Embed Size (px)
Citation preview

Pancreatic Cancer
Malcolm J. Moore MD
Princess Margaret Hospital
Pancreatic Cancer
US incidence: 32,180 new cases estimated for 20051
– 2% of all new cancer cases
Screening, early detection not on the horizon
Most patients are diagnosed with advanced disease
1 CA Cancer J Clin 2005;55:10-30
Pancreatic Cancer – Outcome is Poor
US mortality: 31,800 deaths estimated for 20051
– 4th and 5th leading cause of cancer-related death in males and females, respectively
– 5% to 6% of all cancer deaths
5 year survival less than 5%2.
Median survival 3-4
– metastatic disease 3-6 months
– locally advanced disease 9 months
– Resected disease 14 months1 CA Cancer J Clin 2005;55:10-302 SEER Cancer Statistics Review. http://seer.cancer.gov3 Am J Surg 1993;165:68 4 JCO 2005; 23:4538
Pancreatic Cancer
Epidemiology
– Increases with age
– No major geographical differences
Genetics
– P16, DPC, p53, k-ras
Familial
– Poorly understood
Pancreatic Tumors
Most are ductal adenocarcinomas.
– Most common site is head of pancreas
– Dense fibrous reaction.
– Precursor lesions – PanIN
Other subtypes
– Adenosquamous
– Acinar cell, medullary, undifferentiated
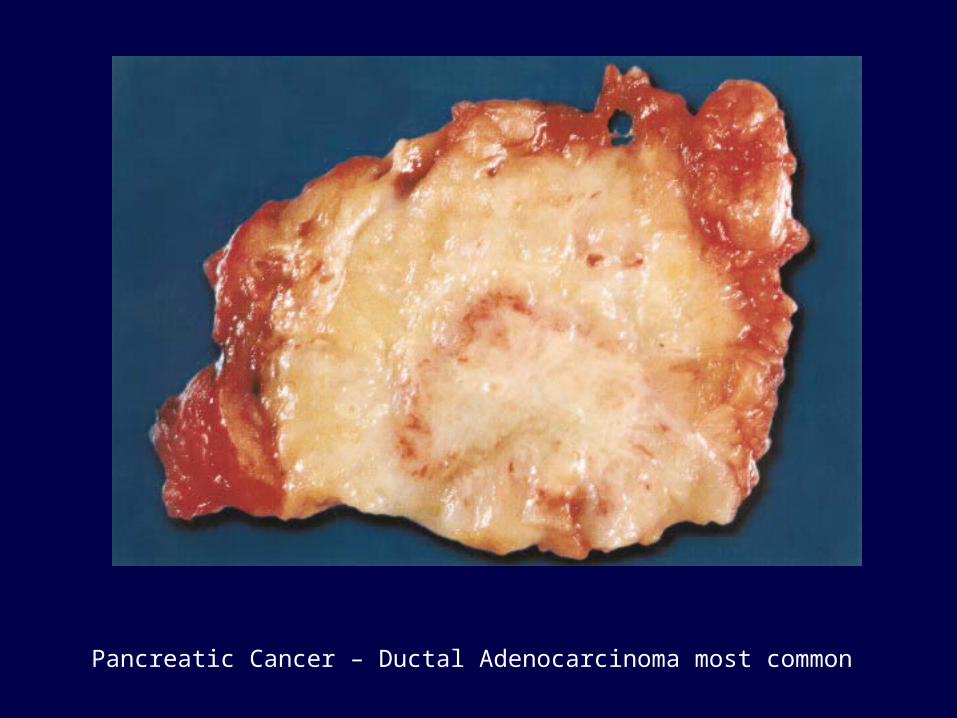
Pancreatic Cancer – Ductal Adenocarcinoma most common
Pancreatic Tumors
Serous cystadenoma/adenocarcinoma.
Mucinous neoplasms
Endocrine tumors
– Range of differentiation-not all malignant
– Functioning vs non
– Well circumscribed
– VascularTumors of the pancreas, Armed Forces Institute of Pathology, Washington 1997. p.145.
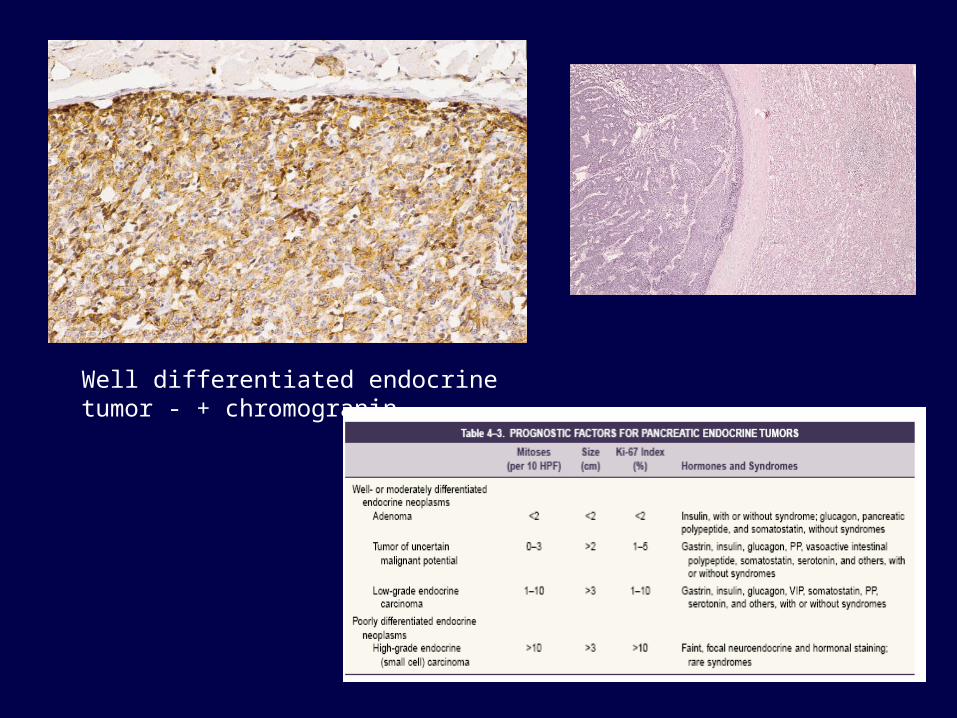
Well differentiated endocrine tumor - + chromogranin
Pathology
Most are ductal adenocarcinoma– But not all, so …
– Biopsy essential
– Although usually can predict non-adenocarcinoma by imaging or clinical course.
Making the diagnosisCommon symptoms
Pain
Gastric obstruction
Biliary obstruction
Diabetes
Hypercoaguability
Malabsorption

CA 19-9
Tumor associated antigen
Elevated in most cases of pancreatic cancer.
Also elevated in other GI cancers, pancreatitis.
Slightly better specificity and sensitivity than CEA.
Unknown value in clinical studies.
Am J Gastroenterol 1999;94:1941-6.
Pain Pancreatic Cancer
Pain often due to local invasion of tumor.
Improved by XRT +/- chemo in 35-65% of cases
Improved by palliative chemo
Celiac axis blocks
Pancreatic Cancer Gastric/duodenal obstruction
Occurs in cancers of pancreatic head.
Consider in patients with refractory nausea/vomiting
Remedies are
– Gastrojejunostomy- open or laparoscopic
– Duodenal stenting
? Role of prophylactic gastrojejunostomy
Pancreatic CancerBiliary obstruction
Cancers of pancreatic head.
Often presenting problem.
? Surgical vs Endoscopic stenting.
– Both effective.
– Surgery a better long term solution.
– Stent occlusion/replacement
Percutaneous drainage not recommended
Pancreatic CancerDiabetes
? A risk factor for disease.
Can be a presenting problem.
More than just loss of pancreatic function.
Treat symptomatically.
Not a contraindication to steroids
HypercoaguabilityWell recognized association -Trousseau’s
syndrome.
Can be both central and peripheral.
Generally resistant to oral agents.
Long term therapy required.
Association with early deaths
? Role of prophylactic anti-coagulation
Malabsorption
Pancreatic insufficiency
One reason for weight loss
Use of narcotics may mask usual symptoms
Trial of pancreatic enzymes
Surgery
Only 15-20% are resectable.
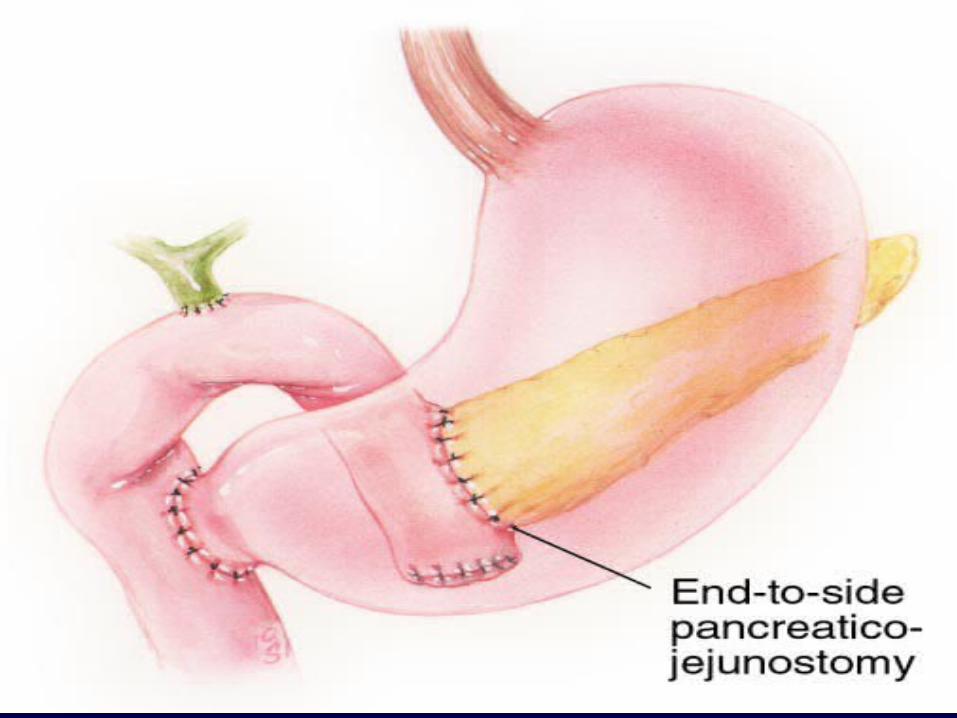
Whipples resection (pancreaticoduodenectomy) for tumors of the head
– 3 anastamoses
– Should be done in high volume centres
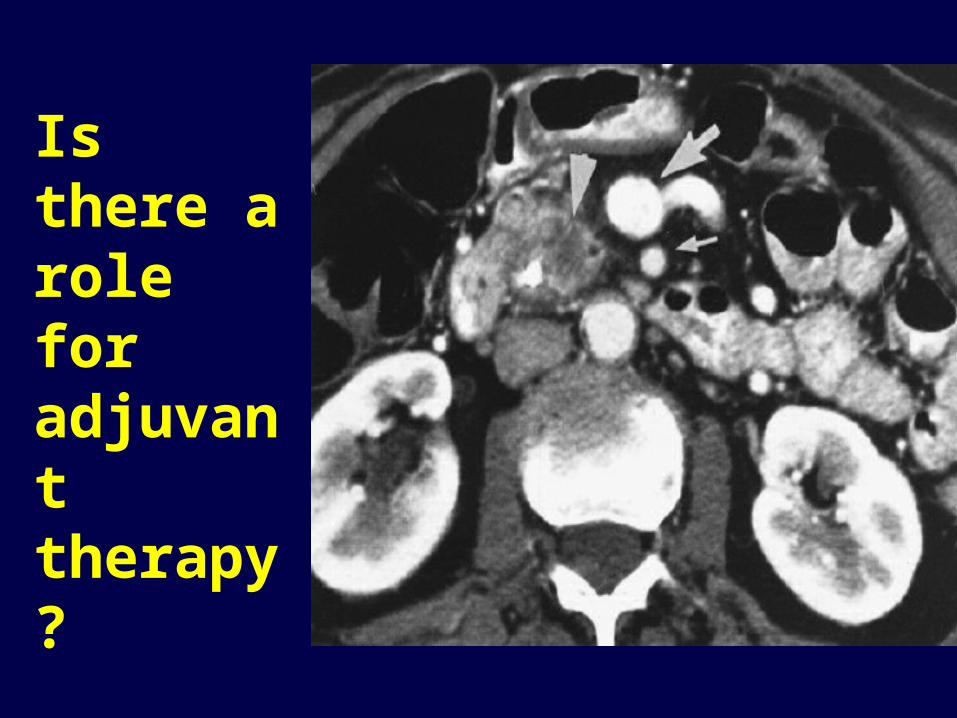
Is there a role for adjuvant therapy?

