Embed Size (px)
Citation preview

Palmetto Government Benefits Administrators
Durable Medical Equipment Regional Carrier P.O. Box 100141 Columbia, SC 29202-3141
MARCH 1995 ISSUE 10PAGE 95-1
Alabama GeorgiaArkansas KentuckyColorado LouisianaFlorida Mississippi
New Mexico South CarolinaNorth Carolina Tennessee
Oklahoma TexasPuerto Rico Virgin Islands
DMERCMEDICARE ADVISORY
ATTENTION PHYSICIANS AND SUPPLIERSIN THIS ISSUE:Anti-Fraud Unit
Supplier Sanctions ................................................................ 95-15Appeals Workload ....................................................................... 95-2Back to Basics Workshop Series Begins .................................... 95-1Bladder Stimulators ..................................................................... 95-2Claim Filing Reminders ............................................................. 95-14
CMN Filing Reminders .......................................................... 95-14Crossover Update
Medigap Policies .............................................................. 95-12-13Complementary/Supplemental Policies ................................ 95-13Identification of Crossover Remark Codes ............................ 95-13
DMERC Medicare Advisory Update ............................................ 95-3Durable Medical Equipment (DME) Repair Claims ................... 95-11Electronic Data Interchange (EDI)
Electronic Mailbox Directory ................................................. 95-17Electronic Submission of MSP Claims ............................. 95-17-18
HCPCS Code Changes ............................................................. 95-25HCPCS Codes and Modifiers Not Available for Use ................. 95-24HCPCS Codes Requiring A CMN ........................................ 95-20-24HCPCS Codes Update:
New DMERC Level III Codes And Modifiers ................ 95-25-26Health Maintenance Organizations (HMOs) and Medicare ....... 95-10Home Blood Glucose Monitor Pricing Change .......................... 95-27Immunosuppressive Drugs
Sandimmunne ....................................................................... 95-27Prograf .................................................................................. 95-27
Incontinence Disposable Supplies .............................................. 95-2
Infusion PumpsDobutamine ............................................................................. 95-4Home Parenteral Inotropic Therapy: Data Collection Form .... 95-5
Interest Rate Payable on Clean Claims Update .......................... 95-2Investigational Devices Not Covered by Medicare ...................... 95-2Julian Date Reference & Calendar ............................................ 95-16Lymphedema Pumps/Pneumatic Compressors ........................ 95-19Medical Policy Update ................................................................ 95-3Modifier Instructions for New Medical Policies ............................ 95-4Oxygen: New Documentation Requirements ............................. 95-4Prior Authorization Telephone Number Discontinued ................. 95-2Professional Relations Adds More Staff ...................................... 95-8
New Ombudsmen ................................................................... 95-8Ombudsmen Reassignment .................................................... 95-9Ombudsmen Addresses and Territories ................................. 95-9
Puerto Rico Postal Information ................................................. 95-14Q & A ........................................................................................ 95-15Region C Directory .................................................................... 95-39
Palmetto GBA Region C DMERC Contacts .......................... 95-39National Numbers ................................................................. 95-39
Span Dates Needed When Filing Claims .................................. 95-10Workshop Notice......................................................................... 95-6Workshop Registration Form ...................................................... 95-71995 DME Fee Schedule for New HCPCS Codes ............... 95-37-381995 DME Fee Schedule for Virgin Islands and Puerto Rico95-28-341995 PEN Pricing ................................................................. 95-35-361995 Surgical Dressing Fee Schedule ...................................... 95-37
New Alphabetized Table of Contents
Back to Basics Workshop Series Begins
Palmetto Government Benefits Administrators (Palmetto GBA) will be conducting a new series of educationalworkshops throughout the South and Southwest Region from April 4, 1995 - May 24, 1995. These full-day workshopswill cover general information about Palmetto GBA and the basics of claims filing. The workshop content will be designedto educate new billers or suppliers and offer a refresher course in DMERC billing guidelines.
A list of the dates and locations for these workshops, along with the actual registration form, are listed on pages 95-6-7 of this advisory. Please note the registration form enclosed in this advisory is the actual form you must use to registerfor one of these workshops. A separate registration form will not be mailed to you.
Details on pages 95-6-7

Page 95-2 March 1995 DMERC Medicare Advisory
Medical devices which have not been approved for marketing by the Food and DrugAdministration (FDA) are considered investigational by Medicare and are not covered.According to the Medicare program, investigational medical devices do not meet themedical criteria for coverage and are not reasonable and necessary for the diagnosisor treatment of illness or injury, or to improve the functioning of a malformed bodymember. Medicare payment, therefore, may not be made for medical procedures orservices using devices which have not been approved for marketing by the FDA.
INVESTIGATIONALDEVICES NOTCOVERED BYMEDICARE
The use of spinal cord electrical stimulators, rectal electrical stimulators (including theContinaid), and bladder wall stimulators (including the Mentor Bladder Pacemaker)cannot be considered reasonable and necessary. Therefore, payment cannot bemade under the Medicare program for these devices or for their implantation. Pelvicfloor stimulators, whether inserted into the vaginal canal or rectum, or implanted in thepelvic area, used as a treatment for urinary incontinence, either as a bladder pacer ora retraining mechanism, are not covered. The safety and effectiveness of thesedevices are unproven.
BLADDERSTIMULATORS
INCONTINENCEDISPOSABLESUPPLIES
Medicare does not cover or reimburse for disposable incontinence supplies such asdiapers, chucks or rubber sheets. Do not bill the DMERCs using the following HCPCScodes when supplying diapers, chucks, rubber sheets or other disposable inconti-nence supplies.
A4327 - Female external urinary collection device; metal cup, eachA4328 - Female external urinary collection device; pouch, eachA4329 - External catheter starter set, male/female, includes catheters/urinary
collection device, bag/pouch and accessories
PRIORAUTHORIZATIONTELEPHONE NUMBERDISCONTINUED
INTEREST RATEPAYABLE ON CLEANCLAIMS UPDATE
The Treasury Department has announced, effective January 1, 1995, the new PromptPayment interest rate will be 8.125 percent. The new rate will be effective forscheduled Medicare payment dates of January 1 through June 30, 1995. The rate isapplicable to clean paper and electronic claims that have not been paid by the 30th dayafter the date of receipt. The new rate has been approved by the Secretary of theTreasury and was published in the Federal Register on January 3, 1995.
APPEALSWORKLOAD
Palmetto Government Benefits Administrators (Palmetto GBA) has received a greaterthan anticipated volume of written appeals over the past few months, and is activelyworking to resolve pending appeals within the 45 day timeframe. Please rememberthat appeals may be conducted over the telephone by contacting the Dedicated WorkTeams at (803) 691-4300.
As noted on page 94-223 of the DMERC Medicare Advisory, December 1994 issue,effective February 1, 1995 the prior authorization telephone number was discontinueddue to low physician participation and misuse of the telephone lines by nonphysiciancallers. Prior authorization may still be obtained for POVs, TENS and seat liftmechanisms through a written request submitted by the ordering physician. The priorauthorization process is conducted by our specially-trained review personnel. Priorauthorization does not guarantee payment by Medicare for the product. Theauthorized determination is a confirmation that the patient's condition, as described,meets the criteria defined in the DMERC medical policies.
Send written prior authorization requests to: Palmetto GBA, Prior AuthorizationDept., Medicare Region C DMERC, P.O. Box 100235, Columbia, SC 29202-3235.

March 1995 DMERC Medicare Advisory Page 95-3
DMERC MEDICAREADVISORY UPDATE
t CMN Instruction Clarification: On page 94-9 of the DMERC Medicare Advisory,January 1994 issue, and on page 94-129 of the DMERC Medicare Advisory, June1994 issue, instruction is given on the completion of CMN 10.01 for Enteral Nutrition,omitting question 8 from the needed question set for correct filing of the CMN. EnteralNutrition suppliers submitting their first claim to Palmetto GBA need to ensure thatquestions 2,6,8, and 9-13 are completed.
t HCPCS Code Description Corrections: On page 94-220 of the DMERCMedicare Advisory, December 1995 issue, the descriptions for HCPCS codesL3140 and L3150 are listed incorrectly. Effective January 1, 1995, the descrip-tions for these codes are as follows:
L3140 - Foot, abduction rotation bar, including shoesL3150 - Foot, abduction rotation bar, without shoes
t DME Fee Schedule Corrections: On pages 94-255-274 of the DMERC Medi-care Advisory, December 1994 issue, some fee schedules for a few states weremisprinted. Those codes, along with their corrected prices, are listed as follows:
Code Category State Correct PriceE0193 DME Capped Rental Items NM 775.83E0193 DME Capped Rental Items PR 1459.64E0271 Inexpensive or Routinely Purchased (New) FL 170.01E0950 Inexpensive or Routinely Purchased (Used) FL 59.70K0037 Inexpensive or Routinely Purchased (Used) FL 32.54
MEDICAL POLICYUPDATE
Home Blood Glucose Monitor (Correction)
The Home Blood Glucose Monitor Medical Policy listed in the Medicare Region CDMEPOS Supplier Manual incorrectly states that normal, low, and high calibratorsolution/chips (A4256) are not covered separately. Effective March 1, 1995, thesesolutions/chips may be reimbursed separately only when purchased after the initialissue of the Home Blood Glucose Monitor.
Orthopedic Footwear (Correction)
The Orthopedic Footwear Medical Policy published in the DMERC Medicare Advisory,December 1994 issue, is inadvertently missing code L3219. Please make a note toinclude code L3219 (Orthopedic footwear, man's shoes, oxford) in the OrthopedicFootwear Medical Policy on page 94-220 of the DMERC Medicare Advisory, Decem-ber 1994 issue.
Therapeutic Shoes (Correction)
The Therapeutic Shoe Medical Policy on page 94-219 of the DMERC MedicareAdvisory, December 1994 issue, incorrectly states, "On hard copy claims, thisstatement should be on a separate sheet attached to the claim. On electronic claims,it would be put in the HAØ record." Please strike these sentences from the TherapeuticShoe Medical Policy.
Note: This information will be published in a revision to the Region C DMEPOSSupplier Manual.

Page 95-4 March 1995 DMERC Medicare Advisory
OXYGEN: NEWDOCUMENTATIONREQUIREMENTS
MODIFIERINSTRUCTIONS FORNEW MEDICALPOLICIES
The following modifiers are available for usage according to the DMERC Medical Policyguidelines for Epoetin Alpha (EPO), Lower Limb Prostheses, Therapeutic Shoes andOrthopedic Footwear. For these DMERC Medical Policies and their modifier require-ments, please refer to pages 94-207-222 of the DMERC Medicare Advisory, December1994 issue.
EJ - Subsequent Claim (For Epoetin, Alpha-Epo Injection Only)
ZX - Specific requirements found in the Documentation section of the medical policyhave been met and evidence of this is available in the supplier's record.
K0 - Lower limb extremity prosthesis functional Level 0 - Does not have the ability orpotential to ambulate or transfer safely with or without assistance and a prosthesisdoes not enhance their quality of life or mobility
K1 - Lower extremity prosthesis functional Level 1 - Has the ability or potential to usea prosthesis for transfers or ambulation on level surfaces at fixed cadence. Typicalof the limited and unlimited household ambulator.
K2 - Lower extremity prosthesis functional Level 2 - Has the ability or potential forambulation with the ability to traverse low level environmental barriers such ascurbs, stair or uneven surfaces. Typical of the limited community ambulator.
K3 - Lower extremity prosthesis functional Level 3 - Has the ability or potential forambulation with variable cadence. Typical of the community ambulator who hasthe ability to traverse most environmental barriers and may have vocational,therapeutic, or exercise activity that demands prosthetic utilization beyond simplelocomotion.
K4 - Lower extremity prosthesis functional Level 4 - Has the ability or potential forprosthetic ambulation that exceeds basic ambulation skills, exhibiting high impact,stress, or energy levels. Typical of the prosthetic demands of the child, active adult,or athlete.
Effective June 1, 1995, additional documentation must be provided on all initial andrevised Certificates of Medical Necessity (CMN) for oxygen (HCFA-484 form) for thefollowing patients:
t Any new patient, as of June 1, 1995 or after, whose prescribed flow rate exceeds fourliters per minute (LPM)
t Any existing patient whose prescription increases as of June 1, 1995 or after, to a flowrate greater than four liters per minute (LPM)
Documentation must be furnished on the HCFA-484 form and must consist of arterialblood gas values or oxygen saturation levels obtained from tests conducted on oxygen ata flow rate of four liters per minute (LPM). Test results should be indicated in Item 3A ofthe HCFA-484 form, with notation in Item 3B that testing was conducted on a four liter perminute flow rate of oxygen.
Claims received with the following modifiers will not be approved for additional paymentwhen the supporting documentation as described above is not included on the HCFA-484form:
QF - Flow rate exceeds 4LPM, with a portable systemQG - Flow rate exceeds 4LPM, without a portable system
Additionally, patients receiving oxygen from a stationary unit at a flow rate greater than fourliters per minute and also receiving portable oxygen will be reimbursed on the portablecomponent or for the higher flow rate, whichever is greater, but not both.
The Region C DMERC Medical Policy on infusion pumps lists criteria for coverage ofhome dobutamine infusion (code XX009-Dobutamine, 250mg). Effective immediately,the Region C DMERC will consider coverage of dobutamine infusionand other inotropicdrugs on an individual case by case basis, for patients who are not cardiac transplantcandidates. Information on the expanded criteria includes; invasive hemodynamicmonitoring, cardiac ejection fraction, pulmonary wedge pressure, and New York HeartAssociation (NYHA) class information.
For dobutamine infusion documentation, a suggested form for data collection andsubmission to the DMERC is provided on the opposite page. Please photocopy this formfor your files and use as appropriate, if desired.
INFUSION PUMPS:Dobutamine

March 1995 DMERC Medicare Advisory Page 95-5
HOME PARENTERAL INOTROPIC THERAPY: DATA COLLECTION FORM
Patient's Name: Age:
1) Results of invasion hemodynamic monitoring:
Cardiac Pulm. Art. WedgeOutput Pressure Pressure Date
Before inotrope infusion
On inotrope infusion
Drug Dose mcg/kg/min
2) Cardiac medications (digoxin, diuretics, vasodilators) during attempted weaningfrom inotrope infusion (list name, dose, frequency):
3) Does this represent maximum tolerated doses of these medications?(If no, please explain)
4) NYHA class on above medication prior to inotrope infusion:
5) Have attempts to wean the patient off inotrope infusion in the hospital failed?(If no, please explain)
6) Initial home prescription: Drug mcg/kg/minhrs/day days/week (or every days)
7) NYHA class at the time of discharge:
8) Is the patient capable of going to the physician for outpatient evaluation?(If no, please explain)
The above statements and any additional explanations included separately are true andaccurate and there is documentation present in the patient's medical record to supportthese statements.
Physician Signature: Date:
Physician Name Printed/Typed:
Physician Specialty:
2/16/94

Page 95-6 March 1995 DMERC Medicare Advisory
April 1995Apr. 4 Columbia, SC Holiday Inn Coliseum, 630 Assembly St., 29201 (803) 799-7800Apr. 6 Raleigh, NC Holiday Inn, I-40 at Research Triangle Park, Exit 282, 27709 (919) 941-6000Apr. 10 Jackson, MS Holiday Inn Downtown, 200 East Amite St., 39201 (601) 969-5100Apr. 10 Atlanta, GA Westin Peachtree, 210 Peachtree St. NW, 30303 (404) 659-1400Apr. 12 Asheville, NC Radisson, One Thomas Wolfe Plaza, 28801 (704) 252-8211Apr. 13 Savannah, GA Marriott Riverfront, 100 General McIntosh Blvd., 31401 (912) 233-7722Apr. 18 Oklahoma City, OK Medallion Hotel, One North Broadway, 73102 (405) 235-2780Apr. 18 Ft. Lauderdale, FL Sheraton at Ft. Laud. Airport, 1825 Griffin Rd., (Dania, FL), 33004 (305) 920-3500Apr. 20 Denver, CO Embassy Suites - Denver Airport, 4444 N. Havana, 80239 (303) 375-0400Apr. 21 San Juan, PR Radisson Normandie, Munoz Rivera Ave., 00901 (809) 729-2929Apr. 24 Jacksonville, FL Omni, 245 Water St., 32202 (904) 355-6664Apr. 26 Orlando, FL Delta Orlando Resort, 5715 Major Blvd., 32819 (407) 351-3340Apr. 28 New Orleans, LA Doubletree Hotel, 300 Canal St., 70130 (504) 581-1300Apr. 28 Dallas (Irving), TX Doubletree Guest Suites, 4650 West Airport Freeway, 75062 (214) 790-0093
May 1995May 2 Lexington, KY Hyatt Regency, 400 W. Vine St., 40507 (606) 253-1234May 4 Nashville, TN Regal Maxwell House, 2025 Metro Center Blvd., 37228 (615) 259-4343May 8 Little Rock, AR Robinson Convention Center, #7 State House Plaza, 72201 (501) 376-4781May 10 Lubbock, TX Holiday Inn Lubbock Plaza, 3201 South Loop 289, 79423 (806) 797-3241May 12 Houston, TX Sheraton Crown Hotel, 15700 J.F.K. Blvd., 77032 (713) 442-5100May 15 Shreveport, LA Holiday Inn Downtown, 102 Lake St., 71101 (318) 222-7717May 16 San Antonio, TX Plaza San Antonio Hotel, 555 S. Alamo St., 78205 (210) 229-1000May 17 Mobile, AL Ramada Conference Ctr., 600 S. Beltline Hwy., 36608 (205) 344-8030May 22 Memphis, TN Adams Mark, 939 Ridge Lake Blvd., 38120 (901) 684-6664May 22 Albuquerque, NM Albuquerque Marriott Hotel, 2101 Louisiana Blvd., 87110 (505) 881-6800May 24 Tulsa, OK Radisson Inn - Tulsa Airport, 2201 N. 77th East Ave., 74115 (918) 835-9911May 24 Birmingham, AL Sheraton Civic Center, 2101 Civic Center Blvd., 35203 (205) 324-5000
DATE CITY/STATE SPECIALTY WORKSHOP LOCATIONS PHONE
WORKSHOP NOTICE
Palmetto Government Benefits Administrators (Palmetto GBA), the Medicare Region C Durable Medical EquipmentRegional Carrier (DMERC), is sponsoring a series of full day workshops throughout the South and Southwest regionfrom April 4, 1995 - May 24, 1995. The agenda for each of our Back to Basics Workshops will consist of the following:
8:30 - Registration 12 noon - 1:30 p.m. - Lunch Break (Lunch will not be provided.)9:00 a.m. - 12 noon - Claims Filing 1:30 p.m. - 4:00 p.m. - Palmetto GBA Overview
We are inviting you, and more specifically, new billers to attend a full day workshop. These workshops will be held inthe various locations listed below. Please share the information in this workshop notice with all individuals planning toattend a workshop.
To Register:Please return a completed registration form along with payment two weeks in advance of the workshop you wish toattend. The registration form can be found on the following page and photocopied as often as necessary. The fee isa nonrefundable $30.00 per person. If your completed registration is received two weeks prior to your workshop, aconfirmation card will be sent to you. Please do not call to verify your registration. Cash at the door is unacceptable.Please complete the registration form and return it, along with payment, to the new return address on the registrationform.
Each individual attending a workshop can expect to receive workshop materials, as well as complementary coffee, teaand assorted sodas. The ombudsmen staff will conduct each full day workshop and will be available to answer yourquestions.
NOTE: Specific resolution of individual claim denials will not be possible due to our inability to gain access to ourprocessing system in meeting room facilities.
Lunch will not be provided and parking will not be validated. Invitations will not be mailed separately.
BACK TO BASICS: A Full Day Workshop For Beginning Billers

March 1995 DMERC Medicare Advisory Page 95-7
Return This Form and Payment To:
Palmetto GBA WorkshopsP.O. Box 25163Columbia, SC 29224
Supplier No.:
( )
Supplier Name:
Supplier Address:
Name(s) of people attending:
Phone Number: Contact Person:
Date:
City:
Select the date and city you wishto attend from the workshoplisting on the previous page:
Payment Information:
Number of people attending the workshop
Total Amount Due/Enclosed
Use our Fed Ex address:Palmetto GBA Workshops300 Arbor Lake Drive, Suite 1300Columbia, SC 29223
Please make checks payable to Palmetto GBA Workshops.
Checks must be received by the Palmetto GBA office before theworkshop begins. Payment will not be accepted at the door onthe day of the workshop. All registration fees are nonrefundable.
x $30.00 (per person)
Please Note Our New Address For Workshop Registration
OR
BACK TO BASICSWORKSHOP REGISTRATION FORM
Due in advance of your selected workshop with your nonrefundable payment

Page 95-8 March 1995 DMERC Medicare Advisory
PROFESSIONALRELATIONS ADDSMORE STAFF
As part of our continuing efforts to meet your educational needs, Palmetto GBA ispleased to announce we are increasing our Professional Relations staff to includeadditional ombudsmen. By adding ombudsmen and giving each a smaller territory tocover, we hope to foster more personal working relationships and provide greateraccessibility for our services. This will result in the reassignment of some of ourpresent staff. We have also designated a specific ombudsman to service supplierslocated outside of Region C whose patients live in our jurisdiction.
Alison SantoroOmbudsman
Vince TemplesOmbudsman
Sharon BriggmanOmbudsman
New Ombudsmen
Sharon Briggman is the new om-budsman for North Carolina . She willbe relocating to North Carolina in Julyof 1995. She has a B.A. degree fromNorth Carolina Central University(NCCU) in Durham, N.C. Sharon joinsPalmetto GBA with two years experi-ence in government claims auditingand has extensive knowledge of Medi-care policies. Prior to her position as aclaims auditor, Sharon was a corpo-rate trainer, where she was respon-sible for conducting in-service trainingand testing. As a customer servicerepresentative for CHAMPUS, Sharondealt directly with providers and ben-eficiaries, functioning as a liaison be-tween/for all parties. Sharon looksforward to using her public relationsabilities in her new position as theombudsman for North Carolina. Untilher relocation to North Carolina, shecan be reached at (803) 735-1034,Ext. 35760.
Alison Santoro, as noted on page94-206 of the DMERC Medicare Ad-visory, December, 1994 issue, is thenew ombudsman for southernFlorida, Puerto Rico and the VirginIslands*. She will be relocating toMiami, Florida, in April 1995 after afew months of intense training at theRegion C offices in Columbia, SouthCarolina. She looks forward to hermove to Florida and her challenge tosuccessfully support Palmetto GBAsuppliers. In the interim, Alison canbe reached at (803) 735-1034, Ext.35715.
*The territory of the Virgin Islands was inad-vertently left out of the description on page94-206 of the DMERC Medicare Advisory,December Issue.
Vince Temples, as noted on page94-206 of the DMERC MedicareAdvisory, December, 1994 issue, isthe new ombudsman covering Geor-gia and Tennessee. He is locatedin Atlanta, Georgia. Vince is excitedabout settling back into his nativestate and applying his experience toenhance Palmetto GBA and RegionC supplier relations. Vince can bereached at (404) 663-7644.

