a general practitioner and involve residential care staff and of course the patient and their family. The mode of operation is completely different from traditional rapid response, lifesaving treatment and transport that characterises emergency paramedic care.
Amongst the complex patients cared for by extended care paramedics in the 2009 pilot were a group of patients with palliative care emergencies. A true team relationship between these ambulance paramedics and palliative care staff quickly evolved. This role has now been formally studied with independent evaluation of feedback from both patients and carers on their experiences. The results have been extremely positive with the vast majority of patients and carers being extremely satisfied with the skill and attitude displayed. This positive result is a reflection not only on one isolated component, but of the health care team working together to deliver patient focused integrated care.
Currently extended care paramedics attend cases from the large number of emergency 000 calls. The extended care paramedics are attending those patients who have already decided to call 000, therefore they are not diverting patients from already existing functional care streams.
In the past a patient with an emergency in a palliative care setting who called 000, would be transported to a busy Emergency Department. They might receive further analgesia en route but there was no scope for the paramedic to substantially alter the patient’s symptoms or condition. In the Emergency Department they would be seen by a caring team who unfortunately were not the palliative care team and were not involved in this patient’s ongoing care. Most of the significant changes to management plans and future planning would occur as an inpatient and then arrangements would have to be made to support that care in the patient’s own environment before they could be discharged.
Now, the same patient can be assessed in their own home. A management plan discussed between the paramedics and the palliative care team can be implemented. Any further blood tests can be carried out in the home and an ongoing plan for follow-up can be created at the time. If necessary the extended care paramedic can remain with the patient to assess the effects of the new treatment plan and an opportunity to adjust it again with further consultation exists. From the point of view of the patient, this is so much better. From the point of view of
the health system this is so much more efficient.
The very positive results seen in the group of palliative care patients that were managed by a palliative care/paramedic collaboration points the way towards a future model that is truly patient focused and not governed by historical health silos. Nurse practitioners and extended care paramedics are both stepping up to meet the patient’s needs. By forming multidisciplinary teams focused on managing not only a patient’s acute emergency, but also their ongoing care we have the potential to meet more and more of the patient’s needs. Most patients in a palliative care situation would prefer to be managed in their own environment. We can improve their management by forming different and unusual alliances involving not only general practitioners and palliative care teams but also including community-based advanced practitioners, allied health practitioners, nurse practitioners and extended care paramedics.
There are benefits in using existing systems with established infrastructure and depth of resources to form multidisciplinary teams. When we consider the overall benefit of these teams, we need to measure the impact on the patient and the whole of health rather than within small, isolated financial silos.
Like all good ideas, once suggested it seems so obvious that one wonders why it wasn’t done before. The current state of evolution of the extended care paramedic and the nurse practitioner seem to be on convergent paths, but only represent a stage in the evolution of what will be a truly patient centred care process. The challenge will be letting go of our current concepts of how care should be provided so that different models can evolve. We already have evidence that the patient at the centre of our model is happy and satisfied with their care. The patient is after all the ultimate expert in this system.
Hugh Grantham ASMProfessor of Paramedics, Flinders UniversitySenior Medical Practitioner, SAAS
April 2013

Page 7
Every year during the last week of May we actively promote the concepts and philosophies of palliative care and the services and options available to people dealing with advanced terminal illness. Our objective is to equip both the broader community and all health care providers with the knowledge and information they need in order to make a positive difference in the lives of people who are dying, people caring for someone at the end of life, or people coping with loss and grief.
In 2013 the theme is ‘Palliative Care – everyone’s business’, which was chosen to encourage everybody to consider their part in end of life care, and to talk about their preferences when it comes to dying.
Dr Mary Brooksbank, Chair of Palliative Care Council South Australia, said “Palliative care is about living and dying well and supporting not only the individual, but also their families and carers. It’s important that everyone knows what care and support is available, and how they can receive it, so that we can ensure all Australians receive quality care at the end of their lives.”
