-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
The body has multiple systems that help regulate and maintain
normal housekeeping – nervous, circulatory, immune, endocrine and
gastrointestinal systems, to name a few. These systems not only
modulate different tissues and organs to function properly, but
also facilitate communications both within the system and with
other systems.
As recent as the 1990s, another system was identified and termed
the Endocannabinoid System. It also helps with communication, and
it prepares the body against attack by a variety of harmful
insults: stress, carcinogens, pain, inflammation, infections, UV
damage, etc. Initially the definition was confined to what were
referred to as the endocannabinoids (ECs), that being two molecules
– arachidonoylethanolamide or anandamide (AEA) and
2-arachidonoylgycerol (2-AG) – produced by the body which act on
the two cannabinoid receptors (CB1 and CB2) located throughout the
body (mainly the central nervous system and immune system,
respectively). The enzymes that help in the synthesis and breakdown
of ECs were included as part of the system.
Further research has since identified more players thought to
have critical roles in this system, including additional enzymes,
other receptors (including some “orphan” receptors), as well as
other molecules that the body produces including fatty acids
palmitoylethanolamide (PEA), oleolylethanolamide (OEA),
stearolyethanolamide (SEA), linoylethanolamide (LEA) etc. As a
result, the definition of this vital system has been expanded
within the scientific community to be more encompassing, and now
is
Palmitoylethanolamide (PEA) is an 18-carbon long-chain fatty
acid that is typically found in eggs, milk, cheese, meats and
peanuts, and is especially abundant in soy lecithin (Appendix
1).
PEA is an intriguing health molecule that has been studied for
over eighty years. What makes it unique is being a natural molecule
made by the body whenever the demand arises; for example, during
stress (psychological and physical), infections (viral and
bacterial [e.g., colds and flu]), various forms of inflammation,
trauma, allergies, pain, cardiac disease, kidney disease and
obesity. It is responsible for maintaining overall cellular health
or homeostasis.
In the body, PEA is synthesized from the phospholipids which
make up all membranes. Since all cells are made up of membranes, it
is no wonder PEA is found everywhere in the body and is available
to all cells efficiently and quickly. PEA is significant not only
as a cellular messenger, relaying information to and fro in the
body, but also in acting as a quick fix or solution to cellular
needs. In short, PEA is a go-to-molecule which maintains optimal
cellular health throughout the body.
Synthesis of PEA takes place by the enzyme N-acylated
phosphatidylethanolamine–phospholipase
referred to as the Endocannabinoidome. In common parlance,
however, it is still referred to as the Endocannabinoid System,
hence the title of this White Paper.
BAC KGRO UND: THE ENDOCANNABINOID SYSTEM
INTRODUCTION: PALMITOYLETH ANOL AMIDE (P EA)
Palmitoylethanolamide (PEA): The Multiple Target Molecule
By Dr. Traj Nibber, Founder and CEO of Advanced Orthomolecular
Research
KEY PLAYER IN THE ENDOCANNABINOID SYSTEM
PEA: The Multiple Target Molecule
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
D (NAPE-PLD). Once PEA has performed its function, it is rapidly
broken down by two enzymes, fatty acid amide hydrolase (FAAH) and
N-acylethanolamine acid amide hydrolase (NAAA) (Fig. 1).
ORIGIN
Alvin F. Coburn first studied PEA while researching the effects
of egg yolk in preventing the recurrence of rheumatic fever in poor
children living in New York in 1939. He found that the phospholipid
fraction in egg yolk could effectively prevent streptococcal
infection. Additional follow-up studies in New York as well as
Chicago confirmed the effectiveness of the phospholipid fraction
during outbreaks of infection. Later, soy phospholipids were found
to be a more plentiful and cheaper source, and it was confirmed
that PEA was indeed the active fraction. Since then, PEA has been
extensively studied in numerous health conditions (Appendix 2).
MECH ANISM O F ACT IO N
It is important to know how a drug works, especially at the
molecular level. Knowing a drug’s “mechanism of action” allows
researchers to develop optimal formulations, dose and delivery
systems to be tested in clinical trials. It took almost fifty years
after PEA’s initial discovery before its mechanism of action was
finally worked out. The credit for this goes to Italian
researcher Rita Levi-Montalcini and her work in the early 1990s.
Italian scientists remain world leaders in the field of PEA
research.
PEA has actions both in the central nervous system and the
peripheral nervous system. However, PEA does not have a direct
effect on CB1 or CB2 receptors, which differentiates it from the
action of specific phytocannabinoids derived from marijuana or hemp
(e.g., cannabidiol [CBD] or tetrahydrocannabinol [THC]). Instead,
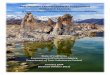
PEA works through a number of different mechanisms (Fig. 2). •
Direct action by down-regulating the mast cells. Mast cells are
present throughout the body and play a key role in immunity,
inflammation, allergies and neural health. PEA has been shown to
either prevent their recruitment to the site of damage and/or
inhibit their degranulation or release of histamine and other key
inflammatory mediators in many pathological conditions. Researchers
have shown that when treated with PEA, mast cells switch from an
“active” stage to a “resting” phenotype, meaning they become
dormant. This suggests PEA could be a powerful molecule for immune
health, inflammation, pain, neuro-protection and especially
allergies.