Original Adjuvant TrialGITSG [N=43]1
Median survival 20 versus 11 months
5 year survival 18 vs 8%
But… - 43 patients in 8 years.
A larger EORTC trial (n=114 pancreatic cancer) failed to confirm the benefit of adjuvant CRT 2
5-FU + XRT with systemic 5-FU X 1 yr
vs
No additional treatment
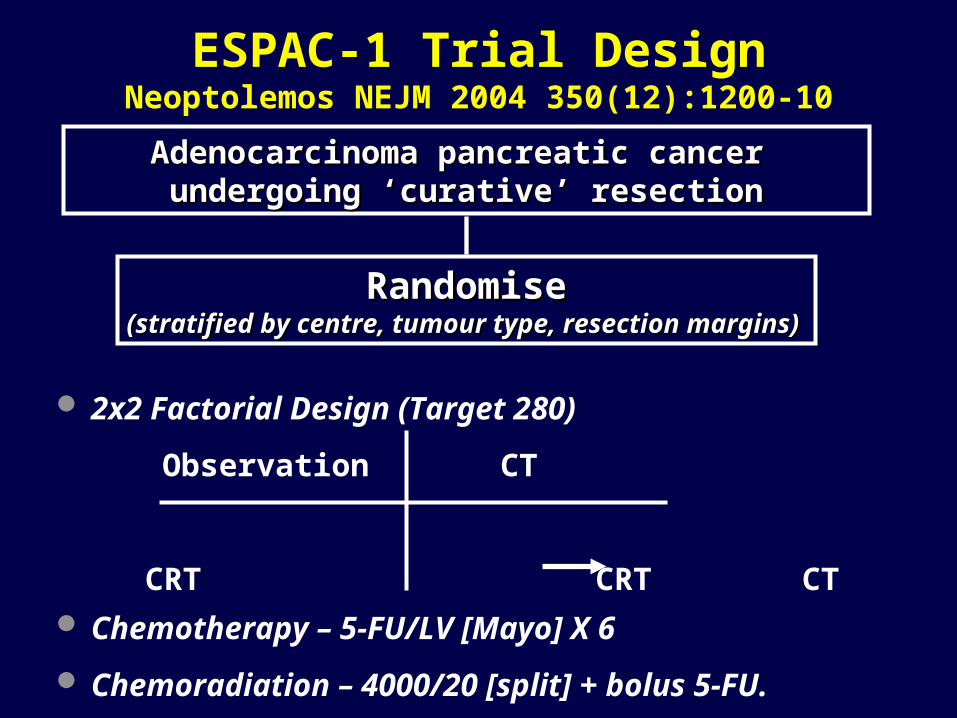
ESPAC-1 Trial DesignNeoptolemos NEJM 2004 350(12):1200-10
2x2 Factorial Design (Target 280)
Observation CT
CRT CRT CT Chemotherapy – 5-FU/LV [Mayo] X 6
Chemoradiation – 4000/20 [split] + bolus 5-FU.
Adenocarcinoma pancreatic cancer Adenocarcinoma pancreatic cancer undergoing ‘curative’ resectionundergoing ‘curative’ resection
RandomiseRandomise(stratified by centre, tumour type, resection margins)(stratified by centre, tumour type, resection margins)
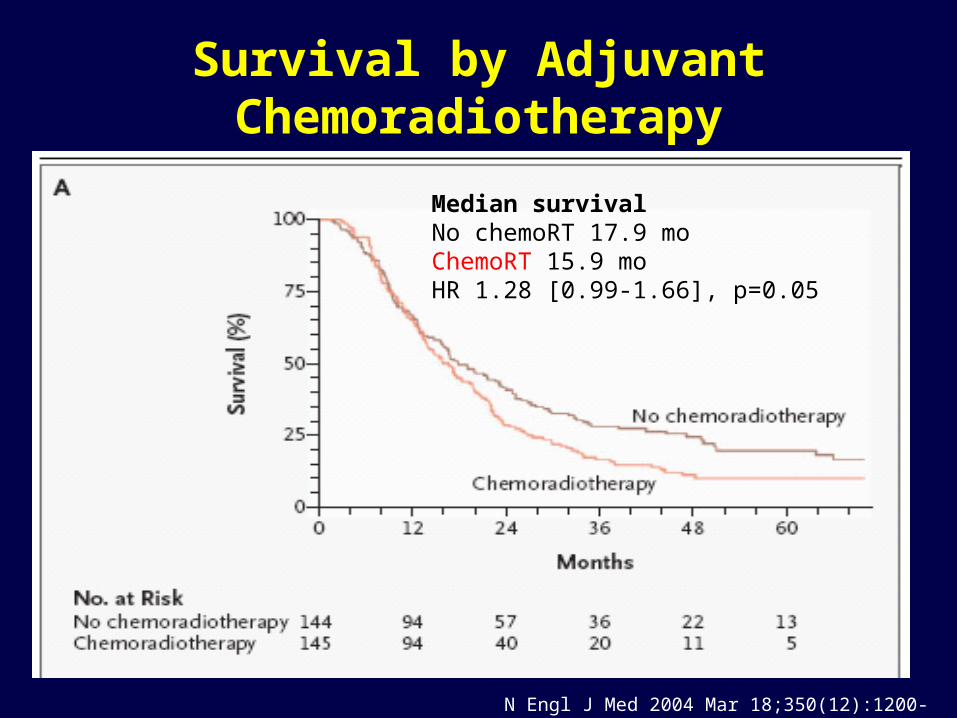
Survival by Adjuvant Chemoradiotherapy
Median survivalNo chemoRT 17.9 moChemoRT 15.9 moHR 1.28 [0.99-1.66], p=0.05
N Engl J Med 2004 Mar 18;350(12):1200-10
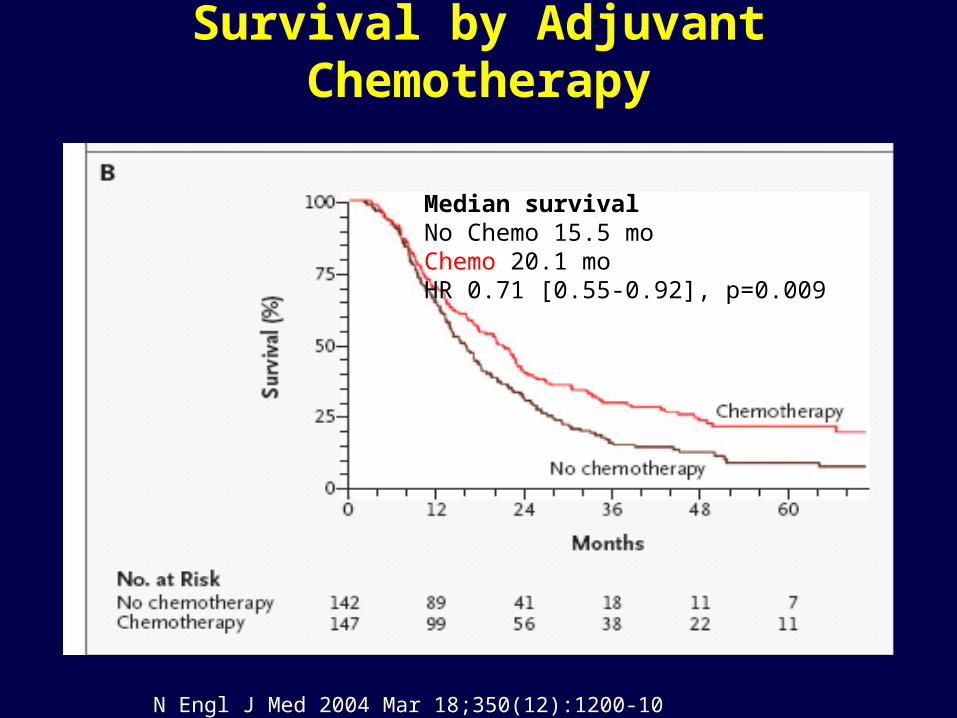
Survival by Adjuvant Chemotherapy
Median survivalNo Chemo 15.5 moChemo 20.1 moHR 0.71 [0.55-0.92], p=0.009
N Engl J Med 2004 Mar 18;350(12):1200-10
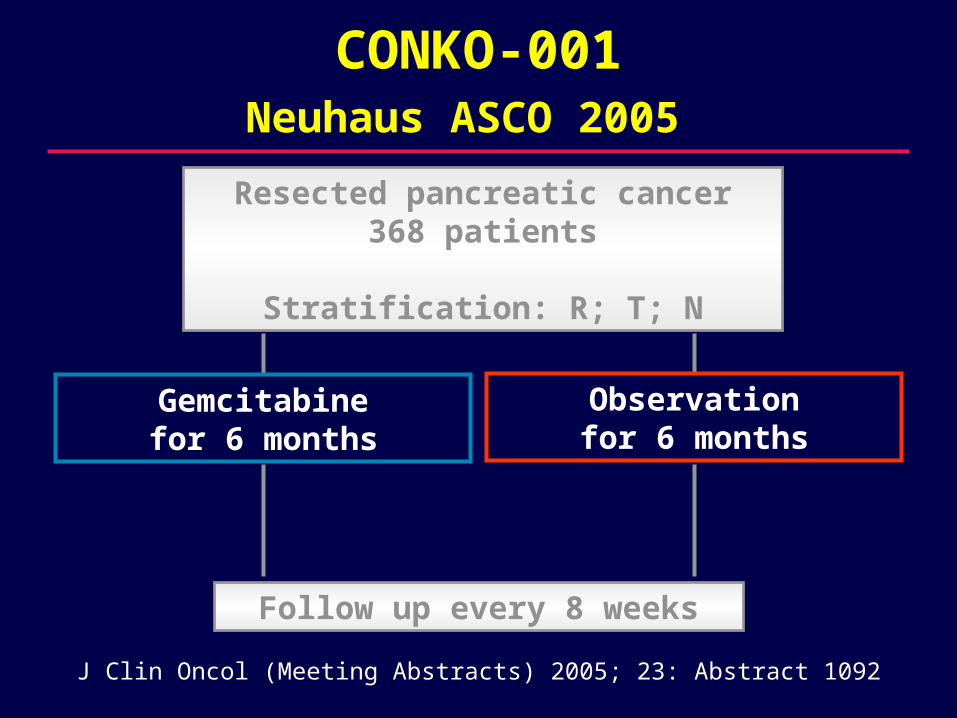
CONKO-001Neuhaus ASCO 2005 Resected pancreatic cancer
368 patients
Stratification: R; T; N
Follow up every 8 weeks
Gemcitabinefor 6 months
Observationfor 6 months
J Clin Oncol (Meeting Abstracts) 2005; 23: Abstract 1092
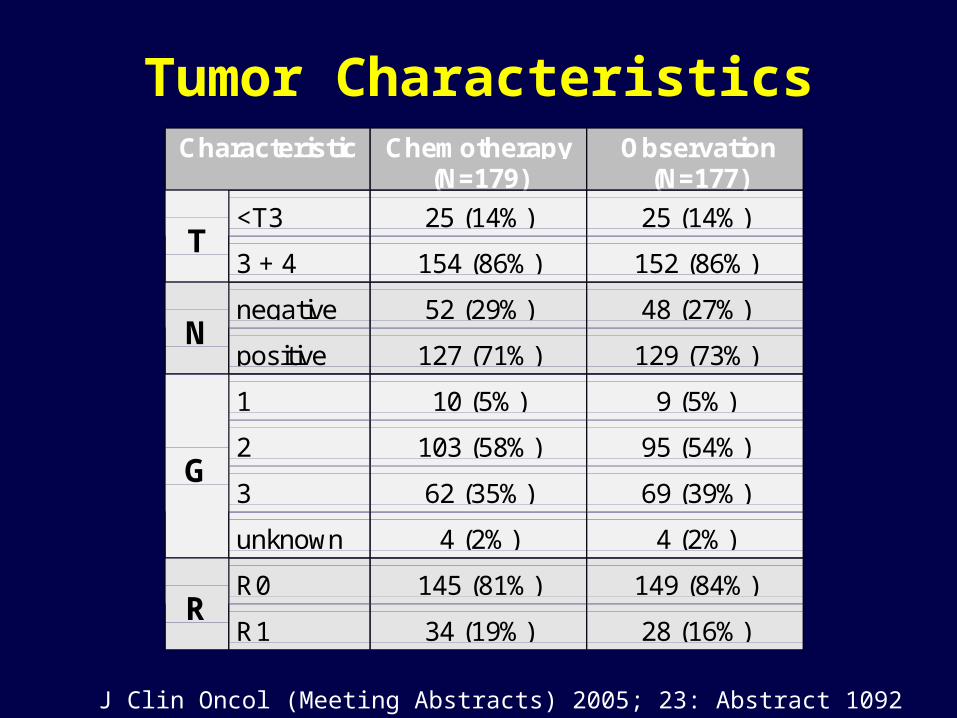
Tumor CharacteristicsCharacteristic Chemotherapy
(N=179)Observation
(N=177)
<T3 25 (14%) 25 (14%)T
3 + 4 154 (86%) 152 (86%)
negative 52 (29%) 48 (27%)N
positive 127 (71%) 129 (73%)
1 10 (5%) 9 (5%)
2 103 (58%) 95 (54%)
3 62 (35%) 69 (39%)G
unknown 4 (2%) 4 (2%)
R0 145 (81%) 149 (84%)R
R1 34 (19%) 28 (16%)
J Clin Oncol (Meeting Abstracts) 2005; 23: Abstract 1092
months
847260483624120
cu
mu
lative
dis
ea
se
fre
e s
urv
iva
l100%
75%
50%
25%
0%
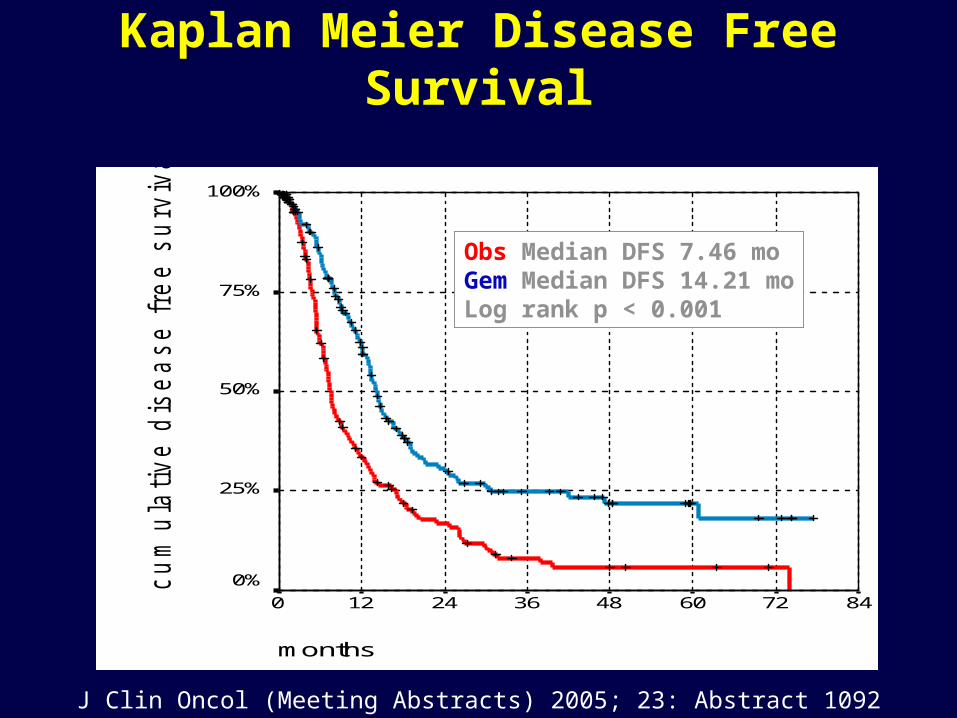
