Embed Size (px)
Citation preview
PARADIGM SHIFTING
Three Rivers takes referrals only from
Psychiatric Hospitalizations,
or sometimes Crisis Stabilization Units.
Children ages 6-12, highest level of acuity.
Small Program—only 12 beds
“Hey everybody, let’s try not to restrain kids! Central Office doesn’t want us to.”
So the Program Director and I went in during a crisis and tried our darndest to de-escalate an enraged child to role model restraint avoidance. He punched us for ten minutes and finally had to be held.
Thus, our first step was a step backwards.
Don’t do this.
Restraints for the year : 274 (about 2 per month per child.)
Learning: Restraint Reduction happens upstream from crises
It can’t mean just let kids hurt us.
Ultimately it means violence prevention.

Coercive Techniques
Restraint, escort, restrictive rules, guilt trips, threats of consequences
?
Framing the Project
64 thousand dollar question: Is there an approach or technique that is more effective at influencing youth behavior than the traditional approach?
Seriously, is it possible to make staff safer, reduce violence, and reduce restraints?
“We’re supposed to use Sensory Stuff.”
Gave ourselves training in Sensory Integration.
Deep pressure, Heavy work, Vestibular, Tactile.
Learned some new games.
Staff didn’t really feel comfortable with or excited about the new games. This did not pan out.
The sensory supports during school began to foster a new pattern where staff were offering supports instead of consequences for agitated kids. Maybe the first crack in the old paradigm.
We did all get behind the idea of getting kids more active.
2002-2003