National Palliative Care Week will be held from 19th to 25th May 2013 and the official launch breakfast will be in Canberra on May 16th with Senior Australian of the Year Emeritus Professor Ian Maddocks.
April 2013
May 19th to 26th is National Palliative Care Week and 2013 is the year that we promote Palliative Care as everyone’s business.
Death, dying and loss, like the matter of good health and maintenance, is everyone’s responsibility. For those people where prevention, early detection, and treatments fail, caring becomes as important as curing and we encourage you to host a Time to Remember event to help make palliative care everyone’s business.
Time to Remember offers an opportunity to gather with friends, family, colleagues
or team mates to remember special people who have died and support your local Hospice or Palliative Care Service. Log onto www.timetoremember.org.au and download the Host’s Guide to holding a successful Time to Remember. It has a planning list, invitations and ideas that will help to take the hard work out of it. So please consider becoming a Time to Remember 2013 Host and help terminally ill people and their families. You only have to visit a hospice or speak to someone with a hospice connection to see the impact this specialist care has on patients, their families and friends.
Palliative Care Australia and Palliative Care ACT invite you to attend the 12th Australian Palliative Care Conference from Tuesday 3rd to Friday 6th September 2013 in Canberra.
Palliative Care – everyoneʼs business will bring together over 700 delegates from across Australia and the world to explore the importance of palliative care in all its dimensions. Clinicians, researchers, volunteers, allied health practitioners, educators, carers and all those who have a passion for palliative care will share best practice, hear the latest research, be challenged by keynote speakers and build valuable networks.
Thereʼs no better time to visit Canberra.
2013 marks the centenary of Australiaʼs national capital and there are many fantastic events and activities planned that you can experience. Centenary celebrations will include the Centenary Gala Ball on Thursday 5th September in the Great Hall at Parliament House.
Key note speakers have been announced. Donʼt miss this opportunity to hear Professor Eric Cassell, Associate Professor Amy Chow (University of Hong Kong) and Professor Irene Higginson.
12TH AUSTRALIAN PALLIATIVE CARE CONFERENCE 3RD -‐ 6TH SEPTEMBER 2013 CANBERRA AUSTRALIA KEY NOTE SPEAKERS PROFESSOR ERIC CASSELL A/PROFESSOR AMY CHOW PROFESSOR IRENE HIGGINSON
12th Australian Palliative Care Conference 3rd-6th Septemer 2-13
Palliative Care Australia and Palliative Care ACT invite you to attend the 12th Australian Palliative Care Conference from Tuesday 3rd to Friday 6th September 2013 in Canberra.
Palliative Care – everyone’s business will bring together over 700 delegates from across Australia and the world to explore the importance of palliative care in all its dimensions. Clinicians, researchers, volunteers, allied health practitioners, educators, carers and all those who have a passion for palliative care will share best practice, hear the latest research, be challenged by keynote speakers and build valuable networks.
There’s no better time to visit Canberra. 2013 marks the centenary of Australia’s national capital and there are many fantastic events and activities planned that you can experience. Centenary celebrations will include the Centenary Gala Ball on Thursday 5th September in the Great Hall at Parliament House. Key note speakers have been announced. Don’t miss this opportunity to hear Professor Eric Cassell, Associate Professor Amy Chow (University of Hong Kong) and Professor Irene Higginson.
Watch PCCSA weekly bulletin for news of local venues to participate and how to order your National Palliative Care Week collateral. There will be pens, posters, and new items to help you celebrate and spread the word, palliative care is everyone’s business. A tribute wall is also being developed and more information will be available soon.
We are very grateful to Alfred James and Sons Pty Ltd Funeral Directors for providing sponsorship to ensure we reach as many people as possible during this week.
Professor Eric Cassell
Associate Professor
Amy Chow
Professor Irene
Higginson

Page 8
Telehealth - bringing health care to the rural and remote communities
April 2013
Information and communication technology (ICT) is now being used to deliver better healthcare to patients. Telehealth has been widely used around the world and enables health professionals to provide healthcare services to patients in rural and remote areas. It has also provided great opportunities to patients who currently have difficulties in accessing health-related services due to the barriers of location, time and the cost of travel. Telehealth exists in various forms: video consultation, remote monitoring, asynchronous care and teleconferencing. The only form of Telehealth currently funded by the Australian Government is video consultation.