• Direct action on orphan receptors like GPCR55 and GPR119 that
produce results similar to the classical activation of the CB1 and
CB2 receptors by phytocannabinoids like THC and CBD.
• Direct action on the perioxisome proliferator activated
receptor alpha and delta and gamma (PPAR-alpha, delta and gamma).
PPARs are transcription factors in the nucleus that can switch on
and off genes that control pain and inflammation. PPARs also have
other functions in obesity and glucose metabolism.
• Indirect action on other receptors like transient receptor
potential vanilloid-type 1 (TRPV1, also known as capsaicin
receptor), which opens or closes ion channels allowing a flow of
sodium, magnesium and potassium ions into cells and is associated
with transferring pain signals.
• Direct action by inhibiting enzymes such as fatty acid amide
hydrolase (FAAH) and monoacylglycerol (MAGL) that degrade the
naturally produced endocannabinoids (ECs) AEA and 2-AG
respectively, thus allowing for prolonged therapeutic action of
these ECs on CB2 receptors.
PEA: The Multiple Target Molecule
Figure 1. Diagrammatic representation of the synthesis and
breakdown of PEA.(Source: Skaper et al., 2018, p. 15)
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
UNIQUE EFFECTS OF PE A
Entourage EffectThe entourage effect is an indirect mechanism of
action whereby the biological effects of ECs and phytocannabinoids
are enhanced by related naturally produced molecules like PEA,
which do not produce those effects by themselves. The enhanced
effect may occur either by preventing the breakdown of ECs or
phytocannabinoids through inhibiting the enzymes that degrade them,
or by increasing the receptor binding affinity of ECs or
phytocannabinoids. PEA has been shown to display the entourage
effect in different health conditions. An elegant demonstration of
this occurred in hypertensive rats, where it was observed that
blood pressure was reduced with the addition of PEA to otherwise
ineffective doses of AEA (Garcia et al., 2009).
Cannabinomimetic effectsA remarkable feature of PEA is that its
chemical structure is very similar to the ECs (both AEA and 2-AG),
even more so than the phytocannabinoids (derived from various
sources, chiefly hemp and marijuana) (Fig. 3). In fact, the
structural similarities allow PEA to produce effects similar to the
ECs as well as enhancing the effects ofexogenous
phytocannabinoids.
PEA Formulation and BioavailabilityPEA is a lipid molecule so it
has poor solubility, absorption and overall bioavailability. In
order to overcome these hurdles, novel delivery systems are
required, including nano-emulsions, liposomes, solid lipid
particles and other nano-delivery systems (Conte et al., 2017).
Alternatively, bioavailability may also be improved through
by-passing the first-pass effect of the liver, so that absorption
occurs via the lymphatic system as opposed to the circulatory
system (Zgair et al., 2017).
FIG URE 2. DIAGR AM M ATIC REP RESENTATION OF MECH ANISMS OF
ACTION OF PEA.
PEA: The Multiple Target Molecule
A shows synthesis and breakdown. B depicts a direct effect of
PEA on PPAR-alpha and GPR55 receptors. C depicts a direct effect of
PEA by inhibiting FAAH enzyme, thereby elevating AEA and 2-AG
levels which activate CB2 and TRPV1 receptors. D depicts an
indirect effect on TRPV1 by having a direct effect on AEA and 2AG.
E shows a direct effect of PEA on PPAR-alpha. (Source: Petrosino
& Di Marzo, 2017, p. 1351)
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
FIG URE 3 . CHE M ICAL STRUCTU RES OF PEA, ENDOCANNABINOIDS AND
PHYTOCANNABINOIDS.
PEA: The Multiple Target Molecule
(Source: Tsuboi et al., 2018, p. 2)
CLINICAL AP PL ICAT ION SAs stated previously, PEA is the body
’s go-to-molecule and is made on demand when required under disease
conditions. Due to its ubiquitous nature and presence in all cells,
PEA has wide-ranging therapeutic applications.
1. Analgesic EffectsPEA is produced by the body as a
“compensatory factor” when confronted with pain. At least 6,000
patients with chronic pain and inflammation have been entered into
clinical trials of PEA since the first studies in the 1970s. PEA
has shown to be an important therapeutic molecule with an
impressively positive risk/benefit ratio. Further, recent data
support the hypothesis of deficient synthesis of PEA in pathologic
states. For example, a study on fibromyalgia described deficient
synthesis of PEA in the trapezius muscles in patients, and proposed
that supplementation with PEA might be a useful therapeutic
intervention in this chronic condition
(Ghaufori et al., 2013). This deficiency theory is not unlike
the hypothesis of Ethan Russo, a long time researcher of
cannabinoids, who first proposed in 2004 that a deficiency in the
ECs may exist and be the causative factor in many pathological
conditions (Russo, 2004). Several studies have shown that when PEA
is used concurrently with opioid-type drugs (e.g., Tapentadol) for
lower back pain, the dose of the opioid was significantly reduced,
which alleviated some of the side-effects of the drug (Passavanti
et al., 2017).
