Embed Size (px)
Citation preview

Papillary Lesions of the Breast
A Practical Approach to Diagnosis
Julie M. Jorns, MD
� Papillary lesions of the breast span the spectrum ofbenign, atypical, and malignant. Subclassification of theselesions may be diagnostically challenging, especially withlimited sampling via core biopsy. This review outlines thefeatures of papillary lesions of the breast and provides apractical approach to distinguishing diagnostically chal-lenging lesions by using key morphologic features and,when helpful, immunohistochemical studies.
(Arch Pathol Lab Med. 2016;140:1052–1059; doi:10.5858/arpa.2016-0219-RA)
Papillary lesions of the breast are a heterogeneous groupof neoplasms, which includes benign intraductal papil-
loma (IDP) as well as papilloma with atypia (atypicalpapilloma) and ductal carcinoma in situ (DCIS), papillaryDCIS, and variants of papillary carcinoma. These neoplasmsare unified by ‘‘papillary’’ morphology, consisting ofarborizing fronds with fibrovascular cores of variousthicknesses and lining epithelium. Identification of papillaryarchitecture is often straightforward. However, subclassifi-cation can often prove diagnostically challenging, especiallywhen there is limited lesional tissue present, such as withsuboptimal core biopsy sampling. Key areas of diagnosticchallenge include differentiation of (1) benign IDP with floridhyperplasia and atypical papilloma; (2) atypical papillomaand IDP with DCIS; (3) IDP with widespread DCIS, papillaryDCIS, and papillary carcinoma variants; and (4) pseudoin-vasion and associated frank invasive carcinoma.1,2
INTRADUCTAL PAPILLOMA
Intraductal papilloma is a benign, circumscribed, intra-ductal proliferation comprising fibrovascular cores coveredby benign inner myoepithelial and outer epithelial layers.Intraductal papilloma can be broadly divided into central,which involve large, central lactiferous ducts, and periph-eral, which involve the terminal duct lobular units. Central
IDPs tend to be solitary, and peripheral IDPs are usuallymultiple. Multiple peripheral IDPs are commonly referred toas papillomatosis. Clinically, central IDPs present with nippledischarge that is often bloody. Central papillomas may bemammographically occult or may present with a mass thatcan be large enough to be appreciated via palpation.Peripheral IDPs are most frequently identified as smallmasses or densities on radiographic studies. Both may havemicrocalcifications because these lesions may infarct and/orbecome sclerotic with time.3–5
On histologic examination, IDPs may have variableamounts of epithelium, from one to multiple layers. Theepithelium is often of columnar morphology and/or displaysusual ductal hyperplasia (UDH) and/or apocrine metaplasia.Less frequently, there may be squamous, chondroid, orosseous metaplasia, findings more often identified in thesetting of abundant sclerosis. Depending on the degree ofepithelium present, the myoepithelium may be variablyprominent but is uniformly present, both at the peripheryand within the papillae. Uncommonly, myoepithelialhyperplasia may be seen. Sclerosis is variably prominentand is more pronounced with prior infarction, which may bespontaneous because of limited space for growth within theinvolved duct or torsion of fibrovascular cores, or it may be aresult from biopsy or other trauma.1,2,6–9 Examples of benignIDPs are shown in Figure 1, A through F.
PAPILLOMA WITH ATYPIA (ATYPICAL PAPILLOMA)
There is variability in criteria used for the diagnosis of IDPwith atypia, both in practice and in the literature.10 However,we refer to IDPs with foci of architectural and cytologic atypiathat quantitatively and qualitatively fail to fulfill criteria for thediagnosis of DCIS as papilloma with atypia or atypicalpapilloma; this diagnosis is equivalent to that of atypicalductal hyperplasia elsewhere in the breast. Typically, the IDPexhibits focal solid or cribriform epithelial expansion of small(,0.3 cm) size and composed of small, monotonousepithelial cells. Foci of atypia are negative for high–molecular-weight cytokeratin (CK) 5/6 and diffusely positivefor estrogen receptor (ER) via immunohistochemical (IHC)staining. An example of IDP with atypia and correspondingCK5/6 IHC is shown in Figure 2, A through C.