CONKO-001 Kaplan Meier Disease Free Survival
Obs Median DFS 7.46 mo Gem Median DFS 14.21 moLog rank p < 0.001
J Clin Oncol (Meeting Abstracts) 2005; 23: Abstract 1092
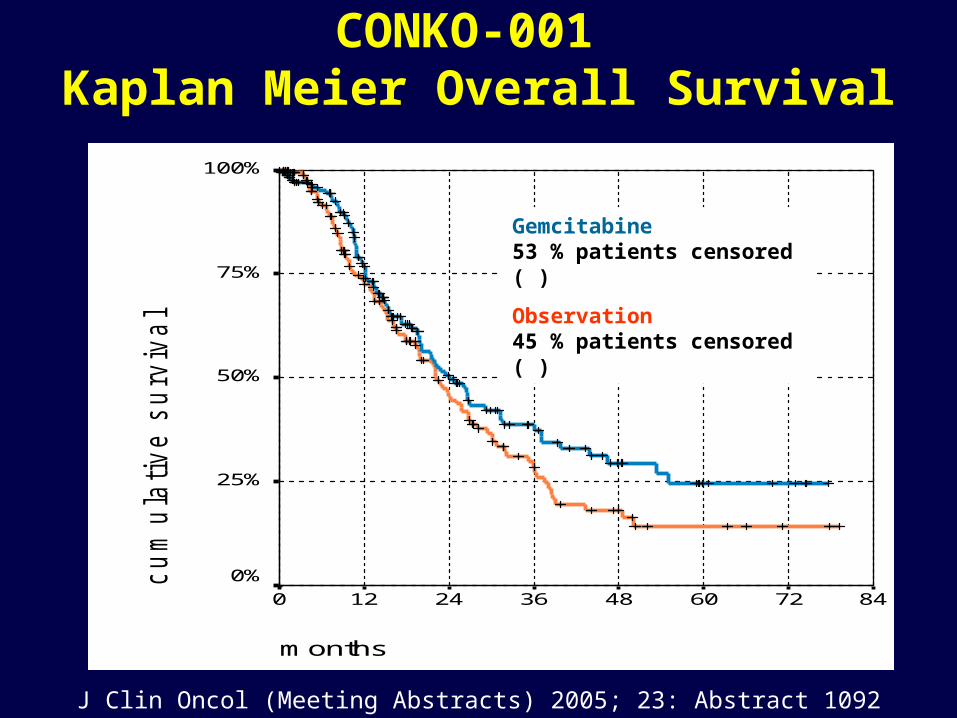
CONKO-001 Kaplan Meier Overall Survival
months
847260483624120
cu
mu
lative
su
rviv
al
100%
75%
50%
25%
0%
Gemcitabine53 % patients censored (+)
Observation45 % patients censored (+)
J Clin Oncol (Meeting Abstracts) 2005; 23: Abstract 1092
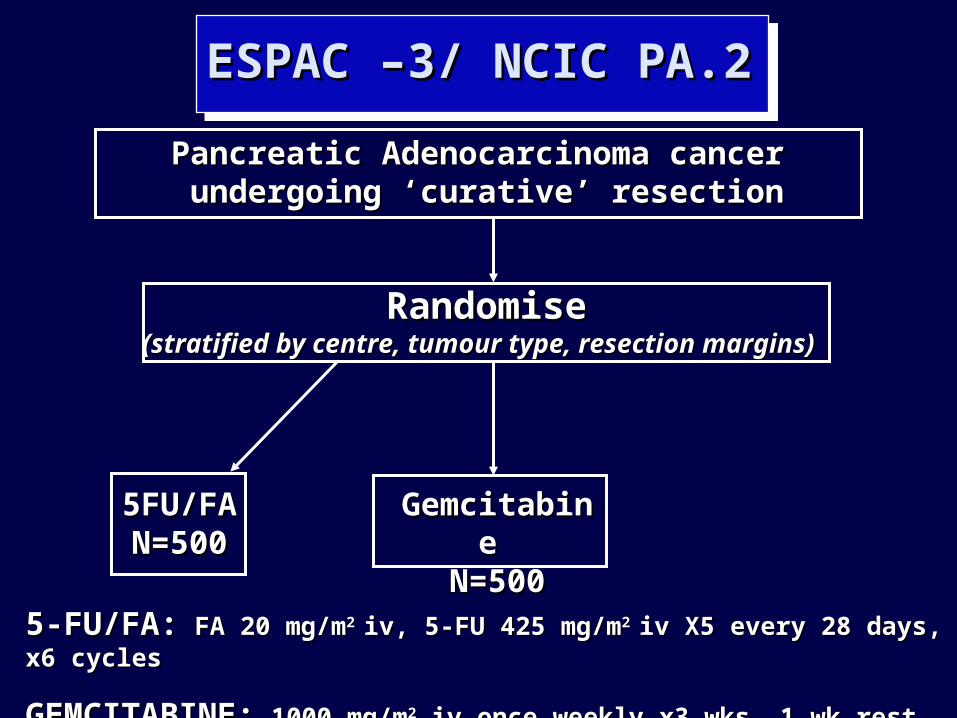
ESPAC –3/ NCIC PA.2ESPAC –3/ NCIC PA.2
Pancreatic Adenocarcinoma cancer Pancreatic Adenocarcinoma cancer undergoing ‘curative’ resectionundergoing ‘curative’ resection
RandomiseRandomise(stratified by centre, tumour type, resection margins)(stratified by centre, tumour type, resection margins)
Gemcitabine Gemcitabine N=500N=500
5FU/FA5FU/FAN=500N=500
5-FU/FA:5-FU/FA: FA 20 mg/mFA 20 mg/m2 2 iv, 5-FU 425 mg/miv, 5-FU 425 mg/m2 2 iv X5 every 28 days, x6 cyclesiv X5 every 28 days, x6 cycles
GEMCITABINE:GEMCITABINE: 1000 mg/m1000 mg/m22 iv once weekly x3 wks, 1 wk rest, x6 cycles iv once weekly x3 wks, 1 wk rest, x6 cycles
Adjuvant Therapy of Pancreatic Cancer
Adjuvant 5FU improves survival compared to observation
Preliminary results show improved PFS (and now survival) with adjuvant gemcitabine vs. observation
The optimal chemotherapy regimen (5FU/gemcitabine) not known
Role of XRT still controversial.
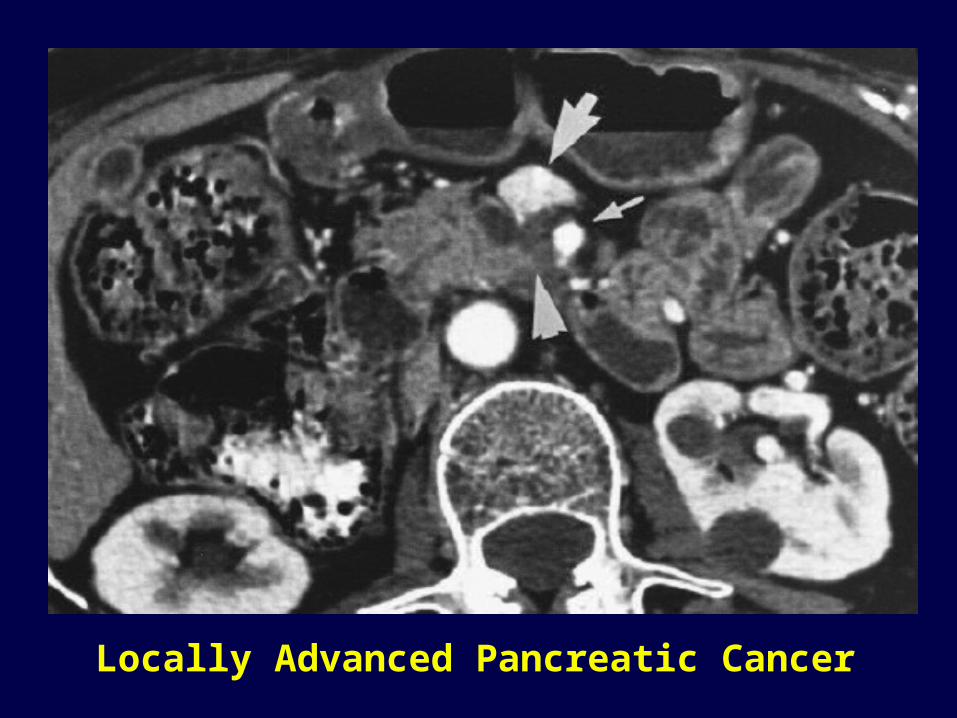
Locally Advanced Pancreatic Cancer
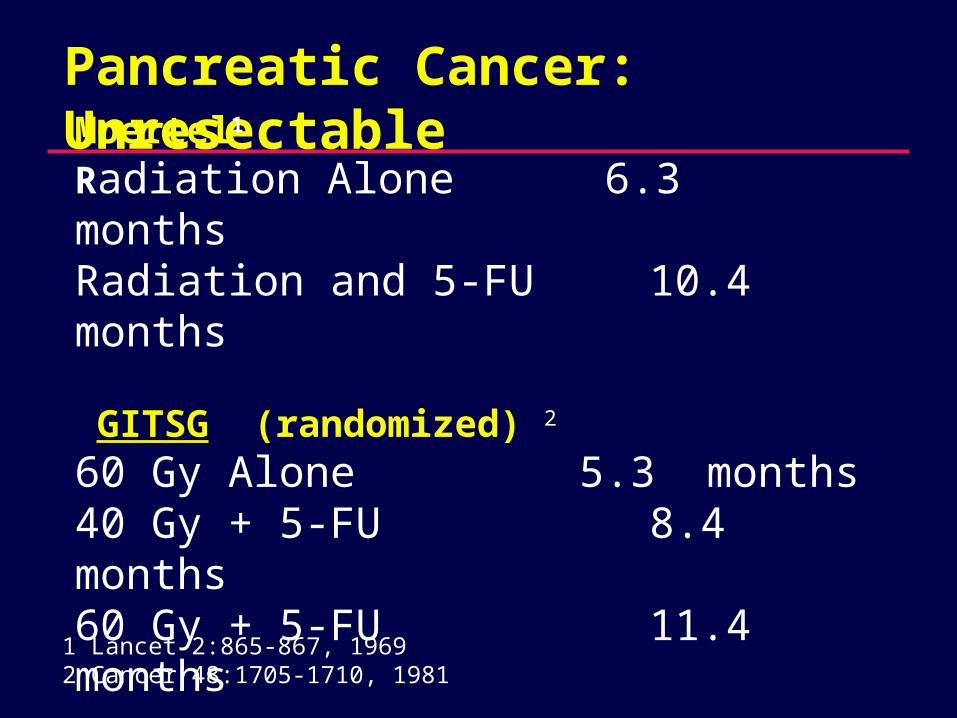
Pancreatic Cancer: Unresectable
Moertel1
Radiation Alone 6.3 monthsRadiation and 5-FU 10.4 months
GITSG (randomized) 2
60 Gy Alone 5.3 months40 Gy + 5-FU 8.4 months60 Gy + 5-FU 11.4 months
1 Lancet 2:865-867, 19692 Cancer 48:1705-1710, 1981
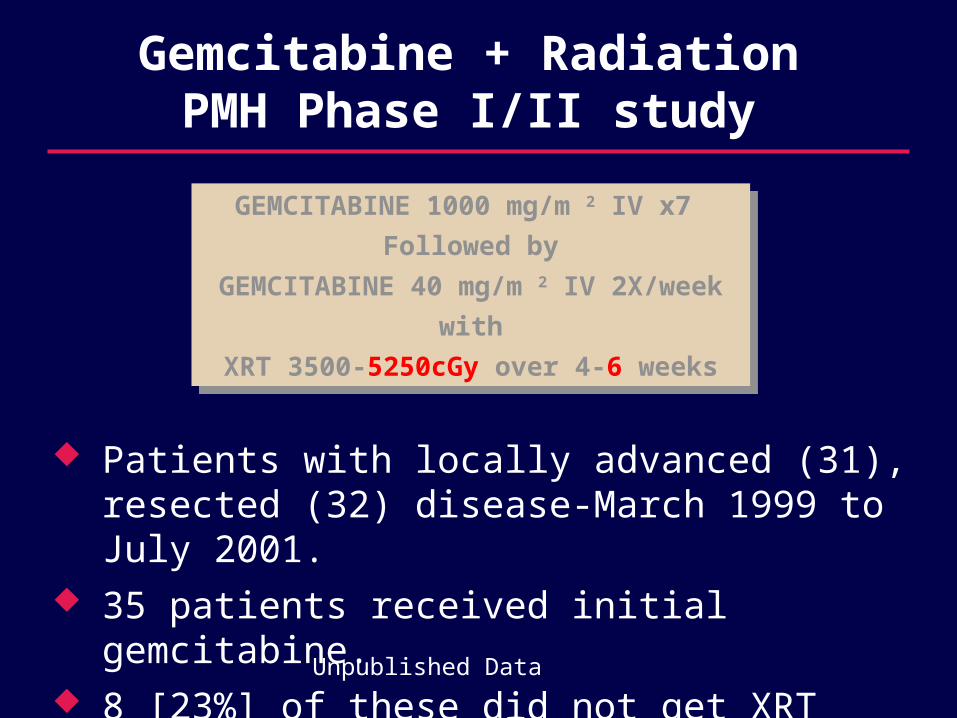
Gemcitabine + RadiationPMH Phase I/II study
Patients with locally advanced (31), resected (32) disease-March 1999 to July 2001.