2. Chronic Pain One of the most important public health problems
worldwide, chronic pain remains a major challenge in medicine and
can have serious impact on quality of life. While acute pain is
self-limiting and usually easily dealt with, chronic pain is more
difficult to address and causes significant personal and social
issues. Depending on its origin, chronic pain can be classified as
inflammatory (e.g., osteoarthritis, rheumatoid arthritis) or
neuropathic. Neuropathic pain can arise
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
from a disease or injury to the central or peripheral nervous
systems; thermal and mechanical pain stimuli are amplified
(hyperalgesia), while stimuli which were previously undetected are
now perceived as aching (allodynia). PEA was found to exert pain
relief in various animal models of inflammatory and neuropathic
pain (Luongo et al., 2017). In all these models of pain, there was
a significant decrease in plasma PEA levels. Increasing ECs and/or
PEA levels lessened pain perception and also increased pain
threshold levels. The analgesic effects of PEA were found to be due
to either increasing AEA levels via inhibiting its breakdown by
FAAH enzymes, or direct action on PPAR receptors and opening up
TRPV1 channels, with the cumulative effect being reduction of pain
signals.
3. Anti-Inflammatory Action Numerous animal models have
documented the anti-inflammatory action of PEA, including rat paw
edema, phorbol ester-induced ear edema, colitis, as well as topical
application of various irritants. There is likely a two-pronged
approach to this action. First, PEA prevents mast cell activation
and release of numerous contents (degranulation), including
histamine, inflammatory cytokines, chemokines, tryptases and
proteases. Second, PEA stimulation of PPAR-alpha likely also
mediates the anti-inflammatory action by preventing NF-kappaB
translocation from the cytoplasm into the nucleus that would
otherwise activate the inflammatory cascade.
4. Neuro-ProtectionInflammation can be especially perilous where
the nervous system is involved, that is, neuro-inflammation. The
microglia, mast cells and astrocytes play a critical role in the
health of the nervous system. However, it can be a Jekyll and Hyde
scenario – when acutely activated these cells help resolve the
inflammation, but if the inflammation is chronic (e.g., diabetes,
obesity or other conditions) then these cells create havoc in the
brain and may be causative factors in various neurological
disorders like Alzheimer ’s, Parkinson’s, multiple sclerosis,
autism, amyotrophic lateral sclerosis, cerebral ischemia and
traumatic brain injury. All three cells communicate with each other
or cross-talk, with each apprising the other of any changes in the
local environment (Appendix 3).
PEA levels are three times higher than EC levels in the central
nervous system, suggesting PEA plays a major role in
neuro-protection. PEA is locally produced and broken down in mast
cells and microglia,
helping to modulate their behavior. In this regard, PEA acts as
a local enforcer of the very cells that produce it. Deficiency of
PEA may lead to cognitive issues like dementia, depression and
other motor abnormalities. Animal studies have shown improved
neuronal survival with PEA supplementation, as well as prevention
of localized neuro-inflammation via multiple pathways.
5. PEA for Preventing Flu, Colds and Upper Respiratory
Infections Between 1969 and 1975 six large human clinical studies
to evaluate the effectiveness of PEA to reduce the number of days
lost to colds and flu were conducted in the former Czechoslovakia.
Five of these were in adults (groups of factory workers and
soldiers) and one in children. In these double blind placebo
controlled studies, patients were monitored for high temperature,
headaches, sore throats, muscle pain, coughs and general malaise
and fatigue.
The effectiveness of PEA in reducing all the symptoms and days
lost to illness was very impressive (Appendix 4), and effects were
evident usually within the second week of the treatment. In all six
studies, PEA had clear treatment effect in reducing the incidence
and frequency of respiratory infections and was found to be an
effective influenza prophylaxis. No side-effects were observed.
Health authorities observed the ease of application of PEA, and
noted its potential in flu epidemics.
6. Antioxidant PEA has been shown to neutralize the damaging
effects of free radicals by binding to them and preventing their
destructive action. This is particularly important for the extra
sensitive and highly prone neurons.
7. Allergies Due to its powerful mast cell stabilization
properties, PEA should be useful in all forms of allergies,
including airborne, food and contact allergic dermatitis. When
activated, mast cells are key initiators of allergic responses
through their release of inflammatory and allergic mediators like
histamine, prostaglandins and other growth factors. Additionally,
mast cells interact or cross-talk with other key players in the
inflammatory process, including dendritic cells, macrophages,
lymphocytes etc. Antihistamines work by preventing histamine
release. PEA should be a powerful alternative with
PEA: The Multiple Target Molecule
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
its inhibiting action on mast cell degranulation, and without
the side-effect of drowsiness caused by antihistamines.
8. MigraineTraditional phytocannabinoids like CBD and THC,
and/or their combination, have been documented to produce
anti-migraine effects. With migraines, EC levels decrease, and
increasing ECs has been shown to reduce migraine episodes. Due to
its structural similarity to ECs, it is conceivable that PEA may be
helpful in migraine management.
9. DepressionOver 350 million people world-wide are affected by
depression, with women at twice the risk as men. It is estimated
one in twenty people in the Western world suffer from at least one
depressive episode in a year. Despite the use of antidepressants,
less than one-third achieve remission, and many still have residual
depressive symptoms. Antidepressants work by increasing monoamines
like serotonin and norepinephrine in the central nervous system.