PAPILLOMA WITH DCIS
Intraductal papillomas that exhibit foci of architectural andcytologic atypia, which would be deemed DCIS elsewhere inthe breast, are designated as IDP with DCIS. These lesions
Accepted for publication May 19, 2016.From the Department of Pathology, University of Michigan, Ann
Arbor.The authors have no relevant financial interest in the products or
companies described in this article.Presented at the New Frontiers in Pathology meeting, October 22–
24, 2015; Ann Arbor, Michigan.Reprints: Julie M. Jorns, MD, Department of Pathology, University
of Michigan, 1500 E Medical Center Dr, Room 2G332, Ann Arbor,MI 48109 (email: [email protected]).
1052 Arch Pathol Lab Med—Vol 140, October 2016 Papillary Lesions of the Breast—Jorns

are usually larger than 0.3 cm and have a solid or cribriform
growth pattern with cytologic enlargement, monotony, and
readily identifiable cell borders. Ductal carcinoma in situ
involving an IDP is usually of low or intermediate nuclear
grade and, thus, shares the IHC staining pattern of atypia,
with the involved foci being CK5/6� and ER being diffusely
positive. An example of IDP with DCIS is shown in Figure 3,
A and B.
Figure 1. Two examples of benign intraductal papilloma. Benign intraductal papilloma with sclerotic capsule, prominent fibrovascular cores andbenign epithelial, and myoepithelial lining at low-power magnification (A) and high-power magnification (B). C through F, Branching benignintraductal papilloma (C) with foci of usual ductal hyperplasia (D), apocrine metaplasia (E), and columnar cell morphology (F) (hematoxylin-eosin,original magnifications 340 [A and C], 3200 [B], and 3400 [D through F]).
Arch Pathol Lab Med—Vol 140, October 2016 Papillary Lesions of the Breast—Jorns 1053

PAPILLARY DCIS
Papillary DCIS is a variant of DCIS with prominentpapillary architecture (ie, delicate papillae with fibrovascularcores). However, the epithelium is neoplastic, and there is
complete involvement of involved ducts with no discernablebenign IDP. Papillary DCIS often exhibits involvement ofmultiple ducts, as seen in all types of DCIS, and is frequentlyseen alongside other patterns of DCIS. Papillary DCIS ismost commonly of low or intermediate nuclear grade andthus is CK5/6� and ER is diffusely positive. Myoepithelium ispresent at the periphery of the duct and is sparse to absentwithin the papillae.11,12 Microcalcifications are variable, andnecrosis is uncommon.1,2 An example of papillary DCIS isshown in Figure 4, A and B.
PAPILLARY CARCINOMA
Papillary carcinoma is an uncommon variant of breastcancer representing just 1% to 2% of breast carcinomas.Papillary carcinoma is more often seen in older women,with a mean age in the seventh decade, as compared withother breast cancer subtypes. Nearly one-half of cases arepresent as a central breast mass, which are usuallycircumscribed on imaging studies. Nearly one-third ofpatients also report bloody nipple discharge. Papillarycarcinoma variants include encapsulated and solid types.2
Encapsulated Papillary Carcinoma
Encapsulated papillary carcinoma was previously referredto as intracystic or encysted papillary carcinoma and wasthought to be a variant of DCIS. The World HealthOrganization classifies these as tumors in situ, and theyare managed accordingly.2–13 However, recent publicationshave shown that most either completely lack myoepithe-lium, both within papillae and at the periphery or, lessfrequently, have very sparse myoepithelium at the peripheryonly. Because of this, authors have suggested that they likelyrepresent a good-prognosis subtype of invasive carcino-ma14–17 or may, at least, be a lesion in transition.2
Encapsulated papillary carcinoma usually presents as asolid mass with surrounding cystic space and a thick,encircling fibrotic capsule. The microscopic features areidentical to that of DCIS within an IDP or papillary DCIS;however, DCIS morphology is present throughout the lesion,and the lesion is typically larger and expansile. Like atypiaand DCIS, the carcinomatous epithelium in encapsulatedpapillary carcinoma is negative for CK5/6. These carcinomasare usually low to intermediate grade and, accordingly, are ERdiffusely positive, although high-grade tumors with less-consistent ER staining are occasionally encountered.18
Encapsulated papillary carcinoma may have associated,frankly invasive components, which are usually of the ductaltype and, when present, should be staged according to thegreatest dimension of invasive ductal carcinoma.2,13 Figure 5,A and B, highlights a case of encapsulated papillarycarcinoma with lack of myoepithelium.