Digression—some quick observations about sensory interventions
Emotions are physical. People with overwhelming emotional distress have distressed nervous systems.
They may or may not, however, instantly enjoy healing sensory input. It’s new. A person who is used to over-stimulating themselves may not like soothing and calming. It takes some practice and getting used to.
It’s probably new to the whole social culture. The program needs to attend to making it a natural pathway of behavior for both staff and consumer to use sensory interventions. It tends to lose momentum.
There can be an immediate benefit in changing the kind of conversation that takes place between staff and a client who is agitated– a shift away from threat of consequences and even away from asking them to tell you what they are upset about (being asked to explain your feelings when you are upset may well be an unwelcome demand), toward simply offering something to make them feel better. This is a big difference.
Sensory Approaches have become fundamental. A kit in every classroom and one for staff. A sensory room. Swing in the Quiet Room. A rocking chair in every bedroom.
A Few Reflections on Sensory Approaches
I really liked this idea of “Massive Doses of Signals of Caring,”and it doesn’t threaten anyone --mostly.
Children’s Art Gallery Mural on wall Names on doors Emphasize kind tone of voice Emphasize listening Wanting kids to have fun Subtle changes in what staff were willing to do for kids—less worry about
jealousy (this may threaten some practices). Try to accommodate individual preferences and requests (this may
threaten some practices). Create special whole-program activities (We did a winter festival, went to
the cape, Holiday show etc.) Make sure we provide the resources for kids to have fun.
First Real Structural Change– Shortening Duration of Consequences
“Kids don’t even remember why they are on these restrictions!”
Kids need to have fun to stay motivated. They need vitality.
The purpose of these restrictions is to motivate kids! Is that happening? Is there a more potent way to get kids to want to do better?
Quick recovery is MORE motivating than days of restriction.
2003-2004
These were incremental shifts in both practice and thinking.
For kids to be motivated to avoid missing activities, those activities have to be fun.
Adjusted budget to get more money into the activities budget Brought topic of activities planning routinely to shift meetings Assigned someone to be Activities Coordinator and plan activities for the staff
to do. This ended up being a bad plan. Staff became more passive about activities, and there were many conflicts. For us the only road to success was getting the staff who were going to do the activities excited about trying new things, having fun, and planning ahead.
We encourage staff to play with the kids and not stand apart like guards or shepherds, though that’s okay sometimes.
(2004-2005)
Activities serve many purposes: (not just to pass the time).
1. Increase resilience to stress by creating a reservoir of pleasure2. Show we care3. Foster bonding with staff through having fun together.4. Offer joint pressure, and heavy work to calm nervous system5. Foster feeling that life is worth living– counter feelings of hopelessness & apathy6. Provide leverage so kids will do repair work, or avoid consequences altogether
Created New Simplified Level System
• Simple• Non judgmental• Quick Recovery• Emphasize Learning over Suffering as a response to problems
• Two Levels: Stop & Think and Getting Along.• Stop & Think had two types
Yellow for immediate recovery andRed for longer repair, but can be done in 24 hours.
Getting Along was called Green. So it became a Red-Yellow-Green Level system. We Liked it. (restraints still high in 2005)
2005
Restraints for the year: 251
For ConsequencesReplacing Doing Time with Doing Work.
• Being able to actively repair damage fosters hope, empowerment and healthy guilt instead of toxic shame. (Doing time seems to foster the feeling of having failed and taking your punishment). The message that emotional damage can be repaired is a powerful healing message.
• We tried having clinicians make up work for kids to do following a serious behavioral incident. That didn’t work well. Too repetitive and not tailored to the actual incident.
• Tried using: Review and Role Play your Skills Plan. That also become rote.
• Finally staff (during a Restraint Review Committee Meeting) offered that they design the repair work for each incident tailored to that particular incident and that particular child. In the past that may have turned into “individualized punishment.” However, the staff appreciate the spirit of Repair, Learn, Practice for next time. They naturally need support in keeping this process meaningful and targeted.
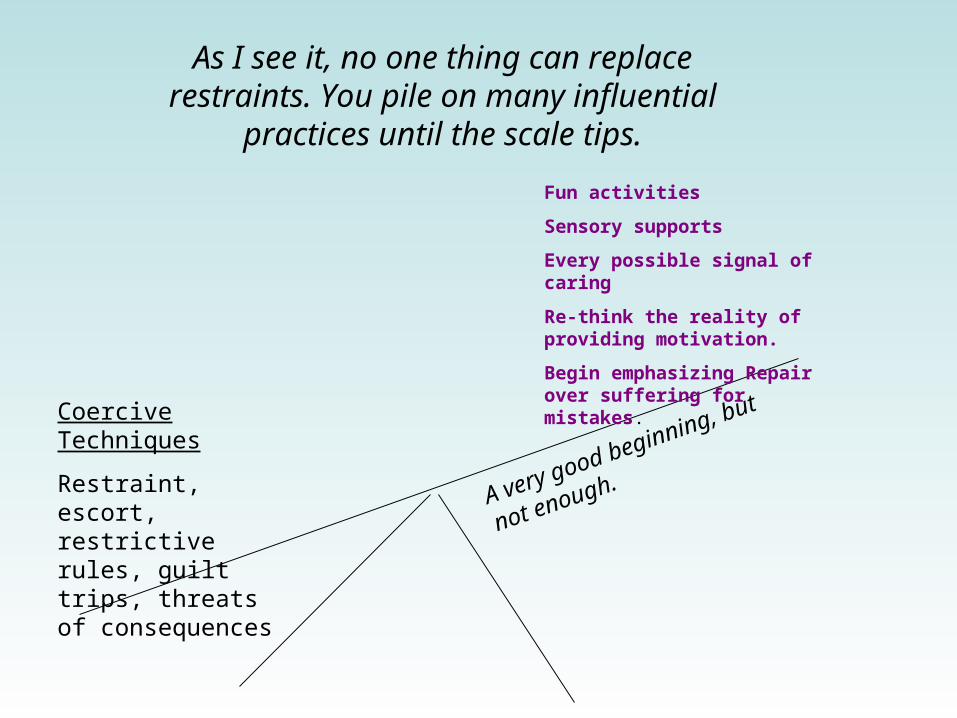
Coercive Techniques
Restraint, escort, restrictive rules, guilt trips, threats of consequences
Fun activities
Sensory supports
Every possible signal of caring
Re-think the reality of providing motivation.
Begin emphasizing Repair over suffering for mistakes.
As I see it, no one thing can replace restraints. You pile on many influential practices until
the scale tips.
A very good beginning, but
not enough.

