Embed Size (px)
Citation preview

BEHAVIOR THERAPY 21, 273-280, 1990
Panic Disorder in Association With Relaxation Induced Anxiety: An Attentional Training Approach to Treatment
ADRIAN WELLS
Center for Cognitive Therapy Umverslty of Pennsylvama
A case of relaxation induced anxiety in a patient with Panic Disorder is reported. The study reports the use of an attenttonal training procedure which was effective in eliminating panic and facilitated tension reduction without producing anxiety. A two treatment (ABCB) design revealed that a procedure evoking external attentlonal focus eliminated panic attacks, whereas autogenlc training Increased the frequency of panic attacks and the intensity of anxiety. The possible roles of self-focus in mediating panic and the effects of relaxation are briefly discussed.
Relaxation techniques have been widely used in the treatment of tension and anxiety related disorders. However recent evidence suggests that these procedures may elicit or exacerbate anxiety in certain individuals (e.g., Heide & Borkovec, 1983, 1984, Braith, McCullogh, & Bush, 1988). Braith et al. (1988) found a 17°/0 incidence rate of relaxation induced anxiety (RIA) during progres- sive relaxation among a group of chronically anxious college students. In a similar sample of subjects, Heide and Borkovec (1983) found a 30.8070 inci- dence rate of RIA in subjects under progressive relaxation and an incidence of 53.8070 in subjects under mantra meditation. According to Heide and Bor- kovec (1984) clients with generalized anxiety appear to be especially prone to RIA. However, the prevalence of RIA in clinical patients is currently unknown.
Five mechanisms have been proposed as underlying the RIA phenomenon (Heide & Borkovec, 1984). Essentially these are: fear of the sensations and cognitions released through relaxation, fear of losing control, fear of anxiety symptoms to which attention is drawn during relaxation, heightened aware- ness of dissatisfaction with self, and experiencing negative cognitive activity unrelated to relaxation. Since most relaxation procedures require an increase in individuals' self-focused attention, this may increase awareness of anxiety and heighten awareness of self-discrepancies. Wells (1987) demonstrated that patients with generalized anxiety and panic disorder report elevated levels of
I would like to thank Dr. Susan G. O'Leary for her helpful comments on an earlier draft of this manuscript. Requests for reprints should be sent to: Dr. Adrian Wells, University of Penn- sylvania, Center for Cognitive Therapy, Room 602, 133 South 36th Street, Philadelphia, PA 19104-3246.
273 0005-7894/90/0273-028051 00/0 Copyright 1990 by Association for Advancement of Behavior Therapy
All rights of reproduction in any form reserved.

274 WELLS
self-attention. He proposed that self-focused processing may elicit or exacer- bate anxiety. Preoccupation with somatic symptoms and catastrophic interpre- tation of such symptoms is considered to be a central feature in panic dis- orders (e.g., Clark, 1986; Beck, 1988). It is possible, therefore, that heightened self-directed processing underlies both the development of panic disorder and the occurrence of RIA. Thus, a technique designed to re-orient patients' at- tention and produce a shift away from self-focus could lead to the amehora- tion of panic and concomitant reductions in the levels of anxiety and tension.
METHOD Subject
The patient was a 40-year-old female secretary who presented with pamc attacks, neck tension, and an inability to relax. The patient sausfied DSM l l l -R criteria (American Psychiatric Association, 1987) for panic disorder without agoraphobic avoidance. The panic attacks were associated with auto- matic thoughts concerning loss of control (fainting/collapsing) and death. She reported that the problem had been present for 12 months and that her first panic attack occurred approximately 6 months after her father's death from cancer. A few months after her first attack she discovered that a close friend had undergone surgery for cancer. No other stresses were evident.
At assessment, she stated that she felt anxious about relaxing. Her response to relaxation was tested by presenting progressive relaxation (Jacobsen, 1938) which resulted in an exacerbation of anxiety and discontinuation of the exercise.