March 1995 DMERC Medicare Advisory Page 95-9
SC
KY
Claudia AmorteguiP.O. Box 100141Columbia, SC 29202-3141(803) 735-1034 Ext. 35714
Keith Smith10991-55 San Jose Blvd.Suite 139Jacksonville, FL 32223(904) 287-6860
AL
Vince TemplesP.O. Box 767337Roswell, GA 30076(404) 663-7644
Sheri ThompsonP.O. Box 100141Columbia, SC 29202-3141(803) 735-1034 Ext. 35726
Bobby SmithP.O. Box 9225Jackson, MS 39286(601) 366-4983
Alison SantoroP.O. Box 100141Columbia, SC 29202-3141(803) 735-1034, Ext. 35715(Will relocate to Florida,April 1995)
LA
MS
AR
Sharon BriggmanP.O. Box 100141Columbia, SC 29202-3141(803) 735-1034, Ext. 35760
NC
FL
FL
PR
VI
Out ofRegion C
To Be AnnouncedIn the interim, contact Sheri ThompsonP.O. Box 100141Columbia, SC 29202-3141(803) 735-1034 Ext. 35726
GATN
* Ombudsmen are those who investigate reported complaints, reports findings, and help to achieve equitablesettlements, through training and education of the supplier community.
The portion of the state (Florida) which the ombudsman covers.
OK
CO
NM
TX
PROFESSIONALRELATIONS ( Cont'd)
*Ombudsmen Addresses and Their Territories

Page 95-10 March 1995 DMERC Medicare Advisory
HEALTHMAINTENANCEORGANIZATIONS(HMOs) ANDMEDICARE
A medicare beneficiary may choose to have covered items and services furnished tohim/her through a Health Maintenance Organization (HMO). The HMO must have acontract with the Secretary of Health and Human Services (HHS) in order to participatein the Medicare program. A “Medicare” HMO must provide the same services for whicha beneficiary would be eligible to receive from Medicare if he were not an HMO enrollee.In other words, the beneficiary is still technically “on Medicare”; he has simply selecteda different carrier and is required to receive services according to that carrier’sarrangements. The beneficiary’s entitlement to Medicare is based on the same criteriawhether his health care expenses are payable by an HMO or by traditional Medicarecarriers and intermediaries.
There are two methods for determining if your patient may be enrolled in an HMO. First,during the initial interview with the patient, ask if the patient is enrolled in an HMO orif Medicare Part B is the patient's primary insurance carrier. Second, see if there is asticker attached to the Medicare identification card indicating that the beneficiary hashealth insurance benefits through an HMO. Some HMOs give their members HMOidentification stickers to apply to the medicare card, but the beneficiary may or may nothave one attached. Remember, the patient is still a Medicare beneficiary, and thestandard Medicare card is all that the Health Care Financing Administration (HCFA)issues.
Beneficiaries may enroll or disenroll in an HMO as often as they wish, or change fromone HMO to another, However, once the choice is made, enrollment in an HMO iseffective for at least one full month. Effective dates are the first day of the month throughand including the last day of the month of enrollment.
SPAN DATESNEEDED WHENFILING CLAIMS
Failure to use span dates, (i.e., a span of time between the from and to dates ofservice), will result in incorrect payment for the following items :
Parenteral and Enteral Nutrition Formula/Solution
B4150 - B4156 (Enteral)B4164 - B4216 (Parenteral)B5000 - B5200 (Parenteral)XX030 - XX076 (Enteral)
Supply Kits
B4034 - B4036 (Enteral)B4220 - B4224 (Parenteral)
Continuous Passive Motion (CPM) Device
E0935
Infusion Pump Supplies
K0110 - K0111

March 1995 DMERC Medicare Advisory Page 95-11
Please note the following changes in billing instructions for repairs of Durable MedicalEquipment (DME).
Effective for claims received on or after May 1, 1995, code E1350 represents labor timecharges only for DME repairs. Bill one unit for each hour of labor time. The allowancefor labor is $40.00 per hour or $40.00 per unit of labor.
Replacement parts must be billed with the appropriate HCPCS code that represent theitem or part being replaced, along with a pricing modifier (NU, UE, RR) and areplacement modifier (RP). If you are replacing a part that has not been assigned aspecific HCPCS code, use a miscellaneous HCPCS code (E1399, or K0108 forwheelchair parts) to bill each part. Repairs are only reimbursed for equipmentpurchased by the Medicare beneficiary. Therefore, each claim for repair chargesshould indicate that the patient owns the equipment. If a claim is being submitted forlabor charges only, the claim should indicate the type of equipment being repaired (i.e.repair of patient owned "wheelchair").
Itemization must accompany each claim that contains miscellaneous codes forreplacement parts.
Example One : Two hours of labor were performed on an electric wheelchair. Theelevating legrests, a caster pin lock, a belt for the motor and a posterior pad for the headrest are replaced. The claim should be billed as follows:
Itemized List of Miscellaneous PartsLINE 4 - Belt for motor, 48 inches (give manufacturer’s name and model # of chair)LINE 5 - Posterior pad for the headrest (give manufacturer’s name and model # ofchair)
Example Two: One hour of labor is performed on a TENS unit. The lead wires arereplaced. This claim should be billed as follows:
(NO ITEMIZED LIST NECESSARY)
Example Three:1 1/2 hours of labor is performed on a seat lift mechanism. A motorand bolt are replaced. The claim should be billed as follows:
Itemized List of Miscellaneous PartsLINE 2 - Motor for electric mechanism (give type and brand name)LINE 3 - Bolt (give type and brand name)
TIPS:t Until May 1, 1995, you may continue to follow instructions provided in the
Repair policy on page 15.57 of the DMEPOS Supplier Manual or you mayimmediately begin following the procedures described above.
t When billing labor hours, if the time is 30 minutes or longer, round up tothe nearest hour.
DURABLE MEDICALEQUIPMENT (DME)REPAIR CLAIMS

Page 95-12 March 1995 DMERC Medicare Advisory
CROSSOVER UPDATE
Medigap Policies
Palmetto Government Benefits Administrators (Palmetto GBA) has negotiated agree-ments with all state Medicaid agencies within Region C to provide for the automaticcrossover of claim information.
Your Medicare remittance will contain an indicator which will identify each Medicareclaim that Palmetto GBA has forwarded to a Medicaid fiscal agent.
A Medigap policy meets the statutory definition of a "Medicare supplemental policy"contained in Section 1882(g)(1) of Title XVIII of the Social Security Act. It is a healthinsurance policy or other health benefit plan offered by a private entity to thosepersons entitled to Medicare benefits and is specifically designed to supplementMedicare benefits. It fills in some of the "gaps" in Medicare coverage by providingpayment for some of the charges for which Medicare does not have responsibility dueto the applicability of deductibles, coinsurance amounts, or other limitations imposedby Medicare. It does not include limited benefit coverage available to Medicarebeneficiaries such as "specified disease" or "hospital indemnity" coverage. Also, itexplicitly excludes a policy or plan offered by an employer to employees or formeremployees, as well as that offered by a labor organization to members or formermembers.
The Medigap crossover process eliminates the need for beneficiaries or participatingproviders to file separate claims to Medigap insurers. Palmetto GBA will automaticallytransmit claim information to Medigap insurers when the beneficiary elects to assigntheir Medigap benefits to a participating provider.
Your Medicare remittance will contain an indicator which will identify each Medicareclaim that Palmetto GBA has forwarded to a Medigap insurer. To ensure that PalmettoGBA has the necessary information to effect this Medigap claim crossover, you shouldadhere to the claims filing instructions that follow.
For paper claims submission, the following information must be completed to ensureautomatic crossover claims to Medigap insurers. If this required information ismissing or incomplete, no transfer of claim information will occur.
Item 9: Enter the last name, first name, and the middle initial of the enrolleein the Medigap policy, if it is different from that shown in Item 2 [of theHCFA-1500 (12/90) form]. Otherwise, enter the word SAME. If theMedigap benefits are not assigned, leave blank.
NOTE: Participating suppliers are to complete Item 9 and its subdivisions onlywhen the beneficiary wishes to assign his or her benefits under aMedigap policy to the participating supplier.
Item 9a: Enter the policy and/or group number of the Medigap enrolleepreceded by “MEDIGAP.”
Item 9b: Enter the Medigap enrollee’s birth date and sex.
Item 9c: Enter the claims processing address for the Medigap insurer.
NOTE: Leave Item 9c blank only if an Other Carrier Name and Address(OCNA) number, which is a carrier-assigned unique identifier of aMedigap insurer, appears in Item 9d. For use of the OCNA numberin Item 9d, please see page 94-191-195 of this DMERC MedicareAdvisory.
Item 9d: Enter the Medigap insurer's OCNA number. Enter the name of theMedigap enrollee's insurance company only when it is not available onthe OCNA list.

March 1995 DMERC Medicare Advisory Page 95-13
CROSSOVER UPDATE(Cont'd)
For Electronic Media Claim (EMC) submission, the following information must becompleted to ensure automatic crossover claims to Medigap insurers. If this requiredinformation is missing or incomplete, no transfer of claim information will occur.
Data Field: DA0.04 Should contain an “I” to indicate Medigap, MSP orMedicaid
Data Field: DA0.06 Should contain “MG”Data Field: DA0.07 Should contain the first five positions of the OCNA
Number which is the other carrier-assigned uniqueidentifier found on pages 94-191-195
Data Field: DA0.08 Should contain the last four* positions of the OCNANumber which is the other carrier-assigned uniqueidentifier found on pages 94-191-195
Data Field: DA0.18 Should contain the Medigap policy number
Use of the OCNA number will automate the crossover process for both paper copy andelectronic claims. Please refer to pages 94-192-195 of the DMERC MedicareAdvisory , September 1994 issue, for an updated OCNA list. OCNA information is tobe used in Item 9d of the HCFA-1500 (12/90) form or for electronic claim submissionuse Data Field DA0.07 and DA0.08.
* Data Field DA0.08 has been corrected to read "last four" instead of "first five."
The following is a list of commonly used Crossover Remark codes and theirdefinitions as found on remittance notices.
Code Description
M The claim information is also being forwarded to the patient's supplementalinsurer. Send any questions regarding supplemental benefits to them.
G The claim information has also been forwarded to Medicaid for review.
@ Information was not sent to the Medigap insurer due to incorrect/invalidinformation you submitted concerning that insurer. Please verify yourinformation and submit your secondary claim directly to that insurer.
& Because Medigap benefits were assigned, this claim was sent to theMedigap insurer.
Identification ofCrossover RemarkCodes
Complementary/Supplemental Policies
Non-Medigap Medicare Supplemental policies are Medicare supplement policies thatdo not meet the definition of Medigap policies. Often these policies are referred to asComplementary Coverage policies.
Do not list these Non-Medigap Medicare Supplemental policies on the HCFA-1500(12/90) form. If we have an agreement with a Non-Medigap Medicare Supplementalinsurer, Palmetto GBA will automatically forward the Medicare claim information tothat insurer and indicate that we did so on your Medicare remittance.
The most current list of these insurers as of February, 1995 is shown below.
Acordia Senior of the Southeast, Inc.c/o BCBS of Kentucky
Aetna Life and Casualty InsuranceAmerican Postal Workers UnionAmerican Republic InsuranceBCBS of AlabamaBCBS of ArkansasBCBS of ColoradoBCBS of FloridaBCBS of LouisianaBCBS of MichiganBCBS of New MexicoBCBS of North CarolinaBCBS of OklahomaBCBS of South Carolina
BCBS of TexasGovernment Employee
Hospital AssociationGroup Health IncorporatedHumana Health Care PlanKirke-Van Orsdel, Inc.Mutual of OmahaNational Association of Letter CarriersOlympic HealthPrudential (AARP)Union Fidelity (ASO) American GeneralUnited American Insurance CompanyUSAA Life Insurance CompanyUSAble Life Insurance

Page 95-14 March 1995 DMERC Medicare Advisory
t When submitting paper claims, please type the information on the claim form. Iftyping is not possible, please be sure to print the information on the claim formlegibly. This will help to ensure that the correct information is being consideredfor payment.
t When preparing a paper claim for submission, please refrain from placinginformation in the upper right-hand corner of a HCFA-1500 (12/90) form. Thisspace on the claim form is reserved for the placement of a document controlnumber.
t Wheelchair options and accessories, including accessories coded with K0108,as well as nebulizer, CPAP and suction pump accessories coded K0168 - K0192,are categorized as inexpensive and routinely purchased. Claims for accessoriesmust include one of the following pricing modifiers as appropriate:
NU - New equipmentRR - Initial rental (use the RR modifier when DME is to be rented)UE - Used durable medical equipment
t Separate reimbursement will be allowed by the DMERCs for a humidifier, as longas the CPAP device is covered. Suppliers who bill for this equipment for existingCPAP patients should submit their claims using HCPCS code E0601 for theCPAP (if appropriate) and HCPCS code K0268 for the humidifier. The humidifierbilled for an existing CPAP patient, after the initial issue of the CPAP, can bereimbursed as a purchase. Rentals can be reimbursed up to the purchaseallowance. Code K0193 (CPAP with humidifier) is used only for newly placedCPAPs with humidifier. Pricing for code K0268 can be found on page 95-38 of thisadvisory. (Note: K0268 requires a pricing modifier, NU, UE or RR.)
t When billing the DMERC for injectable Ganciclovir, administered through an IVinfusion pump, use the HCPCS code J1570, Injection ganciclovir sodium, 500 mg,(Cytovene). Do not continue to use the Not Otherwise Classified (NOC) codeJ7799, as this will cause delays in claim processing.
t For those claims which require a completed Certificate of Medical Necessity(CMN), please be sure to complete all the sections of the CMN including thebeneficiary information. Thoroughly completing all of the information on the CMNwill help to expedite the processing of your claims.
t Refer to page 94-11 and 94-12 of the DMERC Medicare Advisory, January issue,for clarification on initial CMN versus revised CMN. Only one initial CMN can besubmitted and accepted either electronically or on paper. Any correction must bemarked as "Revision" with the corrected information and the initial start date.
CLAIM FILINGREMINDERS
PUERTO RICOPOSTALINFORMATION
Palmetto GBA has recently become aware of incorrect postal information on claimssubmitted for beneficiaries who reside in Puerto Rico. According to the Puerto RicanPostal Service, there are only four acceptable ways to specify Puerto Rican addresses.Please submit claims using the correct address format, as noted below.
1. Use HC (highway contract) followed by a number, then Box followed by a number.For Example: Luis Rodriguez Ortiz
HC 435 Box 1901Ponce, PR 00926
2. Use RR (rural route) followed by a number, then Box followed by a number.For Example: Isabela Gómez Cabrera
RR 688 Box 435Bayamón, PR 00947
3. Use the street (calle, avenida) address followed by a number on the first addressline, then urbanización (subdivision) followed by a name on the second addressline.
For Example: Gloria Ortega de MartínezCalle Bolivar 32Urb. Los CedrosSan Juan, PR 00978
4. Use a P.O. Box just as in the United States.For Example: Carlos Cortés Santiago
P.O. Box 1599Guayama, PR 00784-1599
CMN FilingReminders

March 1995 DMERC Medicare Advisory Page 95-15
Providing answers to your questions/concernson an on-going basis.
These questions were submitted to Palmetto GBA by Region C suppliers, and the answers are being published so thatall may benefit.
1. Q Are bandage contact lenses covered by Palmetto GBA?A No. However, when contact lenses used for corneal bandages are applied in a physician's office, they are
covered by Medicare as a supply incident to a physician's service. Payment for bandage contact lenses isusually included in the allowance for the physician's service.
2. Q Why doesn't the DMERC publish pricing for drugs and medication?A Pricing for drugs and medications is always updated quarterly, and sometimes as often as monthly. Therefore,
provision of current allowances for drugs and medications is not feasible in a quarterly publication.
3. Q When can electric wheelchairs that are in the capped rental category be purchased?A Electric wheelchairs in the capped rental category can only be purchased at the time of issue, or beginning with
the tenth month of rental. They may not be purchased at any other time during the rental period.
4. Q What type of documentation should be submitted to obtain prior authorization?A The DMERCs prefer the physician submit a completed DMERC Certificate of Medical Necessity (CMN) to
request prior authorization for the item.
5. Q Does Palmetto GBA need to be notified if a beneficiary changes suppliers? Does the new supplier have to filea new CMN?
A No. Palmetto GBA does not need to receive notice if the beneficiary changes suppliers. If a change in supplierhas occurred, a new initial CMN is not required. CMN's and recertifications provided by the previous supplierare acceptable for the new supplier's claims. However, it is the responsibility of the new supplier to obtain acopy of the beneficiary's current CMN prior to submitting claims.
6. Q Does Palmetto GBA cover paclitaxel (taxol)?A No. Palmetto GBA does not cover paclitaxel (taxol). Taxol should be administered under the supervision of
a physician experienced in the use of cancer chemotherapeutic agents. Since it is unsafe to administer taxolin the home setting, it cannot be covered for home infusion therapy.
Q A&
ANTI-FRAUD UNIT
Supplier Sanctions
The following suppliers are being excluded from participation in the Title XVIII(Medicare) program, per Office of Inspector General, Office of Investigations, P.O.Box 2288, Atlanta, GA 30301.
South Carolina
James L. Altman Specialty: Medical Doctor819 Carn Street DOB: 09/17/24Walterboro, SC 29488-1057 Period of Exclusion: Indefinite
John D. Stellwagen Specialty: D.P.M.210 N. Pine Street DOB: 11/08/55Seneca, SC 29678 Period of Exclusion: Indefinite
Medcare City Pharmacy Specialty: DME SupplierP.O. Box 155 DOB: N/AClover, SC 29710 Period of Exclusion: 5 Years
Alex C. Garrett Specialty: D.C.1097 W. Butler Rd. DOB: 12/05/58Greenville, SC 29607 Period of Exclusion: Indefinite
Anti-Fraud Hot-Line (803) 788-5414

Page 95-16 March 1995 DMERC Medicare Advisory
JULIAN DATEREFERENCE
The Claim Control Number (CCN) is a unique number the DMERCs assign to eachclaim for tracking purposes. The 14 digits of each CCN can provide you with processinginformation (see page 94-227 of the DMERC Medicare Advisory, December, 1994issue for a more specific breakdown). The first five digits identify the year and the juliandate the claim was received by Palmetto GBA. To help you identify the date your claimwas received, the following julian date calendar is provided.
Day Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Day1 001 032 060 091 121 152 182 213 244 274 305 335 12 002 033 061 092 122 153 183 214 245 275 306 336 23 003 034 062 093 123 154 184 215 246 276 307 337 34 004 035 063 094 124 155 185 216 247 277 308 338 45 005 036 064 095 125 156 186 217 248 278 309 339 56 006 037 065 096 126 157 187 218 249 279 310 340 67 007 038 066 097 127 158 188 219 250 280 311 341 78 008 039 067 098 128 159 189 220 251 281 312 342 89 009 040 068 099 129 160 190 221 252 282 313 343 910 010 041 069 100 130 161 191 222 253 283 314 344 1011 011 042 070 101 131 162 192 223 254 284 315 345 1112 012 043 071 102 132 163 193 224 255 285 316 346 1213 013 044 072 103 133 164 194 225 256 286 317 347 1314 014 045 073 104 134 165 195 226 257 287 318 348 1415 015 046 074 105 135 166 196 227 258 288 319 349 1516 016 047 075 106 136 167 197 228 259 289 320 350 1617 017 048 076 107 137 168 198 229 260 290 321 351 1718 018 049 077 108 138 169 199 230 261 291 322 352 1819 019 050 078 109 139 170 200 231 262 292 323 353 1920 020 051 079 110 140 171 201 232 263 293 324 354 2021 021 052 080 111 141 172 202 233 264 294 325 355 2122 022 053 081 112 142 173 203 234 265 295 326 356 2223 023 054 082 113 143 174 204 235 266 296 327 357 2324 024 055 083 114 144 175 205 236 267 297 328 358 2425 025 056 084 115 145 176 206 237 268 298 329 359 2526 026 057 085 116 146 177 207 238 269 299 330 360 2627 027 058 086 117 147 178 208 239 270 300 331 361 2728 028 059 087 118 148 179 209 240 271 301 332 362 2829 029 088 119 149 180 210 241 272 302 333 363 2930 030 089 120 150 181 211 242 273 303 334 364 3031 031 090 151 212 243 304 365 31
Day Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Day1 001 032 061 092 122 153 183 214 245 275 306 336 12 002 033 062 093 123 154 184 215 246 276 307 337 23 003 034 063 094 124 155 185 216 247 277 308 338 34 004 035 064 095 125 156 186 217 248 278 309 339 45 005 036 065 096 126 157 187 218 249 279 310 340 56 006 037 066 097 127 158 188 219 250 280 311 341 67 007 038 067 098 128 159 189 220 251 281 312 342 78 008 039 068 099 129 160 190 221 252 282 313 343 89 009 040 069 100 130 161 191 222 253 283 314 344 910 010 041 070 101 131 162 192 223 254 284 315 345 1011 011 042 071 102 132 163 193 224 255 285 316 346 1112 012 043 072 103 133 164 194 225 256 286 317 347 1213 013 044 073 104 134 165 195 226 257 287 318 348 1314 014 045 074 105 135 166 196 227 258 288 319 349 1415 015 046 075 106 136 167 197 228 259 289 320 350 1516 016 047 076 107 137 168 198 229 260 290 321 351 1617 017 048 077 108 138 169 199 230 261 291 322 352 1718 018 049 078 109 139 170 200 231 262 292 323 353 1819 019 050 079 110 140 171 201 232 263 293 324 354 1920 020 051 080 111 141 172 202 233 264 294 325 355 2021 021 052 081 112 142 173 203 234 265 295 326 356 2122 022 053 082 113 143 174 204 235 266 296 327 357 2223 023 054 083 114 144 175 205 236 267 297 328 358 2324 024 055 084 115 145 176 206 237 268 298 329 359 2425 025 056 085 116 146 177 207 238 269 299 330 360 2526 026 057 086 117 147 178 208 239 270 300 331 361 2627 027 058 087 118 148 179 209 240 271 301 332 362 2728 028 059 088 119 149 180 210 241 272 302 333 363 2829 029 060 089 120 150 181 211 242 273 303 334 364 2930 030 090 121 151 182 212 243 274 304 335 365 3031 031 091 152 213 244 305 366 31
Julian Date CalendarPerpetual
Julian Date CalendarFor Leap Years Only(i.e. 1992, 1996, etc.)
March 1995 DMERC Medicare Advisory Page 95-17
ELECTRONIC DATAINTERCHANGE (EDI)
Electronic MailboxDirectory
When electronic submitters transmit files to Palmetto GBA, their claims are depositedinto individual electronic mailboxes where Palmetto GBA will retrieve them. Thesesame mailboxes are used for the deposit and retrieval of claim reports and electronicremittance notices (ERNs). By requesting a mailbox directory, submitters candetermine the exact content of their mailboxes. Your communications software shouldbe programmed to request the mailbox directory.
The figure below shows an example of a typical mailbox which contains:t an electronic remittance notice ready for retrieval;t a claim file not yet cycled by Palmetto GBA;t a claim receipt listing ready for retrieval.
t Mailbox ID is the unique six-digit code assigned to each submitter.t Batch # is an internal number Palmetto GBA assigns to each file in the mailbox.t # of Records refers to the number of data segments in the file.
t Batch ID is a system code that differentiates between claims (DCLMNSF), claimreports (DRPTCLM), and ERNs (DERNNSF).
t Time is the military time that the action began, e.g., the claims were submitted orthe report was placed in the mailbox.
t JDate is the Julian date of the transaction.t Status codes are as follows:
A - File added via Advantis or an off-line utility.D - Ready to delete. This file has been completely processed.E - Extracted. Palmetto GBA has extracted this data from the mailbox.I - Incomplete transmission. The file should be resubmitted.R - Ready to be retrieved by the submitter.S - SPC. File added via Software Protocol Converter.T - Transmitted. The file has been retrieved by the submitter.
Electronic billers may obtain more information by contacting the EDI Help Line.
EDI Help Line - (803) 788-9751
Electronic Submissionof Medicare SecondaryPayor (MSP) Claims
Most vendor software, Palmetto GBA’s PACES included, allows you to enjoyelectronic submission of your Medicare Secondary Payor (MSP) claims. First,contact your software vendor and ensure that your software will allow you tosubmit MSP claims. Then be sure that you have included the information outlinedbelow in your primary and secondary insurance records. Your software shouldcontain instructions to guide you through submitting an MSP claim. If you areuncertain as to where in your software the fields referenced below are and thename your particular software gives them, consult your software vendor foradvice.
For MSP claims, all required Medicare insurance information is to be entered inthe Secondary Insurance record. The difference in submitting MSP claimselectronically is that the non-Medicare primary insurance information is entered inthe Primary Insurance. For MSP claims, the Primary Insurance record shouldcontain all required information about the beneficiary’s non-Medicare primaryinsurance and how much that primary insurance has/has not paid toward satisfy-ing the claim charges.