PEA has been shown to exert antidepressant and anxiolytic
properties in animal models of depression (Crupi et al., 2013; Yu
et al., 2011). It has also been shown to prevent the spreading of
cortical depression wave following traumatic brain injury or
cerebral ischemia. Notably, antidepressants have been found to
increase levels of PEA in the brain, suggesting a protective role
of PEA during depression. There is also a link between stress and
low plasma PEA levels.
Animal studies have demonstrated that PEA can produce
antidepressant effects similar to the drug fluvoxamine. Researchers
in Iran studied the effect of PEA as an adjunct to the popular
antidepressant drug citalopram in a double blind placebo controlled
study. By week two, the citalopram plus PEA group experienced
significantly greater antidepressant effect than the citalopram
alone group (Ghazizadeh-Hashemi et al., 2018).
The antidepressant effect of PEA is likely to be multifactorial
with TRPV1 receptor activation of TRPV1 and PPAR’s alpha, delta and
gamma, but possibly other receptors like GPR55 as well. Finally,
PEA’s inhibition of FAAH and NAAA enzymes that degrade AEA may also
contribute to its antidepressant effect.
10. Digestive Disorders and a Key Role of PEA in Gut-Brain Axis
The gastrointestinal tract has a dense concentration of cannabinoid
receptors for AEA and 2-AG to maintain gut homeostasis and modulate
gut motility and secretion of digestive enzymes. These play a key
role in intestinal inflammatory diseases like inflammatory bowel
diseases (IBD) such as Crohn’s disease and ulcerative colitis, and
inflammatory bowel syndrome (IBS). Recently, a double blind placebo
controlled study has shown the efficacy of PEA in reducing pain
severity in IBS patients (Barbara et al., 2014). This is consistent
with PEA’s anti-inflammatory and analgesic effects. In previous
animal models it has been shown that PEA is produced by the colon
in response to inflammatory insults, and that PEA supplementation
exerts anti-inflammatory effects in the gut; colon weight and
length, which are considered a reliable and sensitive indicator of
severity of inflammation, were markedly reduced by PEA (Borrelli et
al., 2014). A more recent twelve-week study in IBS patients showed
that PEA (dose of palmithoylethanolamide/polydatin 200 mg/20 mg
twice a day) significantly reduced pain severity and improved
quality of life (Cremon et al., 2017). Additional animal studies
seem to suggest that PEA may also play a protective role in liver
fibrosis and liver damage (Ohara et al., 2018).
The gut microbiome and the endocannabinoid system seem to be
intertwined and cross-talk with each other on matters of energy
utilization, thus impacting obesity and diabetes. Additional
research suggests that PEA may also influence the gut microbiome in
a positive manner, especially in affecting intestinal permeability
(e.g., leaky gut syndrome). PEA seems to act as “gate keeper” and
reduces permeability through the tight junctions of any pathogenic
gut microbes, preventing their entry into circulation which could
cause low grade inflammation affecting various organs like the
liver.(Cani et al., 2016) (Appendices 5 and 6).
The gut-brain axis refers to the link between the gut and brain
and the bidirectional communication and interactions that have
physiological and psychological effects. Due to the strong
interaction of the endocannabinoid system with both the
gastrointestinal tract and the brain, PEA is an ideal molecule for
addressing gut-brain axis issues.
PEA: The Multiple Target Molecule
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
11. Cardiovascular and Cerebrovascular Role Recently, plasma PEA
has been shown to have strong association with, and may be
predictive of, coronary dysfunction in morbidly obese individuals,
and as such has been proposed as a novel bio-marker in heart
disease. Moreover, due to its non-invasiveness, plasma PEA level
testing may be more acceptable and cost effective compared to
coronary angiography (Quercioli et al., 2017). However, more work
needs to be done to establish whether the sensitivity and
specificity of PEA could reach the standards for clinical
application.
Numerous animal studies have shown that PEA plays a major role
in neuro-protection. PEA acts on the glial cells which are the key
immune cells in the brain that constantly survey the environment
(immunosurveillance) in preparation for insult and injury,
especially neuro-inflammation of the brain (e.g., cerebrovascular
injury like stroke). Recently, a combination of PEA and the
antioxidant flavonoid luteolin was evaluated in 250 stroke patients
for neurological improvement in cognition, pain, degree of
spasticity and quality of life. There was significant improvement
in all the clinical indices, and evidence suggests a role for this
formulation in stroke prevention and recovery (Caltagirone et al.,
2016).
12. Cannabis DependencyPEA may be an innovative treatment for
cannabis dependency since it has remarkable chemical structural
similarities to the endogenous cannabinoids (AEA and 2-AG), even
more structurally similar than phytocannabinoids derived from
cannabis (THC or CBD). PEA may act as an antagonist and/or agonist
to block various receptors and have a powerful entourage effect
(Coppola and Mondola, 2013). This hypothesis needs to be confirmed.
Some predicted effects of PEA include: 1) clinically significant
reduction in withdrawal symptoms in cannabis dependent patients; 2)
clinically significant reduction of craving in cannabis dependent
patients; 3) clinically significant reduction of cannabis
consumption; and 4) prevention of cannabis-induced neurotoxicity
and neuro-psychiatric disorders. Whether PEA may play an important
role in reducing dependency and help in the opioid crisis remains
to be seen.