35 patients received initial gemcitabine. 8 [23%] of these did not get XRT
GEMCITABINE 1000 mg/m 2 IV x7
Followed by
GEMCITABINE 40 mg/m 2 IV 2X/week
with
XRT 3500-5250cGy over 4-6 weeks
GEMCITABINE 1000 mg/m 2 IV x7
Followed by
GEMCITABINE 40 mg/m 2 IV 2X/week
with
XRT 3500-5250cGy over 4-6 weeks
Unpublished Data
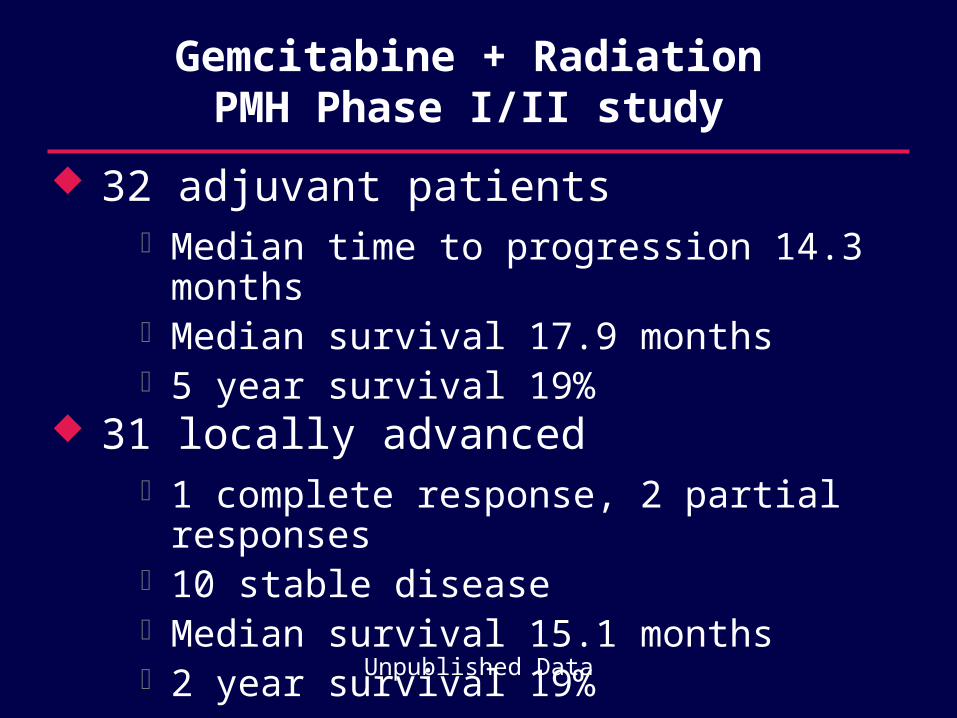
Gemcitabine + RadiationPMH Phase I/II study
32 adjuvant patients Median time to progression 14.3 months Median survival 17.9 months 5 year survival 19%
31 locally advanced 1 complete response, 2 partial responses 10 stable disease Median survival 15.1 months 2 year survival 19%
Unpublished Data
Locally Advanced Pancreatic Cancer
Chemoradiation in locally advanced pancreatic cancer improves:
– survival 1-2
– and pain in 35-65% of patients 3-6
Outcomes are still poor and better radiation sensitizers are needed
Most use up front chemo for 2 months and then chemo XRT
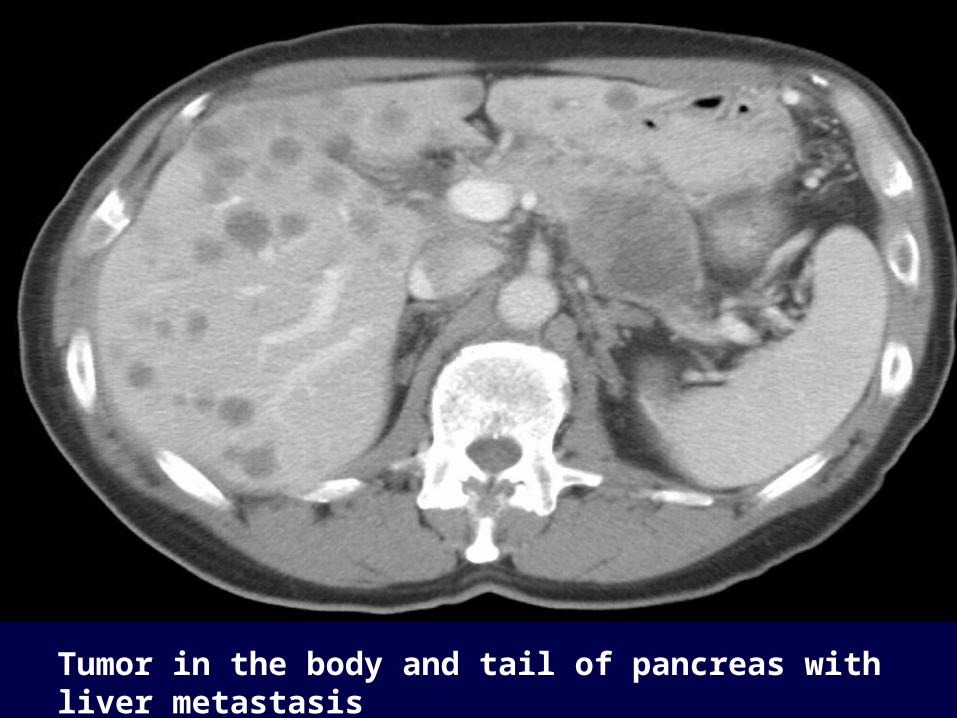
Tumor in the body and tail of pancreas with liver metastasis
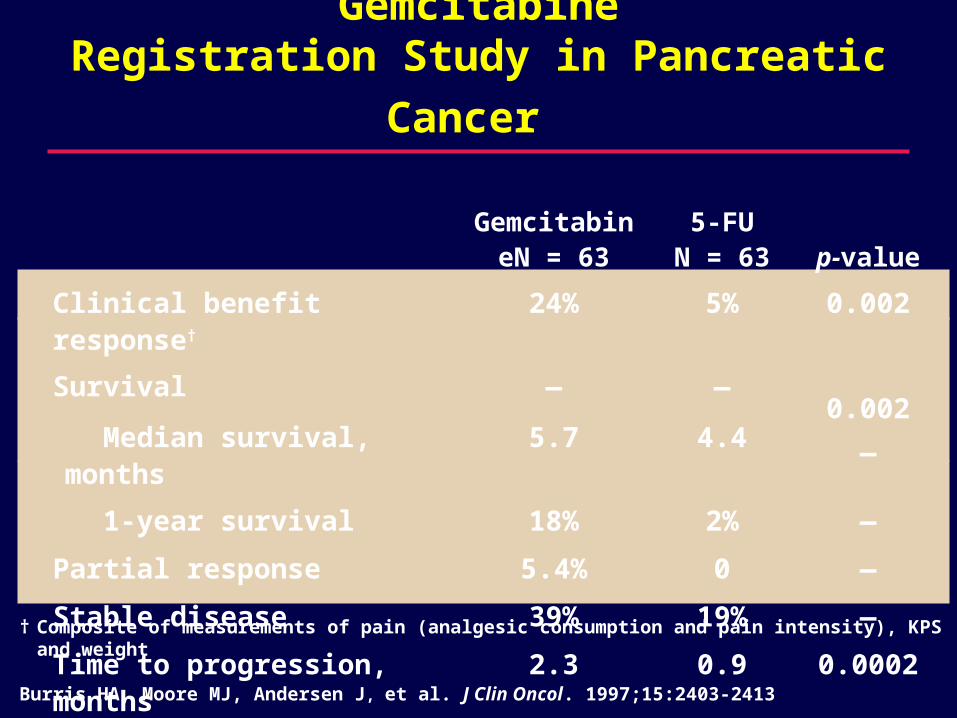
Gemcitabine
Registration Study in Pancreatic Cancer
† Composite of measurements of pain (analgesic consumption and pain intensity), KPS and weight
Burris HA, Moore MJ, Andersen J, et al. J Clin Oncol. 1997;15:2403-2413
GemcitabineN = 63
5-FUN = 63 p-value
Clinical benefit response† 24% 5% 0.002
Survival
Median survival, months
—
5.7
—
4.4
0.002
—
1-year survival 18% 2% —
Partial response 5.4% 0 —
Stable disease 39% 19% —
Time to progression, months 2.3 0.9 0.0002
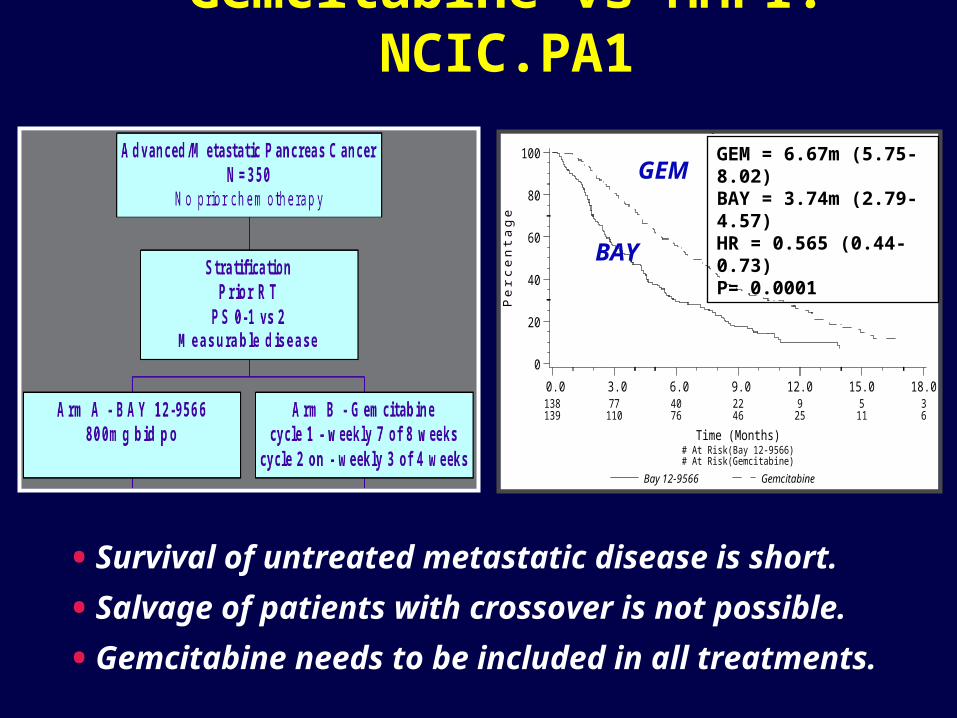
Gemcitabine vs MMPI: NCIC.PA1PA.1 - FINAL ANALYSIS
Overall Survival By Arm
Bay 12-9566 Gemcitabine
Pe
rce
nta
ge
0
20
40
60
80
100
Time (Months) # At Risk(Bay 12-9566) # At Risk(Gemcitabine)
0.0138139
3.077110
6.04076
9.02246
12.09
25
15.0511
18.036
GEM = 6.67m (5.75-8.02)BAY = 3.74m (2.79-4.57)HR = 0.565 (0.44-0.73)P= 0.0001BAY
GEM
• Survival of untreated metastatic disease is short.