Benefits of Telehealth The Australian Government has introduced Telehealth funding to improve healthcare for patients living in rural and remote locations and to better utilise the skills of the current health workforce.
The major benefits of Telehealth for patients include the reduction of travel cost and time, improved access to specialist services and a reduction in hospital admissions. Patients are able to see health professionals and have their health assessments completed in a timely manner, thus improving health outcomes.
Health practitioners also benefit from providing ongoing support to rural health practitioners. They can share knowledge and also engage in collaborative practice across many specialities. For example, a GP working in a rural location who supports a patient during a video consultation is able to provide a thorough clinical handover to the specialist working in the metropolitan area. Therefore, practitioners can deliver the appropriate and timely healthcare service to patients.
When to UseTelehealth Telehealth consultations are seen as an alternative to the standard face-to-face consultation. It is at the health practitioner’s discretion whether the patient is suitable for a video consultation. There are many factors that need to be considered when this type of Telehealth is being offered and provided to patients. For example, it is important to respect the patient’s autonomy regarding the
choice of using Telehealth over a face-to-face consultation. It is vital that the patient understands the risks and benefits involved. It is also important that the General Practitioner and/or the Specialist are aware of the type of physical examination that could be required during a video consultation. This allows the Specialist to provide a thorough consultation. The Medical Board of Australia and the Royal Australasian College of Physicians have developed Telehealth Guidelines for doctors who participate in using Telehealth. These guidelines provide advice on how to conduct video consultations effectively and include comprehensive information on the clinical, technical and contextual aspects of Telehealth. For more information, refer to the websites below:
http://www.racptelehealth.com.au/guidelines/
http://www.medicalboard.gov.au/Codes-Guidelines-Policies.aspx
Telehealth MBS Incentives
In 2011, financial incentives were introduced for eligible health professionals and aged care services to undertake video consultation. The purpose of these incentives is to encourage and support the initial and ongoing provision of Telehealth to eligible patients by an eligible health practitioner. Video consultations funded under the Medicare Benefits Schedule will have two ends: the patient-end and the specialist-end. The patient-end refers to the end at which the patient sits, which could incorporate support from General Practitioners, Nurse Practitioners, Practice Nurses, Midwives and Aboriginal health care workers. These health practitioners are providing clinical support to the patient during a video consultation with a Specialist. At the specialist-end, the Specialist provides the consultation via a video link to the patient.
To be able to receive the financial incentives, the health practitioners involved must be either a Specialist and/or a General Practitioner (or Practice staff providing support on behalf of a GP). The Specialist can be located anywhere in Australia to provide video consultations to eligible patients. The Medicare Benefits Schedule classifies eligible patients as those who are located in the rural
and remote area, or care recipients of a Residential Aged Care Facility or a patient of an eligible Aboriginal Medical Service. There is a 15km distance requirement which applies to patients who are supported by the patient-end from a rural and remote location. This distance requirement does not apply to patients in Residential Aged Care Facilities and Aboriginal Medical Services.
There are Medicare rebates available at the specialist-end and patient-end. There are 17 telehealth items in conjunction with the 55 existing items for Telehealth that specialists can claim. For the patient-end, there are 23 Telehealth items that can be claimed relating to the support provided to the patient during a video consultation with the specialist. These are available to General Practitioners, Practice Nurses, Aboriginal health workers, Nurse Practitioners, and Midwives. A complete list of the Telehealth MBS items can be found at:
http://www.mbsonline.gov.au/internet/mbsonline/publishing.nsf/Content/connectinghealthservices-itemlist
Healthfirst NetworkHealthfirst Network is funded by the Department of Health and Ageing to deliver Telehealth education and provide support to health professionals and support staff. Healthfirst Network is providing telehealth training which is accredited by the Royal Australian College of General Practitioner and the Australian College of Rural and Remote Medicine. The training session covers the basics of Telehealth, equipment characteristics and integration into practice processes. Healthfirst Training Australia has also developed 3 units of competency on Telehealth at certificate IV level. This training provides more in-depth knowledge of Telehealth and its applications. There are also 3 Telehealth Training and support officers who can provide basic support to implement Telehealth capabilities in your practice or facility. These services are at no cost until May 2013.