13. Autism Spectrum DisorderWhilst the exact mechanism for
autism is not fully understood, glutamate excitotoxicity of the
neurons and neuro-inflammation are thought to be
the key mechanisms involved. In addition, there is overactivity
of mast cells. This excessive activation may be controlled by PEA
since it helps modulate mast cells. A recent human clinical trial
showed that PEA may augment the effects of risperidone, a
prescription drug used to treat autism-related irritability and
hyperactivity disorder, thus allowing reduction of the required
dose. With PEA, the microglial cells were protected and there was
evidence of improved synaptic plasticity and higher levels of
dopamine. A reduced dose of risperidone meant fewer side-effects of
the prescription drug (Khalaj et al., 2018). Other case reports
have confirmed PEA having beneficial effects (Bertolino et al.,
2017; Antonucci et al., 2015). Large scale studies need to be
conducted.
C ONC LUSIONSThis fat-derived signalling compound has a long
history, with PEA’s effects on pain being known for half a century.
It is not a classic endocannabinoid, despite having some metabolic
and structural similarities to other so-called ‘signalling’
molecules. It is now receiving more attention in the areas of
chronic pain, inflammation and other diseases. Because it interacts
with several receptors it has potential in numerous applications
requiring ‘multiple target’ approaches.
PEA: The Multiple Target Molecule
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
REFERENCESdell’Istituto superiore di sanità, 53, 125-134.
23. Iuvone, T. et al. (2016). Ultramicronized
palmitoylethanolamide reduces viscerovisceral hyperalgesia in a rat
model of endometriosis plus ureteral calculosis: Role of mast
cells. Pain, 157, 80-91.
24. Kahlich, R. et al. (1979). Studies on prophylactic effcacy
of N-2-hydroxyethyl palmitamide (Impulsin) in acute respiratory
infections. Serologically controlled field trials. Journal of
Hygiene Epidemiology Microbiology and Immunology, 23, 11-24.
25. Keppel Hesselink, J.M., de Boer, T. et Witkamp, R.F. (2013).
Palmitolyethanolamide: A natural body-own anti-inflammatory agent,
effective and safe against influenza and common cold. International
Journal of Inflammation, 2013:151028.
http://dx.doi.org/10.1155/2013/151028
26. Khalaj, M. et al. (2018). Palmitoylethanolamide as
adjunctive therapy for autism: Efficacy and safety results from a
randomized controlled trial. Journal of Psychiatric Research, 103,
104-111.
27. Kilaru, A., Blancaflor, E. B., Venables, B. J.,
Tripathy, S., Mysore, K. S. et Chapman, K.D. (2007). The
N-acylethanolamine-mediated regulatory pathway in plants. Chemistry
and Biodiversity, 4, 1933-1955.
28. Lam, P.M., Marczylo, T. H. et Konje, J.C. (2010).
Simultaneous measurement of three N-acylethanolamides in human
bio-matrices using ultra performance liquid chromatography–tandem
mass spectrometry. Analytical and Bioanalytical Chemstry, 398,
2089-2097.
29. Luongo, L., Starowicz, K., Maione, S. et Di Marzo, V.
(2017). Allodynia lowering induced by cannabinoids and
endocannabinoids (ALICE). Pharmacological Research, 119,
272-277.
30. Masek, K., Perlik, F., Klima, J. et Kahlich, R. (1974).
Prophylactic efficacy of N-2-hydroxyethyl palmitamide (Impulsin) in
acute respiratory tract infections. European Journal of Clinical
Pharmacology, 7, 415-419.
31. Mounessa, J. S., Siegel, J. A., Dunnick, C.A. et
Dellavalle, R.P. (2017). The role of cannabinoids in dermatology.
Journal of the American Academy of Dermatology, 77, 188-190.
32. Ohara, M. et al. (2018). Palmitoylethanolamide ameliorates
carbon tetrachloride-induced liver fibrosis in rats. Frontiers in
Pharmacology, 9:709. http://dx.doi.org/10.3389/fphar.2018.00709
33. Orefice, N. S., Alhouayek, M., Carotenuto, A., Montella, S.,
Barbato, F. et Comelli, A. (2016). Oral palmitoylethanolamide
treatment is associated with reduced cutaneous adverse effects of
interferon-β1a and circulating proinflammatory cytokines in
relapsing-remitting multiple sclerosis. Neurotherapeutics, 13,
428-438.
34. Paladini, A., Fusco, M., Cenacchi, T., Schievano, C.,
Piroli, A. et Varrassi, G. (2016). Palmitoylethanolamide, a special
food for medical purposes, in the treatment of chronic pain: A
pooled data meta-analysis. Pain Physician, 19, 11-24.
35. Palma, E., Reyes-Ruiz, J.M., Lopergolo, D., Roseti, C.,
Bertollini, C. et Ruffolo, G. (2016). Acetylcholine receptors from
human muscle as pharmacological targets for ALS therapy.
Proceedings of the National Academy of Sciences of the U.S.A., 113,
3060-3065.