No shame. No ridicule.
I think it is worthwhile to honestly validate the thinking behind traditional practices. Not to frame them as abusive and stupid. While acknowledging that the field has made some very profound advances
I personally do not find the facts that some other programs were abusive inspiring.
I find moving toward the creation of something beautiful inspiring. That is how I have approached my staff.
Something Beautiful

The argument for more coercive means of behavior management
As a result of trauma, children have ingrained patterns of self protection that are ultimately destructive of their relationships and selves. Because they are so profoundly fear-driven, children will not give up these behaviors easily.
These children cannot be motivated by empathy for others because they are frozen in self-protection. Therefore, to motivate them we need to create an environment where the results they get from their dysfunctional and dangerous behaviors are less rewarding to them personally than are those from an alternative behavior we are attempting to teach them. Our job is to frustrate their habitual pattern in order to coax them to try new behaviors for which we then reward them and hope they find intrinsically rewarding.
The argument for more coercive means of behavior management --cont.
Also, the more times a child repeats a pattern of violent behavior, the more ingrained it becomes. Permissiveness leads to neurological reinforcement of the problem behavior.
Coercive techniques often do work in the short run to create compliance or a safer feeling for many people present during crises. The longer term damage to treatment can be either consciously or unconsciously sacrificed to the immediate need for order. Restraints are inherently risky, but violence is guaranteed to hurt.
This is not a mean-spirited idea, but it is seriously flawed and outdated by current understanding.

Children’s trauma-induced, fear-based behavior is indeed deeply ingrained; however, new patterns will not emerge by the further application of threats, power struggles, and physical coercion. These children need to be surrounded by feelings of emotional safety and physical safety. Not judged or blamed. Not threatened and not over-powered.
Experiences of empowerment, pleasure and cooperation will be keys to their recovery more than experiences of obedience under threat. They will risk trying new behaviors because they feel they have allies who offer hopefulness and forgiveness, who genuinely care about their success, and who are not forcing them.
Paradigm Shift
You have to decide whether to act more confident than you actually feel about the belief this change will work. Probably you do.
Leadership has to find a balance between insisting on change while listening to and engaging staff.
Some Thoughts on Leadership
A Key Point:
There are quite a lot of initiatives you can introduce before you have to start giving up current practices. The program’s clinical thinking can gradually shift while undertaking these relatively less threatening changes.
Later, I found it helpful to try to replace the question, “Will this new approach work” with the question “Is there anything we haven’t tried yet?” Until we’ve actually done everything we can think of, we can’t say it doesn’t work.
• Validation of the reasoning and good intentions of past practice
• Intellectual Honesty. Besides validation, use current understanding of how trauma effects the brain, research on impermanence of changes based on fear of consequences, example of success in working in a different way. Ask the questions if children are learning to feel safe, connected, supported, forgiven, hopeful, and competent. That life holds pleasure and that people believe in them.
• Frame the goal as reducing incidents of violence, making staff safer. The main concern of staff is whether they will be put in greater danger due to these changes. The answer must be No. Restraint reduction does not mean that children should be allowed to perpetrate violence on others. It is about becoming more effective in reducing and responding to dangerous behavior.
Helping Everyone Buy In

Helping Everyone Buy In
• No one has all the answers. We are all pioneers. That can be a fun feeling-- certainly a better feeling than the frame that we’re being forced to change because other programs abused kids. (which is true in part, but unhelpful) The fact is that non-coercive care is worth learning.
•Again, there are many innovations to introduce before you need to take anything away. Ultimately the paradigm shift does require abandoning many practices; but you can build a lot of momentum introducing supportive interventions before you start taking anything away.
•Pay noticeable, public attention to staff who offer helpful observations and attitudes. What staff learn about how to help children is precious. Show that.
• Talk directly about the issue of change in itself.

Talk directly about the issue of change in itself.
• Not all change is good, but nothing gets better without it.
• Let’s not be so arrogant or rigid so as to believe that we can’t grow and learn.
•“Are you saying we’re no good?” “I’m saying we’re great and can do better.” Even “best practices” are only best until we imagine something better.
• In the face of dangerous behaviors, let’s not speculate about whether this new approach can work. Let’s ask, “Is there anything we haven’t tried yet to support getting the best from this youth?”
Mountain Metaphor
After some time—probably a couple of years-- I told staff that we are committed to climbing this mountain. They were welcome to point out the obstacles and warn of dangers involved. But we were not going to discuss any more whether or not we are going up.