Measures In this case study, the frequency of panic attacks were recorded in a daily
diary. Mulhall's (1978) personal questionnaire (PQRST) was used to assess self-report levels of neck tension. The patient was also required to rate levels of anxiety on a ten-point scale ranging from "no anxiety" to "extreme anxiety" following each treatment session. The state subscale of the State-Trait Anxiety Inventory (Spielberger, Gorsuch, & Lushene, 1970) was administered at the end of each experimental block.
Design An ABCB design was used to evaluate the relative effectiveness of atten-
tional training and relaxation training. The relaxation condition consisted of standard autogenic exercises (Schultz & Luthe, 1969). It was predicted that external attention focus would reduce panic frequency and lead to a reduction in anxiety and tension symptoms. However, heightened self-focus associated with autogenic exercises would increase panic and elevate anxiety levels and self-report tension.
Autogenic training was chosen in preference to a tension-release procedure such as progressive relaxation because the patient had been sensitized to the negative effects of progressive relaxation in a provocation test at assessment.

PAnic 275
The treatment rationale consisted of informing the patient that an alternative relaxation program consisting of two sets of exercises would be used to facili- tate symptom reduction.
PROCEDURE Baseline
The patient was instructed to complete the panic diary on a daily basis. Panic attacks were defined as occurring suddenly and reaching their peak within 10 min and consisting of at least four symptoms, Only attacks meeting these criteria were to be recorded, and the nature of recorded attacks were reviewed each session. At each session the PQRST was administered. Sessions were held weekly. The patient was unable to attend session two thus PQRST data are missing for the session; however; she did complete the panic diary for this period.
Treatment 1
The first stage of treatment involved training the patient in external atten- tional focusing. Treatment commenced in session five. The therapist used scripted instructions to guide the patient through an exercise involving external attentional monitoring and attention switching in an auditory mode. The tech- nique was designed so that attentional demands increased as the exercise progressed. The patient was instructed to focus on specific sounds in the con- sulting room, for example, the sound of the therapists voice as instructions were given and then the sound of a clock. The patient's attention was then guided to different sounds outside of the room but still within the building. This was followed by instructions to focus on sounds which were outside the building and in the near distance and then sounds in the far distance. With each new focus the therapist gave the following verbal instructions: "Focus all of your attention on the sound of . . . . No other sound matters. Absorb only that sound. I f your attention strays re-focus on that one sound. Do not allow yourself to be distracted. Focus only on that sound". Following this selec- tive attention phase, the procedure moved onto attentional switching in which the patient was instructed to focus on one specified sound and then another specified sound in rapid succession. This was introduced as follows: "Now ! would like you to switch your attention f rom one sound to another as quickly as you can. Focus on the sound of . . . . Focus only on that sound. No other sounds mater. Now focus on the sound of . . . . Focus only on that sound; no other sounds matter". The exercise ended with a divided attention instruc- tion: "Now try to focus on as many different sounds as you can at the same time. Expand your attention and absorb all of the sounds. Focus on all of the sounds. Name the sounds that you can hear simultaneously". The exercise was practiced for 15 min per session.
For all treatment periods diary data were collected at the beginning of each session and PQRST and anxiety data were obtained at the end of each ses- sion. The patient was instructed to practice the attentional training procedure at home for a period of 15 min per day.

276 WELLS
Treatment 2
After 35 days of attentional training the second treatment condition was introduced. In this condition two types of exercise from the range of standard autogenic exercises were practiced (heaviness and warmth), (Schultz & Luthe, 1969). The therapist instructed the patient to focus on her body, specifically sensations in each arm and then sensations in each leg. The therapist then suggested that the patient's right arm was heavy and then instructed the pa- tient to repeat four times the suggestion: "My right arm is heavy." The ther- apist instructed the patient to visualize lead weights attached to each arm m order to increase sensations of heaviness. This procedure was repeated with the left arm and then each leg in turn, each time using the appropriate sugges- tion. Following this phase, the theme of warmth was used in the same manner in which the heaviness theme had been used. The exercise was implemented for a period of 15 rain per session, and the patient was instructed to practice the exercises at home for a period of 15 min per day. This phase resulted m an exacerbation of symptoms and was discontinued on the patient's request after session 12 (following 21 days of practice).