36. Passavanti, M.B. et al. (2017). The beneficial use of
ultramicronized palmitoylethanolamide as add-on therapy to
Tapentadol in the treatment of low back pain: A pilot study
comparing prospective and retrospective observational arms. BMC
Anesthesiology, 17, 171-178.
37. Petrosino, S. et Di Marzo, V. (2017). The pharmacology
of palmitoylethanolamide and first data on the therapeutic efficacy
of some of its new formulations. British Journal of Pharmacology,
174, 1349-1365.
38. Phan, N. Q., Siepmann, D., Gralow, I. et Ständer S.
(2010). Adjuvant topical therapy with a cannabinoid receptor
agonist in facial postherpetic neuralgia. Journal of the German
Society of Dermatology, 8, 88-91.
39. Plesnik, V., Havrlantova, M., Jancova, J., Januska, J. et
Macková, O. (1977). Impulsin in the prevention of acute respiratory
diseases in school children. Ceskoslovenská Pediatrie, 32,
365-369.
40. Quercioli, A. et al. (2017). Plasma palmitoylethanolamide
(PEA) as a potential biomarker for impaired coronary function.
International Journal of Cardiology, 231, 1-5.
41. Russo, E. (2004). Clinical endocannabinoid deficiency
(CECD): Can this concept explain therapeutic benefits of cannabis
in migraine, fibromyalgia, irritable bowel syndrome and other
treatment-resistant conditions? Neuro Endocrinology Letters, 25,
31-39.
42. Schuel, H. et al. (2002). N-acylethanolamines in human
reproductive fluids. Chemisty and Physics of Lipids, 121,
211-227.
43. Sharma, C., Sadek, B., Goyal, S.M., Sinha, S., Kamal, M.A.
et Ojha, S. (2015). Small molecules from nature targeting G-protein
coupled cannabinoid receptors:
1. Antonucci, N., Cirillo, A. et Siniscalco, D. (2015).
Beneficial effects of palmitoylethanolamide on expressive language,
cognition, and behaviors in autism: A report of two cases. Case
Reports in Psychiatry, 2015:325 061.
http://dx.doi.org/10.1155/2015/325061 Barbara, G., Cremon, C. et
Stanghellini, V. (2014). Inflammatory bowel disAntonucciease and
irritable bowel syndrome: Similarities and differences. Current
Opinion in Gastroenterology, 30, 352-358.
2. Barry, A. et al. (2018). Plasma N-acylethanolamine and
endocannabinoid levels in burning mouth syndrome: Potential role in
disease pathogenesis. Journal of Oral Pathology and Medicine, 47,
440-442.
3. Bertolino, B. et al. (2017). Beneficial effects of
co-ultramicronized palmitoylethanolamide/luteolin in a mouse model
of autism and in a case report of autism. CNS Neuroscience and
Therapuetics, 23, 87-98.
4. Borrelli, F. et al. (2015). Palmitoylethanolamide, a
naturally occurring lipid, is an orally effective intestinal
anti-inflammatory agent. British Journal of Pharmacology, 172,
142-158.
5. Brotini, S., Schievano, C. et Guidi, L. (2017).
Ultra-micronized palmitoylethanolamide: An efficacious adjuvant
therapy for Parkinson’s disease. CNS and Neurological Disorders
Drug Targets, 16, 705-713.
6. Bruun, S. et al. (2018). Satiety factors oleylethanolamide,
stearoylethanolamide, and palmitoylethanolamide in mother ’s milk
are strongly associated with infant weight at four months of
age–data from the Odense Child Cohort. Nutrients, 10:1747.
https://doi.org/10.3390/nu10111747
7. Caltagirone, C. et al. (2016). Co-ultramicronized
palmitoylethanolamide/luteolin in the treatment of cerebral
ischemia: From rodent to man. Translational Stroke Research, 7,
54-69.
8. Cani, P.D., Plovier, H., Van Hul, M., Geurts, L., Delzenne,
N.M., Druart, C. et Everard, A. (2016). Endocannabinoids–at the
crossroads between the gut microbiota and host metabolism. Nature
Reviews – Endocrinology, 12, 133-143.
9. Chirchiglia, D., Chirchiglia, P. et Signorelli, F. (2018).
Nonsurgical lumbar radiculopathies treated with ultramicronized
palmitoylethanolamide (umPEA): A series of 100 cases. Neurologia i
neurochirurgia polska, 52, 44-47.
10. Clemente, S. (2012). Amyotrophic lateral sclerosis treatment
with ultramicronized palmitoylethanolamide: A report of two cases.
CNS and Neurological Disorders Drug Targets, 11, 933-936.
11. Conte, R., Marturano, V., Peluso, G., Calarco, A. et
Cerruti, P. (2017). Recent advances in nanoparticle-mediated
delivery of anti-inflammatory phytocompounds. International Journal
of Molecular Sciences, 18, 709-732.
12. Coppola, M. et Mondola, R. (2013). Palmitoylethanolamide:
From endogenous cannabimimetic substance to innovative medicine for
the treatment of cannabis dependence. Medical Hypotheses, 81,
619-622.