• Salvage of patients with crossover is not possible.
• Gemcitabine needs to be included in all treatments.
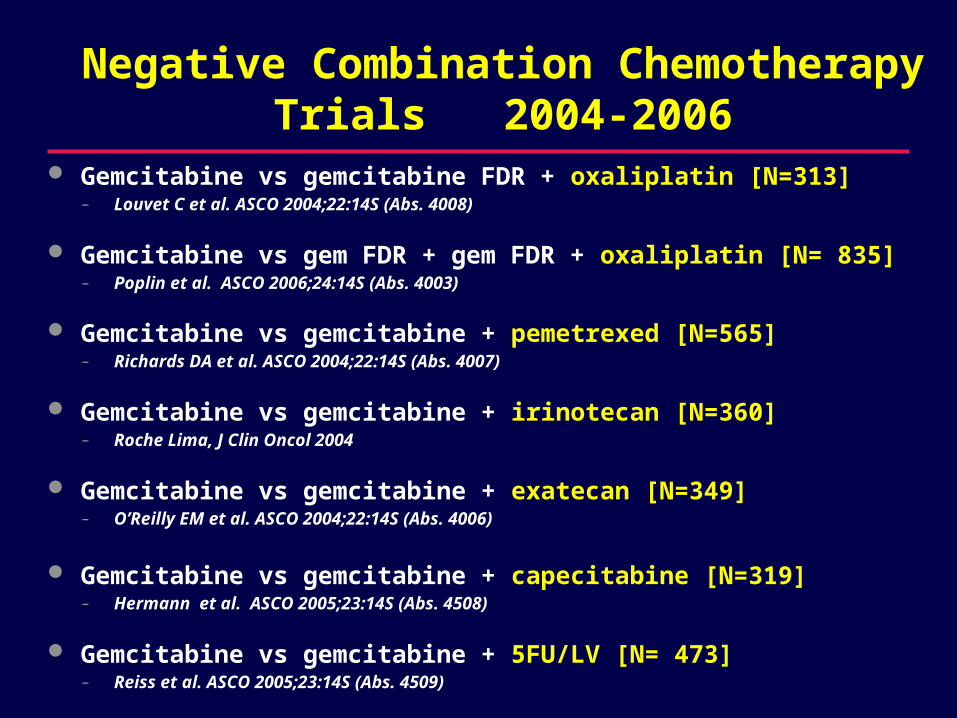
Negative Combination Chemotherapy Trials 2004-2006
Gemcitabine vs gemcitabine FDR + oxaliplatin [N=313]– Louvet C et al. ASCO 2004;22:14S (Abs. 4008)
Gemcitabine vs gem FDR + gem FDR + oxaliplatin [N= 835]– Poplin et al. ASCO 2006;24:14S (Abs. 4003)
Gemcitabine vs gemcitabine + pemetrexed [N=565]– Richards DA et al. ASCO 2004;22:14S (Abs. 4007)
Gemcitabine vs gemcitabine + irinotecan [N=360]– Roche Lima, J Clin Oncol 2004
Gemcitabine vs gemcitabine + exatecan [N=349]– O’Reilly EM et al. ASCO 2004;22:14S (Abs. 4006)
Gemcitabine vs gemcitabine + capecitabine [N=319]– Hermann et al. ASCO 2005;23:14S (Abs. 4508)
Gemcitabine vs gemcitabine + 5FU/LV [N= 473]– Reiss et al. ASCO 2005;23:14S (Abs. 4509)
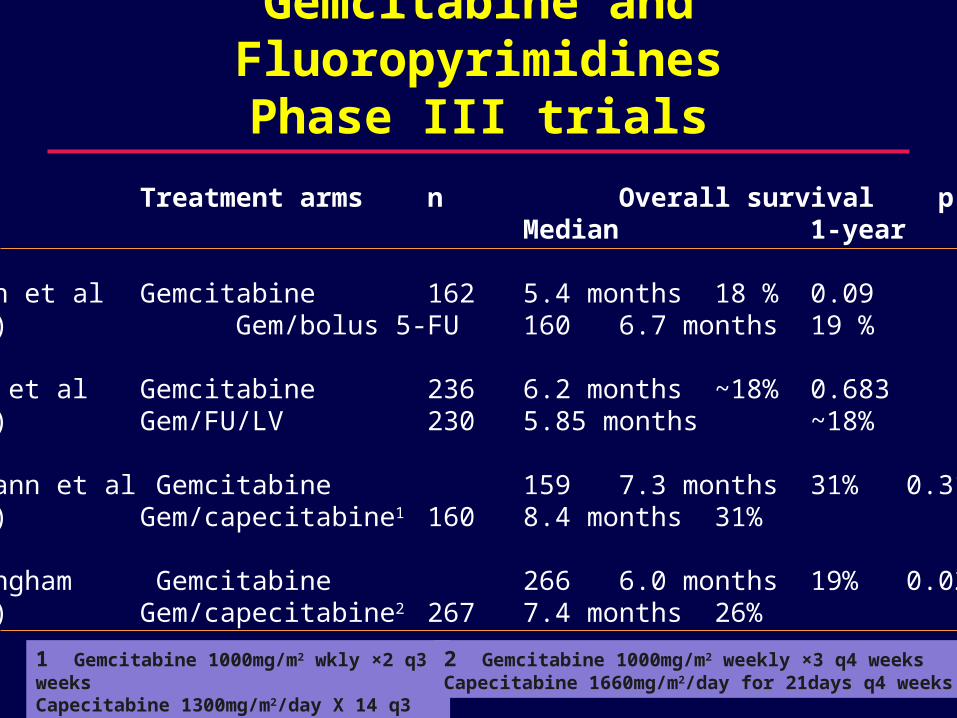
Gemcitabine and Fluoropyrimidines Phase III trials
Trial Treatment arms n Overall survival pMedian 1-year
Berlin et al Gemcitabine 162 5.4 months 18 % 0.09(2002) Gem/bolus 5-FU 160 6.7 months 19 %
Riess et al Gemcitabine 236 6.2 months ~18% 0.683(2005) Gem/FU/LV 230 5.85 months ~18%
Herrmann et al Gemcitabine 159 7.3 months 31% 0.314(2005) Gem/capecitabine1 160 8.4 months 31%
Cunningham Gemcitabine 266 6.0 months 19% 0.026(2005) Gem/capecitabine2 267 7.4 months 26%
1 Gemcitabine 1000mg/m2 wkly ×2 q3 weeksCapecitabine 1300mg/m2/day X 14 q3 weeks
2 Gemcitabine 1000mg/m2 weekly ×3 q4 weeksCapecitabine 1660mg/m2/day for 21days q4 weeks
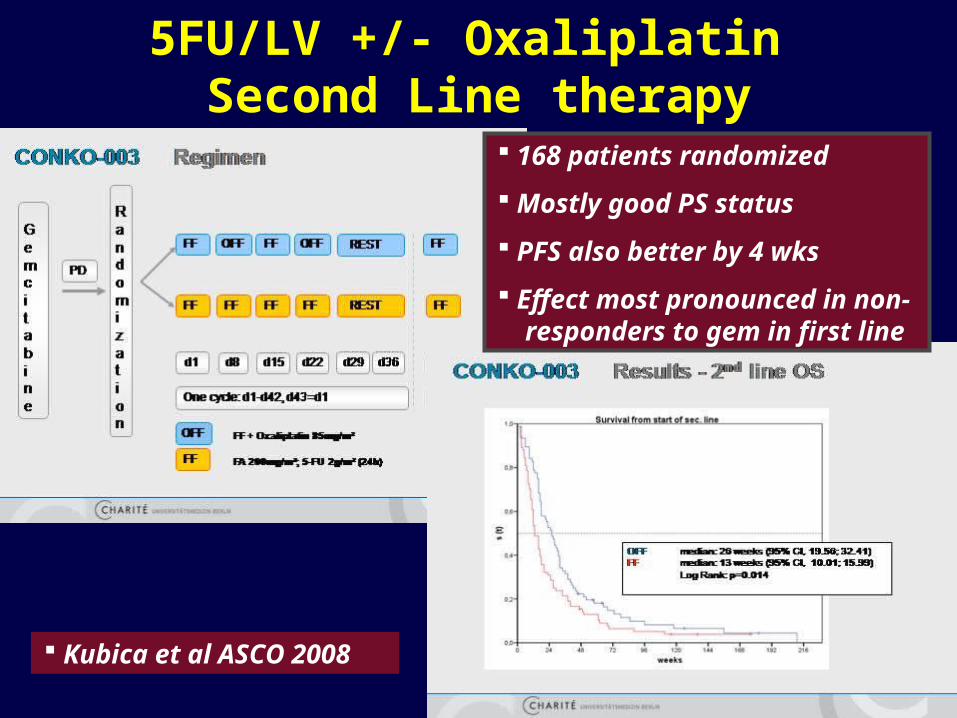
5FU/LV +/- Oxaliplatin Second Line therapy
168 patients randomized
Mostly good PS status
PFS also better by 4 wks
Effect most pronounced in non- responders to gem in first line
Kubica et al ASCO 2008
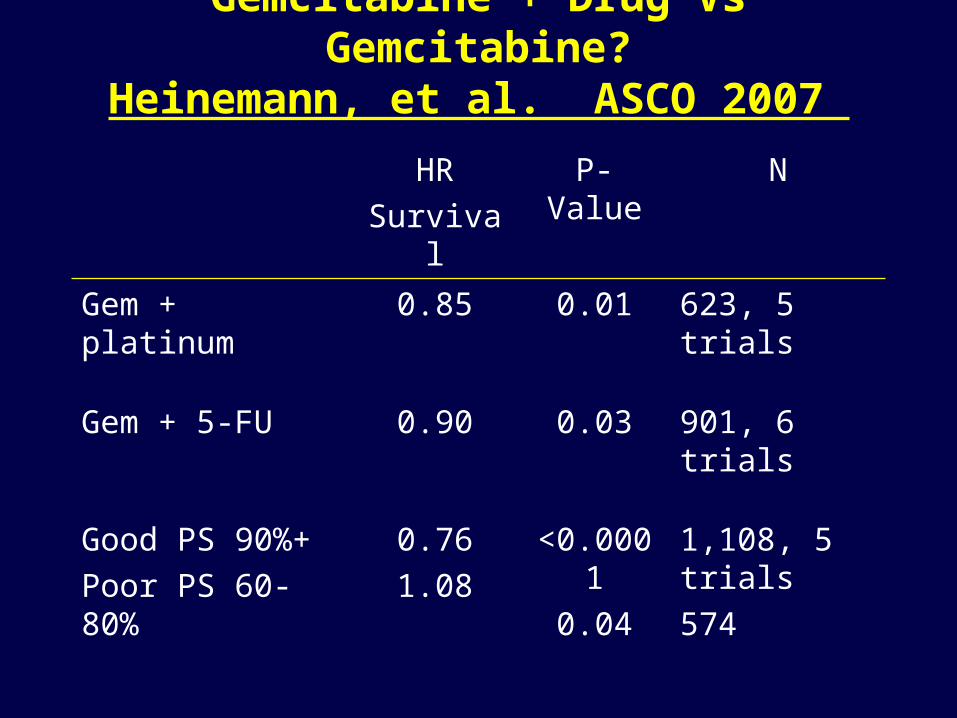
Gemcitabine + Drug Vs Gemcitabine?Heinemann, et al. ASCO 2007
HRSurvival
P-Value N
Gem + platinum
0.85 0.01 623, 5 trials
Gem + 5-FU 0.90 0.03 901, 6 trials
Good PS 90%+Poor PS 60- 80%
0.761.08
<0.0001
0.04
1,108, 5 trials574
Combination Chemotherapy in Pancreatic Cancer
One positive study in first line ?