Page 95-18 March 1995 DMERC Medicare Advisory
Electronic Submissionof MSP Claims(Cont'd.)
Information required on the Primary Insurance Record when the beneficiary has anon-Medicare primary insurer includes:
DA0-01, Field 4 Claim Filing Indicator (Please check with your software vendorto determine if your software automatically enters an “I” in thisfield for you.)
DA0-01, Field 5 Source of Pay Code (Most software vendors automaticallyenter these codes, linking them to the Insurance Type codeentered in the DA0-01, Field 6. Consult your software vendorto determine how your software does this.)
DA0-01, Field 6 Insurance Type CodeDA0-01, Field 9 Payor Name
(“Payor” refers in this instance to the beneficiary’s non-Medicare primary insurance carrier)
DA0-01, Field 10 Group NumberDA0-01, Field 11 Group NameDA0-01, Field 16 Patient Signature SourceDA0-01, Field 17 Patient Relationship to InsuredDA0-01, Field 18 Insured Identification NumberDA0-01, Field 19 Insured Last NameDA0-01, Field 20 Insured First NameDA0-01, Field 21 Insured Middle Initial (Optional)DA0-01, Field 23 Insured SexDA0-01, Field 24 Insured Date of BirthDA1-01, Field 4 Payor Address Line 1DA1-01, Field 5 Payor Address Line 2 (Optional)DA1-01, Field 6 Payor CityDA1-01, Field 7 Payor StateDA1-01, Field 8 Payor Zip CodeDA1-01, Field 9 Disallowed Cost Containment Amount (From EOMB)DA1-01, Field 10 Disallowed Other Amount (From EOMB)DA1-01, Field 11 Allowed Amount (From EOMB)DA1-01, Field 12 Deductible Amount (From EOMB)DA1-01, Field 13 Coinsurance Amount (From EOMB)DA1-01, Field 14 Payor Paid Amount (From EOMB)DA1-01, Field 16 Adjudication Indicator 1 (Conditional)DA1-01, Field 17 Adjudication Indicator 2 (Conditional)DA1-01, Field 18 Adjudication Indicator 3 (Conditional)DA1-01, Field 24 Balance Due (From EOMB)DA2-01, Field 4 Insured Address Line 1DA2-01, Field 5 Insured Address Line 2 (Optional)DA2-01, Field 6 Insured CityDA2-01, Field 7 Insured StateDA2-01, Field 8 Insured Zipcode
When entering the beneficiary’s Medicare information in the Secondary InsuranceRecord, enter the Medicare required information as you would if it were in thePrimary Insurance Record, but be sure to enter a Medicare Secondary ReasonCode in the DA0-02, Field 6, instead of an Insurance Type Code.
Medicare Secondary Reason Code (DA0-02, Field 6)
This field indicates in the Secondary Insurance Record, the reason that Medicare isthe beneficiary’s secondary insurance. Valid codes are:
12 - Working Aged Beneficiary/Spouse with Employer Group Health Plan13 - ESRD Beneficiary in the 12 Month Coordination Period with an Employer’s
Group Health Plan14 - No Fault Insurance, Including Auto/Other15 - Worker’s Compensation Insurance16 - PHS or Other Federal Agency41 - Black Lung42 - VA43 - Disabled Beneficiary Under Age 65 With LGHP44 - Any Liability Insurance

March 1995 DMERC Medicare Advisory Page 95-19
LYMPHEDEMAPUMPS/PNEUMATICCOMPRESSORS
It has been brought to our attention that there is some confusion throughout thesupplier community as to which HCPCS code should be used to properly bill for thevarious lymphedema pumps available. The following grid is provided to offerclarification in this area.
Manufacturer/Brand Name Model Name/No. HCPCS Code
Bio Compressions Systems/Sequential Circulator 2000 E06513000 E06523001 E06523004 E0652
Huntleigh Flowplus (AC330) E0650Flowpress (AC300) E0651
Flowtron E0650Lymphatron E0651
Lymphatron(AC340) E0651Lymphatron Trio (AC350) E0652
Jobst/Extremity Pump Clinical Model E0650System 7000 E0650
System 7500 (II) E0651
Kendall Home Rx (5550) E0651
Lympha Press 103A E0651103M E0652
201A - Mini E0651201-M E0652
Talley/Hemaflow 2 Pump Intermittent E0650Sequential E0651
Talley/Multicom 100 E0650200 E0650300 E0651
300G E0652500 ('93 & '94 model) E0652 *
Talley/Multipulse 1000 E0652
Wright Linear Pump II E0652IV E0652
Chattanooga PresSsion E06514320 E06504322 E0650
Advantage 2100 E0652
Thera-Con Sequential E0652
* Talley/Multicom model '92 or before = E0651

Page 95-20 March 1995 DMERC Medicare Advisory
HCPCS CODESREQUIRING A CMN
A4311 Insertion tray without drainage bag with indwelling catheter, Foley type, two-way latex with coating(teflon, silicone, silicone elastomer or hydrophilic, etc.) 05.01
A4312 Insertion tray without drainage bag with indwelling catheter, Foley type, two-way, all silicone 05.01A4314 Insertion tray with drainage bag with indwelling catheter, Foley type, two-way latex with coating (Teflon, silicone,
silicone elastomer or hydrophilic, etc.) 05.01A4315 Insertion tray with drainage bag with indwelling catheter, Foley type, two-way, all silicone 05.01A4338 Indwelling catheter; Foley type, two-way latex with coating (Teflon, silicone, silicone elastomer, or hydrophilic, etc.) 05.01A4340 Indwelling catheter; specialty type, (e.g., coude, mushroom, wing, etc.) 05.01A4344 Indwelling catheter, Foley type, two-way, all silicone 05.01B4150 Category I, Semi-Synthetic: Intact, Protein/Protein Isolates, (100 calories = 1 unit) 10.01B4151 Enteral Nutrition Formulae, Category 1B, Blenderized: Intact, Protein/Protein, Isolates - Naturalized, (100 calories = 1 unit) 10.01B4152 Enteral Nutrition Formulae, Category II - Intact, Protein/Protein Isolates, (Calorically Dense), (100 calories = 1 unit) 10.01B4153 Enteral Nutrition Formulae, Category III, Hydrolyzed Protein/Amino Acid, (100 calories = 1 unit) 10.01B4154 Enteral Nutrition Formulae, Category IV: defined formula for special metabolic need, (100 calories=1 unit) 10.01B4155 Enteral Nutrition Formulae, Category V: modular components (protein, carbohydrates, fat) 100 calories = 1 unit 10.01B4156 Enteral Nutrition Formulae, Category VI - Standard, (100 calories = 1 unit) 10.01B4164 Parenteral Nutrition Solution, Dextrose, 50% or less (500ML = 1 unit) Home Mix 10.01B4168 Parenteral Nutrition Solution, Amino Acid, 3.5% or less (500 ML = 1 unit) Home Mix 10.01B4172 Parenteral Nutrition Solution, Amino Acid, 5.5% through 7% (500 ML = 1 unit) Home Mix 10.01B4176 Parenteral Nutrition Solution, Amino Acid, 7% through 8.5% (500 ML = 1 unit) Home Mix 10.01B4178 Parenteral Nutrition Solution, Amino Acid, Greater than 8.5% (500 ML = 1 unit) Home Mix 10.01B4180 Parenteral Nutrition Solution, Dextrose, Greater than 50% (500 ML = 1 unit) Home Mix 10.01B4184 Parenteral Nutrition Solution, Lipids, 10% with Administration set (500 ML = 1 unit) 10.01B4186 Parenteral Nutrition Solution, Lipids, 20% with Administration set (500 ML = 1 unit) 10.01B4189 Parenteral Nutrition Solution; Compounded Amino Acid & Carbohydrates with electrolytes, trace elements &
vitamins, including preparation, any strength, 10 to 51 grams of protein - Pre-Mix 10.01B4193 Parenteral Nutrition Solution; Compounded Amino Acid & Carbohydrates with electrolytes, trace elements &
vitamins, including preparation, any strength, 52 to 73 grams of protein - Pre-Mix 10.01B4197 Parenteral Nutrition Solution; Compounded Amino Acid & Carbohydrates with electrolytes, trace elements &
vitamins, including preparation, any strength, 74 to 100 grams of protein - Pre-Mix 10.01B4199 Parenteral Nutrition Solution; Compounded Amino Acid & Carbohydrates with electrolytes, trace elements &
vitamins, including preparation, any strength, over 100 grams of protein - Pre-Mix 10.01B4216 Parenteral Nutrition; Additives (Vitamins, Trace Elements & Electrolytes) Home Mix, per day 10.01B5000 Parenteral Nutrition Solution; Compounded Amino Acid & Carbohydrates with electrolytes, trace elements &
vitamins, including preparation, any strength, per gram, Renal, Aminosyn RF, Nephramine, Renamine Pre-Mix 10.01B5100 Parenteral Nutrition Solution; Compounded Amino Acid & Carbohydrates with electrolytes, trace elements &
vitamins, including preparation, any strength, per gram, Hepatic, Freamine HBC, Hepatamine - Pre-Mix 10.01B5200 Parenteral Nutrition Solution; Compounded Amino Acid & Carbohydrates with electrolytes, trace elements &
vitamins, including preparation, any strength, per gram, Stress-branch chains amino acids - Pre-Mix 10.01B9000 Enteral Nutrition Pump, no alarm 10.01B9002 Enteral Nutrition Pump, with alarm 10.01B9004 Parenteral Nutrition Pump - Portable 10.01B9006 Parenteral Nutrition Pump - Stationary 10.01E0180 Pressure pad, alternating, with pump 01.01E0181 Pressure pad, alternating, with pump, heavy duty 01.01E0194 Air-fluidized bed 01.01E0250 Hospital bed, fixed height, with any type side rails, with mattress 01.01E0251 Hospital bed, fixed height, with any type side rails, without mattress 01.01E0255 Hospital bed, variable height, hi-lo, with any type side rails, with mattress 01.01E0256 Hospital bed, variable height, hi-lo, with any type side rails, without mattress 01.01E0260 Hospital bed, semi-electric (head and foot adjustment), with any type side rails, with mattress 01.01E0261 Hospital bed, semi-electric (head and foot adjustment), with any type side rails, without mattress 01.01E0265 Hospital bed, total electric, (head, foot and height adjustments), with any type side rails, with mattress 01.01E0266 Hospital bed, total electric (head, foot and height adjustments), with any type side rails, without mattress 01.01E0277 Alternating Pressure Mattress 01.01E0290 Hospital Bed, fixed height, without side rails, with mattress 01.01E0291 Hospital bed, fixed height, without side rails, without mattress 01.01E0292 Hospital bed, variable height, hi-lo, without side rails, with mattress 01.01E0293 Hospital bed, variable height, hi-lo, without side rails, without mattress 01.01E0294 Hospital bed, semi-electric (head and foot adjustment), without side rails, with mattress 01.01E0295 Hospital bed, semi-electric (head and foot adjustment), without side rails, without mattress 01.01E0296 Hospital bed, total electric (head, foot and height adjustments), without side rails, with mattress 01.01E0297 Hospital bed, total electric (head, foot and height adjustments), without side rails, without mattress 01.01
DMERCHCPCS HCPCS CMNCODE DESCRIPTION REQUIRED
The following HCPCS codes are the only codes that require a Certificate of MedicalNecessity (CMN). The specific CMN required for each code is indicated on this chart.CMNs are required per code, not per patient. When electronically submitting claims thatrequire a CMN, the specific CMN record for each code must also be transmitted with thatclaim to Palmetto Government Benefits Administrators. When submitting paper versions ofthe claims, be sure to include each code which requires a CMN, on the CMN. If additionalspace is required to list the codes, use the Warranty Section of the CMN to continue yourlisting. This chart replaces all previously published copies of this information.

March 1995 DMERC Medicare Advisory Page 95-21
DMERCHCPCS HCPCS CMNCODE DESCRIPTION REQUIRED
E0424 Stationary compressed gaseous oxygen system, rental; includes contents (per unit), regulator,flow meter, humidifier, nebulizer, cannula or mask, and tubing; one unit = 50 cu. ft. 484
E0431 Portable gaseous oxygen system, rental; includes regulator, flowmeter, humidifier, cannula or mask, and tubing 484E0434 Portable liquid oxygen system, rental; includes portable container, supply reservoir, humidifier, flowmeter, refill adaptor,
contents gauge, cannula or mask, and tubing 484E0439 Stationary liquid oxygen system, rental; includes use of reservoir, contents (per unit), regulator, flowmeter,
humidifier, nebulizer, cannula or mask, and tubing; one unit = 50 lbs. 484E0441 Oxygen contents, gaseous, per unit (for use with owned stationary gaseous stationary systems or when both a
stationary and portable gaseous system are owned; one unit = 50 cu. ft.) 484E0442 Oxygen contents, liquid, per unit (for use with owned liquid stationary systems or when both a stationary and
portable liquid system are owned; one unit = 10 lbs.) 484E0443 Portable oxygen contents, gaseous, per unit (for use only with portable gaseous systems and no
stationary gas or liquid system is used; one unit = 5 cu. ft.) 484E0444 Portable oxygen contents, liquid, per unit (for use only with portable liquid systems when no stationary gas or
liquid system is used; one unit = 1 lb.) 484E0600 Suction pump, home model, portable 03.01E0601 Continuous airway pressure (CPAP) device 03.01E0607 Home blood glucose monitor 09.01E0609 Blood glucose monitor, with special features, (e.g., voice synthesizers, automatic timers, etc.) 09.01E0627 Seat lift mechanism incorporated into a combination lift-chair mechanism 07.01E0628 Separate seat lift mechanism for use with patient owned furniture - electric 07.01E0629 Separate seat lift mechanism for use with patient owned furniture - non-electric 07.01E0650 Pneumatic compressor, non-segmental home model 04.01E0651 Pneumatic compressor, segmental home model without calibrated gradient pressure 04.01E0652 Pneumatic compressor, segmental home model with calibrated gradient pressure 04.01E0655 Non-segmental pneumatic appliance for use with pneumatic compressor, half arm 04.01E0660 Non-segmental pneumatic appliance for use with pneumatic compressor, full leg 04.01E0665 Non-segmental pneumatic appliance for use with pneumatic compressor, full arm 04.01E0666 Non-segmental pneumatic appliance for use with pneumatic compressor, half leg 04.01E0667 Segmental pneumatic appliance for use with pneumatic compressor, full leg 04.01E0668 Segmental pneumatic appliance for use with pneumatic compressor, full arm 04.01E0671 Segmental gradient pressure pneumatic appliance, full leg 04.01E0672 Segmental gradient pressure pneumatic appliance, full arm 04.01E0673 Segmental gradient pressure pneumatic appliance, half leg 04.01E0720 TENS, two-lead, localized stimulation 06.01E0730 TENS, four-lead, larger area/multiple nerve stimulation 06.01E0731 Form fitting conductive garment for delivery of TENS or NINES (with conductive fibers separated from the patients
skin by layers of fabric) 06.01E0747 Osteogenesis stimulator, non-invasive 04.01E0776 IV pole 09.01E0781 Ambulatory infusion pump, single or multiple channels, with administrative equipment, worn by patient 09.01E0791 Parenteral Nutrition infusion pump, stationary, single or multi-channel 09.01E1050 Fully-reclining wheelchair, fixed full length arms, swing away detachable elevating leg rests 02.01E1060 Fully-reclining wheelchair, detachable arms, desk or full length, swing away detachable elevating leg rests 02.01E1065 Power attachment (to convert any wheelchair to motorized wheelchair) (e.g., Solo) 02.01E1070 Fully-reclining wheelchair, detachable arms, desk or full length, swing away detachable foot rests 02.01E1083 Hemi-wheelchair, fixed full length arms, swing away detachable elevating leg rests 02.01E1084 Hemi-wheelchair, detachable arms, desk or full length arms, swing away detachable elevating leg rests 02.01E1085 Hemi-wheelchair, fixed full length arms, swing away detachable footrests 02.01E1086 Hemi-wheelchair, detachable arms, desk or full length, swing away detachable foot rests 02.01E1087 High strength lightweight wheelchair, fixed full length arms, swing away detachable elevating leg rests 02.01E1088 High strength lightweight wheelchair, detachable arms, desk or full length, swing away detachable elevating leg rests 02.01E1089 High strength lightweight wheelchair, fixed full length arms, swing away detachable foot rests 02.01E1090 High strength lightweight wheelchair, detachable arms, desk or full length, swing away detachable foot rests 02.01E1091 Youth wheelchair, any type 02.01E1092 Wide heavy duty wheelchair, detachable arms, desk or full length, swing away detachable elevating leg rests 02.01E1093 Wide heavy duty wheelchair, detachable arms, desk or full length, swing away detachable foot rests 02.01E1100 Semi-reclining wheelchair, fixed full length arms, swing away detachable elevating leg rests 02.01E1110 Semi-reclining wheelchair, detachable arms, desk or full length, elevating leg rests 02.01E1130 Standard wheelchair, fixed full length arms, fixed or swing away detachable foot rests 02.01E1140 Wheelchair, detachable arms, desk or full length, swing away detachable foot rests 02.01E1150 Wheelchair, detachable arms, desk or full length, swing away detachable elevating leg rests 02.01E1160 Wheelchair, fixed full length arms, swing away detachable elevating leg rests 02.01E1170 Amputee wheelchair, fixed full length arms, swing away detachable elevating leg rests 02.01E1171 Amputee wheelchair, fixed full length arms, without foot rests or leg rests 02.01E1172 Amputee wheelchair, detachable arms, desk or full length, without foot rests or leg rests 02.01E1180 Amputee wheelchair, detachable arms, desk or full length, swing away detachable foot rests 02.01E1190 Amputee wheelchair, detachable arms, desk or full length, swing away detachable elevating leg rests 02.01E1195 Heavy duty wheelchair, fixed full length arms, swing away detachable elevating leg rests 02.01E1200 Amputee wheelchair, fixed full length arms, swing away detachable foot rests 02.01E1210 Motorized wheelchair, with micro-switch control, fixed full length arms, swing away detachable elevating leg rests 02.01E1211 Motorized wheelchair, with micro-switch control, detachable arms, desk or full length, swing away detachable
elevating legrests 02.01
HCPCS Codes Requiring A CMN (Cont'd)