13. Cordaro, M. et al. (2017). Effects of a co-micronized
composite containing palmitoylethanolamide and polydatin in an
experimental model of benign prostatic hyperplasia. Toxicology and
Applied Pharmacology, 329, 231-240.
14. Cremon, C. et al. (2017). Randomised clinical trial: The
analgesic properties of dietary supplementation with
palmitoylethanolamide and polydatin in irritable bowel syndrome.
Alimentary Pharmacology and Therapeutics, 45, 909-922.
15. Crupi, R., Paterniti, I., Ahmad, A., Campolo, M., Esposito,
E. et Cuzzocrea, S. (2013). Effects of palmitoylethanolamide and
luteolin in an animal model of anxiety/depression. CNS and
Neurological Disorders Drug Targets, 12, 989-1001.
16. Del Giorno, R., Skaper, S., Paladini, A., Varrassi, G.
et Coaccioli, S. (2015). Palmitoylethanolamide: Results from
prospective and retrospective observational studies. Pain and
Therapy, 4, 169-178.
17. Eberlein, B., Eicke, C., Reinhardt, H.W. et Ring, J. (2008).
Adjuvant treatment of atopic eczema: assessment of an emollient
containing N-palmitoylethanolamine (ATOPA study). Journal of the
European Academy of Dermatology and Venereology, 22, 73-82.
18. Garcia, M.C., Adler-Graschinsky, E. et Celuch, S.M. (2009).
Enhancement of the hypotensive effects of intrathecally injected
endocannabinoids by the entourage compound palmitoylethanolamide.
European Journal of Pharmacology, 610, 75-80.
19. Ghaufori, N., Ghafouri, B., Larsson, B., Stensson, N.,
Fowler, C. J. et Gerdle, B. (2013). Palmitoylethanolamide and
stearoylethanolamide levels in the interstitium of the trapezius
muscle of women with chronic widespread pain and chronic
neck-shoulder pain correlate with pain intensity and sensitivity.
Pain, 154, 1649-1658.
20. Ghazizadeh-Hashemi, M. et al. (2018). Palmitoylethanolamide
as adjunctive therapy in major depressive disorder: A double blind,
randomized and placebo-controlled trial. Journal of Affective
Disorders, 232, 127-133.
21. Gouveia-Figueira, S. et Nording, M.L. (2014). Development
and validation of a sensitive UPLC-ESI-MS/MS method for the
simultaneous quantification of 15 endocannabinoids and related
compounds in milk and other biofluids. Analytical Chemistry, 86,
1186-1195.
22. Indraccolo, U., Indraccolo, S. R. et Mignini, F.
(2017). Micronized palmitoylethanolamide/trans-polydatin treatment
of endometriosis-related pain: A meta-analysis. Annali
PEA: The Multiple Target Molecule
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
REFERENCESPotential leads for drug discovery and development.
Evidence-Based Complementary and Alternative Medicine, 2015:
238482. http://dx.doi.org/10.1155/2015/238482
44. Skaper, S.D. et al. (2014). Palmitoylethanolamide, a
naturally occurring disease-modifying agent in neuropathic pain.
Inflammopharmacology, 22, 79-94.
45. Skaper, S.D., Facci, L., Zusso, M. et Giusti, P. (2018). An
inflammation-centric view of neurological disease: Beyond the
neuron. Frontiers in Cellular Neuroscience, 12:72.
http://dx.doi.org/10.3389/fncel.2018.00072
46. Tsuboi, K., Uyama, T., Okamoto, Y. et Ueda, N. (2018).
Endocannabinoids and related N-acylethanolamines: Biological
activities and metabolism. Inflammation and Regeneration, 38:28.
https://doi.org/10.1186/s41232-018-0086-5
47. Venables, B.J., Waggoner, C.A. et Chapman, K.D. (2005).
N-aAcylethanolamines in seeds of selected legumes. Phytochemistry,
66, 1913-1918.
48. Visse, K., Blome, C., Phan, N. Q., Augustin, M. et
Ständer, S. (2017). Efficacy of body lotion containing
N-palmitoylethanolamide in subjects with chronic pruritus due to
dry skin: a dermatocosmetic study. Acta Dermato-Venerologica, 97,
639-641.
49. Yu, H. L., Deng, X.Q., Li, Y. J., Li, Y. C.,
Quan, Z. S. et Sun, X.Y. (2011). N-palmitoylethanolamide, an
endocannabinoid, exhibits antidepressant effects in the forced swim
test and the tail suspension test in mice. Pharmacological Reports,
63, 834-839.