Solid Papillary Carcinoma
Solid papillary carcinoma is a variant of papillarycarcinoma with distinctive morphology characterized byclosely apposed cellular nodules of carcinomatous epithe-lium. The solid nests are typically arranged in a multinodularor jigsawlike pattern within a background of dense fibrosisbut lack an encircling fibrotic capsule. The cells are usuallylow to intermediate grade and often have a neuroendocrineappearance. Unlike the previously described papillarylesions fibrovascular cores may be more delicate and thusmore difficult to identify. Like the encapsulated variant,these tumors are considered in situ but lack myoepithelium
Figure 2. Papilloma with focal atypia (atypical papilloma) at low-power magnification (A) (circle) and high-power magnification (B),and corresponding cytokeratin 5/6 immunohistochemical stain (C)showing lack of epithelial staining and supporting atypia (hematoxylin-eosin, original magnifications 320 [A] and 3400 [B]; originalmagnification 3400 [C]).
1054 Arch Pathol Lab Med—Vol 140, October 2016 Papillary Lesions of the Breast—Jorns

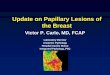
Figure 3. A, Intraductal papilloma with ductal carcinoma in situ (DCIS) with solid growth (circles), moderate cytologic atypia, and prominent cellborders (inset). B, Corresponding cytokeratin 5/6 immunohistochemical staining showing loss of staining within the foci of DCIS (hematoxylin-eosin,original magnifications 340 [A] and 3400 [inset], original magnification 340 [B]).
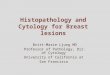
Figure 4. A, Multiple ducts involved by papillary ductal carcinoma in situ, with (B) diffuse, strong positivity for estrogen receptor viaimmunohistochemical staining (hematoxylin-eosin, original magnification 320 [A]; original magnification 320 [B]).
Figure 5. A, Encapsulated papillary carcinoma with thick, fibrous capsule, and (B) corresponding p63 immunohistochemical stain showingcomplete lack of myoepithelium at the periphery and within papillae (hematoxylin-eosin, original magnification 310 [A]; original magnification 310[B]).
Arch Pathol Lab Med—Vol 140, October 2016 Papillary Lesions of the Breast—Jorns 1055

and thus may be better classified as a good-prognosissubtype of invasive carcinoma.2 Additionally, solid papillarycarcinomas are negative for CK5/6 and are often positive forneuroendocrine markers, such as synaptophysin and chro-mogranin. Solid papillary carcinomas may also exhibitintracellular and extracellular mucin production and maybe associated with a frank, invasive component withmucinous or other histology.19–21 An example of a case ofsolid papillary carcinoma is shown in Figure 6.
DIAGNOSTIC CHALLENGES
Differentiating IDP With UDH and Atypia
Atypical papilloma may be difficult to distinguish fromIDP with florid UDH. Histologic features establishing atypiaare identical to those required for diagnosis elsewhere in thebreast and may include focal, solid or cribriform architectureand cytologic monotony. However, florid UDH within anIDP may exhibit increased cell size and reactive changes thatcan be worrisome for atypia. In this setting, IHC may behelpful in establishing the diagnosis of atypia because theselesions have negative staining for CK5/6 and have strong,diffuse positive staining for ER. In contrast, UDH stainsstrongly positive with CK5/6 and, typically, is less strongly
Figure 6. Solid papillary carcinoma comprising irregular nests withindense, fibrotic stroma. Fibrovascular cores (inset) are uniformly presentbut are more subtle than in other papillary lesions of the breast(hematoxylin-eosin, original magnifications 340 and 3400 [inset]).
Figure 7. Case with both benign intraductal papilloma and usual ductal hyperplasia (UDH) (A), with corresponding cytokeratin 5/6immunohistochemical (IHC) stain highlighting UDH (B), and focus of atypia (C), with corresponding cytokeratin 5/6 IHC stain showing loss ofstaining in atypical epithelium (D) (hematoxylin-eosin; original magnification 3200 [A and C]; original magnification 3200 [B and D]).