– Gemcitabine + Capecitabine.
One positive study in second line.
– 5FU + oxaliplatin.
Many negative studies
Incremental benefit of combination chemotherapy.
– Restricted to patients with (very) good PS
Is it worth doing any more studies?
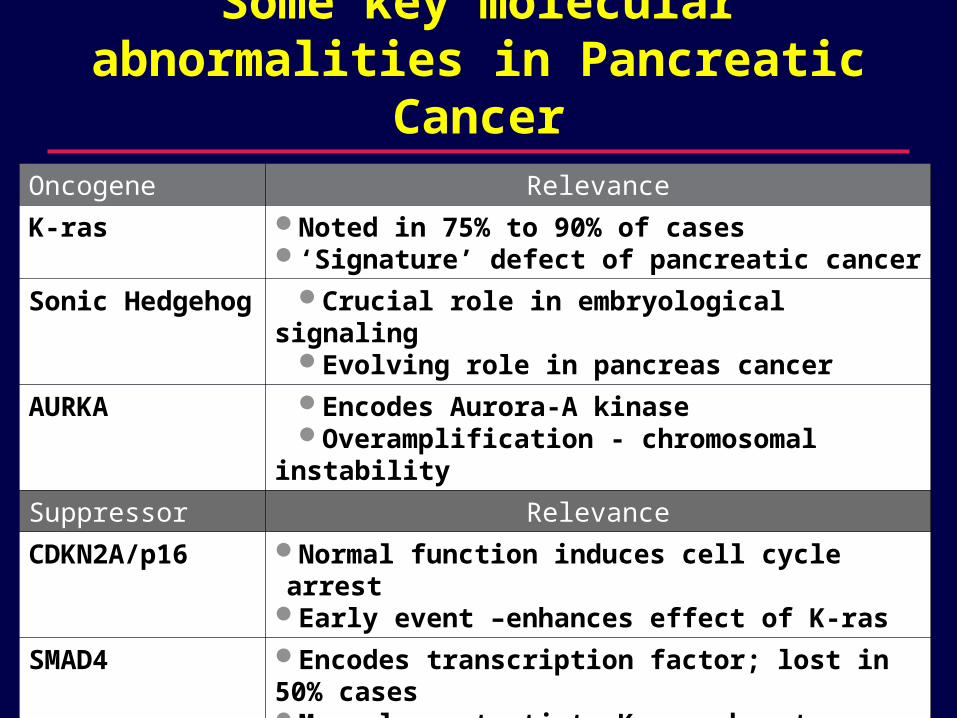
Oncogene Relevance
K-ras Noted in 75% to 90% of cases‘Signature’ defect of pancreatic cancer
Sonic Hedgehog
Crucial role in embryological signaling Evolving role in pancreas cancer
AURKA Encodes Aurora-A kinaseOveramplification - chromosomal
instability
Suppressor Relevance
CDKN2A/p16 Normal function induces cell cycle arrestEarly event –enhances effect of K-ras
SMAD4 Encodes transcription factor; lost in 50% casesMay also potentiate K-ras phenotype
p53 Role in cell cycle arrest and apoptosis Loss contributes to chromosomal instability
Some key molecular abnormalities in Pancreatic Cancer
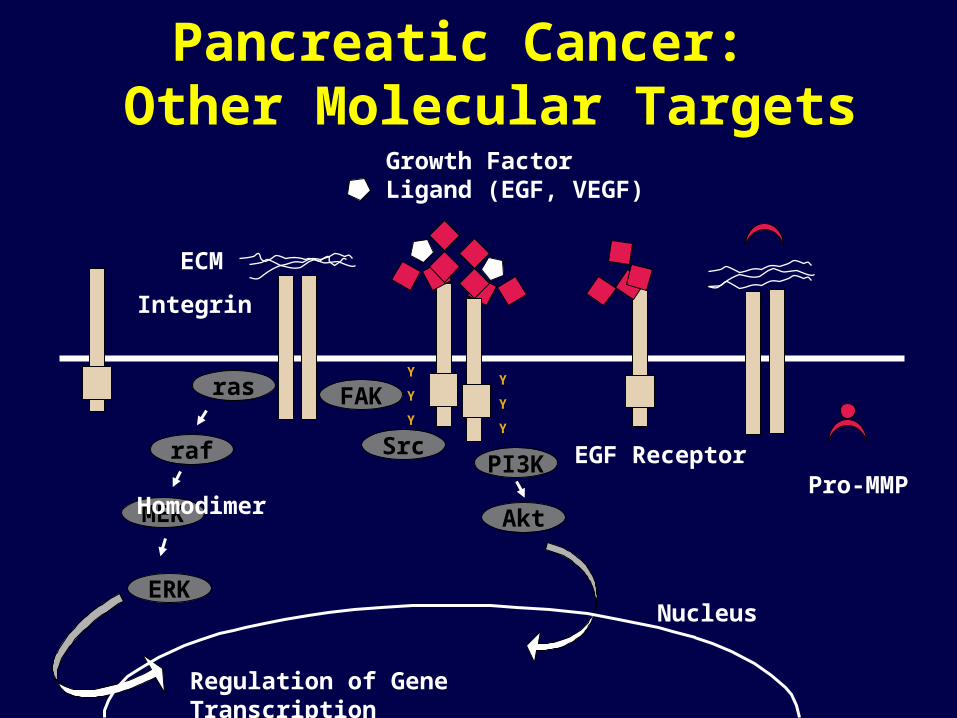
Y
Y
Y
Y
Y
Y
ras FAK
Srcraf
ERK
MEK
ECM
Integrin Homodimer
PI3K
Akt
Nucleus
Regulation of Gene Transcription
Pro-MMP
Growth Factor Ligand (EGF, VEGF)
EGF Receptor
Pancreatic Cancer: Other Molecular Targets
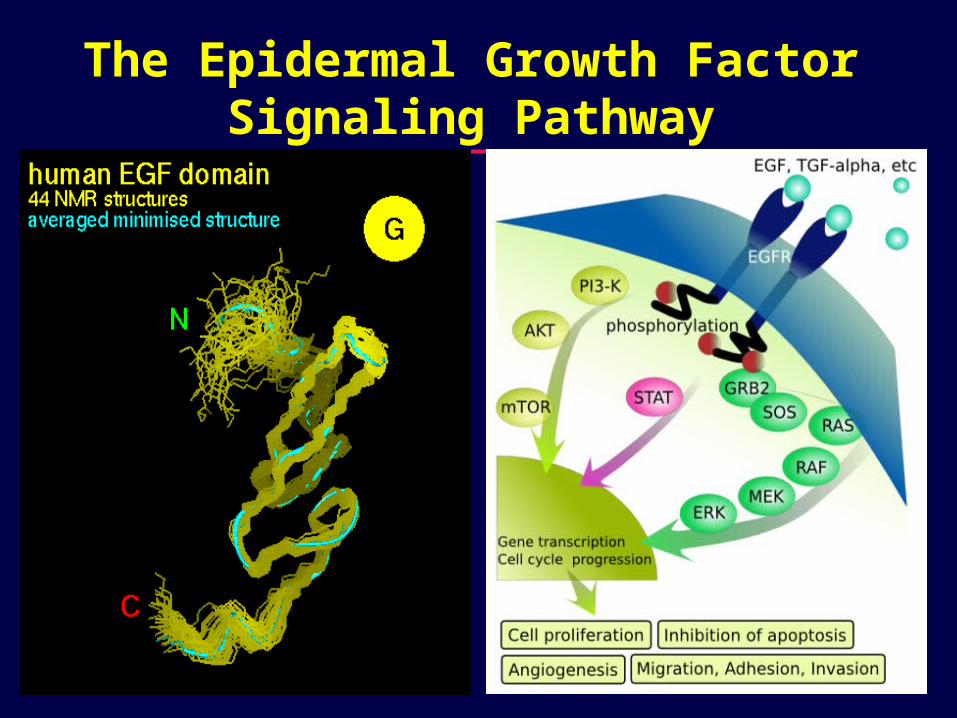
The Epidermal Growth Factor Signaling Pathway
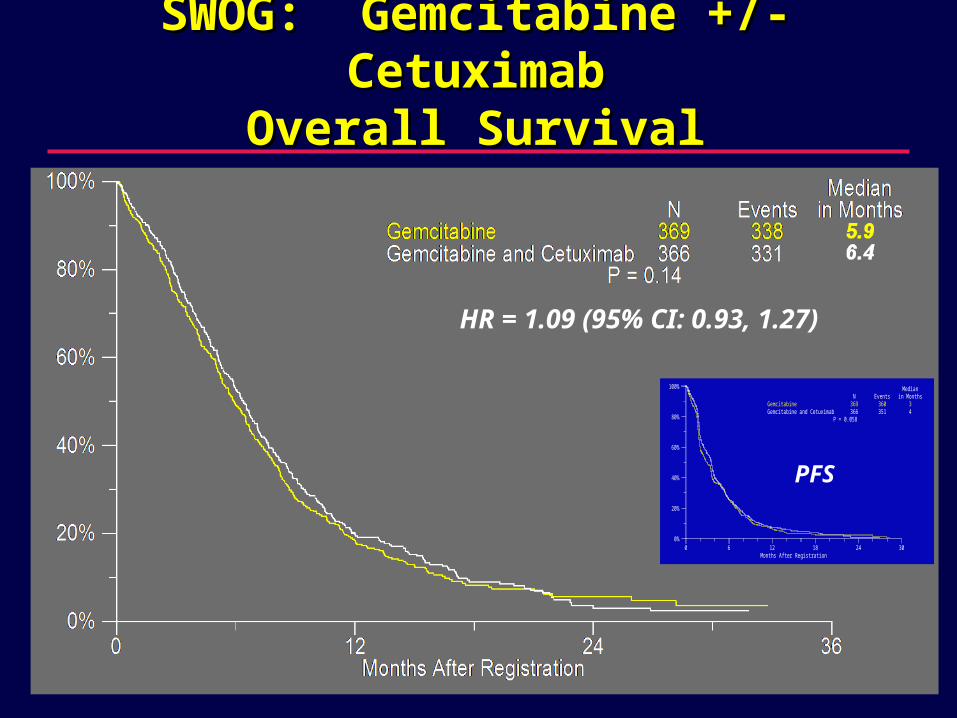
SWOG: Gemcitabine +/- CetuximabSWOG: Gemcitabine +/- CetuximabOverall SurvivalOverall Survival
HR = 1.09 (95% CI: 0.93, 1.27)
Progression-Free Survival by Treatment Arm
0%
20%
40%
60%
80%
100%
0 6 12 18 24 30Months After Registration
GemcitabineGemcitabine and Cetuximab
N369366
Events360351
Medianin Months
34
P = 0.058
PFS
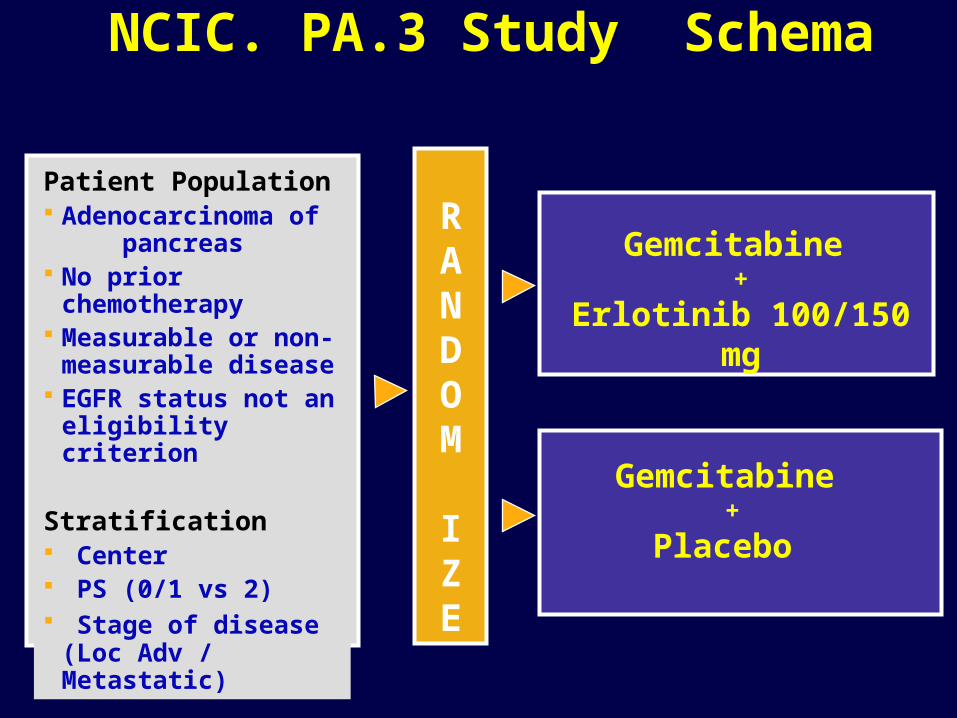
Patient Population Adenocarcinoma of
pancreas No prior
chemotherapy Measurable or non-
measurable disease
EGFR status not an eligibility criterion
Stratification Center PS (0/1 vs 2) Stage of disease
(Loc Adv / Metastatic)