There was a return to treatment 1 in session 13 and this phase lasted for 42 days and was terminated at the end of week 18. Session 19 was used to collect diary data from the previous week. Treatment was not administered at this data end point.
Follow-up assessments were conducted at intervals of 3 months and 12 months after the final session. At each follow-up session the patient was inter- viewed in order to determine the number of panic attacks experienced during the preceding week .and month and since termination.
RESULTS AND DISCUSSION Frequencies of panic attacks reported during baseline, treatment and follow-
up phases are presented in Figure 1, which shows a moderate frequency of panic attacks during baseline and zero frequency rapidly following the introduc- tion of attentional training. The absence of panic attacks was maintained across the five sessions of attention training.
During autogenic training, panic attacks recurred and rapidly increased in frequency above baseline levels. Re-introduction of attention training initially reduced panic frequency below baseline levels and then to zero frequency which was maintained across four sessions.
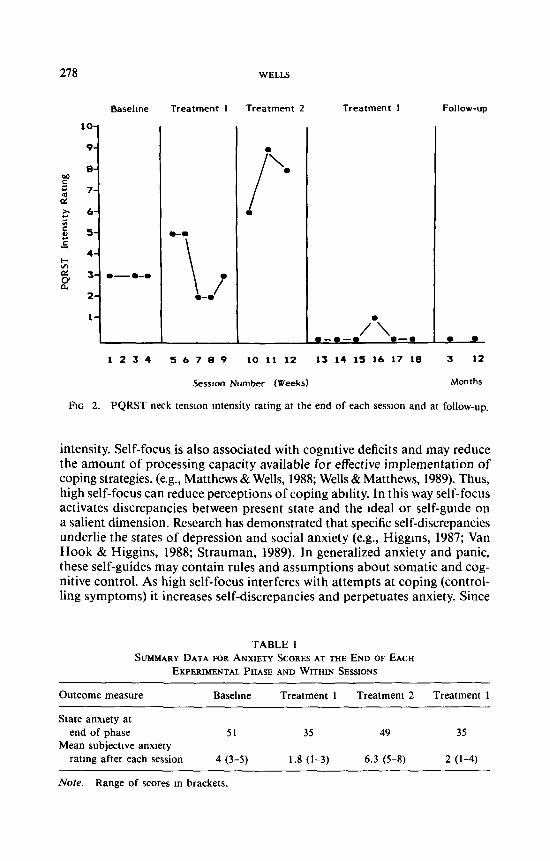
The data for PQRST self-report neck tension are displayed in Figure 2. Neck tension increased above baseline during the first attentional training sessions, and then fluctuated at and below baseline intensity through sessions, 7, 8, and 9. The introduction of autogenic exercises produced a rapid increase in the intensity of within session neck tension which was above any previously recorded levels. When attention training was re-introduced, levels of neck ten- sion rapidly decreased to zero intensity.
Mean self-report ratings for anxiety intensity immediately following atten- tion training and autogenic exercises are displayed in Table 1. These data show

P A N I C 2 7 7
I0-
9-
8 -
¢0 6 -
r- c0 5 -
E Z
FIG. 1.
B a s e h n e Treatment 1 T r e a t m e n t 2 T r e a t m e n t 1
\ 2" I1--•
/ /
9 ~ e ~ e ~ o
I 2 3 4 5 6 7 8 @ t O l I 1 2 1 3 14 1 5 1 6 1 7 18
Weeks
Frequency of panic attacks reported in each week and at follow-up.
Follow-up
3 12
Months
that while attentional exercises decreased anxiety, autogenic exercises increased anxiety in relation to baseline levels. State-anxiety scores measured at the end of each intervention phase are also displayed in Table 1 from which it is ap- parent that attentional training was associated with a decrease in state-anxiety below baseline levels. The effect of introducing autogenic exercises restored state-anxiety levels to an intensity approximating that of baseline.