1056 Arch Pathol Lab Med—Vol 140, October 2016 Papillary Lesions of the Breast—Jorns

ER positive. However, it is important to note that columnarcell alteration (columnar cell change/hyperplasia) andapocrine metaplasia, which are commonly seen in IDPs,are also negative for CK5/6 and thus may be a pitfall in staininterpretation.22,23 Figure 7, A through D, shows a case withareas of IDP with both UDH and atypia and thecorresponding CK5/6 staining.
Differentiating IDP With Atypia From IDP With DCIS
Differentiation of atypia from low-grade DCIS is bestmade morphologically, while accounting for the size of theabnormal area, because it shares the staining pattern seen inatypia. Thus, staining for CK5/6 and ER do not allow fordistinction.23,24 However, these stains may be helpful inhighlighting the area of interest to help determine the extentof involvement of an area that appears morphologicallyabnormal.
Differentiating IDP With Extensive DCIS, Papillary DCIS,and Papillary Carcinoma
An IDP with DCIS is often larger than ducts involved bypapillary DCIS and may be as large as papillary carcinoma.Of importance, IDP with DCIS should still exhibit areasrecognizable as benign IDP, whereas carcinomatousepithelium appears throughout in papillary DCIS andpapillary carcinoma. Additionally, papillary DCIS is typi-cally multifocal, whereas IDP with DCIS and papillarycarcinoma most often have larger, solitary lesions. Fortu-nately, these lesions with morphologic overlap can usuallybe distinguished with the help of IHC because an IDP withDCIS should have myoepithelial staining both at theperiphery and within papillae of the papillary lesion. Thisdiffers from papillary DCIS, which typically has peripheralstaining only, and papillary carcinoma, which typicallylacks myoepithelium altogether or has just very focalperipheral staining.
Despite different patterns of involvement and staining,IDP with extensive DCIS, papillary DCIS, and papillarycarcinoma may be difficult to distinguish, especially if thereis limited lesional tissue present on core biopsy. Fragmen-tation can also make it difficult to determine whether thereis a solitary lesion or a multifocal process and can alsocause difficulty in stain interpretation. Confoundingmatters, these lesions may coexist. For example, papillaryDCIS may be present elsewhere in a patient with an IDPinvolved by DCIS or in a patient with papillary carcinoma.Therefore, different staining patterns may be presentwithin different areas of the core biopsy. In these cases,we cannot always provide definitive diagnoses and,instead, usually designate the lesion as papillary carcinoma,at least in situ and defer definitive classification to theexcision.
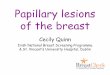
Figure 8 shows a schematic of key features most helpful indifferentiating IDP with DCIS, papillary DCIS, and papillarycarcinoma, taking into account that there may be overlaps offeatures as well as cases with more than one lesion.
Differentiating Pseudoinvasion From Invasive Carcinoma
Benign IDPs with abundant sclerosis represent an area ofsignificant diagnostic challenge because benign glandsentrapped within sclerosis can appear infiltrative and mayalso exhibit reactive atypia, mimicking an invasive carcino-ma. A key feature that helps to establish the diagnosis ofbenign, entrapped glands is background benign histology(ie, there is no indication of a neoplastic process in the IDPor elsewhere). Other features of benignity are confinementwithin investing sclerosis and, if previously biopsied,association with hemorrhage and/or fibrotic biopsy tract.Myoepithelium is usually retained in sclerotic foci withentrapped benign glands, at least in a patchy distribution,further supporting a benign process (Figure 9, A and B).Thus, myoepithelial IHC stains may be helpful to differen-tiate difficult cases from a low-grade invasive carcinoma.
Figure 8. Diagram of key morphologic andimmunohistochemical features useful in dif-ferentiating intraductal papilloma (IDP) withductal carcinoma in situ (DCIS), papillaryDCIS, and papillary carcinoma. Areas ofoverlap may represent coexistence of morethan one lesion.