For further information please contact the Healthfirst Network telehealth team on 8404 3400 or [email protected].
Kaye FaheyHealthFirst
Page 9April 2013
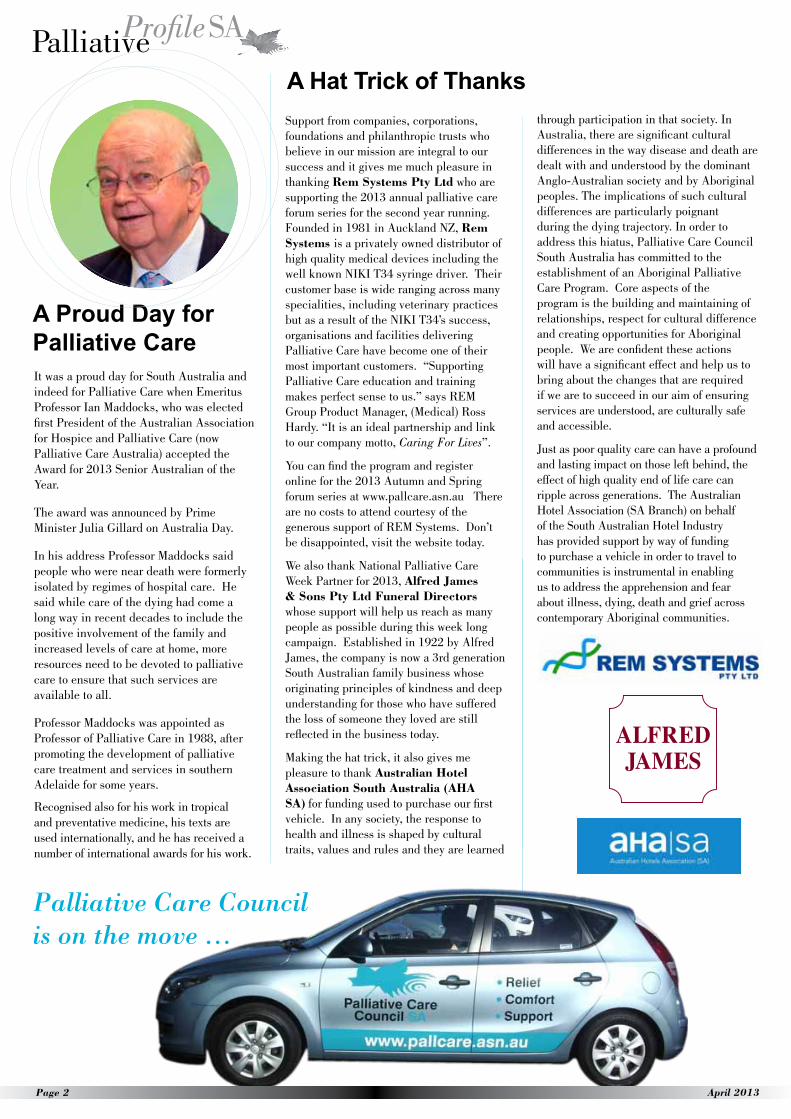
PCCSA is calling for Expressions of Interest (EOI) from local Aboriginal artists or designers to submit artwork that can be adapted and reproduced on our first ever Reconciliation Action Plan (RAP).
In 2003 PCCSA commissioned two Aboriginal artists from Port Augusta to create artwork for a brochure that would be recognised in all South Australian Aboriginal communities. It has been ten years since the art was created and we were very pleased to learn the original works were ‘taken home’ late last year and are now displayed outside the Banksia Palliative Care Ward at Port Augusta Hospital.
