Embed Size (px)
Citation preview
Paraneoplastic Facial and Upper Extremity Edema:A New Clinical Entity?Berna Aksoy,1* MD, Abdülkadir Cengiz,2 MD, Temel Sarıoğlu,3 MD
Address: 1Dermatology, 2Internal Medicine and 3Radiology Clinics, TDV 29 Mayis Hospital, Ankara, TurkeyE-mail: [email protected]* Corresponding Author: Dr. Berna Aksoy, Özel Konak Hastanesi, Yenişehir mah. Dönmez sok. No: 53 Bekirpaşa,İzmit, Kocaeli, 41050, Türkiye
Case Report
Published:J Turk Acad Dermatol 2010; 4 (1): 04102cThis article is available from: http://www.jotad.org/2010/1/jtad04102c.pdfKey Words: edema, orofacial, paraganglioma, paraneoplastic, upper extremity
Abstract
Observations: Chronic orofacial edema may be a sign of a number of different clinical entities mostof which are intermittently recurrrent, chronic and erythematous. In this case report, we report apatient with paraneoplastic chronic orofacial and hand edema. Fifty four-year-old female patientwas admitted with a complaint of swelling of the face and hands that had been present for 5 years.Upper abdominal computed tomography revealed a hypodense, solid, retroperitoneal massmeasuring 53x85x100 mm in the left middle abdominal quadrant. The patient had been operatedand the histopathological investigation of this retroperitoneal mass revealed paraganglioma. Fourand a half months following the operation the patient reported that her facial edema decreasedin intensity by 90%. Here, we present a case of retroperitoneal paraganglioma existing with chronicfacial and upper extremity edema that was thought to be a paraneoplastic phenomenon.
Introduction
Chronic orofacial edema may be a sign of anumber of different clinical entities [1]. Here-ditary angioedema, thyroid disorders, supe-rior vena cava syndrome, dental infections,recurrent erysipelas, chronic herpes simplexlabialis, Crohn's disease, sarcoidosis, amyloi-dosis, local neoplasms, facial vasculitis, facialedema with eosinophilia, Ascher's syndromeand Melkersson-Rosenthal syndrome may bepresent with chronic orofacial edema [1, 2,3]. Most of them are intermittently recurr-rent, chronic and erythematous. A number ofchronic orofacial edema cases were reportedin the literature related to local factors inclu-ding facial, neck or chest problems.
Here, we describe a patient with paraneoplas-tic chronic orofacial and hand edema that
seems to result from a distant etiologic factor:Paraganglioma (PGL)
Case ReportFifty four-year-old female patient was admittedwith a complaint of swelling of her face and handswhich had been present for five years. The facialand hand edema had been present and prominentevery morning and decreased in intensity and dis-appeared at night. There was only edema withouterythema, pruritus and dyspnea. The edema hadnot been associated with cosmetics, oral hygieneproducts, foods and sun exposure but edema hadbeen increased in intensity with hot weather. Noother provocative factors such as cold, sunlight,physical exercise or infection (herpes, streptococ-cus and chronic periodontal infections) could beidentified by patient history or examination. Shehad had no known allergies. The patient had de-scribed myalgia but not proximal muscular weak-
Page 1 of 4(page number not for citation purposes)
ness. She had denied any gastrointestinal, cardio-logical, respiratory or endocrine disorders. Shehad never been hospitalized and never had facialparalysis. In the past medical history, the patienthad been in menopause, using oral iron pills foranemia and had underwent operation for carpaltunnel syndrome. The patient did not describe anysimilar findings in her family. The patient lost 5kilos of weight and had a cough but her generalsystemic health was normal. In dermatologic ex-amination; a non-pitting, indurated, non-tenderedema was detected on the face, particularly in theeyelids, cheeks and upper lip and also in thehands [Figure 1]. There were no peripheral lym-phadenopathies. The tongue was normal. Therewere inconspicuous collateral vessels and fullnessin the jugular veins increasing with inspirium.