Neither staff nor clinicians nor children have been complaining about the Behavioral System we use now
We let go of the Red Yellow Green system, for a few reasons
1. Staff found that telling a child they had “dropped” to Red or Yellow was causing a large percentage of behavioral escalations. Some staff were avoiding dropping kids just to avoid triggering them.
2. Staff wanted to be able to respond uniquely and authentically to problems without any: “This behavior equals this consequence” judicial system. They wanted to say, “Here’s what just happened. You need to take care of this.” within the guideline of Talk, Fix-it, Smile, or Review, Repair, Practice and get back to hopeful feeling about the future.
3. We can exercise our judgment about whether a given activity will be helpful or safe for a child based on real reasons and not generic rules.
4. There was a somewhat unanticipated, but huge benefit of changing the culture between adults and kids. Less us against them. Kids believe we are on their side.
What!? No Level system?!
2008
Restraints for year: 91 (about 1/3 of previous year) basically the same for 2009 as well

What!? No Level system?!Well, we do have something called “Safety Protocol.” Which means that you don’t watch
TV or go off grounds until you finish your repair work.
There is no “This equals that” for consequences, though we do have general guidelines that kids will clean up what they spit on, etc.
We made a significant mistake that in our effort to avoid power struggles we were ignoring a lot of disruptive and even escalated behaviors. Mayhem began to flourish. We adjusted by emphasizing that staff be assertive and persistent in both their tone and expectations, but not resorting to immediate threats in addressing problems.
The fear that making individualized responses to children will cause complaints of unfairness by peers has just not materialized. Not sure why. Maybe because treating each person uniquely is so permeated into the culture.
The concern that staff will become punitive or vengeful surfaces occasionally with children who are particularly violent or offensive. It is not overwhelming. We keep focused on the common ground of asking how to get the best behavior from each child. For some few, strong consequences for misbehavior seem to help. For most, other supports for success are most effective.
Training in New Skills
We explored for new training content that emphasized not just de-escalation, but crisis prevention and culture change.
Specific techniques to Maximize Staff Influence and Minimize the use of coercive techniques.
• Moment to moment assessment of a child’s level of stability• Matching an intervention to that level• Building Partnering Relationships• Pre-teaching• Motivation without threats• Early Intervention• Ways to build up a child’s mood and resilience• Creating situations that are as safe as possible• Being persistent without escalating a situation• Individualizing your response to each child• Emphasizing intrinsic rewards of positive behavior• Facilitating soothing and self-soothing• Power of Refocusing attention
The shift in thinking is the shift from prioritizing justice to prioritizing healing. This includes a shift toward a skills-deficit model.
You say…
“You’re not ready for a performance yet, let’s keep practicing. Don’t give up. I’ll teach you. You can learn this.”
Not, for example…
“I can’t let this guy get away with hitting a wrong note. They need to be punished or they’ll never learn.”
You don’t punish your piano student for making mistakes.
Paradigm Shift
The middle ground between
Accountability can mean
How you act matters: to people who care about you, to people you directly affect, and to you. You have a responsibility to your relationships.
• To repair damage• To try to prevent damage• To avoid situations that are unsafe
“Our job is to catch kids making mistakes and make sure they get a consequence.”
No accountability and culture of permissiveness
Began to take pride in avoiding restraints
Wanting to avoid restraints naturally stimulated conversations about:
• Eliminating unnecessary rules that created power struggles with kids or with their families.
• In general we shifted from Rules to Values. We became more flexible with families and kids without abandoning our values—at all.
• Looked for accommodations to help kids have success. Prioritize individual needs over group norms to help child succeed. (for example, a child that couldn’t handle the stimulation in the dining room).
• How to effectively and quickly share what staff learn about triggers and supports for each child.
2010 restraints for the year: 12
Coercive TechniquesRestraint, escort, restrictive rules, guilt trips, threats of consequences
The single biggest shift is the change in attitude from belief that consequences are the most potent agent of change, to belief that education and emotional supports are effective and efficient agents of change.
Early Intervention: means staff intervene before they need to. This includes taking opportunities to build positive experiences with kids, teaching outside the context of a failure, and it means offering support when a child is only slightly agitated—which also means becoming skilled at assessing children’s level of dyscontrol or agitation
Attitude of maximizing influence
Coercive TechniquesRestraint, escort, restrictive rules, guilt trips, threats of consequences
• Use Repair and Practice in response to problem behaviors• Requires strong avenues of communication within the program• Prioritize kids feeling emotionally and physically safe.• Foster Partnering Relationships• Staff stay self-regulated• Teach Self soothing strategies (not only sensory approaches—self talk, being alone, etc.)• Motivation enhanced through feeling hopeful, cared for, supported, (not just threats)• Support social skills –teach, pre-teach, practice, coach in the moment.• Adjust environment to minimize conflicts, maximize supports.• Provide fun activities--Make sure there are fun things to look forward to—staff make them fun with attitude.•Eliminate unnecessary rules
Coercive TechniquesRestraint, escort, restrictive rules, guilt trips, threats of consequences
Maximize Staff Influence: The most valuable asset a staff can have when engaging with a child is influence. Consider what are the qualities that make a person the most influential.
Maximize Learning: before during and after incidents. Consider most educational response and environment—prioritize this over justice.
Foster experiences of Success: adjust environment, pre-teach, coach in the moment, offer every conceivable support so children develop a pool experiences that support confidence and hope, and familiarity with a new skill or behavior.
Build up Resilience: Connection, Fun, Competence, Hope, Safety, Contribution, Empowerment.
Build Alliance with Family