Follow-up. The patient was interviewed at 3 months and 12 months follow- up sessions, and elimination of panic attacks and neck tension was maintained across that time. For the first two months the patient had continued to prac- tice the attentional procedure on an irregular basis, and then she had discon- tinued practice.
In summary, the results of this study show that attentional training, which promotes external focus, can eliminate panic attacks between sessions and re- duce self-report tension within sessions without exacerbating anxiety. In con- trast, autogenic exercises, which require self-focused attention, can intensify anxiety and panic symptoms. These data are consistent with the view that heightened somatic self-focus is associated with both panic disorder and RIA.
Relaxation procedures which increase self-directed attention may have nega- tive consequences for some individuals. Previous studies have shown that self- focus is positively associated with anxiety in threatening situations (Wells, 1985; 1987). Wells (1987;1989) has proposed a theory of anxiety in which self-focus plays a central role. The theory asserts that high levels of self-focus increase awareness of somatic symptoms and lead to an exaggerated perception of their
278 WELLS
Basel ine T rea tmen t 1 T rea tmen t 2 T rea tmen t 1
t O -
e-
,7, 7 - to ¢v
4 -
G'
2 -
1-
Fxc 2.
Follow-up
I ~ e - - I
/ \ e - - 9 - - q e - - •
1 2 3 4 ~ b 7 8 • 10 11 12 13 14 15 l b 17 t8
I •
3 12
Session Number (Weeks) Months
PQRST neck tension intensity rating at the end of each session and at follow-up.
intensity. Self-focus is also associated with cognitive deficits and may reduce the amount of processing capacity available for effective implementation of coping strategies. (e.g., Matthews & Wells, 1988; Wells & Matthews, 1989). Thus, high self-focus can reduce perceptions of coping abdity. In this way self-focus activates discrepancies between present state and the ~deal or self-grade on a salient dimension. Research has demonstrated that specific self-discrepancies underlie the states of depression and social anxiety (e.g., Higgms, 1987; Van Hook & Higgins, 1988; Strauman, 1989). In generalized anxiety and panic, these self-guides may contain rules and assumptions about somatic and cog- nitive control. As high self-focus interferes with attempts at coping (control- ling symptoms) it increases self-discrepancies and perpetuates anxiety. Since
TABLE 1 SUMMARY DATA FOR ANXIETY SCORES AT THE END OF EACH
EXPERIMENTAL PHASE AND WITHIN SESSIONS
Outcome measure Baseline Treatment 1 Treatment 2 Treatment 1
State anxiety at end of phase 51 35 49 35
Mean subjective anxiety rating after each session 4 (3-5) 1.8 (1-3) 6.3 (5-8) 2 (1-4)
Note. Range of scores m brackets.

PANIC 279
relaxation training increases self-focus it may heighten awareness of symp- toms and self-discrepancies thereby exacerbating anxiety.
There is a growing literature which suggests that exposure to interoceptive cues is effective in the treatment of panic disorder (e.g., Barlow, Craske, Cerny, & Klosco, 1989; Beck, 1988). Barlow et al. (1989) compared the effectiveness of exposure plus cognitive therapy with relaxation training and with a combi- nation of all of these techniques. Their results demonstrated that the treat- ments involving exposure to somatic symptoms plus cognitive skills training were more effective than relaxation training alone in reducing the frequency of panic attacks in panic patients. Relaxation training on the other hand was superior in reducing psychosomatic symptoms. These data suggest that relax- ation has a more general effect on anxiety. However, in the study there was a higher drop-out rate among the patients receiving relaxation than among patients receiving only exposure. The occurrence of RIA may partially ac- count for these drop-out rates.