Page 95-22 March 1995 DMERC Medicare Advisory
DMERCHCPCS HCPCS CMNCODE DESCRIPTION REQUIRED
E1212 Motorized wheelchair, with micro-switch control, fixed full length arms, swing away detachable foot rests 02.01E1213 Motorized wheelchair, with micro-switch control, detachable arms, desk or full length, swing away detachable foot rests 02.01E1220 Wheelchair; specially sized or constructed, (indicate brand name, model number, if any) and justification 02.01
E1221 Special-sized wheelchair with fixed arms, foot rests 02.01E1222 Special-sized wheelchair with fixed arms, elevating leg rests 02.01E1223 Special-sized wheelchair with detachable arms, foot rests 02.01E1224 Special-sized wheelchair with detachable arms, elevating leg rests 02.01E1230 Power operated vehicle (three or four wheel nonhighway) Specify brand name and model number 07.01E1240 Lightweight wheelchair, detachable arms, desk or full length, swing away detachable elevating leg rests 02.01E1250 Lightweight wheelchair, fixed full length arms, swing away detachable foot rests 02.01E1260 Lightweight wheelchair, detachable arms, desk or full length, swing away detachable foot rests 02.01E1270 Lightweight wheelchair, fixed full length arms, swing away detachable elevating leg rests 02.01E1280 Heavy duty wheelchair, detachable arms, desk or full length, elevating leg rests 02.01E1285 Heavy duty wheelchair, fixed full length arms, swing away detachable foot rests 02.01E1290 Heavy duty wheelchair, detachable arms, desk or full length, swing away detachable foot rests 02.01E1295 Heavy duty wheelchair, fixed full length arms, elevating leg rests 02.01E1400 Oxygen concentrator, manufacturer specified maximum flow rate does not exceed 2 liters per minute,
at 85 percent or greater concentration 484E1401 Oxygen concentrator, manufacturer specified maximum flow rate greater than 2 liters per minute, does not
exceed 3 liters per minute, at 85 percent or greater concentration 484E1402 Oxygen concentrator, manufacturer specified maximum flow rate greater than 3 liters per minute,
does not exceed 4 liters per minute, at 85 percent or greater concentration 484E1403 Oxygen concentrator, manufacturer specified maximum flow rate greater than 4 liters per minute,
does not exceed 5 liters per minute, at 85 percent or greater concentration 484E1404 Oxygen concentrator, manufacturer specified maximum flow rate greater than 5 liters per minute,
at 85 percent or greater concentration 484E1405 Oxygen and water vapor enriching system with heated delivery 484E1406 Oxygen and water vapor enriching system without heated delivery 484J2920 Methylprednisolone sodium succinate up to 40 mg. 08.01J2930 Methylprednisolone sodium succinate up to 125 mg. 08.01J7500 Azathioprine, (e.g., Imuran) - oral, tab, 50 mg., 100s ea 08.01J7501 Azathioprine, (e.g., Imuran) - parenteral, vial, 100 mg, 20 ml ea 08.01J7502 Cyclosporine, (e.g., Sandimmune) - oral, sol; 100 mg/ml, 50 ml each 08.01J7503 Cyclosporine, (e.g., Sandimmune) - parenteral, amp, IV, 250 mg, 5 ml. 10S each 08.01J7504 Lymphocyte immune globulin, antitymocyte globulin, (e.g., Atgam) - parenteral, amp, 50 mg/ml, 5 ml each 08.01J7505 Monoclonal antibodies, (e.g., Muromonab CD3; Orthoclone) parenteral, amp, 5 mg/5 ml, 5 ml each 08.01J7506 Prednisone, any dosage, 100 tablets 08.01K0001 Standard wheelchair 02.01K0002 Standard hemi (low seat) wheelchair 02.01K0003 Lightweight wheelchair 02.01K0004 High strength, lightweight wheelchair 02.01K0005 Ultralightweight wheelchair 02.01K0006 Heavy duty wheelchair 02.01K0007 Extra heavy duty wheelchair 02.01K0008 Custom manual wheelchair /base 02.01K0009 Other manual wheelchair/base 02.01K0010 Standard-weight frame motorized/power wheelchair 02.01K0011 Standard-weight frame motorized/power wheelchair with programmable control parameters for
speed adjustment, tremor dampening, acceleration control and braking 02.01K0012 Lightweight portable motorized/power wheelchair 02.01K0013 Custom motorized/power wheelchair base 02.01K0014 Other motorized/power wheelchair base 02.01K0016 Detachable, adjustable height armrest, complete assembly, each 02.01K0017 Detachable, adjustable height armrest, base, each 02.01K0018 Detachable, adjustable height armrest, upper portion each 02.01K0020 Fixed, adjustable height armrest, pair 02.01K0022 Reinforced back upolstery 02.01K0025 Hook-on headrest extension 02.01K0028 Fully reclining back 02.01K0029 Reinforced seat upholstery 02.01K0030 Solid seat insert, planar seat, single density foam 02.01K0031 Safety belt/pelvic strap 02.01K0046 Elevating legrest, lower extension tube, each 02.01K0047 Elevating legrest, upper hanger bracket, each 02.01K0048 Elevating legrest, complete assembly 02.01K0050 Ratchet assembly 02.01K0053 Elevating footrests, articulating (telescoping), each 02.01K0101 One-arm drive attachment 02.01K0106 Arm trough, each 02.01K0119 Azathioprine - oral, tab, 50mg 08.01K0120 Azathioprine - parenteral, 100 mg. 08.01K0121 Cyclosporine 0 oral, 25 mg. 08.01
HCPCS Codes Requiring A CMN (Cont'd)

March 1995 DMERC Medicare Advisory Page 95-23
HCPCS Codes Requiring A CMN (Cont'd)
DMERCHCPCS HCPCS CMNCODE DESCRIPTION REQUIRED
K0122 Cyclosporine - parenteral, 250 mg 08.01K0123 Lymphocyte immune globulin, antithmocyte globuline - parenteral, 250 mg 08.01K0124 Monoclonal antibodies - parenteral, 5 mg 08.01K0125 Prednisone - oral, 5mg. 08.01K0148 Hydrogel dressing, each 05.01K0166 Methylprednisolone - oral, 4mg. 08.01K0167 Prednisolone - oral, 5 mg. 08.01K0193 CPAP device, with humidifier 03.01K0195 Elevating leg rest, pair (for use with capped rental wheelchair base) 02.01K0280 Extension drainage tubing, any type/length, with connector/adaptor, used with urinary leg bag or urostomy pouch, each 05.01K0284 External infusion pump, mechanical, reusable, for extended drug infusion 09.01L1900 Ankle-foot orthosis, (AFO), spring wire, dorsiflexion assist calf band 04.01L1920 AFO, single upright with static or adjustable stop, (Phelps or Perlstein type) 04.01L1930 AFO, custom fitted, plastic 04.01L1940 AFO, molded to patient model, plastic 04.01L1960 AFO, posterior solid ankle, molded to patient model, plastic 04.01L1980 AFO, single upright, free plantar dorsiflexion, solid stirrup, calf band/cuff, (single bar BK orthosis) 04.01L1990 AFO, double upright, free plantar dorsiflexion, solid stirrup, calf band/cuff, (double bar BK orthosis) 04.01L2000 Knee-ankle-foot orthosis, (KAFO), single upright, free knee, free ankle, solid stirrup, thigh and calf bands/cuffs,
(single bar AK orthosis) 04.01L2010 KAFO, single upright, free ankle, solid stirrup, thigh and calf bands/cuffs, (single bar AK orthosis), without knee joint 04.01L2020 KAFO, double upright, free knee, free ankle, solid stirrup, thigh and calf bands/cuffs, (double bar AK orthosis) 04.01L2030 KAFO, double upright, free ankle, solid stirrup, thigh and calf bands/cuffs, (double bar AK orthosis), without knee joint 04.01L2036 KAFO, full plastic, molded to patient model 04.01L2037 KAFO, full plastic, single upright, free-knee, molded to patient model 04.01L2038 KAFO, full plastic, without knee joint, multiaxis ankle, molded to patient model (lively orthosis or equal) 04.01L2102 AFO, fracture orthosis, tibial fracture cast orthosis, plaster type casting material, molded to patient 04.01L2104 AFO, fracture orthosis, tibial fracture cast orthosis, synthetic type casting material, molded to patient 04.01L2106 AFO, fracture orthosis, tibial fracture cast orthosis, thermoplastic type casting material, molded to patient 04.01L2108 AFO, fracture orthosis, tibial fracture cast orthosis, molded to patient model 04.01L2112 AFO, fracture orthosis, tibial fracture orthosis, soft custom fitted 04.01L2114 AFO, fracture orthosis, tibial fracture orthosis, semi-rigid custom fitted 04.01L2116 AFO, fracture orthosis, tibial fracture orthosis, rigid custom fitted 04.01L2122 KAFO, fracture orthosis, femoral fracture cast orthosis, plaster type casting material, molded to patient 04.01L2124 KAFO, fracture orthosis, femoral fracture cast orthosis, synthetic type casting material, molded to patient 04.01L2126 KAFO, fracture orthosis, femoral fracture cast orthosis, thermoplastic type casting material, molded to patient 04.01L2128 KAFO, fracture orthosis, femoral fracture cast orthosis, molded to patient model 04.01L2132 KAFO, fracture orthosis, femoral fracture cast orthosis, soft custom fitted 04.01L2134 KAFO, fracture orthosis, femoral fracture cast orthosis, semi-rigid custom fitted 04.01L2136 KAFO, fracture orthosis, femoral fracture cast orthosis, rigid custom fitted 04.01XX010 Immunosuppressive drug, not otherwise classified 08.01XX030 Category IV Enteral Product, 100 calories = 1 unit, Accupep HPF 10.01XX031 Category IV Enteral Product, 100 calories = 1 unit, Aminaid 10.01XX032 Category IV Enteral Product, 100 calories = 1 unit, Entera opd 10.01XX033 Category IV Enteral Product, 100 calories = 1 unit, Glucerna 10.01XX034 Category IV Enteral Product, 100 calories = 1 unit, Hepatic aid 10.01XX035 Category IV Enteral Product, 100 calories = 1 unit, Impact 10.01XX036 Category IV Enteral Product, 100 calories = 1 unit, Impact with fiber 10.01XX037 Category IV Enteral Product, 100 calories = 1 unit, Imunaid 10.01XX038 Category IV Enteral Product, 100 calories = 1 unit, Lipisorb 10.01XX039 Category IV Enteral Product, 100 calories = 1 unit, Nepro 10.01XX040 Category IV Enteral Product, 100 calories = 1 unit, New Replete 10.01XX041 Category IV Enteral Product, 100 calories = 1 unit, New Replete with Fiber 10.01XX042 Category IV Enteral Product, 100 calories = 1 unit, Nutrihep 10.01XX043 Category IV Enteral Product, 100 calories = 1 unit, Nutrivent 10.01XX044 Category IV Enteral Product, 100 calories = 1 unit, Peptamen 10.01XX045 Category IV Enteral Product, 100 calories = 1 unit, Perative 10.01XX046 Category IV Enteral Product, 100 calories = 1 unit, Pregestimil 10.01XX047 Category IV Enteral Product, 100 calories = 1 unit, Protain XL 10.01XX048 Category IV Enteral Product, 100 calories = 1 unit, Provide 10.01XX049 Category IV Enteral Product, 100 calories = 1 unit, Pulmocare 10.01XX050 Category IV Enteral Product, 100 calories = 1 unit, Reabilan HN 10.01XX051 Category IV Enteral Product, 100 calories = 1 unit, Suplena 10.01XX052 Category IV Enteral Product, 100 calories = 1 unit, Stresstein 10.01XX053 Category IV Enteral Product, 100 calories = 1 unit, Traumacal 10.01XX054 Category IV Enteral Product, 100 calories = 1 unit, Traumaid HBC 10.01

Page 95-24 March 1995 DMERC Medicare Advisory
HCPCS Codes Requiring A CMN (Cont'd)
DMERCHCPCS HCPCS CMNCODE DESCRIPTION REQUIRED
XX055 Category IV Enteral Product, 100 calories = 1 unit, Travasorb Hepatic 10.01XX056 Category IV Enteral Product, 100 calories =1 unit, Travasorb MCT 10.01XX057 Category IV Enteral Product, 100 calories = 1 unit, Travasorb Renal 10.01XX059 Category V Enteral Product, 100 calories = 1 unit, Casec 10.01XX060 Category V Enteral Product, 100 calories = 1 unit, Controlyte 10.01XX061 Category V Enteral Product, 100 calories = 1 unit, Elementra 10.01XX062 Category V Enteral Product, 100 calories = 1 unit, Fibrad 10.01XX063 Category V Enteral Product, 100 calories = 1 unit, Lipomul 10.01XX064 Category V Enteral Product, 100 calories = 1 unit, MCT Oil 10.01XX065 Category V Enteral Product, 100 calories = 1 unit, Microlipid 10.01XX066 Category V Enteral Product, 100 calories = 1 unit, Moducal 10.01XX067 Category V Enteral Product, 100 calories = 1 unit, Nutrisource 10.01XX068 Category V Enteral Product, 100 calories = 1 unit, Polycose 10.01XX069 Category V Enteral Product, 100 calories = 1 unit, Promod 10.01XX070 Category V Enteral Product, 100 calories = 1 unit, Promix 10.01XX071 Category V Enteral Product, 100 calories = 1 unit, Propac 10.01XX072 Category V Enteral Product, 100 calories = 1 unit, Sumacal 10.01XX073 Category IV Enteral Product, 100 calories = 1 unit, Advera 10.01XX074 Category IV Enteral Product, 100 calories = 1 unit, Crucial 10.01XX075 Category IV Enteral Product, 100 calories = 1 unit, Diabetisource 10.01XX076 Category IV Enteral Product, 100 calories = 1 unit, Isosource VHN 10.01
HCPCS CODES ANDMODIFIERS NOTAVAILABLE FOR USE
The following new HCPCS codes and modifiers were published on pages 94-250-254of the DMERC Medicare Advisory, December 1994 issue. Although published in theDecember issue, these new codes should not be used by DMEPOS suppliers. Thesecodes will not be available for use by DMEPOS suppliers until the DMERCs formallypublish a Medical Policy which addresses the code(s). As soon as the DMERCs haveapproved Medical Policies for these codes, the policies and their codes will bepublished in a DMERC Medicare Advisory.
KK Inhalation Solution Compounded from An FDA Approved FormulationKL Product Characteristics Defined in Medical Policy Are MetJ7645 Ipratropium Bromide 0.02%, per ml, inhalation solution, administered through DMEK0140 Acetylcysteine, compounded, per mg, inhalation solution administered through DMEK0141 Albuterol Sulfate, compounded, per mg, inhalation solution administered through DMEK0142 Cromolyn sodium, compounded, per mg, inhalation solution administered through DMEK0143 Isoetharine Hydrochloride, compounded, per mg, inhalation solution administered through DMEK0144 Isoprotherenol Hydrochloride, compounded, per mg, inhalation solution administered through DMEK0145 Metaproterenol, compounded, per mg, inhalation solution administered through DMEK0146 Terbutaline, compounded, per mg, inhalation solution administered through DMEK0156 Powered pressure-recuding mattress overlay (including low air loss)K0157 Powered alternating pressure-reducing mattress overlay with pumpK0158 Powered pressure-reducing mattress (including low air loss)K0159 Powered pressure-reducing mattress (including low air loss) with adjuvant featuresK0160 Powered pressure-reducing bed (including low air loss)K0161 Powered pressure-reducing bed (incuding low air loss) with adjuvant featuresK0182 Water, distilled, used with large volume nebulizer, 1000 mlK0269 Aerosol compressor, adjustable pressure, light duty for intermittent useK0270 Ultrasonic Generator with small volume ultrasonic nebulizerK0271 Pouch, drainable; with faceplate attached; reusable; rubber or vinyl, eachK0272 Pouch, drainable; without faceplate attached; reusable; rubber or vinyl, eachK0273 Pouch, urinary; with faceplate attached; reusable; rubber or vinyl, eachK0274 Pouch, urinary; without faceplate attached; reusable; rubber or vinyl, eachK0275 Ostomy faceplate; convex; reusable; rubber or vinyl, eachK0276 Ostomy faceplate; convex; custom fitted reusable; rubber or vinyl, eachK0279 Skin Barrier; with flange (solid, flexible or accordion) with built-in convexity, extended wear, any size, eachK0283 Saline Solution, per 10 ml, metered dose dispenser, for use with inhalation drugs
HCPCS CODES AND MODIFIERS NOT FOR CURRENT USE.PLEASE REFRAIN FROM USING THE FOLLOWING CODES AND
MODIFIERS UNTIL FURTHER NOTICE

March 1995 DMERC Medicare Advisory Page 95-25
Effective for claims with dates of service June 1, 1995 or after, the following HCPCScodes will no longer be valid for submission to the DMERCs.
Effective 6/1/95 - No longer valid codesA4454 Tape, all types, all sizesL7500 Repair of prosthetic device, hourly rate
Effective June 1, 1995, the above codes have been replaced by the following codes,respectively:
Required codes - Effective 6/1/95K0265 Tape, all types, per 18 square inchesK0285 Repair of prosthetic device, labor component, per 15 minutes
HCPCS CODECHANGES
Effective January 1, 1995, the following DMERC Level III Codes and Modifiers replacethe DMERC Level III Codes and Modifiers published in the September 1993 MedicareRegion C DMERC DMEPOS Supplier Manual, appendix C. Please photocopy thesepages (page 95-25-27 of this advisory) and replace the old appendix C of the manualwith this list of new DMERC Level III Codes and Modifiers. This information will bepublished in a revision to the Medicare Region C DMERC DMEPOS Supplier Manual.
HCPCS CODESUPDATE:NEW DMERC LEVELIII CODES ANDMODIFIERS
Code Description
XX001 STERILE SALINE, UNIT DOSE, UP TO 5ml, EACHXX002 BLOOD GLUCOSE TEST OR REAGENT STRIP FOR HOME BLOOD GLUCOSE
MONITOR, PER 25 STRIPS
XX003 PLATFORMS FOR HOME BLOOD GLUCOSE MONITOR, 50 PER BOXXX004 URINARY INTERMITTENT CATHETER WITH INSERTION TRAYXX005 THERAPEUTIC AGENT FOR URINARY CATHETER IRRIGATION
XX006 OSTOMY DEODORANT, ALL TYPES, PER OUNCEXX007 ADHESIVE REMOVER WIPES, 50 PER BOXXX008 OSTOMY FILTERS, ANY TYPE, EACH
XX009 DOBUTAMINE, 250mgXX010 IMMUNOSUPPRESSIVE DRUG, NOT OTHERWISE CLASSIFIEDXX011 NONADHESIVE APPLIANCE DISC, EACH
XX014 TRACHEOSTOMA FILTER(S), ANY TYPE, ANY SIZE, EACHXX030 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, ACCUPEP HPFXX031 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, AMINAID
XX032 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, ENTERA OPDXX033 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, GLUCERNAXX034 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, HEPATIC AID
XX035 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, IMPACTXX036 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, IMPACT WITH FIBERXX037 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, IMMUN-AID
XX038 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, LIPISORBXX039 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, NEPROXX040 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, REPLETE
XX041 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, REPLETE WITH FIBERXX042 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, NUTRIHEPXX043 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, NUTRIVENT
XX044 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, PEPTAMENXX045 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, PERATIVEXX046 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, PREGESTIMIL
XX047 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, PROTAIN XLXX048 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, PROVIDEXX049 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, PULMOCARE
XX050 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, REABILAN HN
« NEW CODE APPROVED BY HCFA (EFFECTIVE JAN.3,1995)
A PRODUCT NAME CHANGE APPROVED BY HCFA (EFFECTIVE JAN.3,1995)
«
A
DMERC Level III Codes

Page 95-26 March 1995 DMERC Medicare Advisory
ZU ADVANCE NOTICE OF POSSIBLE MEDICAL NECESSITY DENIAL ON FILEXA IV POLE WITH PEN INFUSION PUMP
Z X THE SPECIFIED COVERAGE CRITERIA IN THE MEDICAL POLICY HAVE BEEN MET ANDDOCUMENTATION IS AVAILABLE IN THE SUPPLIER’S RECORDS
ZY POTENTIALLY NONCOVERED ITEM OR SERVICE BILLED FOR DENIAL OR AT BENEFICIARY’S
REQUEST
HCPCS CODESUPDATE:NEW DMERC LEVELIII CODES ANDMODIFIERS(CONT'D)
DMERC Level III Modifiers
Code Description
XX051 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, SUPLENA
XX052 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, STRESSTEINXX053 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, TRAUMA-CALXX054 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT,TRAUM-AID HBC
XX055 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, TRAVASORB HEPATICXX056 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, TRAVASORB MCTXX057 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, TRAVASORB RENAL
XX058 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, VIVONEX T.E.N.XX059 CATEGORY V ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, CASECXX060 CATEGORY V ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, CONTROLYTE
XX061 CATEGORY V ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, ELEMENTRAXX062 CATEGORY V ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, FIBRADXX063 CATEGORY V ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, LIPOMUL
XX064 CATEGORY V ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, MCT OILXX065 CATEGORY V ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, MICROLIPIDXX066 CATEGORY V ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, MODUCAL
XX067 CATEGORY V ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, NUTRISOURCEXX068 CATEGORY V ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, POLYCOSEXX069 CATEGORY V ENTERAL PRODUCT, 100 CALOIRES = 1 UNIT, PROMOD
XX070 CATEGORY V ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, PROMIXXX071 CATEGORY V ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, PROPACXX072 CATEGORY V ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, SUMACAL
XX073 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, ADVERAXX074 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, CRUCIALXX075 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, DIABETISOURCE
XX076 CATEGORY IV ENTERAL PRODUCT, 100 CALORIES = 1 UNIT, ISOSOURCE VHNYY001 DYNAMIC ADJUSTABLE ELBOW EXTENSION/FLEXION ORTHOSISYY002 DYNAMIC ADJUSTABLE WRIST EXTENSION/FLEXION ORTHOSIS
YY003 DYNAMIC ADJUSTABLE KNEE EXTENSION/FLEXION ORTHOSISYY004 DYNAMIC ADJUSTABLE ANKLE EXTENSION/FLEXION ORTHOSISYY005 REPLACE SOFT INTERFACE MATERIAL, DYNAMIC ADJUSTABLE
EXTENSION/FLEXION ORTHOSISYY006 DYNAMIC ADJUSTABLE FINGER EXTENSION/FLEXION ORTHOSISZZ001 MISCELLANEOUS SUPPLY, ACCESSORY OR SERVICE COMPONENT OF
ANOTHER ITEMZZ002 INCONTINENCE SUPPLY, COMPONENT OF ANOTHER ITEMZZ003 SUCTION PUMP SUPPLY OR ACCESSORY, COMPONENT OF ANOTHER ITEM
ZZ004 CPAP SUPPLY, COMPONENT OF ANOTHER ITEMZZ005 PROSTHETIC AND ORTHOTIC SUPPLY OR SERVICE, COMPONENT OF
ANOTHER ITEM
ZZ006 TENS SUPPLY OR ACCESSORY, COMPONENT OF ANOTHER ITEMZZ007 TRACHEOSTOMY SUPPLY, COMPONENT OF ANOTHER ITEMZZ008 DELIVERY, SET-UP AND DISPENSING SERVICE, COMPONENT OF
ANOTHER ITEMZZ009 OXYGEN SUPPLY OR ACCESSORY, COMPONENT OF ANOTHER ITEMZZ010 TRANSTRACHEAL OXYGEN CATHETER FOR PATIENT OWNED EQUIPMENT
ZZ011 TRANSTRACHEAL OXYGEN CATHETER, COMPONENT OF ANOTHER ITEM
« NEW CODE APPROVED BY HCFA (EFFECTIVE JAN.3,1995)
A PRODUCT NAME CHANGE APPROVED BY HCFA (EFFECTIVE JAN.3,1995)
DMERC Level III Codes (Cont'd)
««««
Modifier Description