50. Zgair, A. et al. (2017). Oral administration of cannabis
with lipids leads to high levels of cannabinoids in the intestinal
lymphatic system and prominent immunomodulation. Nature Scientific
Reports, 7:14542. http://doi.org/10.1038/s41598-017-15026-z
PEA: The Multiple Target Molecule
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
PEA: The Multiple Target Molecule
APPENDIX 1 . CO M M O N FOOD S OURC ES OF PALMITOYLET H A N OL
AM ID E (PEA)
APPENDIX 2. PAL M ITOYL E T H ANOL AMIDE (PEA) EFFICACY IN
CLINICAL STUD IE S A ND CL IN ICAL APPLICATIONS
Food Source
Pathology
References
References
Concentration of PEA (ng·g—1 fresh weight)
Bovine Milk
Elk Milk
Human Breast Milk
Human breast milk (110 ± 32.3 lactation days)
Common bean (Phaseoulus vulgaris)
Garden pea (Pisum sativum)
Southern or black-eyed peas (Vigna unguiculata)
Tomato
Medicago sativa
Corn
Soybean (Glycine max)
Soy lecithin
Peanut (Arachis hypogaea)
Amyotrophic lateral sclerosis
Autism
Benign prostatic hyperplasia (especially a combination of PEA
with R+Lipoic acid)
Burning mouth syndrome
0.25
1.81
8.98 ± 3.35 nmol·L—1
23.4 ± 7.2 nmol·L—1
53.5
100
138
100
1150
200
6700
950 000
3730
Gouveia-Figueira & Nording, 2014
Gouveia-Figueira & Nording, 2014
Lam et al., 2010
Schuel et al., 2002
Venables et al., 2005
Venables et al., 2005; Kilaru et al., 2007
Venables et al., 2005
Kilaru et al., 2007
Venables et al., 2005
Kilaru et al., 2007
Venables et al., 2005; Kilaru et al., 2007
Kilaru et al., 2007
Venables et al., 2005; Kilaru et al., 2007
Amyotrophic lateral sclerosis
Antonucci et al., 2015; Bertolino et al., 2017
Cordaro et al., 2017
Barry et al., 2018
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
PEA: The Multiple Target Molecule
APPENDIX 3. D IAGR AM M AT IC R EPRESENTATION OF THE C ROSS-TALK
BETWEE N M AST CE L L AND MIC ROGLIA, TWO KEY PL AYERS IN
NEURO-INFL AM M AT IO N
Pathology References
Chronic pain (including neuropathic pain) of differing
etiologies
Dermatological uses including pruritus, facial postherpetic
neuralgia, atopic eczema, contact dermatitis and non-specified
itch
Endometriosis
Fibromyalgia
Improving satiety and thus supporting weight loss
Non-surgical lumbar radiculopathies
Parkinson’s disease (adjuvant therapy)
Relapsing-remitting multiple sclerosis (add-on therapy for the
treatment of interferon-β1a-related adverse effects)
Stroke (adjuvant therapy)
Skaper et al., 2014; Paladini et al., 2016
Visse et al., 2017; Phan et al., 2010; Eberlein et al., 2008;
Mounessa et al., 2017
Iuvone et al., 2016; Indraccolo et al., 2017
Del Giorno et al., 2015
Bruun et al., 2018
Chirchiglia et al., 2018
Brotini et al., 2017
Orefice et al., 2016
Caltagirone et al., 2016
(Source: Skaper et al., 2018, p. 7)
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
PEA: The Multiple Target Molecule
APPENDIX 4. E FFE CT IVE NE S S OF PALMITOYLETH ANOL AMIDE (PEA)
ON COL D S A ND FL U IN A SERIES OF C LINICAL STUDIES CONDUCTED IN
CZE CHOS LOVAKIA
Study year % ProtectionPEA (n) Significance (p)Placebo (n)
References
1972a
1972b
1973
1974
1975
19771
223
436
436
411
235
196
221
463
465
199
118
224
45%
32%
34%
52%
59%
16%
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
PEA: The Multiple Target Molecule
(Source: Cani et al., 2016, p.3)
APPENDIX 5. S HOW IN G CE RTAIN “ GATEKEEPERS” OF THE TIGHT
JUNCT IO N S AL LOW E N TRY OF MIC ROBES INTO THE CIRCUL ATION CAUS
IN G LOW GR ADE INFL AMMATION
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
PEA: The Multiple Target Molecule
(Source: Cani et al., 2016, p. 5)
APPENDIX 6. S HOW IN G PAL M ITOYLETH ANOL AMIDE (PEA) ACTS AS A
“GATEKE E PE R” TO M AIN TAIN TH AT THE TIGHT J UNCTIONS REMAIN
LOCKE D AND PRE VE N T ENTRY OF MIC ROBES INTO THE CIR CUL AT
ION
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com
PEA: The Multiple Target Molecule
APPENDIX 7. S H OW IN G T HE E F FECTS OF NATUR ALLY PRODUC ED
MOLECULES L IK E PAL M ITOYL ETH ANOL AMIDE (PEA) ON VARIOUS DISE
AS E S
Antioxidant
Antiapoptotic
Anticancer
Chemogenic Pain
Renal Injury
Obesity
Lipid Dysregulation
Diabetes
Brain Cancer
Inflammatory Bowel Disease
Endometriosis
Anti-Inflammatory
Alcohol Addiction
Depression
Anxiety
Neuropathic Pain
Alzheimer’s Disease
Cerebral Ischemia
Ulcerative Colitis
GlucoseHomeostasis
(Source: Sharma et al., 2015, p. 3)
-
AOR Canad a39 00 - 12 St re et NECalg a r y, AB Ca na da T2 E
8H91-8 0 0 -3 87 -017 7 | a or.ca
AO R US3 0 I ndu st r ia l West C l ifton, NJ 0 7 0121-86 6 -215
-0 45 0 | aorhealth.com