Evidence supporting the effectiveness of interoceptive exposure in the treat- ment of panic is not inconsistent with the present self-attention theory. Typi- cally, interoceptive exposure techniques consist of the active elicitation of panicogenic symptoms by patients combined with training in cognitive skills such as symptom re-appraisal and self-instruction. It is conceivable that this provides a means of reducing negative discrepancies by increasing perceptions of symptom control. However, in the Barlow et al. (1989) study approximately one-half of the patients who became panic free following exposure treatment were left with residual anxiety and impaired work and social functioning. This effect could be attributed to self-focus remaining high in these individuals. The wide-range effectiveness of treatment techniques for anxiety and panic may depend on the extent to which they modify excessive self-focused attention.
In conclusion, although a moderate amount of self-focus may facilitate cog- nitive and somatic control, high levels of self-focus may disrupt perceptions of control. An important question to be addressed in future studies is whether the effects of relaxation procedures on anxiety are moderated by levels of back- ground self-attention.
REFERENCES American Psychiatric Association (1987) Dtagnosttc and Stattsttcal Manual of Mental Dtsorders-
Revtsed, 3rd ed. APA, Washington, D.C. Barlow, D.H., Craske, M.G., Cerny, J.A., & Klosco, J.S. (1989) Behavioral treatment of panic
disorder. Behavior Therapy, 20, 261-282. Beck, A.T. (1988) Cogmtlve approaches to panic disorder" Theory and therapy In S. Rachman
and J. Maser (Eds), Panw: Psychologtcal Perspectives. Laurence Earlbaum, NJ. Braith, J.A., McCullough, J.P., & Bush, J.P (1988) Relaxation induced anxiety in a subclimcal
sample of chronically anxious subjects. Journal of Behawor Therapy and Experlmental Psy- chtatry, 19, 193-198.
Clark, D.M. (1986) A cognitive approach to pamc. BehavtorResearch and Therapy, 24, 461-470. He,de, EJ., & Borkovec, T.D. (1983) Relaxation-induced anxiety: Paradoxical anxiety enhance-
ment due to relaxation training. Journal of Consulting and Clinical Psychology, 51,171-182.

280 WELLS
Helde, F.J., & Borkovec, T.D. (1984) Relaxation-reduced anxiety: Mechamsms and theoretical lmphcations Behavior Research and Therapy, 22, 1-12
Higgins, E.T. (1987) Self-discrepancy: A theory relating self and affect Psychological Review, 94, 319-340.
Jacobsen, E. (1938) Progressive Relaxation. Umverslty of Chicago Press. Mulhall, D.J. (1978) Manual for the Personal Questionnaire Rapid Scaling Techmque NFER,
Nelson, Windsor England. Matthews, G., & Wells, A. (1988) Relationships between anxiety, self-consciousness and cognitive
failure. Cognition and Emotton, 2, 123-132. Schultz, J H., & Luthe, W. (1969) Autogemc Therapy, Volume L Autogemc methods. Grune and
Stratton: New York. Splelberger, C.D., Gorsuch, R.L., & Lushene, R.E. (1970) Manual for the State-TrattAnxtety In-
ventory. Palo Alto, CA" Consulting Psychologists Press. Strauman, T.J. (1989) Self-discrepancies in clinical depression and social phobia: Cognitive struc-
tures that underlie emotional disorders. Journal of Abnormal Psychology, 98, 14-22. Van Hook, E., & Hlggms, E.T. (1988) Self related problems beyond the self-concept: Motiva-
tional consequences of discrepant self-guides Journal of Personahty and Soctal Psychology, 558, 625-633.
Wells, A. (1985) Relationship between private self-consciousness and anxiety scores in threatening situations. Psychological Reports, 57, 1063-1066.
Wells, A. (1987) Self-attentional processes in anxiety" An experimental study. Unpublished Ph D thesis, Aston University, England.
Wells, A. (1989) Self-attention and anxiety. Paper presented at the World Congress of Cognmve Therapy, Oxford University.
Wells, A., & Matthews, G (1989) Self-consciousness and cognitive failures as predictors of coping in stressful episodes. (Submitted for publication).
RECEIVED: August 9, 1989 FINAL ACCEPTANCE: March 19, 1990