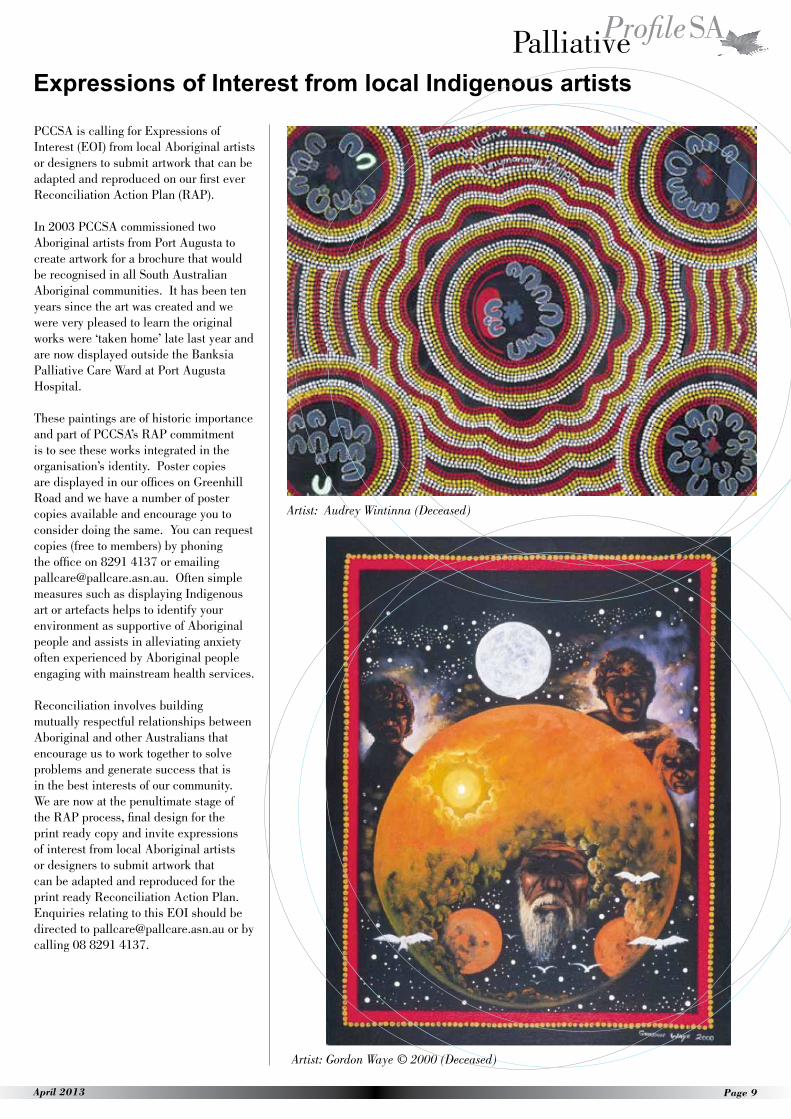
These paintings are of historic importance and part of PCCSA’s RAP commitment is to see these works integrated in the organisation’s identity. Poster copies are displayed in our offices on Greenhill Road and we have a number of poster copies available and encourage you to consider doing the same. You can request copies (free to members) by phoning the office on 8291 4137 or emailing [email protected]. Often simple measures such as displaying Indigenous art or artefacts helps to identify your environment as supportive of Aboriginal people and assists in alleviating anxiety often experienced by Aboriginal people engaging with mainstream health services.
Reconciliation involves building mutually respectful relationships between Aboriginal and other Australians that encourage us to work together to solve problems and generate success that is in the best interests of our community. We are now at the penultimate stage of the RAP process, final design for the print ready copy and invite expressions of interest from local Aboriginal artists or designers to submit artwork that can be adapted and reproduced for the print ready Reconciliation Action Plan. Enquiries relating to this EOI should be directed to [email protected] or by calling 08 8291 4137.