RANDOM I ZE
Gemcitabine +
Erlotinib 100/150 mg
Gemcitabine +
Placebo
NCIC. PA.3 Study Schema
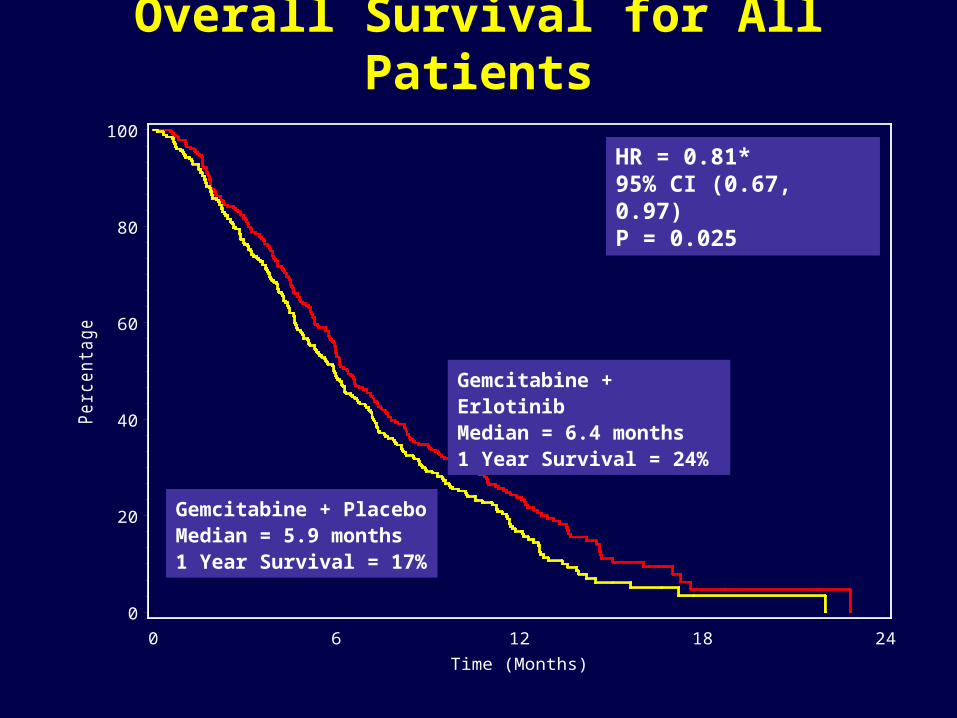
Overall Survival for All PatientsP
erc
enta
ge
0
20
40
60
80
100
Time (Months)0 6 12 18 24
HR = 0.81*95% CI (0.67, 0.97)P = 0.025
Gemcitabine + ErlotinibMedian = 6.4 months1 Year Survival = 24%
Gemcitabine + PlaceboMedian = 5.9 months1 Year Survival = 17%
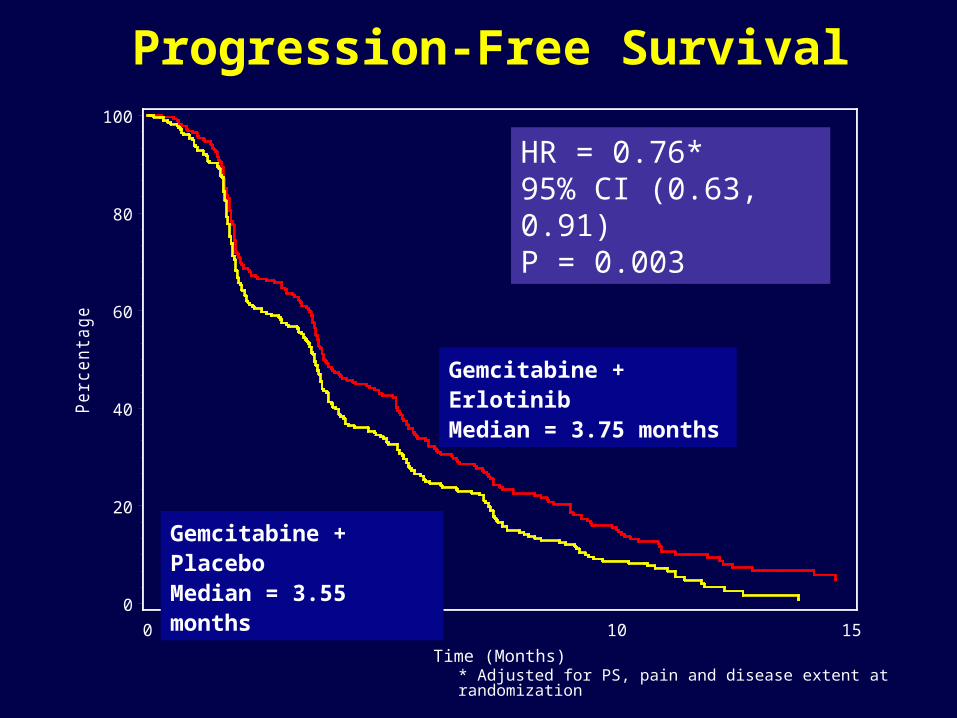
Progression-Free Survival
* Adjusted for PS, pain and disease extent at randomization
Pe
rcen
tage
0
20
40
60
80
100
Time (Months)0 5 10 15
HR = 0.76*95% CI (0.63, 0.91)P = 0.003
Gemcitabine + ErlotinibMedian = 3.75 months
Gemcitabine + PlaceboMedian = 3.55 months
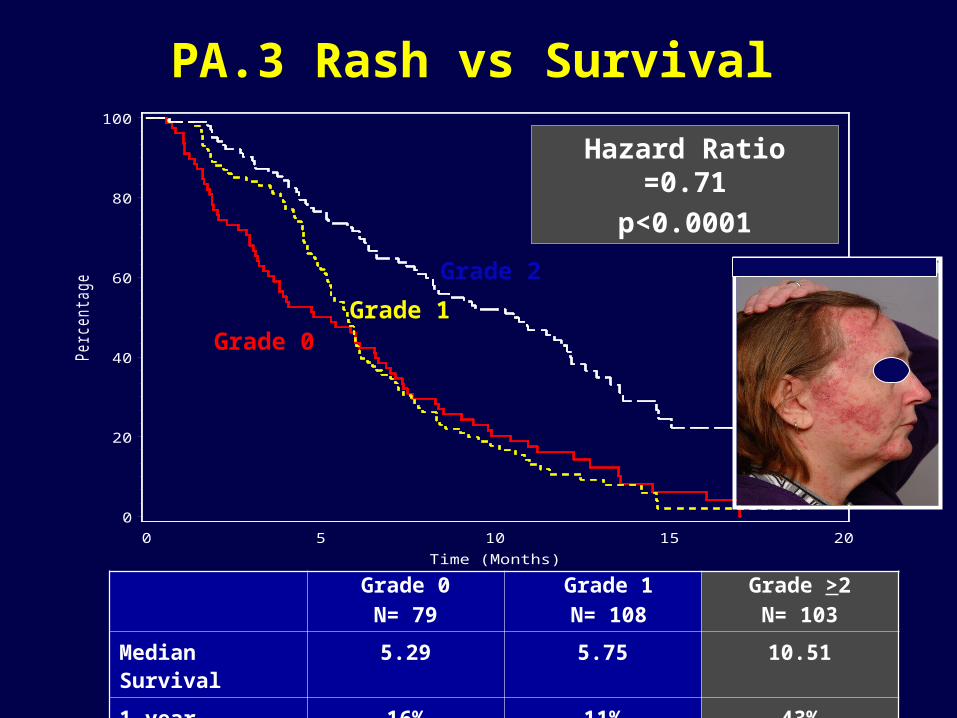
PA.3 Rash vs SurvivalPerc
enta
ge
0
20
40
60
80
100
Time (Months)0 5 10 15 20
Grade 2
Grade 0
Hazard Ratio =0.71
p<0.0001
Grade 1
Grade 0
N= 79
Grade 1
N= 108
Grade >2
N= 103
Median Survival 5.29 5.75 10.51
1 year Survival 16% 11% 43%
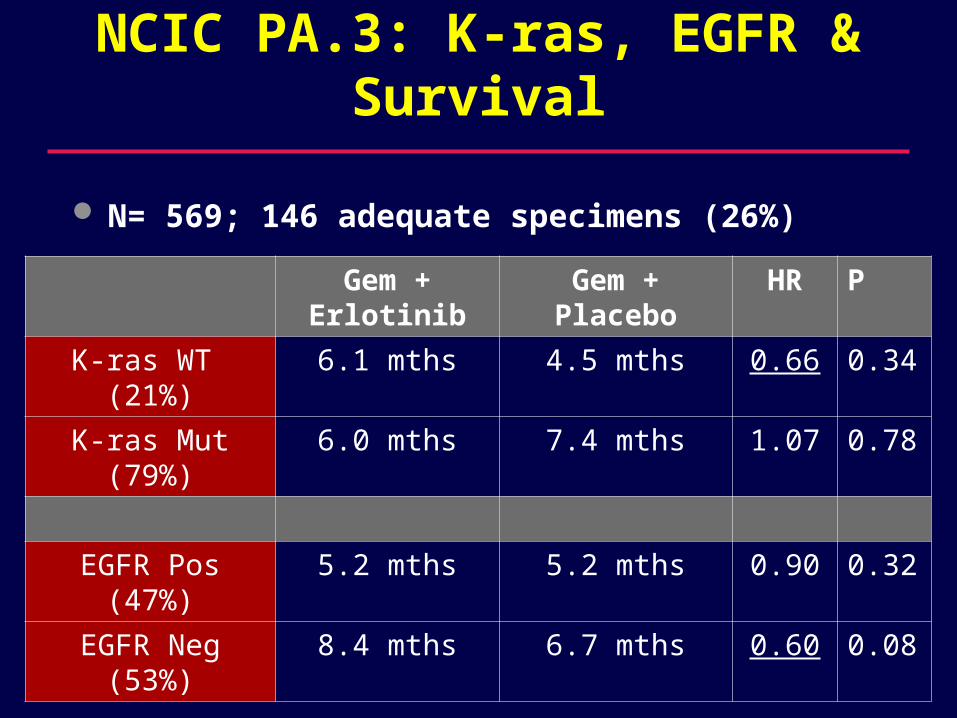
NCIC PA.3: K-ras, EGFR & Survival
N= 569; 146 adequate specimens (26%)
Gem + Erlotinib
Gem + Placebo
HR P
K-ras WT (21%)
6.1 mths 4.5 mths 0.66 0.34
K-ras Mut (79%)
6.0 mths 7.4 mths 1.07 0.78
EGFR Pos (47%)
5.2 mths 5.2 mths 0.90 0.32
EGFR Neg (53%)
8.4 mths 6.7 mths 0.60 0.08
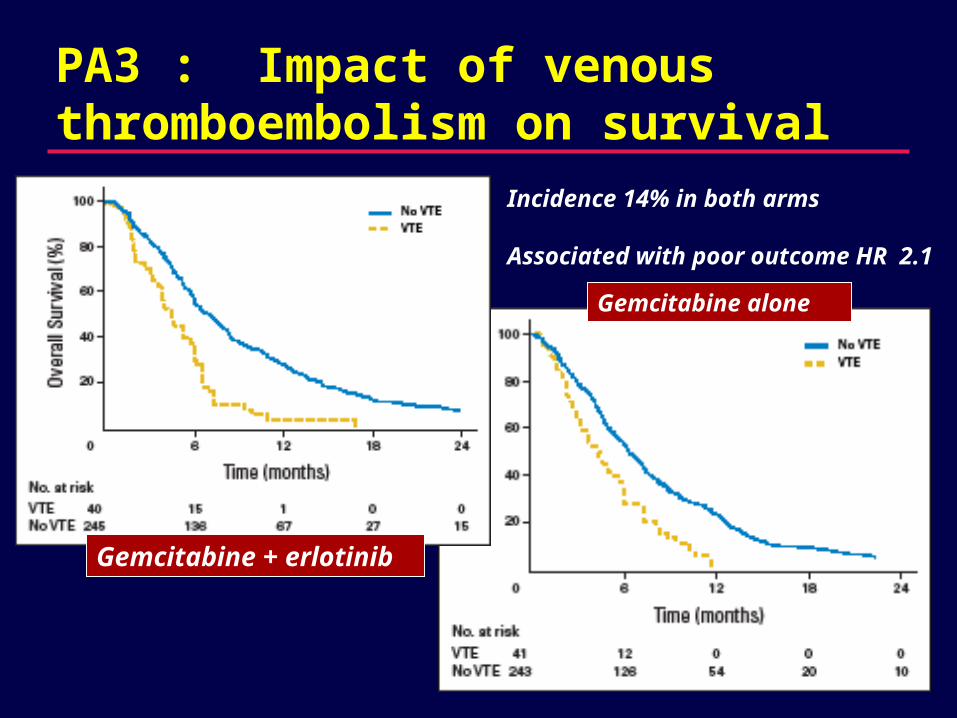
PA3 : Impact of venous thromboembolism on survival
Gemcitabine alone
Gemcitabine + erlotinib
Incidence 14% in both arms
Associated with poor outcome HR 2.1
VEGF and Angiogenesis
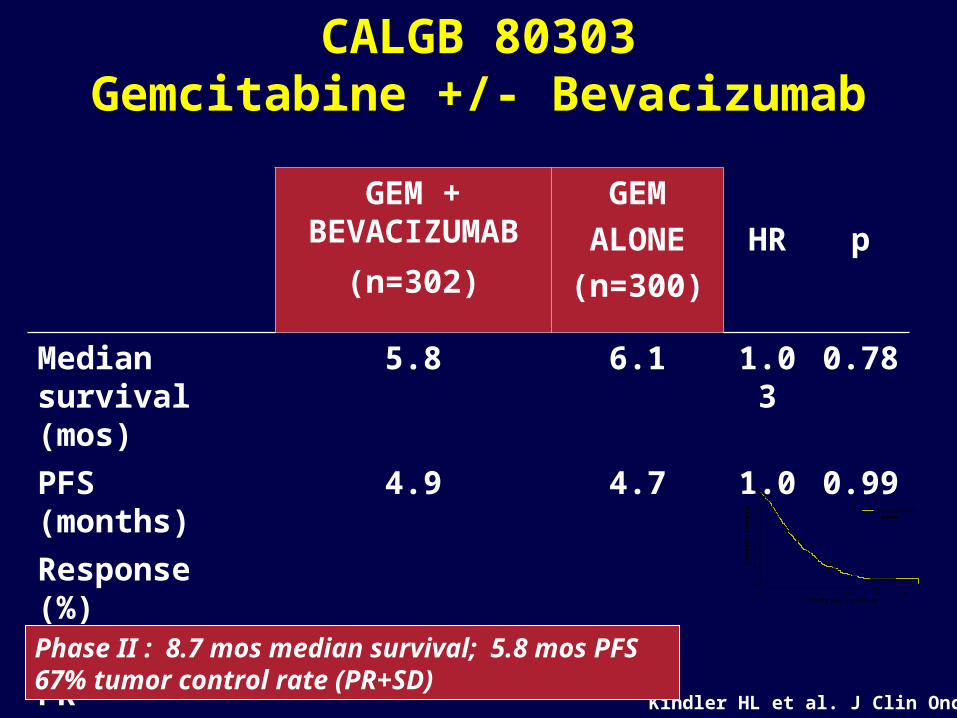
CALGB 80303Gemcitabine +/- Bevacizumab
GEM + BEVACIZUMAB
(n=302)
GEM
ALONE
(n=300)
HR p
Median survival (mos)
5.8 6.1 1.03 0.78
PFS (months) 4.9 4.7 1.0 0.99
Response (%)
CR + PR 11 10
SD 36 31
Kindler HL et al. J Clin Oncol
Phase II : 8.7 mos median survival; 5.8 mos PFS 67% tumor control rate (PR+SD)