March 1995 DMERC Medicare Advisory Page 95-27
The proper coding for the immunosuppressive drug sandimmune is as follows:
Code Description
J7502 Cyclosporine - oral, sol; 100 mg/ml, 50 ml ea.1 unit for each 50ml.
J7502 is only covered for a grandfathered patient.
K0121 Cyclosporin, oral, 25mg. (any form, tablet; capsule, solution)1 unit for each 25mg.
K0121 is effective 10/1/93 for all new patients.
Note: 25mg 1 unit for each tablet/capsule100mg 4 units for each tablet/capsuleSol 50ml bottle 200 units for each bottle
IMMUNOSUPPRES-SIVE DRUGS:
Sandimmunne
HOME BLOODGLUCOSE MONITORPRICING CHANGE
Effective with dates of service on or after February 16, 1995, Home BloodGlucose Monitor (E0607) allowable amounts have been reduced. Thefollowing prices for code E0607 replace the prices published in the DMERCMedicare Advisory, December 1994 issue.
INEXPENSIVE OR ROUTINELY PURCHASED
CODE AL AR CO FL GA KY L A MS NC NM OK PR SC TN TX VI
E0607 $60.18 $60.18 $60.18 $60.18 $60.18 $60.18 $60.18 $60.18 $60.18 $60.18 $60.18 $68.62 $60.18 $60.18 $60.18 $68.62
INEXPENSIVE OR ROUTINELY PURCHASED (USED)
CODE AL AR CO FL GA KY L A MS NC NM OK PR SC TN TX VI
E0607 $45.13 $45.13 $45.13 $45.13 $45.13 $45.13 $45.13 $45.13 $45.13 $45.13 $45.13 $51.46 $45.13 $45.13 $45.13 $51.46
INEXPENSIVE OR ROUTINELY PURCHASED (RENTAL)
CODE AL AR CO FL GA KY L A MS NC NM OK PR SC TN TX VI
E0607 $6.02 $6.02 $6.02 $6.02 $6.02 $6.02 $6.02 $6.02 $6.02 $6.02 $6.02 $6.87 $6.02 $6.02 $6.02 $6.87
The following immunosuppressive drug (Prograf) is covered by Palmetto GBA forMedicare approved organ transplants. If the drug (Prograf) is the primary immunosup-pressive drug regimen and the physician supervising the post-transplant care of thepatient feels in his/her clinical judgment that Prograf should be used for organtransplants, Palmetto GBA will cover the Prograf.
J7507 - Tacrolimus, oral, per 1 mg (Prograf)J7508 - Tacrolimus, oral, per 5 mg (Prograf)
Prograf

Page 95-28 March 1995 DMERC Medicare Advisory
1995 DME FEESCHEDULE:Payment Changesand Updated Prices forVirgin Islands andPuerto Rico
The 1995 Update Factor for Durable Medical Equipment (DME) is a 2.5% increase.For Prosthetics and Orthotics the Update Factor is zero. The following is the 1995fee schedule matrix for the Virgin Islands and Puerto Rico. The fee schedules forthe other Region C states were published in the DMERC Medicare Advisory,December 1994 issue.
NOTE: Fee schedules for HCPCS deleted in 1995 have been included and are validthrough March 31, 1995. Deleted 1995 HCPCS may not be used on or afterApril 1, 1995.
E0600 41.24 38.84E0601 100.63 105.73E0606 18.87 19.97E0608 252.53 312.60E0630 91.77 88.65E0635 103.33 186.98E0744 82.49 120.79E0745 79.97 82.25E0749 205.99 396.20E0781 241.16 158.31E0791 242.12 178.29E0910 18.02 17.18E0920 41.57 57.45E0930 36.44 42.52E0940 31.32 33.69E0941 39.13 41.49E0946 48.22 56.27E0958 39.05 48.47E0968 16.14 19.82E1031 38.68 30.94E1050 91.47 104.07E1060 99.35 121.09E1070 93.66 143.55E1083 70.94 73.99E1084 83.03 93.78E1085 57.28 61.96E1086 75.71 81.76E1087 113.96 155.91E1088 135.82 187.58E1089 108.04 136.20E1090 122.66 167.86E1091 75.10 113.51E1092 115.77 153.71E1093 99.56 141.05E1100 87.83 115.54E1110 86.98 96.18E1130 39.89 59.17E1140 63.10 82.30E1150 73.50 92.29E1160 56.30 71.18E1170 74.42 133.22E1171 69.09 106.34E1172 88.23 99.86E1180 91.29 109.85E1190 105.47 137.46E1195 113.17 116.08E1200 78.39 113.51E1210 314.60 396.06E1211 362.63 396.06E1212 310.58 376.36E1213 334.02 383.52E1221 42.81 55.46E1222 61.07 66.77E1223 65.33 77.48E1224 62.14 87.87
E0450 859.84 1429.62E0453 578.49 672.27E0457 52.59 58.53E0460 561.70 726.12E0500 98.89 86.62E0575 92.58 92.87E0935 17.41 15.26
E0145 18.69 40.28E0146 14.59 14.93E0165 16.74 21.03E0166 28.04 39.78E0180 33.31 39.47E0181 32.84 38.77E0182 20.21 29.79E0186 18.28 43.61E0187 20.92 43.61E0193 775.83 1459.64E0194 2491.85 2437.86E0196 29.26 43.61E0202 56.41 202.65E0235 15.54 17.50E0236 34.68 31.83E0250 74.86 118.71E0251 60.87 90.09E0255 105.83 151.05E0256 75.08 112.60E0260 151.27 222.77E0261 123.36 175.13E0265 180.07 257.24E0266 159.98 228.48E0277 747.88 880.42E0290 66.34 89.89E0291 48.90 64.95E0292 75.71 118.10E0293 64.43 99.03E0294 117.72 180.61E0295 114.71 85.45E0296 147.91 197.07E0297 126.75 172.02E0305 13.60 9.03E0452 231.14 98.97E0459 45.84 48.94E0462 223.13 175.91E0480 33.64 39.70E0550 45.16 74.62E0565 54.96 27.01E0570 17.78 40.27E0585 31.59 43.79
E0143 108.31 137.15E0147 326.46 422.32E0153 62.50 80.43E0154 56.95 72.85E0155 24.17 40.48E0156 23.81 112.51E0157 64.51 68.49E0158 24.63 36.00E0160 29.78 5.36E0161 23.62 26.73E0162 131.24 229.57E0163 99.35 130.91E0164 163.42 224.01E0167 10.82 12.58E0175 50.71 62.86E0176 96.49 145.62E0177 95.61 145.62E0178 109.31 145.62E0179 10.43 41.65E0184 175.39 208.25E0185 288.14 631.96E0191 7.65 11.42E0192 337.48 421.40E0197 169.66 105.81E0198 169.66 524.55E0199 28.87 85.24E0200 71.42 149.99E0205 174.82 234.28E0210 24.99 27.14E0215 54.25 98.20E0220 6.49 7.30E0225 350.10 431.66E0230 6.49 12.45E0237 380.15 399.53E0238 20.71 28.10E0239 344.43 355.16E0249 76.26 114.36E0271 170.01 311.42E0272 154.96 211.42E0275 12.59 14.04E0276 11.98 17.57E0280 34.41 56.94E0310 148.66 177.05E0325 7.74 10.11E0326 8.61 7.13E0560 154.50 165.21E0605 23.81 14.18E0607 190.43 321.90E0609 495.91 685.67E0610 214.27 455.68E0615 393.79 455.68E0621 73.51 84.19E0627 296.38 357.48E0628 296.38 357.48E0629 253.22 357.48
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
FREQUENTLYSERVICED ITEMS
CAPPED RENTAL ITEMS
E1225 40.72 44.62E1228 21.45 26.21E1240 85.03 99.52E1250 58.20 67.19E1260 77.98 87.46E1270 63.38 78.45E1280 118.24 186.98E1285 102.33 113.80E1290 112.73 174.44E1295 109.41 155.31K0001 46.45 66.03K0002 73.33 79.10K0003 72.27 81.81K0004 120.39 164.67K0006 112.97 159.34K0007 158.07 191.16K0010 326.19 382.37K0011 517.16 625.43K0012 248.10 300.06K0101 39.05 48.47K0156 678.41 820.46K0157 32.44 39.47K0158 755.17 880.42K0159 753.79 911.62K0160 798.79 2350.88K0161 1356.82 1640.93K0195 10.69 12.54
A4611 150.42 238.79A4612 64.21 29.26A4613 129.84 95.07A4618 8.01 8.71A4631 91.07 116.06A4635 4.61 4.99A4636 3.79 2.14A4637 1.62 2.43A4640 50.11 68.56E0100 18.98 30.90E0105 44.24 54.70E0110 69.89 89.50E0111 45.63 44.51E0112 33.33 40.35E0113 19.03 20.17E0114 39.62 56.09E0116 21.24 28.05E0130 61.72 81.90E0135 75.52 109.04E0141 103.85 131.42E0142 131.68 141.14
INEXPENSIVE ORROUTINELY PUR-
CHASED ITEMS - NEW,INCLUDING TENS
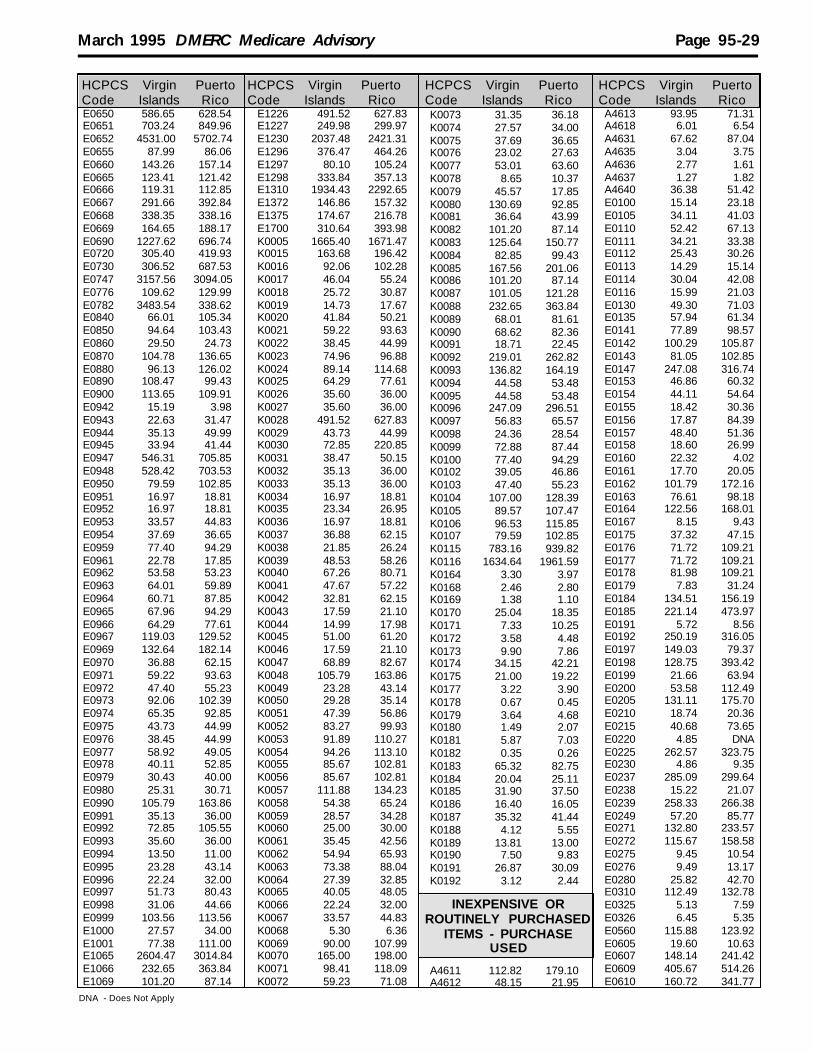
March 1995 DMERC Medicare Advisory Page 95-29
E0650 586.65 628.54E0651 703.24 849.96E0652 4531.00 5702.74E0655 87.99 86.06E0660 143.26 157.14E0665 123.41 121.42E0666 119.31 112.85E0667 291.66 392.84E0668 338.35 338.16E0669 164.65 188.17E0690 1227.62 696.74E0720 305.40 419.93E0730 306.52 687.53E0747 3157.56 3094.05E0776 109.62 129.99E0782 3483.54 338.62E0840 66.01 105.34E0850 94.64 103.43E0860 29.50 24.73E0870 104.78 136.65E0880 96.13 126.02E0890 108.47 99.43E0900 113.65 109.91E0942 15.19 3.98E0943 22.63 31.47E0944 35.13 49.99E0945 33.94 41.44E0947 546.31 705.85E0948 528.42 703.53E0950 79.59 102.85E0951 16.97 18.81E0952 16.97 18.81E0953 33.57 44.83E0954 37.69 36.65E0959 77.40 94.29E0961 22.78 17.85E0962 53.58 53.23E0963 64.01 59.89E0964 60.71 87.85E0965 67.96 94.29E0966 64.29 77.61E0967 119.03 129.52E0969 132.64 182.14E0970 36.88 62.15E0971 59.22 93.63E0972 47.40 55.23E0973 92.06 102.39E0974 65.35 92.85E0975 43.73 44.99E0976 38.45 44.99E0977 58.92 49.05E0978 40.11 52.85E0979 30.43 40.00E0980 25.31 30.71E0990 105.79 163.86E0991 35.13 36.00E0992 72.85 105.55E0993 35.60 36.00E0994 13.50 11.00E0995 23.28 43.14E0996 22.24 32.00E0997 51.73 80.43E0998 31.06 44.66E0999 103.56 113.56E1000 27.57 34.00E1001 77.38 111.00E1065 2604.47 3014.84E1066 232.65 363.84E1069 101.20 87.14
E1226 491.52 627.83E1227 249.98 299.97E1230 2037.48 2421.31E1296 376.47 464.26E1297 80.10 105.24E1298 333.84 357.13E1310 1934.43 2292.65E1372 146.86 157.32E1375 174.67 216.78E1700 310.64 393.98K0005 1665.40 1671.47K0015 163.68 196.42K0016 92.06 102.28K0017 46.04 55.24K0018 25.72 30.87K0019 14.73 17.67K0020 41.84 50.21K0021 59.22 93.63K0022 38.45 44.99K0023 74.96 96.88K0024 89.14 114.68K0025 64.29 77.61K0026 35.60 36.00K0027 35.60 36.00K0028 491.52 627.83K0029 43.73 44.99K0030 72.85 220.85K0031 38.47 50.15K0032 35.13 36.00K0033 35.13 36.00K0034 16.97 18.81K0035 23.34 26.95K0036 16.97 18.81K0037 36.88 62.15K0038 21.85 26.24K0039 48.53 58.26K0040 67.26 80.71K0041 47.67 57.22K0042 32.81 62.15K0043 17.59 21.10K0044 14.99 17.98K0045 51.00 61.20K0046 17.59 21.10K0047 68.89 82.67K0048 105.79 163.86K0049 23.28 43.14K0050 29.28 35.14K0051 47.39 56.86K0052 83.27 99.93K0053 91.89 110.27K0054 94.26 113.10K0055 85.67 102.81K0056 85.67 102.81K0057 111.88 134.23K0058 54.38 65.24K0059 28.57 34.28K0060 25.00 30.00K0061 35.45 42.56K0062 54.94 65.93K0063 73.38 88.04K0064 27.39 32.85K0065 40.05 48.05K0066 22.24 32.00K0067 33.57 44.83K0068 5.30 6.36K0069 90.00 107.99K0070 165.00 198.00K0071 98.41 118.09K0072 59.23 71.08
A4613 93.95 71.31A4618 6.01 6.54A4631 67.62 87.04A4635 3.04 3.75A4636 2.77 1.61A4637 1.27 1.82A4640 36.38 51.42E0100 15.14 23.18E0105 34.11 41.03E0110 52.42 67.13E0111 34.21 33.38E0112 25.43 30.26E0113 14.29 15.14E0114 30.04 42.08E0116 15.99 21.03E0130 49.30 71.03E0135 57.94 61.34E0141 77.89 98.57E0142 100.29 105.87E0143 81.05 102.85E0147 247.08 316.74E0153 46.86 60.32E0154 44.11 54.64E0155 18.42 30.36E0156 17.87 84.39E0157 48.40 51.36E0158 18.60 26.99E0160 22.32 4.02E0161 17.70 20.05E0162 101.79 172.16E0163 76.61 98.18E0164 122.56 168.01E0167 8.15 9.43E0175 37.32 47.15E0176 71.72 109.21E0177 71.72 109.21E0178 81.98 109.21E0179 7.83 31.24E0184 134.51 156.19E0185 221.14 473.97E0191 5.72 8.56E0192 250.19 316.05E0197 149.03 79.37E0198 128.75 393.42E0199 21.66 63.94E0200 53.58 112.49E0205 131.11 175.70E0210 18.74 20.36E0215 40.68 73.65E0220 4.85 DNAE0225 262.57 323.75E0230 4.86 9.35E0237 285.09 299.64E0238 15.22 21.07E0239 258.33 266.38E0249 57.20 85.77E0271 132.80 233.57E0272 115.67 158.58E0275 9.45 10.54E0276 9.49 13.17E0280 25.82 42.70E0310 112.49 132.78E0325 5.13 7.59E0326 6.45 5.35E0560 115.88 123.92E0605 19.60 10.63E0607 148.14 241.42E0609 405.67 514.26E0610 160.72 341.77
K0073 31.35 36.18K0074 27.57 34.00K0075 37.69 36.65K0076 23.02 27.63K0077 53.01 63.60K0078 8.65 10.37K0079 45.57 17.85K0080 130.69 92.85K0081 36.64 43.99K0082 101.20 87.14K0083 125.64 150.77K0084 82.85 99.43K0085 167.56 201.06K0086 101.20 87.14K0087 101.05 121.28K0088 232.65 363.84K0089 68.01 81.61K0090 68.62 82.36K0091 18.71 22.45K0092 219.01 262.82K0093 136.82 164.19K0094 44.58 53.48K0095 44.58 53.48K0096 247.09 296.51K0097 56.83 65.57K0098 24.36 28.54K0099 72.88 87.44K0100 77.40 94.29K0102 39.05 46.86K0103 47.40 55.23K0104 107.00 128.39K0105 89.57 107.47K0106 96.53 115.85K0107 79.59 102.85K0115 783.16 939.82K0116 1634.64 1961.59K0164 3.30 3.97K0168 2.46 2.80K0169 1.38 1.10K0170 25.04 18.35K0171 7.33 10.25K0172 3.58 4.48K0173 9.90 7.86K0174 34.15 42.21K0175 21.00 19.22K0177 3.22 3.90K0178 0.67 0.45K0179 3.64 4.68K0180 1.49 2.07K0181 5.87 7.03K0182 0.35 0.26K0183 65.32 82.75K0184 20.04 25.11K0185 31.90 37.50K0186 16.40 16.05K0187 35.32 41.44K0188 4.12 5.55K0189 13.81 13.00K0190 7.50 9.83K0191 26.87 30.09K0192 3.12 2.44
A4611 112.82 179.10A4612 48.15 21.95
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
INEXPENSIVE ORROUTINELY PURCHASED
ITEMS - PURCHASEUSED
DNA - Does Not Apply