Expressions of Interest from local Indigenous artists
Artist: Audrey Wintinna (Deceased)
Artist: Gordon Waye © 2000 (Deceased)

Page 10 April 2013
I have been involved with palliative care services for the last 23 years in a variety of roles: a specialist palliative care nurse across hospice, community and liaison as well as a project officer for both state and national palliative care projects. The reason for one’s engagement with palliative care services will often determine the level of understanding of the responsibilities the services have beyond direct care to the community.
From the perspective of a patient needing to access palliative care, their concerns will be about access to care, how do I make contact with a palliative care service, what can they do for me and even, ‘does this mean I am dying’? Rarely would the client/patient, or other health service providers be aware of what goes on ‘behind the scenes’ to improve service standards or what a palliative care service is required to do from the perspectives of SA Health, the Commonwealth or even Palliative Care Australia. So the focus of this article is just that, what does go on behind the scenes in specialist palliative care services?
My current role as the PCOC Quality Improvement Facilitator for SA & NT provides me the perfect opportunity to go behind the scenes and support specialist providers of palliative care in the community to provide evidence based quality palliative care and to be able to measure the outcomes of that care. The Palliative Care Outcomes Collaboration (PCOC) is funded through the National Palliative Care Program by the Australian Government Department of Health and Ageing. This program has been in existence since 2005 and currently 103 palliative care services participate nationally.
There are 18 specialist palliative care services in metropolitan and country South Australia. By July 2013, 17 of these services will participate in the quality initiative that is PCOC. The 18th service is the paediatric palliative care service and although not participating at present as they require a different set of assessment tools and database, the paediatric palliative care service is working with PCOC to develop these. This is a very exciting time because it demonstrates the keen interest palliative care services across SA have in improving the quality of care they provide daily for palliative care patients and their families.
The PCOC process is not simple and requires participation and understanding across the multidisciplinary team responsible for providing palliative care. It consists of 5 assessment tools1 that are evidence based and are used by clinicians to assess the following:
1) How sick the patient is, i.e. stable, unstable, deteriorating or terminal
2) How dependent a patient is in relation to activities of daily living and the resources required in meeting their care
3) What is the patient capable of doing in relation to their activity, work and self-care
4) Problems (symptoms) the patient is experiencing, as assessed by the patient, based on the amount of distress caused to them. Some of the symptom issues are pain, fatigue, inability to sleep, difficulty breathing, constipation
5) A clinician assessment about the severity of pain, other symptoms, family, psychological and spiritual issues
By using these tools when a patient is reviewed, either in person or over the phone, a plan of care can be developed which is specific to each individual patient and family. The tools encourage further discussion with the patient and family around what community services are required, who will take responsibility for their medical needs, what specific wishes does the patient and family have about place of death and so on.
Demographic information about the patient and information collected using the PCOC assessment tools is used to generate a series of statistical reports every 6 months. These reports help palliative care services to see how they are performing against nationally agreed benchmarks and other palliative care services within Australia. The role of the PCOC Quality Improvement Facilitator SA/NT is to meet with services after their report has been generated to discuss the results and consider how they might improve outcomes. If required, a plan for improvement is developed with agreed goals and timeframes in the hope that appropriate changes to practice are implemented. The palliative care service undertakes a review against the agreed improvement plan periodically and if there is still no improvement in outcomes, the plan is revisited, possibly altered and the
process of evaluation continues.
Another key quality improvement strategy is the National Standards Assessment Program (NSAP)2. NSAP provides specialist palliative care services the opportunity to rate themselves against the Australian national palliative care standards. This is a process that palliative care services go through every two years in an effort to demonstrate that they are meeting the standards and, where necessary, improving the care they are providing. The standards were developed by Palliative Care Australia and are in the process of being reviewed. There are trained peer mentors from within palliative care who are available to assist participating services in this process. Like PCOC, NSAP engages the entire multidisciplinary specialist palliative care team.