0 5 10 15 20 25
Months from Study Entry
0.0
0.2
0.4
0.6
0.8
1.0
Pro
po
rtio
n S
urv
ivin
g BevacizumabPlacebo
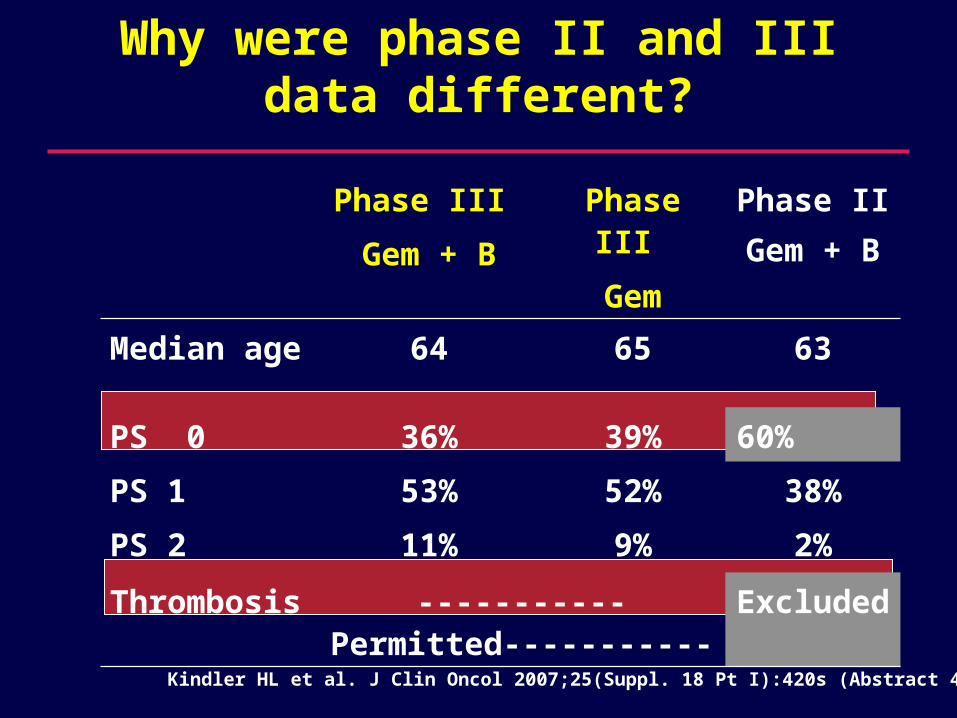
Why were phase II and III data different?
Phase III
Gem + B
Phase III
Gem
Phase II
Gem + B
Median age 64 65 63
PS 0 36% 39% 60%
PS 1
PS 2
53%
11%
52%
9%
38%
2%
Thrombosis -----------Permitted----------- Excluded
Kindler HL et al. J Clin Oncol 2007;25(Suppl. 18 Pt I):420s (Abstract 4508)
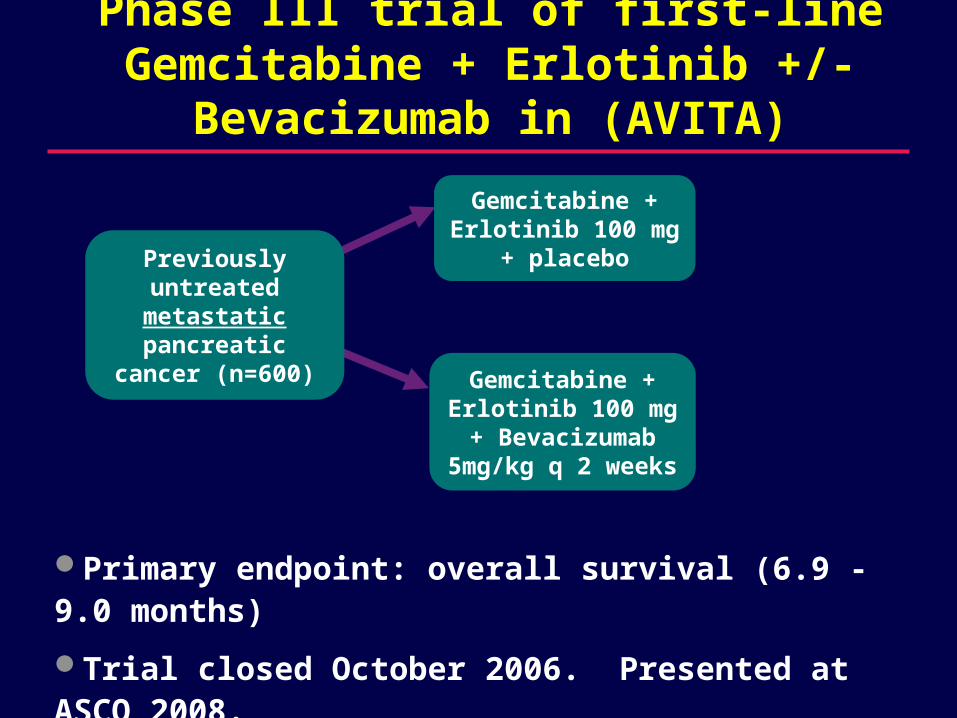
Primary endpoint: overall survival (6.9 - 9.0 months)
Trial closed October 2006. Presented at ASCO 2008.
Previously untreated metastatic pancreatic
cancer (n=600)
Gemcitabine + Erlotinib 100 mg
+ placebo
Gemcitabine + Erlotinib 100 mg + Bevacizumab
5mg/kg q 2 weeks
Phase III trial of first-line Gemcitabine + Erlotinib +/- Bevacizumab in (AVITA)
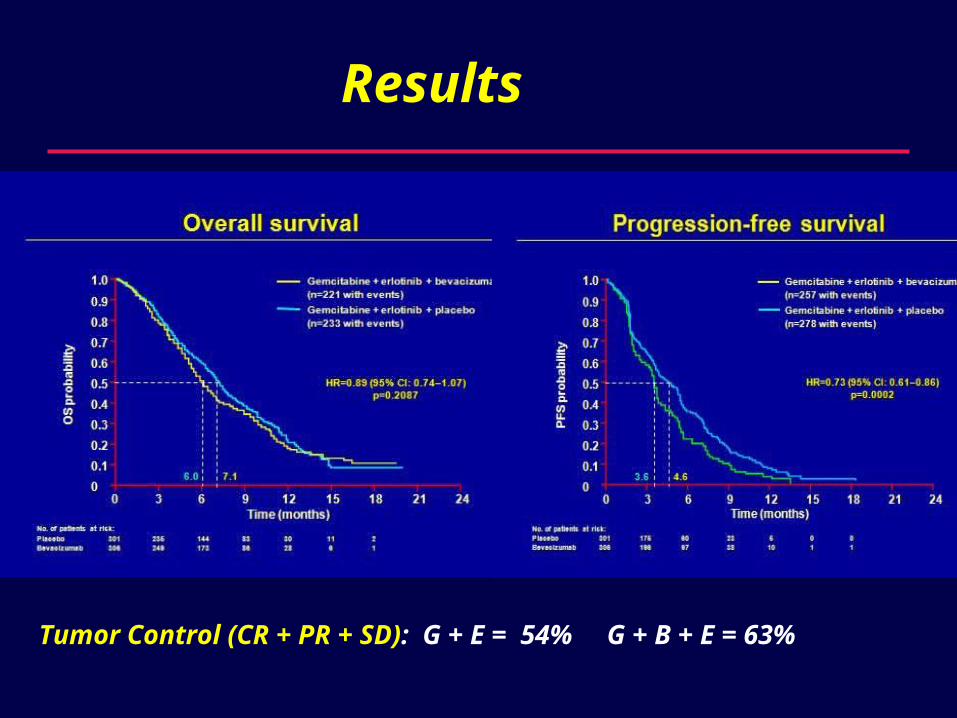
Results
Tumor Control (CR + PR + SD): G + E = 54% G + B + E = 63%
Treating the individual patient
One size (gemcitabine) fits all?
Probably not…
(with an admitted lack of level 1 evidence)
Good performance status - KPS 90 +
– Consider combination chemotherapy – I would use gemcitabine + cisplatin.
K-ras wild type
– Gemcitabine + erlotinib.
Treating the individual patient
Locally advanced disease should be approached differently than metastatic disease.
Prophylactic anticoagulation
– No phase III studies
– VTE is common - associated with bad outcome
– I do it (low molecular wt heparin) routinely.
The way forward inClinical Research
Test novel targets and combinations in the phase II setting.
No phase III studies without a clear signal from phase II.
Separate studies for locally advanced and metastatic disease.
Translational research is critical!!
– Routine tissue collection in trials
– We need to understand a lot more about biology