Page 95-30 M arch 1995 DMERC Medicare Advisory
E1001 58.03 83.25E1065 1953.35 2261.13E1066 178.11 272.89E1069 75.90 65.35E1226 368.62 470.86E1227 187.50 230.84E1230 1611.41 1815.97E1296 282.35 348.19E1297 60.07 78.93E1298 250.38 267.85E1310 1450.83 1719.49E1372 108.71 117.99E1375 132.80 162.59E1700 232.98 295.50K0005 1249.04 1253.61K0015 122.76 147.32K0016 77.68 76.78K0017 34.52 41.43K0018 19.30 23.15K0019 11.04 13.26K0020 31.38 37.67K0021 44.42 71.06K0022 28.83 33.75K0023 56.22 72.66K0024 66.85 86.01K0025 48.21 58.21K0026 26.82 26.99K0027 26.82 26.99K0028 368.62 470.86K0029 32.81 33.75K0030 54.65 165.64K0031 28.52 37.61K0032 26.49 26.99K0033 26.49 26.99K0034 12.73 14.10K0035 17.51 20.21K0036 12.73 14.10K0037 27.66 46.61K0038 16.40 19.68K0039 36.40 43.70K0040 50.44 60.53K0041 35.76 42.92K0042 24.61 46.61K0043 13.20 15.83K0044 11.24 13.48K0045 38.26 45.90K0046 13.20 15.83K0047 51.66 62.00K0048 82.65 122.88K0049 17.44 44.04K0050 21.97 26.36K0051 35.53 42.64K0052 62.45 74.95K0053 68.92 82.71K0054 70.69 84.83K0055 64.26 77.10K0056 64.26 77.10K0057 83.90 100.68K0058 40.78 48.93K0059 21.43 25.72K0060 18.74 22.50K0061 26.60 31.92K0062 41.21 49.46K0063 55.02 66.03K0064 20.52 24.64K0065 30.03 36.04K0066 16.70 44.04K0067 25.20 33.62
K0068 3.98 4.77K0069 67.50 81.00K0070 123.75 148.49K0071 73.80 88.56K0072 44.43 53.32K0073 23.51 27.13K0074 33.58 25.52K0075 41.74 27.49K0076 17.27 20.72K0077 39.75 47.70K0078 6.47 7.78K0079 15.49 13.39K0080 101.72 69.64K0081 27.48 32.99K0082 61.59 65.35K0083 94.24 113.08K0084 62.15 74.58K0085 125.67 150.53K0086 61.59 65.35K0087 75.80 90.96K0088 178.11 272.89K0089 51.00 61.20K0090 51.48 61.78K0091 14.03 16.84K0092 164.26 197.12K0093 102.61 123.14K0094 33.44 40.12K0095 33.44 40.12K0096 185.32 222.37K0097 42.62 49.19K0098 18.29 21.41K0099 54.66 65.58K0100 60.28 70.71K0102 29.29 35.15K0103 36.36 41.42K0104 80.26 96.30K0105 67.17 80.62K0106 72.41 86.89K0107 59.70 77.14K0115 587.38 704.87K0116 1225.99 1471.19
A4611 15.60 29.85A4612 6.42 3.66A4613 12.99 11.89A4618 0.91 1.09A4631 9.29 14.50A4635 0.56 0.63A4636 0.38 0.27A4637 0.23 0.31A4640 5.24 8.57E0100 5.36 3.86E0105 7.98 6.83E0110 12.25 11.19E0111 6.45 5.57E0112 7.60 5.04E0113 4.64 2.52E0114 6.96 7.01E0116 4.86 3.52E0130 12.89 10.24E0135 15.09 13.08E0141 17.13 16.44E0142 20.24 17.64E0143 19.46 17.14
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
INEXPENSIVE ORROUTINELY PURCHASED
ITEMS - RENTAL
E0615 292.11 341.76E0621 55.40 63.14E0627 222.29 268.12E0628 222.29 268.12E0629 189.91 268.12E0650 442.84 78.57E0651 527.43 637.48E0652 3223.90 4277.07E0655 65.97 63.93E0660 107.92 117.85E0665 92.68 91.07E0666 92.40 84.64E0667 218.75 294.63E0668 253.76 281.10E0669 123.49 141.13E0690 918.54 522.57E0747 2360.75 616.75E0776 80.64 97.51E0782 2612.66 253.97E0840 49.48 79.02E0850 70.98 77.56E0860 22.70 18.57E0870 78.93 102.49E0880 72.76 94.53E0890 87.37 74.57E0900 85.13 82.44E0942 11.39 2.97E0943 16.97 23.61E0944 26.35 37.50E0945 26.27 31.08E0947 409.73 529.38E0948 372.67 527.65E0950 59.70 77.14E0951 12.73 14.10E0952 12.73 14.10E0953 25.19 33.63E0954 28.27 27.49E0959 60.28 70.71E0961 17.09 13.39E0962 40.18 39.92E0963 47.07 44.93E0964 45.75 65.89E0965 52.30 70.71E0966 48.21 58.21E0967 89.29 97.14E0969 103.89 136.60E0970 27.66 46.61E0971 44.42 71.06E0972 36.36 41.42E0973 77.68 76.78E0974 50.86 69.64E0975 32.80 33.75E0976 28.83 33.75E0977 44.20 36.80E0978 30.10 39.64E0979 22.83 29.99E0980 18.88 23.04E0990 82.65 122.88E0991 26.49 26.99E0992 54.65 79.17E0993 26.82 26.99E0994 10.13 8.24E0995 17.44 44.04E0996 16.70 24.00E0997 38.79 60.32E0998 23.29 33.50E0999 77.68 85.18E1000 20.67 25.52
E0147 33.13 52.79E0153 6.52 10.07E0154 6.56 9.11E0155 2.95 5.05E0156 3.04 14.06E0157 6.87 8.56E0158 2.71 4.50E0160 3.90 0.67E0161 2.96 3.35E0162 13.77 28.71E0163 18.71 16.38E0164 23.81 28.00E0167 1.13 1.56E0175 5.07 7.85E0176 12.75 18.09E0177 10.94 18.09E0178 13.52 18.09E0179 1.04 5.21E0184 22.13 26.04E0185 40.48 78.99E0191 0.77 1.42E0192 35.12 52.69E0197 23.41 13.23E0198 17.57 65.57E0199 2.88 10.65E0200 9.69 18.74E0205 19.23 29.28E0210 2.35 3.40E0215 5.68 16.10E0220 0.69 0.91E0225 34.50 53.96E0230 0.73 1.56E0237 42.33 49.95E0238 2.08 3.52E0239 34.44 44.39E0249 8.38 14.30E0271 17.66 37.28E0272 16.18 26.43E0275 1.27 1.75E0276 1.41 2.19E0280 3.70 7.11E0310 17.43 22.14E0325 1.16 1.27E0326 0.92 0.90E0560 18.11 20.65E0605 2.77 1.77E0607 22.23 39.22E0609 57.94 85.71E0610 22.60 56.96E0615 44.80 56.96E0621 7.12 10.53E0627 29.63 44.69E0628 29.63 44.68E0629 25.33 44.68E0650 70.50 78.57E0651 79.02 106.25E0652 453.08 712.85E0655 11.42 10.71E0660 14.42 19.64E0665 12.45 15.18E0666 11.67 14.10E0667 32.93 49.11E0668 33.40 37.52E0669 16.47 18.82E0690 126.78 87.08E0747 315.75 456.79E0776 14.29 16.24E0782 348.36 42.33

March 1995 DMERC Medicare Advisory Page 95-31
E0840 14.70 29.26E0850 13.00 12.93E0860 4.98 3.10E0870 12.07 17.09E0880 15.10 15.76E0890 29.57 12.42E0900 21.15 13.74E0942 1.79 0.49E0943 2.48 3.94E0944 3.53 6.25E0945 3.39 5.19E0947 56.66 88.23E0948 52.83 87.93E0950 7.97 12.86E0951 1.76 2.36E0952 1.77 2.36E0953 3.37 5.61E0954 4.25 4.59E0959 7.69 11.80E0961 2.38 2.22E0962 5.36 6.65E0963 6.50 7.49E0964 6.90 10.98E0965 7.65 11.80E0966 6.34 9.72E0967 12.21 16.18E0969 13.97 22.78E0970 3.39 7.77E0971 5.72 11.85E0972 4.85 6.92E0973 8.86 12.78E0974 6.77 11.61E0975 4.37 5.62E0976 3.79 5.62E0977 5.68 6.13E0978 4.01 6.61E0979 3.05 5.00E0980 2.52 3.84E0990 11.01 20.48E0991 3.43 4.50E0992 7.27 13.20E0993 3.54 4.50E0994 1.36 1.38E0995 2.34 5.39E0996 2.21 4.00E0997 5.46 10.07E0998 3.11 5.59E0999 10.13 14.20E1000 3.28 4.25E1001 7.88 13.87E1065 238.09 376.85E1066 23.27 45.48E1069 10.20 10.89E1226 49.15 78.48E1227 25.00 37.50E1230 200.39 302.66E1296 38.24 58.03E1297 8.90 13.15E1298 33.38 44.64E1310 157.74 286.57E1372 18.13 19.67E1375 31.95 27.10E1700 30.47 49.24K0005 166.53 167.15K0015 16.38 19.64K0016 8.86 12.78K0017 4.60 5.52K0018 2.56 3.10
K0019 1.48 1.76K0020 4.19 5.02K0021 5.81 11.85K0022 3.83 5.62K0023 7.49 9.70K0024 8.91 11.48K0025 6.34 9.72K0026 3.54 4.50K0027 3.54 4.50K0028 50.59 78.48K0029 4.37 5.62K0030 7.27 27.59K0031 3.85 6.24K0032 3.44 4.50K0033 3.44 4.50K0034 1.76 2.36K0035 2.34 2.70K0036 1.77 2.36K0037 3.39 7.77K0038 2.18 2.61K0039 4.86 5.83K0040 6.72 8.08K0041 4.78 5.72K0042 3.27 7.77K0043 1.76 2.11K0044 1.50 1.80K0045 5.11 6.12K0046 1.76 2.11K0047 6.91 8.26K0048 11.01 20.48K0049 2.34 5.39K0050 2.92 3.52K0051 4.76 5.69K0052 8.32 9.99K0053 9.18 11.02K0054 9.43 11.31K0055 8.56 10.27K0056 8.56 10.27K0057 11.19 13.43K0058 5.44 6.53K0059 2.85 3.43K0060 2.50 3.00K0061 3.55 4.26K0062 5.49 6.59K0063 7.34 8.80K0064 2.75 3.29K0065 4.00 4.82K0066 2.21 4.00K0067 3.37 4.48K0068 0.54 0.64K0069 9.00 10.80K0070 16.50 19.80K0071 9.84 11.82K0072 5.92 7.10K0073 3.14 3.62K0074 3.03 3.40K0075 4.25 4.59K0076 2.32 2.77K0077 5.30 6.36K0078 0.86 1.05K0079 4.76 2.22K0080 13.56 11.61K0081 3.66 4.41K0082 10.17 10.89K0083 12.57 15.08K0084 8.29 9.93K0085 16.77 20.11K0086 10.17 10.89
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
K0087 10.11 12.13K0088 23.26 45.48K0089 6.79 8.16K0090 6.87 8.24K0091 1.87 2.24K0092 21.89 26.28K0093 13.68 16.43K0094 4.47 5.35K0095 4.47 5.35K0096 24.70 29.64K0097 5.69 6.56K0098 2.44 2.86K0099 7.30 8.74K0100 7.69 11.80K0102 3.91 4.67K0103 4.85 6.92K0104 10.69 12.83K0105 8.94 10.75K0106 9.67 11.59K0107 7.97 12.86K0115 78.33 93.98K0116 163.48 196.16
E0424 308.71 393.04E0431 48.50 49.44E0434 48.50 49.44E0439 308.71 393.04E0441 219.89 185.55E0442 219.89 185.55E0443 28.89 52.21E0444 28.89 52.21E1400 308.71 393.04E1401 308.71 393.04E1402 308.71 393.04E1403 308.71 393.04E1404 308.71 393.04E1405 340.30 436.82E1406 326.49 433.31
A4253 38.35 35.56A4256 8.76 9.10A4259 11.48 10.76A4556 10.93 6.38A4557 17.17 15.18A4558 4.17 1.75A4624 2.01 1.14E0731 273.11 DNAE1701 9.55 10.27E1702 20.32 25.81K0110 20.39 24.48K0111 42.10 48.56K0118 25.95 31.13K0131 16.25 19.52
A4214 1.33 1.12A4310 6.96 15.95A4311 12.18 10.15A4312 13.80 23.13A4313 16.69 16.81A4314 21.98 23.13A4315 23.77 23.13A4316 25.58 23.13A4320 4.41 55.73A4322 2.75 24.27A4323 6.72 6.15A4326 8.77 1.37A4327 36.32 1.14A4328 9.42 1.14A4329 31.41 23.13A4330 5.47 1.14A4338 9.77 7.68A4340 18.68 4.98A4344 14.43 24.51A4346 16.00 15.57A4347 15.58 16.48A4351 1.39 8.26A4352 5.78 8.26A4354 9.03 15.95A4355 8.03 21.31A4356 34.94 29.68A4357 8.74 8.83A4358 5.66 5.01A4359 27.44 25.06A4361 14.06 9.27A4362 3.12 3.16A4363 3.39 6.75A4364 2.64 5.92A4367 6.17 6.59A4397 3.82 6.96A4398 10.38 25.99A4399 10.69 12.82A4400 37.43 50.69A4402 1.44 2.85A4404 1.52 1.61A4454 2.00 1.07A4455 1.09 1.03A4622 43.85 2.74A4623 5.90 2.74A4625 6.24 39.89A4626 2.88 1.14A4630 4.79 4.29A5051 2.03 2.36A5052 1.50 1.14A5053 1.49 1.14A5054 1.45 1.24A5055 1.27 4.56A5061 3.13 3.15A5062 2.34 2.88A5063 2.01 2.14A5064 3.90 1.71A5065 2.86 1.71A5071 4.20 1.71A5072 3.27 1.71A5073 2.75 3.19A5074 5.09 8.36A5075 3.70 3.19A5081 2.96 1.37
OXYGEN AND OXYGENEQUIPMENT
OSTOMY,TRACHEOSTOMY AND
UROLOGICAL SUPPLIES
SUPPLIES
DNA - Does Not Apply

Page 95-32 March 1995 DMERC Medicare Advisory
A5082 9.10 1.37A5093 1.60 1.14A5102 24.92 5.01A5105 36.72 18.23A5112 27.63 5.01A5113 4.23 5.64A5114 8.05 5.64A5119 9.71 6.56A5121 5.72 3.72A5122 10.26 12.74A5123 4.34 3.93A5126 1.01 1.61A5131 14.29 45.59K0132 1.27 1.47K0133 1.57 1.85K0134 3.19 3.73K0135 1.51 1.76K0136 8.92 10.43K0137 2.17 2.54K0138 3.09 3.60K0139 3.29 3.85K0165 4.17 4.87
A4560 16.94 26.70E0750 6712.61 7376.59K0112 202.40 242.89K0113 123.46 148.16K0114 629.86 755.84K0126 108.13 129.76K0127 16.01 19.20K0128 11.68 14.02K0129 114.15 136.98K0130 52.55 63.06K0163 358.10 442.63L0100 440.04 459.85L0110 93.62 93.92L0120 17.29 32.38L0130 141.74 416.13L0140 41.72 80.96L0150 80.59 91.76L0160 109.19 103.63L0170 420.26 413.97L0172 95.36 86.36L0174 179.01 140.33L0180 264.28 270.30L0190 353.98 373.39L0200 340.86 373.39L0210 36.66 21.59L0220 100.58 102.55L0300 132.65 147.38L0310 286.40 323.84L0315 219.44 377.81L0317 270.66 388.60L0320 243.46 156.53L0330 298.70 744.83L0340 425.41 376.84L0350 663.10 742.34L0360 983.42 860.90L0370 315.54 701.65L0380 540.67 286.06L0390 1120.33 1159.29L0400 1248.50 1349.32L0410 1240.37 1511.24
L0420 1318.78 2104.94L0430 968.61 1133.43L0440 732.85 593.70L0500 92.15 172.71L0510 212.53 274.45L0515 143.86 91.76L0520 297.33 323.30L0530 269.96 183.51L0540 356.50 215.89L0550 957.54 988.03L0560 961.10 968.27L0565 730.74 809.59L0600 63.05 63.68L0610 168.35 150.59L0620 367.86 194.95L0700 1317.42 916.14L0710 1367.57 974.10L0810 1706.94 1536.60L0820 1407.59 997.42L0830 2043.41 1739.54L0860 793.85 803.12L0900 104.34 89.16L0910 232.80 185.56L0920 110.60 89.16L0930 263.87 242.88L0940 103.04 134.94L0950 252.46 317.36L0960 45.01 59.38L0970 77.09 46.31L0972 74.31 46.31L0974 116.67 75.46L0976 104.19 75.46L0978 125.43 46.31L0980 11.38 9.88L0982 10.61 9.88L0984 42.66 48.74L1000 1322.98 1651.57L1010 43.73 28.93L1020 56.33 37.79L1025 108.35 183.51L1030 41.45 40.59L1040 50.84 29.03L1050 54.25 29.03L1060 62.32 46.31L1070 58.64 38.86L1080 36.06 11.55L1085 100.31 104.71L1090 65.55 40.59L1100 106.39 52.14L1110 166.43 104.38L1120 25.88 16.30L1200 1021.01 1043.72L1210 227.34 1130.73L1220 192.48 1188.59L1230 493.91 1594.58L1240 51.07 47.21L1250 47.08 36.23L1260 49.30 36.23L1270 50.49 41.72L1280 60.39 58.18L1290 51.22 42.81L1300 1451.36 1592.20L1310 1445.54 1275.65L1500 1237.77 1079.46L1510 1044.08 1727.13L1520 1937.01 2698.64L1600 83.97 187.07L1610 31.27 27.46L1620 96.63 90.02
L1630 110.42 96.62L1640 351.34 647.67L1650 150.87 107.58L1660 111.52 104.30L1680 793.97 809.59L1685 775.12 917.54L1686 792.56 863.57L1700 995.12 1025.48L1710 1164.91 1187.40L1720 858.68 242.88L1730 757.26 852.77L1750 170.94 52.69L1755 1061.92 1187.40L1800 43.34 68.06L1810 69.99 76.74L1815 63.13 75.56L1820 95.89 98.55L1825 35.83 20.86L1830 67.57 72.43L1832 528.24 917.54L1834 572.70 1025.48L1840 674.32 863.57L1844 1065.46 1269.07L1845 669.44 626.09L1846 889.18 663.87L1850 205.98 269.86L1855 954.77 966.12L1858 854.73 1187.40L1860 851.68 921.96L1870 840.45 946.90L1880 544.07 539.73L1900 175.80 199.70L1902 68.08 48.58L1904 316.89 334.63L1906 79.15 80.96L1910 216.80 334.63L1920 243.70 431.78L1930 154.15 127.60L1940 409.07 863.57L1945 603.22 442.58L1950 647.16 695.82L1960 481.60 863.57L1970 614.99 731.40L1980 268.45 231.98L1990 346.41 701.65L2000 745.31 707.65L2010 803.35 724.10L2020 826.65 1052.48L2030 847.60 811.75L2036 1612.01 2320.83L2037 1426.36 1678.01L2038 1223.93 1187.40L2040 115.70 85.63L2050 318.23 356.79L2060 400.56 512.75L2070 88.20 97.15L2080 248.69 296.86L2090 285.74 296.86L2102 380.81 388.60L2104 387.68 458.77L2106 568.47 514.90L2108 844.99 566.72L2112 386.16 377.81L2114 503.91 599.10L2116 554.39 723.24L2122 642.82 631.49L2124 717.69 674.67L2126 1040.42 917.54
L2128 1346.18 1025.48L2132 700.88 809.59L2134 840.34 971.51L2136 1027.50 1619.19L2180 76.31 53.97L2182 59.72 26.99L2184 80.72 37.79L2186 107.87 59.38L2188 260.22 70.17L2190 61.28 48.58L2192 296.52 210.50L2200 32.10 37.79L2210 47.86 37.79L2220 60.53 53.97L2230 50.00 28.93L2240 54.50 14.46L2250 231.55 197.54L2260 174.17 420.99L2265 76.73 91.76L2270 35.79 91.76L2275 82.14 104.94L2280 340.21 373.25L2300 233.93 34.76L2310 80.16 34.76L2320 160.46 144.92L2330 341.16 243.52L2335 148.03 80.96L2340 316.54 323.84L2350 771.70 753.89L2360 44.96 54.89L2370 223.04 248.28L2375 73.63 48.58L2380 80.23 32.38L2385 87.28 28.93L2390 76.04 43.18L2395 101.95 43.18L2397 76.92 94.13L2405 36.77 26.99L2415 119.67 46.31L2425 142.43 69.62L2435 107.85 46.31L2492 75.71 70.17L2500 205.58 127.60L2510 550.95 811.75L2520 369.87 485.76L2525 914.26 2158.91L2526 446.34 1295.35L2530 199.52 202.94L2540 281.45 289.94L2550 227.44 80.96L2570 310.38 289.94L2580 346.99 347.91L2600 133.83 58.02L2610 184.67 75.46L2620 232.31 115.94L2622 199.83 102.55L2624 231.06 145.73L2627 1359.10 1198.20L2628 1403.29 1187.40L2630 196.53 458.77L2640 291.98 463.90L2650 80.28 28.93L2660 121.46 46.31L2670 137.29 28.93L2680 127.62 28.93L2750 64.10 23.21L2760 48.70 28.50L2770 47.42 11.61
PROSTHETICS &ORTHOTICS
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico

March 1995 DMERC Medicare Advisory Page 95-33
L2780 53.10 23.21L2785 24.31 26.45L2795 62.22 38.97L2800 69.51 59.38L2810 50.90 48.58L2820 65.00 226.69L2830 75.40 226.69L2840 33.69 32.38L2850 43.32 43.18L3215 84.37 172.71L3219 94.77 156.53L3224 42.19 86.36L3225 47.40 78.27L3650 43.45 53.97L3660 67.09 63.80L3670 85.49 80.96L3700 51.51 23.21L3710 82.28 28.93L3720 556.10 220.31L3730 749.66 255.08L3740 840.74 701.65L3800 127.50 156.53L3805 270.73 219.56L3810 41.32 28.93L3815 39.62 34.76L3820 65.90 59.06L3825 42.76 51.00L3830 53.98 47.60L3835 58.52 46.31L3840 40.09 34.76L3845 51.77 40.59L3850 98.59 52.14L3855 74.54 58.02L3860 102.02 81.23L3900 825.10 521.91L3901 1133.71 695.82L3902 1553.27 909.25L3904 1867.37 1330.17L3906 260.37 215.89L3907 380.24 485.76L3908 50.94 28.32L3910 260.17 191.38L3912 60.47 37.14L3914 72.65 1052.48L3916 80.98 46.31L3918 49.98 30.23L3920 72.15 37.14L3922 62.35 40.59L3924 68.00 42.91L3926 66.28 46.31L3928 44.48 23.21L3930 40.99 28.93L3932 29.97 23.21L3934 30.73 23.21L3936 57.58 40.59L3938 59.47 38.97L3940 68.55 59.38L3942 47.41 39.40L3944 62.62 45.23L3946 56.51 80.96L3948 41.09 34.76L3950 95.63 54.51L3952 106.13 60.23L3954 70.42 46.31L3960 480.70 405.99L3962 457.52 324.70L3963 1161.17 1133.43L3964 585.99 890.56
L3965 772.40 879.76L3966 719.39 766.41L3968 858.29 982.31L3969 508.56 626.09L3970 255.25 340.03L3972 185.46 235.33L3974 146.64 235.33L3980 225.40 728.64L3982 317.40 728.64L3984 234.77 115.94L3985 496.93 188.91L3986 415.90 127.60L3995 27.80 32.38L4000 830.87 755.62L4010 515.70 647.67L4020 715.82 809.59L4030 438.67 647.67L4040 314.52 777.21L4045 213.76 242.88L4050 358.70 647.67L4055 174.20 296.86L4060 207.09 172.71L4070 183.39 172.71L4080 67.36 80.96L4090 70.04 80.96L4100 84.45 97.15L4110 72.84 97.15L4130 323.31 296.86L4310 316.77 647.67L4320 95.58 53.97L4350 58.25 45.01L4360 187.18 208.33L4370 123.02 120.90L4380 86.54 83.12L5000 350.77 566.72L5010 1072.92 566.72L5020 1375.82 782.82L5050 1698.29 2158.91L5060 2556.67 579.89L5100 1759.50 2158.91L5105 2939.26 3778.10L5150 2707.86 3778.10L5160 2651.72 3886.05L5200 2294.43 3346.32L5210 2246.18 3130.43L5220 2050.20 3022.48L5230 2641.02 2698.64L5250 3847.54 7016.47L5270 3570.56 10309.99L5280 3534.85 7232.36L5300 1959.56 2914.53L5310 3035.74 4641.67L5320 2926.67 4574.74L5330 4087.60 8419.76L5340 4483.63 10309.99L5400 835.55 492.88L5410 290.07 150.69L5420 1055.26 753.89L5430 465.80 2698.64L5450 314.64 208.77L5460 378.55 260.90L5500 891.64 1295.35L5505 1207.51 2266.86L5510 1010.73 1727.13L5520 1219.73 1727.13L5530 1199.12 684.04L5535 1316.84 1813.49L5540 1256.55 1781.10
L5560 1576.67 2590.70L5570 1588.09 742.12L5580 1800.03 985.76L5585 1776.27 2590.70L5590 1852.05 2590.70L5595 3085.92 4317.83L5600 3413.87 4857.56L5610 1437.35 2158.91L5611 1118.55 1133.43L5613 1701.38 1430.29L5614 2883.95 3402.53L5616 942.89 809.59L5618 205.77 181.15L5620 228.35 274.45L5622 335.58 701.65L5624 291.60 384.18L5626 331.00 863.57L5628 346.10 734.03L5629 294.18 323.84L5630 314.74 208.77L5631 406.72 485.76L5632 167.91 58.08L5634 247.57 81.23L5636 235.86 58.08L5637 255.88 701.65L5638 406.49 87.01L5639 991.60 2050.97L5640 591.89 174.01L5642 513.30 202.94L5643 1080.55 782.61L5644 410.05 231.98L5645 553.93 458.77L5646 402.78 376.84L5647 578.06 523.54L5648 507.98 463.85L5649 1321.79 1079.46L5650 451.88 755.62L5651 833.72 755.62L5652 302.68 809.59L5653 404.05 1079.46L5654 243.84 269.86L5655 236.90 593.70L5656 336.56 367.77L5658 271.74 593.70L5660 400.24 294.28L5661 423.71 399.40L5662 367.01 316.94L5663 489.13 397.05L5664 489.13 397.05L5665 355.47 377.81L5666 54.59 58.74L5667 1136.29 1432.44L5668 73.06 72.43L5669 871.32 940.49L5670 194.90 109.78L5672 207.02 115.94L5674 44.37 17.38L5675 60.15 37.79L5676 251.58 512.75L5677 342.30 134.94L5678 27.57 10.79L5680 270.61 222.80L5682 452.61 404.80L5684 34.31 17.38L5686 47.29 23.21L5688 56.53 66.09L5690 71.87 64.77L5692 92.25 64.87
L5694 125.95 138.32L5695 131.68 106.86L5696 139.53 120.76L5697 55.74 54.89L5698 90.92 112.97L5699 132.05 58.02L5700 1936.63 2451.38L5701 2402.56 2943.94L5702 3028.06 3724.51L5704 394.87 458.60L5705 723.93 819.41L5706 706.11 803.27L5707 948.66 1058.99L5710 262.76 384.23L5711 394.52 356.22L5712 341.91 362.06L5714 301.21 144.92L5716 505.99 202.94L5718 632.43 202.94L5722 626.81 539.73L5724 1305.12 1295.35L5726 1207.68 910.41L5728 1838.05 1824.28L5780 794.84 487.05L5785 360.69 404.80L5790 499.18 647.67L5795 745.40 863.57L5810 349.24 269.86L5811 506.32 782.61L5812 392.45 512.75L5816 590.41 350.83L5818 714.51 755.62L5822 1465.87 809.59L5824 1318.17 1025.48L5828 2395.67 2541.04L5830 1413.73 1206.84L5840 1577.60 2066.80L5850 93.05 73.41L5855 214.41 294.10L5910 275.07 485.76L5920 368.35 971.51L5925 233.27 421.13L5940 378.30 647.67L5950 613.31 701.65L5960 888.46 1322.34L5962 408.07 542.82L5964 707.76 773.87L5966 911.71 950.85L5970 140.99 188.91L5972 244.67 188.91L5974 161.78 269.86L5976 490.59 561.32L5978 202.60 129.39L5979 1584.09 1937.34L5980 3380.15 3929.22L5981 2154.36 2562.71L5982 401.35 185.81L5984 395.50 280.66L5986 439.93 185.81L6000 943.43 649.51L6010 1077.83 649.51L6020 957.07 672.61L6050 1538.57 695.82L6055 2005.00 1975.41L6100 1781.53 802.06L6110 1889.62 811.75L6120 2052.79 869.77L6130 2221.61 887.21
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico

Page 95-34 March 1995 DMERC Medicare Advisory
L6200 1893.95 1130.46L6205 2842.34 2644.67L6250 1964.69 1159.66L6300 3139.34 1507.57L6310 2241.60 800.20L6320 1186.42 568.23L6350 3625.73 1797.57L6360 2211.29 869.77L6370 1880.09 649.51L6380 961.24 1187.40L6382 1370.59 1943.02L6384 1764.86 2266.86L6386 371.72 809.59L6388 305.21 263.47L6400 1874.95 788.65L6450 2154.01 1130.63L6500 2219.65 1159.66L6550 2647.32 1507.57L6570 3235.78 1797.57L6580 1087.89 2266.86L6582 961.24 1511.24L6584 1458.93 1943.02L6586 1307.56 1727.13L6588 2003.06 3346.32L6590 1865.69 4101.94L6600 173.63 87.01L6605 171.44 75.46L6610 115.59 69.62L6615 127.60 69.62L6616 52.50 43.17L6620 210.49 150.69L6623 445.33 80.96L6625 369.23 162.35L6628 332.58 37.79L6629 121.66 59.38L6630 149.63 13.93L6632 45.11 37.79L6635 140.28 87.01L6637 254.92 59.38L6640 259.30 87.01L6641 148.50 191.06L6642 201.28 377.81L6645 224.05 197.22L6650 269.14 243.52L6655 55.49 54.51L6660 63.72 58.08L6665 37.03 13.93L6670 41.04 26.66L6672 142.30 323.84L6675 94.36 108.68L6676 101.29 98.70L6680 203.00 442.58L6682 217.69 550.52L6684 309.03 362.27L6686 415.85 771.82L6687 407.54 863.57L6688 378.43 858.17L6689 623.71 998.50L6690 536.48 1052.48L6691 255.86 458.77L6692 393.79 647.67L6700 360.13 174.01L6705 211.43 185.65L6710 239.61 191.38L6715 238.01 191.38L6720 592.26 376.84L6725 286.74 208.77L6730 512.88 208.77
L6735 206.87 174.01L6740 269.70 191.38L6745 246.77 191.38L6750 243.92 191.38L6755 243.23 191.38L6765 254.12 191.38L6770 244.97 191.38L6775 290.26 202.94L6780 310.27 208.77L6790 321.91 231.98L6795 859.20 487.05L6800 703.41 515.98L6805 277.26 168.13L6806 1061.13 1511.24L6807 805.80 1295.35L6808 679.14 1062.19L6809 343.46 794.48L6810 129.49 134.94L6825 764.17 1052.48L6830 940.13 1187.40L6835 818.95 1187.40L6840 568.94 1079.46L6845 657.77 1079.46L6850 478.33 890.56L6855 608.47 1187.40L6860 477.25 318.98L6865 301.42 260.90L6867 744.00 1845.87L6868 176.45 230.54L6870 184.98 155.89L6872 790.75 1899.84L6873 343.55 1727.13L6875 688.19 666.83L6880 466.76 661.06L6890 157.44 485.76L6895 387.66 185.56L6900 1232.25 3508.24L6905 1217.57 2698.64L6910 1265.98 2266.68L6915 434.61 593.70L6920 4633.19 5937.01L6925 5348.95 8743.60L6930 4661.92 6800.58L6935 5449.09 7394.28L6940 6457.48 7664.14L6945 7239.90 9984.98L6950 6923.39 9984.98L6955 8291.71 10309.99L6960 8362.81 10309.99L6965 9839.24 10309.99L6970 10125.49 10309.99L6975 11094.32 10309.99L7010 2535.62 4425.77L7015 4101.78 7016.47L7020 2616.06 2642.42L7025 2734.11 2873.51L7030 4336.22 6044.96L7035 2580.32 2642.42L7040 2118.20 2216.47L7045 1122.13 1053.34L7160 11290.02 10309.99L7165 12328.58 9999.99L7170 4070.69 6476.74L7180 24956.46 10309.99L7185 4978.20 10309.99L7186 7584.08 10309.99L7190 6992.84 10309.99L7191 7841.22 10309.99
L7260 1366.28 2266.86L7261 2487.17 2320.83L7266 687.36 863.57L7272 1545.15 2050.97L7274 4358.53 5748.11L7360 210.49 275.28L7362 194.00 532.44L7364 368.86 532.44L7366 496.86 587.33L8000 25.58 32.38L8010 45.12 49.77L8020 166.50 207.68L8030 224.53 234.49L8300 58.56 97.15L8310 122.59 150.69L8320 37.11 26.99L8330 34.27 37.79L8400 14.57 17.38L8410 17.64 18.57L8415 16.69 17.56L8420 15.63 26.99L8430 18.09 26.99L8435 15.26 17.56L8440 37.56 34.76L8460 46.27 75.56L8465 33.87 21.96L8470 4.64 2.37L8480 6.39 3.57L8485 7.77 9.52L8490 110.86 100.07L8500 527.60 485.76L8501 83.86 86.36Q0134 307.99 310.61V2020 43.52 32.93V2100 36.25 32.93V2101 38.21 32.93V2102 44.23 32.93V2103 31.49 32.93V2104 34.86 32.93V2105 37.96 32.93V2106 41.93 32.93V2107 40.06 32.93V2108 39.88 32.93V2109 44.36 32.93V2110 45.29 32.93V2111 47.21 44.74V2112 51.53 44.74V2113 56.64 44.74V2114 62.92 44.74V2115 53.03 DNAV2116 50.20 54.89V2117 59.15 60.39V2118 58.17 60.39V2200 47.45 40.89V2201 51.39 40.89V2202 58.30 40.89V2203 47.88 40.89V2204 49.15 40.89V2205 53.58 40.89V2206 54.14 40.89V2207 49.83 40.89V2208 51.46 40.89V2209 52.31 40.89V2210 55.88 40.89V2211 58.05 51.87V2212 58.96 51.87V2213 61.17 40.89V2214 74.52 51.87
V2215 69.27 51.87V2216 63.91 65.60V2217 68.76 71.37V2218 90.11 DNAV2219 38.78 6.10V2220 33.43 54.89V2300 58.54 55.99V2301 56.53 55.99V2302 57.34 DNAV2303 55.88 55.99V2304 60.26 55.99V2305 62.17 55.99V2306 63.80 55.99V2307 61.50 55.99V2308 61.57 55.99V2309 63.34 55.99V2310 64.40 55.99V2311 62.09 66.97V2312 62.48 66.97V2313 70.37 66.97V2314 80.22 66.97V2315 99.96 112.31V2316 101.58 105.13V2317 97.36 105.18V2318 135.78 147.89V2319 39.50 29.68V2320 48.49 65.87V2410 76.77 96.33V2430 100.02 138.76V2500 75.24 219.56V2501 114.60 247.02V2502 141.18 246.15V2503 130.03 137.07V2510 87.70 219.56V2511 147.58 246.15V2512 174.37 246.15V2513 146.40 219.56V2520 96.54 219.56V2521 168.07 247.02V2522 163.56 247.02V2523 130.31 220.53V2530 154.84 139.47V2623 804.61 512.75V2624 42.26 54.60V2625 256.95 210.39V2626 138.51 125.97V2627 1097.57 713.84V2628 214.55 545.88V2700 35.06 32.99V2710 59.35 87.82V2715 10.75 55.44V2718 24.53 28.54V2730 14.64 4.30V2740 9.44 8.78V2741 9.11 8.78V2742 9.28 8.78V2743 9.63 8.78V2744 11.54 8.78V2750 14.22 27.25V2755 11.53 9.05V2760 11.78 5.72V2770 17.38 21.96V2780 8.69 21.96
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
HCPCS Virgin PuertoCode Islands Rico
DNA - Does Not Apply

March 1995 DMERC Medicare Advisory Page 95-35
Please note that the allowances listed may not necessarily reflect your allowances.Remember that Medicare calculates your allowance for each procedure code using theprevailing charges, your actual charges and your customary charges. The lowest ofthese charges becomes your allowed charge.
For a profile of your customary charges, you may write to:
Palmetto GBAPricing UnitP.O. Box 100190Columbia, SC 29202
Be sure to include your NSC-assigned supplier number on all requests. If you have anyquestions please contact your Dedicated Work Team at (803) 691-4300.
1995 PEN PRICING
CODE DESCRIPTION PRICE
B4034 Enteral feeding supply kit; syringe, per day 5.60B4035 Enteral feeding supply kit; pump fed, per day 10.67B4036 Enteral feeding supply kit; gravity fed, per day 7.31B4081 Nasogastric tubing with stylet 19.78B4082 Nasogastric tubing without stylet 14.73B4083 Stomach tube - Levine type 2.25B4084 Gastrostomy/Jejunostomy tubing 16.52B4150 Enteral formulae; Category I: semi-synthetic intact protein/protein .61
Isolates, (e.g., Enrich, Ensure, Ensure HN, Ensure Powder, Isocal,Lonalac powder, Meritene, Meritene powder, Osmolite, Osmolite HN,Portagen powder, Sustacal, Renu, Sustagen powder, Travasorb) 100calories = 1 unit
B4151 Enteral formulae; Category I: natural intact protein/protein isolates, 1.43(e.g., Compleat B, Vitaneed, Compleat B Modified) 100 calories = 1 unit
B4152 Enteral formulae; Category II: intact protein/protein isolates .51(calorically dense) (e.g., Magnacal, Isocal HCN, Suscatal HC, EnsurePlus, Ensure Plus HN) 100 calories = 1 unit
B4153 Enteral formulae; Category III: hydrolized protein/amino acids, 1.74[e.g., Criticare HN, Vivonex HN, Vital (Vital HN), Travasorb HN, Isotein HN,Precision HN, PrecisionIsotonic] 100 calories = 1 unit
B4156 Enteral formulae; Category VI: standardized nutrients (Vivonex Std., 1.24Travasorb STD. Precision LR and Tolerex) 100 calories = 1 unit
B4164 Parenteral nutrition solution: carbohydrates (dextrose), 50% or less 15.08(500 ml = 1 unit) - homemix
B4168 Parenteral nutrition solution; amino acid, 3.5%, (500 ml = 1 unit) - homemix 21.96B4176 Parenteral nutrition solution; amino acid, 7% through 8.5%, (500 ml = 51.04
1 unit) - homemixB4178 Parenteral nutrition solution; amino acid, greater than 8.5% (500 ml = 1 unit) 51.04
- homemixB4180 Parenteral nutrition solution; carbohydrates (dextrose), greater than 21.61
50% (500 ml = 1 unit) - homemixB4184 Parenteral nutrition solution; lipids, 10% with administration set 70.86
(500 ml = 1 unit)B4186 Parenteral nutrition solution; lipids, 20% with administration set 94.48
(500 ml = 1 unit)B4189 Parenteral nutrition solution; compounded amino acid and carbohydrates 157.66
with electrolytes, trace elements, and vitamins, including preparation,any strength, 10 to 51 grams of protein - premix
B4193 Parenteral nutrition solution; compounded amino acid and carbohydrates 203.73with electrolytes, trace elements, and vitamins, including preparation,any strength, 52 to 73 grams of protein - premix
B4197 Parenteral nutrition solution; compounded amino acid and carbohydrates 248.02with electrolytes, trace elements and vitamins, including preparation,any strength, 74 to 100 grams of protein - premix
B4199 Parenteral nutrition solution; compounded amino acid and carbohydrates 283.42with electrolytes, trace elements and vitamins, including preparation,any strength, over 100 grams of protein - premix
B4216 Parenteral nutrition; additives (vitamins, trace elements, heparin, 6.85electrolytes) homemix per day
B4220 Parenteral nutrition supply kit; premix, per day 7.10B4222 Parenteral nutrition supply kit; home mix, per day 10.41B4224 Parenteral nutrition administration kit, per day 22.19B5000 Parenteral nutrition solution: compounded amino acid and carbohydrates 10.54
with electrolytes, trace elements, and vitamins, including preparation,any strength, renal - Amirosyn RF, Nephramine, Renamine - premix

Page 95-36 March 1995 DMERC Medicare Advisory
PEN PRICING(Cont'd)
B5100 Parenteral nutrition solution: compounded amino acid and carbohydrates 4.12with electrolytes, trace elements, and vitamins, including preparation,any strength, hepatic - Freamine HBC, hepatamine - premix
B5200 Parenteral nutrition solution: compounded amino acid and carbohydrates 5.68with electrolytes, trace elements, and vitamins, including preparation,any strength, stress - branch chain amino acids - premix
B9000MS Enteral nutrition infusion pump - without alarm 51.55B9000NU Enteral nutrition infusion pump - without alarm 1,121.97B9000RR Enteral nutrition infusion pump - without alarm 103.10B9000UE Enteral nutrition infusion pump - without alarm 841.47B9002MS Enteral nutrition infusion pump - with alarm 54.33B9002NU Enteral nutrition infusion pump - with alarm 1,121.97B9002RR Enteral nutrition infusion pump - with alarm 108.66B9002UE Enteral nutrition infusion pump - with alarm 841.47B9004MS Parenteral nutrition infusion pump, portable 177.15B9004NU Parenteral nutrition infusion pump, portable 2,238.01B9004RR Parenteral nutrition infusion pump, portable 354.30B9004UE Parenteral nutrition infusion pump, portable 1,678.51B9006MS Parenteral nutrition infusion pump, stationary 177.15B9006NU Parenteral nutrition infusion pump, stationary 2,238.01B9006RR Parenteral nutrition infusion pump, stationary 354.30B9006UE Parenteral nutrition infusion pump, stationary 1,678.51E0776NUXA IV Pole 93.30E0776RRXA IV Pole 23.62E0776UEXA IV Pole 29.15K0147 Gastrostomy tube, silicone with sliding ring 37.48XX030 Category IV Enteral product, 100 calories = 1 unit, Accupep HPF 1.99XX031 Category IV Enteral product, 100 calories = 1 unit, Aminaid 1.60XX032 Category IV Enteral product, 100 calories = 1 unit, Entera OPD 1.73XX033 Category IV Enteral product, 100 calories = 1 unit, Glucerna 1.09XX034 Category IV Enteral product, 100 calories = 1 unit, Hepatic Aid 5.16XX035 Category IV Enteral product, 100 calories = 1 unit, Impact 3.95XX036 Category IV Enteral product, 100 calories = 1 unit, Impact with fiber 4.05XX037 Category IV Enteral product, 100 calories = 1 unit, Imunaid 2.96XX038 Category IV Enteral product, 100 calories = 1 unit, Lipisorb 1.33XX039 Category IV Enteral product, 100 calories = 1 unit, Nepro .79XX040 Category IV Enteral product, 100 calories = 1 unit, New Replete 1.05XX041 Category IV Enteral product, 100 calories = 1 unit, New Replete with fiber 1.12XX042 Category IV Enteral product, 100 calories = 1 unit, Nutrihep 4.64XX043 Category IV Enteral product, 100 calories = 1 unit, Nutrivent .77XX044 Category IV Enteral product, 100 calories = 1 unit, Peptamen 3.26XX045 Category IV Enteral product, 100 calories = 1 unit, Perative 1.21XX047 Category IV Enteral product, 100 calories = 1 unit, Protain XL 1.14XX048 Category IV Enteral product, 100 calories = 1 unit, Provide 1.37XX049 Category IV Enteral product, 100 calories = 1 unit, Pulmocare .63XX050 Category IV Enteral product, 100 calories = 1 unit, Reabilan HN 3.09XX051 Category IV Enteral product, 100 calories = 1 unit, Suplena .52XX052 Category IV Enteral product, 100 calories = 1 unit, Stresstein 2.34XX053 Category IV Enteral product, 100 calories = 1 unit, Traumacal .69XX054 Category IV Enteral product, 100 calories = 1 unit, Traumaid HBC 2.20XX055 Category IV Enteral product, 100 calories = 1 unit, Travasorb Hepatic 4.24XX056 Category IV Enteral product, 100 calories = 1 unit, Travasorb MCT 1.10XX057 Category IV Enteral product, 100 calories = 1 unit, Travasorb Renal 1.81XX058 Category IV Enteral product, 100 calories = 1 unit, Vivonex T.E.N. 1.99XX059 Category V Enteral product, 100 calories = 1 unit, Casec 2.72XX060 Category V Enteral product, 100 calories = 1 unit, Controlyte .41XX061 Category V Enteral product, 100 calories = 1 unit, Elementra 10.00XX062 Category V Enteral product, 100 calories = 1 unit, Fibrad .43XX063 Category V Enteral product, 100 calories = 1 unit, Lipomul .52XX064 Category V Enteral product, 100 calories = 1 unit, MCT Oil 1.26XX065 Category V Enteral product, 100 calories = 1 unit, Microlipid .51XX066 Category V Enteral product, 100 calories = 1 unit, Moducal .43XX068 Category V Enteral product, 100 calories = 1 unit, Polycose .45XX069 Category V Enteral product, 100 calories = 1 unit, Promod .86XX070 Category V Enteral product, 100 calories = 1 unit, Promix 2.46XX071 Category V Enteral product, 100 calories = 1 unit, Propac 1.55XX072 Category V Enteral product, 100 calories = 1 unit, Sumacal .27XX073 Category IV Enteral Product, 100 calories = 1 unit, Advera 1.16XX074 Category IV Enteral Product, 100 calories = 1 unit, Crucial 3.31XX075 Category IV Enteral Product, 100 calories = 1 unit, Diabetisource 1.37XX076 Category IV Enteral Product, 100 calories = 1 unit, Isosource VHN 1.42
NOTE: The above information is for billing purposes and does not indicate or guaranteecoverage of the noted items.