Coercive TechniquesRestraint, escort, restrictive rules, guilt trips, threats of consequences
Analyze restraints and patterns of problem behaviors looking for what challenge is that youth overwhelmed by, and what can we do for them.
Resist habit of attributing everything to motivation—and also be serious about increasing motivation (the way you would like to be motivated).
Dote on good staff—in public
Some thoughts on Debriefing Restraints
Debriefing with child:
We decided that when staff debrief with a child they do not being a clipboard. They fill out the form afterward so that the conversation is more natural.
Staff are expected to start with a statement that they are sorry that this happened and that this is not the way we want to work with kids. They want to wonder together about how to keep this from happening again.
It is not safe to assume that children do not like to be restrained. Some like the struggle, the containment, the touch.
We allow touch between staff and children. I think it would be much harder to reduce restraints without that. Touch establishes rapport very powerfully. If the only way a youth can get touched is to get restrained, many will choose this.

Debriefing with adults:
This can be a good source of info about programmatic structures that foster power struggles. (Rules, routines, even physical layout of things.)Or a particular child’s response to them: such as transitions from play to classroom etc.
It reminds staff of all the options that are available to them. (Did we try switching staff? Offering phone call to parent? Remind them of their skills plan?)
It also provides info about child’s response to humor, being given physical space, possible positive distracters, etc.
It does not lend itself to a complete and true functional analysis because staff usually are not aware of agitation in their own body language or tone of voice. They don’t notice that they talked too much at a child who is upset—things like that.
Restraint review committee
I have found these conversations to be more fruitful because they are attended by more people who were not in fact present during the restraint. With other shifts and clinicians participating, more information about a child’s sensitivities and strengths interacts, and we can generate more hope and more ideas about what works for that child. They can’t observe that someone was impatient, but they can offer observations about a child being highly sensitive to impatience.
It’s a mistake to assume that restraints are caused by staff being willful. There are many other causes. I made a little graphic model to represent a hierarchy of less common and more challenging causes of restraint. I don’t expect staff to use it, but I have shared it with clinical staff and it certainly informs my input.
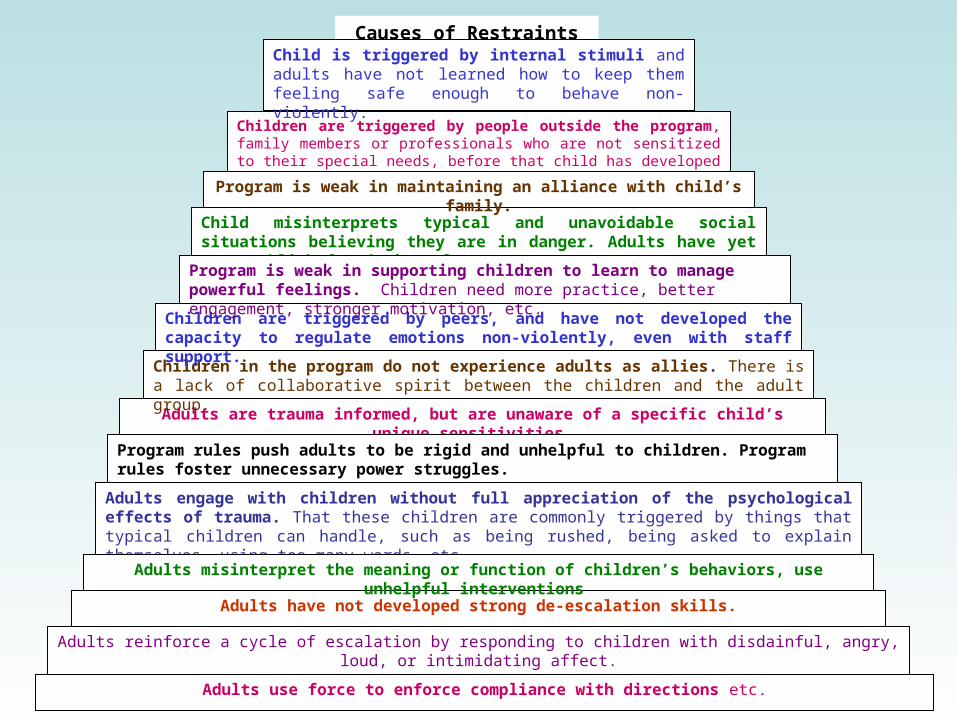
Adults engage with children without full appreciation of the psychological effects of trauma. That these children are commonly triggered by things that typical children can handle, such as being rushed, being asked to explain themselves, using too many words, etc.