Arch Pathol Lab Med—Vol 140, October 2016 Papillary Lesions of the Breast—Jorns 1057

However, epithelial displacement may occur because ofprior biopsy, and in this setting, myoepithelium may bescarce or absent. Therefore, other features (ie, hemorrhage,fibrous tract) are most helpful ruling out an invasiveprocess.25
Papillary DCIS or papillary carcinoma may also havepseudoinvasion within surrounding sclerosis or may haveassociated frankly invasive carcinoma. In the case of DCIS,myoepithelial markers are extremely helpful because theyhighlight the periphery or DCIS-involved glands and areabsent in the invasive component (Figure 10, A and B).Conversely, in the setting of papillary carcinoma, pseudoin-filtration in dense sclerosis may be difficult to differentiatefrom true invasion. Unfortunately, in this case, myoepithe-lial stains are not helpful because they typically show loss inboth papillary carcinoma and invasive carcinoma compo-nents. Therefore, invasion beyond the sclerotic capsule and/or hemorrhagic/fibrotic biopsy tract must be present todiagnose definitive invasion (Figure 11). As noted previous-ly, staging should be assessed based on the frankly invasivecomponent alone, if present.
Figure 9. A, Intraductal papilloma with pseudoinfiltrative, benign-appearing glands within the fibrous capsule and associated fat necrosis/biopsysite change. B, Corresponding muscle-specific actin immunohistochemical stain highlighting myoepithelium throughout, supporting benign,entrapped glands (hematoxylin-eosin, original magnification 3 40 [A]; original magnification 340 [B]).
Figure 10. A, Papillary ductal carcinoma in situ (DCIS), with adjacent infiltrative glands suspicious for microinvasive carcinoma. B, Correspondingp63 immunohistochemical stain, highlighting myoepithelium in DCIS and lack of staining within the infiltrative focus, supporting microinvasivecarcinoma (hematoxylin-eosin, original magnification 3100 [A]; original magnification 3100 [B]).
Figure 11. Frank, invasive ductal carcinoma, arising in associationwith an encapsulated papillary carcinoma. Invasive carcinoma extendsbeyond the fibrotic capsule into the adjacent adipose tissue (hematox-ylin-eosin, original magnification 3100).
1058 Arch Pathol Lab Med—Vol 140, October 2016 Papillary Lesions of the Breast—Jorns

DISCUSSION
Papillary lesions of the breast are a heterogeneous groupthat can usually be distinguished via careful histologicevaluation, with the use of IHC when helpful, andconsideration of clinicoradiographic features. Immunohis-tochemistry using CK5/6 is most helpful in supporting amorphologic impression of atypia. Myoepithelial markersare useful in distinguishing IDP with DCIS, papillary DCIS,and papillary carcinoma, as well as in supporting frankinvasion in the setting of DCIS. However, myoepithelialmarkers are not helpful in establishing invasion in thesetting of papillary carcinoma. Diagnostically challengingcases may represent more than a case of papillary neoplasm,and in some cases, definitive classification may need to bedeferred to complete evaluation of the excision specimen.
References
1. Schnitt SJ, Collins LC. Biopsy Interpretation of the Breast. Vol 4.Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 2009. BiopsyInterpretation Series. Epstein JI, series ed.
2. Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ, eds. WHOClassification of Tumours of the Breast. Lyon, France: IARC Press; 2012. WorldHealth Organization Classification of Tumours; vol 4.
3. Muttarak M, Lerttumnongtum P, Chaiwun B, Peh WC. Spectrum ofpapillary lesions of the breast: clinical, imaging, and pathologic correlation. AJRAm J Roentgenol. 2008;191(3):700–707.
4. Daniel BL, Gardner RW, Birdwell RL, Nowels KW, Johnson D. Magneticresonance imaging of intraductal papilloma of the breast. Magn Reson Imaging.2003;21(8):887–892.
5. Yang WT, Suen M, Metreweli C. Sonographic features of benign papillaryneoplasms of the breast: review of 22 patients. J Ultrasound Med. 1997;16(3):161–168.
6. Flint A, Oberman HA. Infarction and squamous metaplasia of intraductalpapilloma: a benign breast lesion that may simulate carcinoma. Hum Pathol.1984;15(8):764–767.
7. Kobayashi TK, Ueda M, Nishino T, Watanabe S, Yakushiji M. Spontaneousinfarction of an intraductal papilloma of the breast: cytological presentation onfine needle aspiration. Cytopathology. 1992;3(6):379–384.