March 1995 DMERC Medicare Advisory Page 95-37
1995 SURGICALDRESSING FEESCHEDULE
HCPCS AL AR CO FL G A K Y L A MS NC NM OK SC TN TX VI PR
A4460 0.92 0.92 0.92 0.92 0.92 0.92 0.92 0.92 0.92 0.92 0.92 0.92 0.92 0.92 0.92 0.82K0154 12.95 12.95 12.95 12.55 12.95 12.95 12.95 12.95 12.93 12.95 12.95 12.95 12.95 12.55 12.95 14.18K0196 6.62 6.62 6.62 6.62 6.62 6.62 6.62 6.62 6.62 6.62 6.62 6.62 6.62 6.62 6.62 7.95K0197 14.81 14.81 14.81 14.81 14.81 14.81 14.81 14.81 14.81 14.81 14.81 14.81 14.81 14.81 14.81 17.78K0199 4.76 4.76 4.76 4.76 4.76 4.76 4.76 4.76 4.76 4.76 4.76 4.76 4.76 4.76 4.76 5.69K0203 3.77 3.77 3.77 3.77 3.77 3.77 3.77 3.77 3.77 3.77 3.77 3.77 3.77 3.77 3.77 4.52K0204 3.18 3.18 3.18 3.18 3.18 3.18 3.18 3.18 3.18 3.18 3.18 3.18 3.18 3.18 3.18 3.81K0207 6.61 6.61 6.61 6.61 6.61 6.61 6.61 6.61 6.61 6.61 6.61 6.61 6.61 6.61 6.61 7.93K0209 6.75 6.75 6.75 6.75 6.75 6.75 6.75 6.75 6.75 6.75 6.75 6.75 6.75 6.75 6.75 8.11K0210 17.94 17.94 17.94 17.94 17.94 17.94 17.94 17.94 17.94 17.94 17.94 17.94 17.94 17.94 17.94 21.53K0211 26.46 26.46 26.46 26.46 26.46 26.46 26.46 26.46 26.46 26.46 26.46 26.46 26.46 26.46 26.46 31.74K0212 8.74 8.74 8.74 8.74 8.74 8.74 8.74 8.74 8.74 8.74 8.74 8.74 8.74 8.74 8.74 10.50K0214 9.27 9.27 9.27 9.27 9.27 9.27 9.27 9.27 9.27 9.27 9.27 9.27 9.27 9.27 9.27 11.13K0216 0.07 0.07 0.07 0.07 0.07 0.07 0.07 0.07 0.07 0.07 0.07 0.07 0.07 0.07 0.07 0.08K0217 0.39 0.39 0.39 0.39 0.39 0.39 0.39 0.39 0.39 0.39 0.39 0.39 0.39 0.39 0.39 0.46K0219 0.86 0.86 0.86 0.86 0.86 0.86 0.86 0.86 0.86 0.86 0.86 0.86 0.86 0.86 0.86 1.05K0220 2.32 2.32 2.32 2.32 2.32 2.32 2.32 2.32 2.32 2.32 2.32 2.32 2.32 2.32 2.32 2.77K0222 1.91 1.91 1.91 1.91 1.91 1.91 1.91 1.91 1.91 1.91 1.91 1.91 1.91 1.91 1.91 2.31K0223 2.17 2.17 2.17 2.17 2.17 2.17 2.17 2.17 2.17 2.17 2.17 2.17 2.17 2.17 2.17 2.60K0224 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.91K0229 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.25 3.91K0234 5.89 5.89 5.89 5.89 5.89 5.89 5.89 5.89 5.89 5.89 5.89 5.89 5.89 5.89 5.89 7.06K0235 15.16 15.16 15.16 15.16 15.16 15.16 15.16 15.16 15.16 15.16 15.16 15.16 15.16 15.16 15.16 18.20K0236 24.54 24.54 24.54 24.54 24.54 24.54 24.54 24.54 24.54 24.54 24.54 24.54 24.54 24.54 24.54 29.45K0237 7.12 7.12 7.12 7.12 7.12 7.12 7.12 7.12 7.12 7.12 7.12 7.12 7.12 7.12 7.12 8.55K0238 20.53 20.53 20.53 20.53 20.53 20.53 20.53 20.53 20.53 20.53 20.53 20.53 20.53 20.53 20.53 24.64K0240 11.03 11.03 11.03 11.03 11.03 11.03 11.03 11.03 11.03 11.03 11.03 11.03 11.03 11.03 11.03 13.25K0241 2.31 2.31 2.31 2.31 2.31 2.31 2.31 2.31 2.31 2.31 2.31 2.31 2.31 2.31 2.31 2.76K0242 5.47 5.47 5.47 5.47 5.47 5.47 5.47 5.47 5.47 5.47 5.47 5.47 5.47 5.47 5.47 6.56K0243 11.10 11.10 11.10 11.10 11.10 11.10 11.10 11.10 11.10 11.10 11.10 11.10 11.10 11.10 11.10 13.31K0244 35.38 35.38 35.38 35.38 35.38 35.38 35.38 35.38 35.38 35.38 35.38 35.38 35.38 35.38 35.38 42.46K0245 6.54 6.54 6.54 6.54 6.54 6.54 6.54 6.54 6.54 6.54 6.54 6.54 6.54 6.54 6.54 7.83K0246 8.93 8.93 8.93 8.93 8.93 8.93 8.93 8.93 8.93 8.93 8.93 8.93 8.93 8.93 8.93 10.72K0247 21.42 21.42 21.42 21.42 21.42 21.42 21.42 21.42 21.42 21.42 21.42 21.42 21.42 21.42 21.42 25.71K0248 14.63 14.63 14.63 14.63 14.63 14.63 14.63 14.63 14.63 14.63 14.63 14.63 14.63 14.63 14.63 17.55K0249 0.78 0.78 0.78 0.78 0.78 0.78 0.78 0.78 0.78 0.78 0.78 0.78 0.78 0.78 0.78 0.94K0251 1.80 1.80 1.80 1.80 1.80 1.80 1.80 1.80 1.80 1.80 1.80 1.80 1.80 1.80 1.80 2.16K0254 1.10 1.10 1.10 1.10 1.10 1.10 1.10 1.10 1.10 1.10 1.10 1.10 1.10 1.10 1.10 1.32K0255 2.73 2.73 2.73 2.73 2.73 2.73 2.73 2.73 2.73 2.73 2.73 2.73 2.73 2.73 2.73 3.26K0257 1.38 1.38 1.38 1.38 1.38 1.38 1.38 1.38 1.38 1.38 1.38 1.38 1.38 1.38 1.38 1.66K0258 3.87 3.87 3.87 3.87 3.87 3.87 3.87 3.87 3.87 3.87 3.87 3.87 3.87 3.87 3.87 4.64K0259 9.85 9.85 9.85 9.85 9.85 9.85 9.85 9.85 9.85 9.85 9.85 9.85 9.85 9.85 9.85 11.83K0262 0.99 0.99 0.99 0.99 0.99 0.99 0.99 0.99 0.99 0.99 0.99 0.99 0.99 0.99 0.99 1.18K0263 0.26 0.26 0.26 0.26 0.26 0.26 0.26 0.26 0.26 0.26 0.26 0.26 0.26 0.26 0.26 0.31K0264 0.44 0.44 0.44 0.44 0.44 0.44 0.44 0.44 0.44 0.44 0.44 0.44 0.44 0.44 0.44 0.54
INEXPENSIVE OR ROUTINELY PURCHASED (NEW)
CODE AL AR CO FL GA KY LA MS NC N M OK PR SC TN T X VIK0268 103.10 102.00 102.50 96.20 130.00 101.20 105.00 102.00 99.20 101.60 101.40 115.70 101.20 103.90 96.20 115.70
INEXPENSIVE OR ROUTINELY PURCHASED (USED)
CODE AL AR CO FL GA KY LA MS NC N M OK PR SC TN T X VIK0268 77.33 76.50 76.88 72.15 75.23 75.90 78.75 76.50 74.40 76.20 76.05 86.78 75.90 77.93 72.15 86.78
INEXPENSIVE OR ROUTINELY PURCHASED (RENTAL)
CODE AL AR CO FL GA KY LA MS NC N M OK PR SC TN T X VIK0268 10.31 10.20 10.25 9.62 10.03 10.12 10.50 10.20 9.92 10.16 10.14 11.57 10.12 10.39 9.62 11.57
1995 DME FEESCHEDULE FOR NEWHCPCS CODES
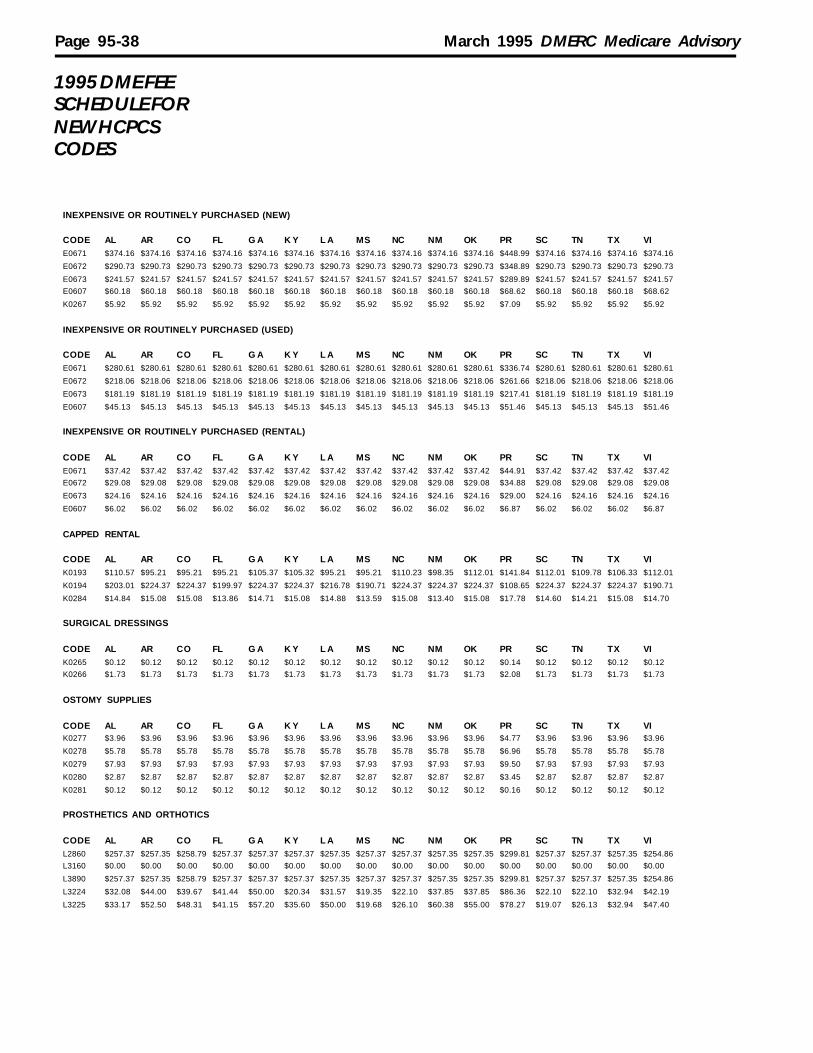
Page 95-38 March 1995 DMERC Medicare Advisory
1995 DME FEESCHEDULE FORNEW HCPCSCODES
INEXPENSIVE OR ROUTINELY PURCHASED (NEW)
CODE AL AR CO FL G A K Y L A MS NC NM OK PR SC TN TX VIE0671 $374.16 $374.16 $374.16 $374.16 $374.16 $374.16 $374.16 $374.16 $374.16 $374.16 $374.16 $448.99 $374.16 $374.16 $374.16 $374.16
E0672 $290.73 $290.73 $290.73 $290.73 $290.73 $290.73 $290.73 $290.73 $290.73 $290.73 $290.73 $348.89 $290.73 $290.73 $290.73 $290.73
E0673 $241.57 $241.57 $241.57 $241.57 $241.57 $241.57 $241.57 $241.57 $241.57 $241.57 $241.57 $289.89 $241.57 $241.57 $241.57 $241.57E0607 $60.18 $60.18 $60.18 $60.18 $60.18 $60.18 $60.18 $60.18 $60.18 $60.18 $60.18 $68.62 $60.18 $60.18 $60.18 $68.62
K0267 $5.92 $5.92 $5.92 $5.92 $5.92 $5.92 $5.92 $5.92 $5.92 $5.92 $5.92 $7.09 $5.92 $5.92 $5.92 $5.92
INEXPENSIVE OR ROUTINELY PURCHASED (USED)
CODE AL AR CO FL G A K Y L A MS NC NM OK PR SC TN TX VIE0671 $280.61 $280.61 $280.61 $280.61 $280.61 $280.61 $280.61 $280.61 $280.61 $280.61 $280.61 $336.74 $280.61 $280.61 $280.61 $280.61
E0672 $218.06 $218.06 $218.06 $218.06 $218.06 $218.06 $218.06 $218.06 $218.06 $218.06 $218.06 $261.66 $218.06 $218.06 $218.06 $218.06
E0673 $181.19 $181.19 $181.19 $181.19 $181.19 $181.19 $181.19 $181.19 $181.19 $181.19 $181.19 $217.41 $181.19 $181.19 $181.19 $181.19
E0607 $45.13 $45.13 $45.13 $45.13 $45.13 $45.13 $45.13 $45.13 $45.13 $45.13 $45.13 $51.46 $45.13 $45.13 $45.13 $51.46
INEXPENSIVE OR ROUTINELY PURCHASED (RENTAL)
CODE AL AR CO FL G A K Y L A MS NC NM OK PR SC TN TX VIE0671 $37.42 $37.42 $37.42 $37.42 $37.42 $37.42 $37.42 $37.42 $37.42 $37.42 $37.42 $44.91 $37.42 $37.42 $37.42 $37.42E0672 $29.08 $29.08 $29.08 $29.08 $29.08 $29.08 $29.08 $29.08 $29.08 $29.08 $29.08 $34.88 $29.08 $29.08 $29.08 $29.08
E0673 $24.16 $24.16 $24.16 $24.16 $24.16 $24.16 $24.16 $24.16 $24.16 $24.16 $24.16 $29.00 $24.16 $24.16 $24.16 $24.16
E0607 $6.02 $6.02 $6.02 $6.02 $6.02 $6.02 $6.02 $6.02 $6.02 $6.02 $6.02 $6.87 $6.02 $6.02 $6.02 $6.87
CAPPED RENTAL
CODE AL AR CO FL G A K Y L A MS NC NM OK PR SC TN TX VIK0193 $110.57 $95.21 $95.21 $95.21 $105.37 $105.32 $95.21 $95.21 $110.23 $98.35 $112.01 $141.84 $112.01 $109.78 $106.33 $112.01
K0194 $203.01 $224.37 $224.37 $199.97 $224.37 $224.37 $216.78 $190.71 $224.37 $224.37 $224.37 $108.65 $224.37 $224.37 $224.37 $190.71
K0284 $14.84 $15.08 $15.08 $13.86 $14.71 $15.08 $14.88 $13.59 $15.08 $13.40 $15.08 $17.78 $14.60 $14.21 $15.08 $14.70
SURGICAL DRESSINGS
CODE AL AR CO FL G A K Y L A MS NC NM OK PR SC TN TX VIK0265 $0.12 $0.12 $0.12 $0.12 $0.12 $0.12 $0.12 $0.12 $0.12 $0.12 $0.12 $0.14 $0.12 $0.12 $0.12 $0.12K0266 $1.73 $1.73 $1.73 $1.73 $1.73 $1.73 $1.73 $1.73 $1.73 $1.73 $1.73 $2.08 $1.73 $1.73 $1.73 $1.73
OSTOMY SUPPLIES
CODE AL AR CO FL G A K Y L A MS NC NM OK PR SC TN TX VIK0277 $3.96 $3.96 $3.96 $3.96 $3.96 $3.96 $3.96 $3.96 $3.96 $3.96 $3.96 $4.77 $3.96 $3.96 $3.96 $3.96
K0278 $5.78 $5.78 $5.78 $5.78 $5.78 $5.78 $5.78 $5.78 $5.78 $5.78 $5.78 $6.96 $5.78 $5.78 $5.78 $5.78
K0279 $7.93 $7.93 $7.93 $7.93 $7.93 $7.93 $7.93 $7.93 $7.93 $7.93 $7.93 $9.50 $7.93 $7.93 $7.93 $7.93
K0280 $2.87 $2.87 $2.87 $2.87 $2.87 $2.87 $2.87 $2.87 $2.87 $2.87 $2.87 $3.45 $2.87 $2.87 $2.87 $2.87
K0281 $0.12 $0.12 $0.12 $0.12 $0.12 $0.12 $0.12 $0.12 $0.12 $0.12 $0.12 $0.16 $0.12 $0.12 $0.12 $0.12
PROSTHETICS AND ORTHOTICS
CODE AL AR CO FL G A K Y L A MS NC NM OK PR SC TN TX VIL2860 $257.37 $257.35 $258.79 $257.37 $257.37 $257.37 $257.35 $257.37 $257.37 $257.35 $257.35 $299.81 $257.37 $257.37 $257.35 $254.86L3160 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00 $0.00
L3890 $257.37 $257.35 $258.79 $257.37 $257.37 $257.37 $257.35 $257.37 $257.37 $257.35 $257.35 $299.81 $257.37 $257.37 $257.35 $254.86
L3224 $32.08 $44.00 $39.67 $41.44 $50.00 $20.34 $31.57 $19.35 $22.10 $37.85 $37.85 $86.36 $22.10 $22.10 $32.94 $42.19
L3225 $33.17 $52.50 $48.31 $41.15 $57.20 $35.60 $50.00 $19.68 $26.10 $60.38 $55.00 $78.27 $19.07 $26.13 $32.94 $47.40

March 1995 DMERC Medicare Advisory Page 95-39
Please retain the list below as your new DMERC telephone directory.
Dedicated Work Teamsand DMERC GeneralInformation (803) 691-4300
Professional Relations (PR) Palmetto GBAProfessional Relations, Medicare Region C DMERCP.O. Box 100141Columbia, SC 29202-3141
PR General Information Number: (803) 735-1034
Individual extensions in Professional Relations may be reached by adding the number threein front of the person's extension. (Ombudsmen addresses and telephone numbers follow.)
Anti-Fraud Unit Palmetto GBAAnti-Fraud Unit, Medicare Region C DMERCP.O. Box 100236Columbia, SC 29202-3236
Anti-Fraud Hot-Line: (803) 788-5414
Individual extensions in the Anti-Fraud Unit may be reached by adding the number four in frontof the person's extension.
Hearings Palmetto GBAHearings Department, Medicare Region C DMERCP.O. Box 100249Columbia, SC 29202
Written Prior Authorization Palmetto GBAPrior Authorization Dept., Medicare Region C DMERCP.O. Box 100235Columbia, SC 29202-3235
Electronic Data Interchange Palmetto GBA(EDI) Electronic Data Interchange, Medicare Region C DMERC
P.O. Box 100145Columbia, SC 29202-3145
EDI Help-Line: (803) 788-9751
DMERC Region A (717) 735-9445DMERC Region B (317) 577-5722DMERC Region D (615) 251-8182
National Supplier Palmetto GBAClearinghouse (NSC) National Supplier Clearinghouse
P.O. Box 100142Columbia, SC 29202-3142(803) 754-3951
Statistical Analysis Durable Palmetto GBAMedical Equipment Regional Statistical Analysis Durable MedicalCarrier (SADMERC) Equipment Regional Carrier (SADMERC)
P.O. Box 100143Columbia, SC 29202-3143
HCPCS Help-Line: (803) 736-6809
REGION CDIRECTORY
Palmetto GBARegion C DMERCContacts
National Numbers

Page 95-40 March 1995 DMERC Medicare Advisory
GLOSSARY
AARP American Association of Retired PersonsAKA Also Known AsALJ Administrative Law JudgeANSI American National Standards InstituteARU Audio Response UnitAWP Average Wholesale PriceCMN Certificate of Medical NecessityCPAP Continuous Positive Airway PressureCPM Continuous Passive MotionCWF Common Working FileDME Durable Medical EquipmentDMEPOS Durable Medical Equipment, Prosthetics, Orthotics, and SuppliesDMERC Durable Medical Equipment Regional CarrierDOB Date of BirthEDI Electronic Data InterchangeEFT Electronic Funds TransferEMC Electronic Media ClaimEOB Explanation of BenefitsEOMB Explanation of Medicare BenefitsEPO Epoetin AlphaERN Electronic Remittance NoticeESRD End-Stage Renal DiseaseFDA Food and Drug AdministrationGHP Group Health PlanHCFA Health Care Financing AdministrationHCPCS HCFA Common Procedure Coding SystemHCT HematocritHICN Health Insurance Claim NumberHAØ Record NSF record that allows electronic submission of extra narrative data.ICD-9-CM International Classification of Diseases-9th Revision-Clinical ModificationIPPB Intermittent Positive Pressure BreathingMCM Medicare Carrier's ManualMSP Medicare Secondary PayerNDC National Drug CodeNSC National Supplier ClearinghouseNSF National Standard FormatNTIS National Technical Information ServiceOBRA 93 Omnibus Budget Reconciliation Act of 1993OCNA Other Carrier Name & AddressOIG Office of Inspector GeneralP & O Prosthetics & OrthoticsPalmetto GBA Palmetto Government Benefits AdministratorsPDR Physician's Desk ReferencePEN Parenteral and Enteral NutritionPOS Place of ServicePOV Power Operated VehicleRMRP Regional Medical Review PoliciesRRB Railroad Retirement BoardSAC Supplier Advisory CommitteeSADMERC Statistical Analysis Durable Medical Equipment Regional CarrierTENS Transcutaneous Electrical Nerve StimulatorUPIN Unique Physician Identification Number
The Region C DMERC Medicare Advisory is published by Palmetto Government Benefits Administrator's Professional RelationsDepartment for suppliers and providers of DMEPOS.

March 1995 DMERC Medicare Advisory Page 95-41
- NOTES -

Page 95-42 March 1995 DMERC Medicare Advisory
- NOTES -

March 1995 DMERC Medicare Advisory Page 95-43
- NOTES -