Adults are trauma informed, but are unaware of a specific child’s unique sensitivities.
Adults have not developed strong de-escalation skills.
Adults use force to enforce compliance with directions etc.
Adults reinforce a cycle of escalation by responding to children with disdainful, angry, loud, or intimidating affect.
Children in the program do not experience adults as allies. There is a lack of collaborative spirit between the children and the adult group.
Children are triggered by peers, and have not developed the capacity to regulate emotions non-violently, even with staff support.
Children are triggered by people outside the program, family members or professionals who are not sensitized to their special needs, before that child has developed the capacity to self-regulate with staff support.
Child misinterprets typical and unavoidable social situations believing they are in danger. Adults have yet to establish foundation of trust.
Program is weak in maintaining an alliance with child’s family.
Adults misinterpret the meaning or function of children’s behaviors, use unhelpful interventions
Program rules push adults to be rigid and unhelpful to children. Program rules foster unnecessary power struggles.
Program is weak in supporting children to learn to manage powerful feelings. Children need more practice, better engagement, stronger motivation, etc.
Causes of Restraints PyramidChild is triggered by internal stimuli and adults have not learned how to keep them feeling safe enough to behave non-violently.
Some Things that are working for us now
• TEAM meeting asks each week for what staff know of triggers and approaches for each child.
• Those recommendations are published weekly and reviewed in shift meeting
• Key items are maintained in staff book called “Milieu Guidelines”• These are adapted into “Recommendations for Parents.”
Repair Work:Smaller repairs can be done immediately.Other repair work can be time consuming. We often have children work
together, especially if they were involved in the same incident.We schedule repair work during an activity time after school. Children can
work efficiently and join the activity. The spirit of this really is non-punitive. How can you mend a relationship? What can you practice to help prevent this from happening again? Is there something to clean up physically. Sometimes repair work is simply playing a game with the person you hit to practice getting along with them.

Current Directions
Be vigilant to maintain what’s working. Make sure that we keep up trainings, enthusiasm, activities, and stay energized to Prevent more than react.
Enhance work with families.
Teach psycho-social skills more effectively
Enhance children feeling ownership and hope regarding their own recovery.
Better nutrition
Better ways to support staff
A system (like functional analysis) to explore all the possible factors contributing to a problem behavior