A further National Palliative Care Program, Caresearch, is collating the evidence that underpins palliative care practice. Caresearch is a web based information portal which provides open access to reliable, regularly updated and reviewed information about managing palliative care symptoms as well as emotional, psychological and spiritual needs. This program is simple to use, written clearly for both clinicians such as palliative care services, General Practitioners, Aged Care Facilities as well as for families and carers. Access is free via the internet on www.caresearch.com.au.3
This article summarises three of several National Palliative Care programs providing support for organisations and services interested in improving the quality of palliative care they provide. I do hope this has assisted in informing the larger community about what goes on behind the scenes in their community/hospice/ inpatient palliative care service.
Janet Taylor, PCOC Quality Improvement Facilitator SA & NT1www.pcoc.org.au 2www.palliativecare.org.au 3www.caresearch.com.au
Ed - Other national palliative care programs are Experience in the Palliative Approach (PEPA), PCC4U and PaCCSC which provide a variety of opportunities and you can obtain more information about these programs by emailing [email protected].
What goes on in SA palliative care services that the larger community never hears about…

Page 11April 2013
Close the Gap Day was celebrated by PCCSA this year at The Queen Elizabeth Hospital on March 26th.
The morning was filled with a range of community events hosted by The Queen Elizabeth Hospital to promote a better understanding of Aboriginal services and programmes, including a Welcome to Country by Aunty Josie Agius, the unveiling of artist Rick Taylor’s new Close the Gap mural in the undercroft, visits by local Aboriginal footballers, and live music during the BBQ lunch.
A palliative care yarning room was set up in the Aboriginal Liaison Unit, and a small number of people came in for a chat about issues for Aboriginal palliative care (and to enjoy the wonderful kangaroo stir fry lunch and fresh herb teas).
In the afternoon, approximately 150 people attended a forum with panelists Robert Dann, Aboriginal Health Council of South Australia, Rosemary Wanganeen, founder of the Australian Institute for Loss and Grief in Adelaide and member of the PCCSA Board, Shane Burgess, Aboriginal Health Worker and developer of Advance Care Yarning*, Bill Edwards, Presbyterian minister working with remote Aboriginal communities since 1950 and experience with interpreting, Dr Sally Williams, Palliative Care specialist, and with Emeritus Professor Ian Maddocks as moderator.
There was a broad ranging discussion across the panel, with many questions from the audience as well as prompts from the Moderator and issues raised in the morning yarning session. A number of topics were listed at the end of the session for possible action. One of the early audience questions was “What is palliative care and why do we need it? Aboriginal people look after their own people.” In the answer it was pointed out that palliative care could support and supplement what a family can offer, without taking away from what the family can do. But there may be
Close the Gap Day 2013
things that could be done more easily, or more comfortably with professional help.
Access to palliative care came up in several ways. One difficulty seemed to be in both community and hospital settings, access to palliative care was dependent on a doctor making the referral, and this didn’t happen even when it was requested. The importance of Aboriginal Health Workers being able to refer patients/clients for palliative care was highlighted.
Cultural safety and respect were emphasised. Historical events still create barriers of fear and mistrust for Aboriginal people who need to access hospital or institutional care, but may choose not to. The importance of seeing the Aboriginal person as an individual, and respecting that person’s choices was discussed. It was pointed out that within the Aboriginal community culture was expressed and valued in a wide range of ways. This extended to things like the importance of going home to country, which would vary from person to person. For some people it would be quite ok to die in hospital, for others going back to their country would be very important, more important than staying for extra treatment, particularly if there were spiritual and cultural duties to attend to.
The important message was to respectfully find out the wishes of the person.
The audience was surprised to learn there were 250 Aboriginal Health Workers in South Australia, most being in Aboriginal Medical services. It was argued that they should be distributed more widely through mainstream services to foster cross- cultural education and familiarization, and to use their skills.
A report of the forum is being prepared, and several of the issues raised will be followed up by PCCSA’s newly appointed Aboriginal project officer, Teresa Onorato.
Thanks must go to Natalie McCabe and Natalie Williams for all their hard work on the day and their support of palliative care.
Mary Brooksbank
*Advance Care Yarning is a Respecting Patient Choices publication that was developed by Shane Burgess using language and examples relevant for Aboriginal people.