8. Ginter PS, Hoda SA, Ozerdem U. Exuberant squamous metaplasia in anintraductal papilloma of breast. Int J Surg Pathol. 2015;23(2):125–126.
9. Reddick RL, Jennette JC, Askin FB. Squamous metaplasia of the breast: anultrastructural and immunologic evaluation. Am J Clin Pathol. 1985;84(4):530–533.
10. Tavassoli FA. Pathology of the Breast. 2nd ed. Boston, MA: Appleton &Lange, McGraw-Hill; 1999.
11. Papotti M, Eusebi V, Gugliotta P, Bussolati G Immunohistochemicalanalysis of benign and malignant papillary lesions of the breast. Am J Surg Pathol.1983;7(5):451–461.
12. Raju UB, Lee MW, Zarbo RJ, Crissman JD Papillary neoplasia of the breast:immunohistochemically defined myoepithelial cells in the diagnosis of benignand malignant papillary breast neoplasms. Mod Pathol. 1989;2(6):569–576.
13. Rakha EA, Badve S, Eusebi V, et al. Breast lesions of uncertain malignantnature and limited metastatic potential: proposals to improve their recognitionand clinical management. Histopathology. 2016;68(1):45–56.
14. Collins LC, Carlo VP, Hwang H, Barry TS, Gown AM, Schnitt SJ. Intracysticpapillary carcinomas of the breast: a reevaluation using a panel of myoepithelialcell markers. Am J Surg Pathol. 2006;30(8):1002–1007.
15. Rakha EA, Gandhi N, Climent F, et al. Encapsulated papillary carcinoma ofthe breast: an invasive tumor with excellent prognosis. Am J Surg Pathol. 2011;35(8):1093–1103.
16. Wynveen CA, Nehhozina T, Akram M, et al. Intracystic papillarycarcinoma of the breast: an in situ or invasive tumor?: results of immunohisto-chemical analysis and clinical follow-up. Am J Surg Pathol. 2011;35(1):1–14.
17. Rakha EA, Tun M, Junainah E, Ellis IO, Green A. Encapsulated papillarycarcinoma of the breast: a study of invasion associated markers. J Clin Pathol.2012;65(8):710–714.
18. Rakha EA, Varga Z, Elsheik S, Ellis IO. High-grade encapsulated papillarycarcinoma of the breast: an under-recognized entity. Histopathology. 2015;66(5):740–746.
19. Maluf HM, Koerner FC. Solid papillary carcinoma of the breast. A form ofintraductal carcinoma with endocrine differentiation frequently associated withmucinous carcinoma. Am J Surg Pathol. 1995;19(11):1237–1244.
20. Nassar H, Qureshi H, Adsay NV, Visscher D. Clinicopathologic analysis ofsolid papillary carcinoma of the breast and associated invasive carcinomas. Am JSurg Pathol. 2006;30(4):501–507.
21. Guo S, Wang Y, Rohr J, et al. Solid papillary carcinoma of the breast: aspecial entity needs to be distinguished from conventional invasive carcinomaavoiding over-treatment. Breast. 2016;26:67–72.
22. Simpson PT, Gale T, Reis-Filho JS, et al. Columnar cell lesions of the breast:the missing link in breast cancer progression?: a morphological and molecularanalysis. Am J Surg Pathol. 2005;29(6):734–746.
23. Nofech-Mozes S, Holloway C, Hanna W. The role of cytokeratin 5/6 as anadjunct diagnostic tool in breast core needle biopsies. Int J Surg Pathol. 2008;16(4):399–406.
24. Lacroix-Triki M, Mery E, Voigt JJ, Istier L, Rochaix P. Value of cytokeratin 5/6 immunostaining using D5/16 B4 antibody in the spectrum of proliferativeintraepithelial lesions of the breast: a comparative study with 34bE12 antibody.Virchows Arch. 2003;442(6):548–554.
25. Phelan S, O’Doherty A, Hill A, Quinn CM. Epithelial displacement duringbreast needle core biopsy causes diagnostic difficulties in subsequent surgicalexcision specimens. J Clin Pathol. 2007;60(4):373–376.
Arch Pathol Lab Med—Vol 140, October 2016 Papillary Lesions of the Breast—Jorns 1059