What: ACPEL Advance Care Planning and End of Life Care conference
When: 9-11 May 2013Where: Melbourne Convention and Exhibition Centre Info: http://www.acpelsociety.com.au/conference/
What: IHPA - Activity Based Funding Conference 2013 When: 13-16 May 2013Where: Sydney Convention and Exhibition CentreRegister: http://abfconference2013.com/registration.htmlMore Info: http://abfconference2013.com/news/5.html
What: International Centre for Nursing Ethics - 14th Annual Conference
Ethical issues at the end of life: practice and policy imperatives in health care
When: 16 – 17 May, 2013Where: Carson Conference Centre, ANF (Vic Branch), MelbourneInfo: http://www.deakin.edu.au/health/research/aci/icne-
conference/index.php
What: National Palliative Care Week Theme Palliative Care Everyone’s Business......
When 19th – 25th May 2013 Where: Keep a watch on pallcare.asn.au for NPC Week activities.....Register: TBA
What: Dying at home Public ForumWhen: Wednesday 23th May 2013 Where: Adelaide Townhall 128 King William Street Register: www.pallcare.asn.au (registrations open soon)
What: Palliative Care Awards – Nominations Open When: 20th May 2013Where: Online nominations at www.pallcare.asn.au (awards)
What: Hawke Centre Palliative Care Lecture: Professor Roderick Macleod: Who Cares? The role of communities near the end of lifeWhen: 16th July 2013 (Midday to 2pm)Where: Bob Hawke Prime Ministerial Centre, UniSA Campus, North Terrace, AdelaideMore Info: www.pallcare.asn.au
What: Nursing Informatics Conference @ HIC 2013 - Call for Papers
When: 15 July-18 July 2013, 9 - 5pmWhere: Adelaide Convention Centre More Info: www.hisa.org.au/hic2013
What: Inaugural National Palliative Care Research Colloquium
When: 18-19 July 2013Where: MelbourneMore info: https://ap1.salesforce.com/sfc/p/ and http://centreforpallcare.org/index.php/events/
What: Cancer Nurses Society of Australia 16th Winter Congress Theme: Connecting Cancer Care
When: 25-27 July 2013Where: Brisbane Convention and Exhibition CentreMore info: http://www.cnsawintercongress.com.au/ or email: [email protected]
What: PCCSA AGM When: August 27th 2013 6.00pmWhere: 202 Greenhill Road, Eastwood SAMore Info: www.pallcare.asn.au
What: 12th Australian Palliative Care ConferenceWhen: 3-6 September 2013Where: National Convention Centre, Canberra Register: www.dcconferences.com.au/apcc2013
What: Letting Go Part II – futile treatments, communication and advance care planningWhen: 10th September 2013 5.30 – 7.30pmWhere: The Royal Coach Inn, Dequettiville Terrace, Kent TownRegister www.pallcare.asn.au (events)
What: SA Advance Care Planning LegislationWhen: 10th October 2013 Where: The Royal Coach Inn, Dequettiville Terrace, Kent TownRegister www.pallcare.asn.au (events)
What Palliative Care Council SA – Palliative Care AwardsWhen: 14 October 2013Where: TBARegister: TBA
What: Adelaide Symphony Orchestra have generously donated their concert - A night in Vienna in support of palliative care. When: 26th October 2013 Where: Festival CentreRegister: Tickets will be on sale soon. See the next edition for ticket purchase details
Conferences and Coming Events
ContributionsPlease forward material to the Palliative Care Council South Australia Incorporated 202 Greenhill Road, Eastwood SA 5063PO Box 929, Unley SA 5061Email: [email protected] Phone 08 8291 4137 Toll Free: 1800 660 055
AdvertisingIf you are interested in advertising in PalliativeProfileSA please contact Tracey Watters, Email [email protected]
DisclaimerThe views expressed in PalliativeProfile SA are those of the contributors and not necessarily endorsed by the editorial committee. The committee also reserves the right to abridge or not publish submitted articles.