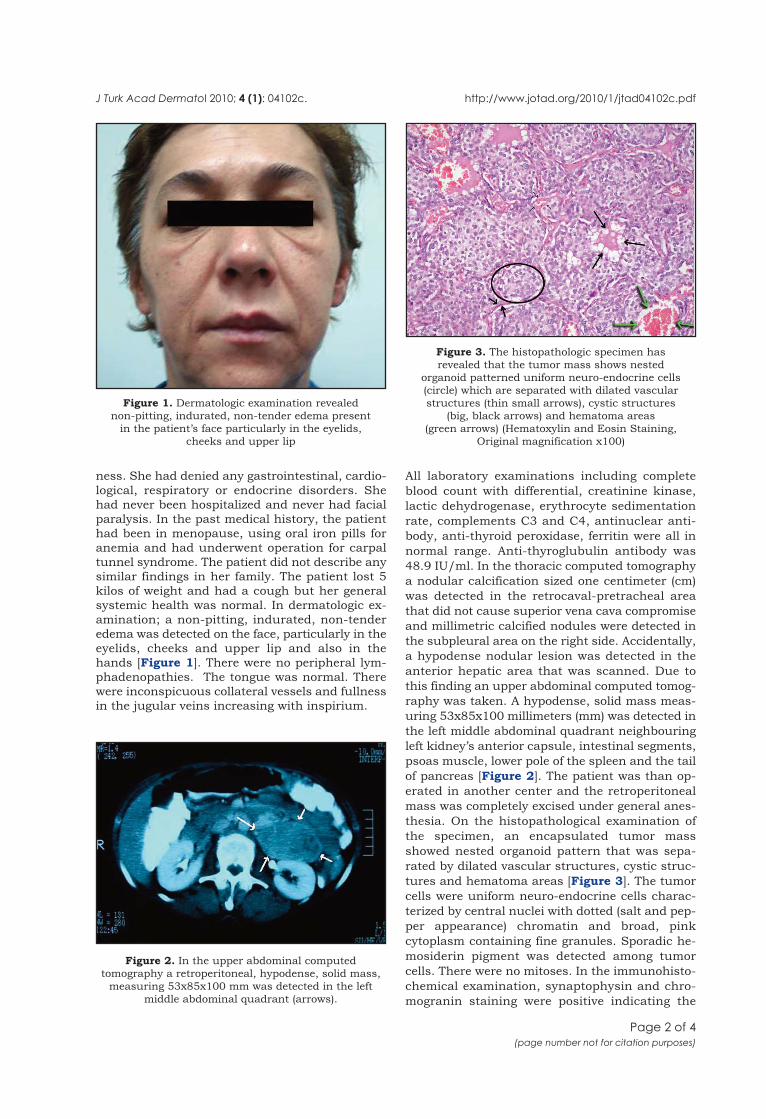
All laboratory examinations including completeblood count with differential, creatinine kinase,lactic dehydrogenase, erythrocyte sedimentationrate, complements C3 and C4, antinuclear anti-body, anti-thyroid peroxidase, ferritin were all innormal range. Anti-thyroglubulin antibody was48.9 IU/ml. In the thoracic computed tomographya nodular calcification sized one centimeter (cm)was detected in the retrocaval-pretracheal areathat did not cause superior vena cava compromiseand millimetric calcified nodules were detected inthe subpleural area on the right side. Accidentally,a hypodense nodular lesion was detected in theanterior hepatic area that was scanned. Due tothis finding an upper abdominal computed tomog-raphy was taken. A hypodense, solid mass meas-uring 53x85x100 millimeters (mm) was detected inthe left middle abdominal quadrant neighbouringleft kidney’s anterior capsule, intestinal segments,psoas muscle, lower pole of the spleen and the tailof pancreas [Figure 2]. The patient was than op-erated in another center and the retroperitonealmass was completely excised under general anes-thesia. On the histopathological examination ofthe specimen, an encapsulated tumor massshowed nested organoid pattern that was sepa-rated by dilated vascular structures, cystic struc-tures and hematoma areas [Figure 3]. The tumorcells were uniform neuro-endocrine cells charac-terized by central nuclei with dotted (salt and pep-per appearance) chromatin and broad, pinkcytoplasm containing fine granules. Sporadic he-mosiderin pigment was detected among tumorcells. There were no mitoses. In the immunohisto-chemical examination, synaptophysin and chro-mogranin staining were positive indicating the
J Turk Acad Dermatol 2010; 4 (1): 04102c. http://www.jotad.org/2010/1/jtad04102c.pdf
Page 2 of 4(page number not for citation purposes)
Figure 1. Dermatologic examination revealednon-pitting, indurated, non-tender edema present
in the patient’s face particularly in the eyelids,cheeks and upper lip
Figure 2. In the upper abdominal computedtomography a retroperitoneal, hypodense, solid mass,
measuring 53x85x100 mm was detected in the leftmiddle abdominal quadrant (arrows).
Figure 3. The histopathologic specimen hasrevealed that the tumor mass shows nested
organoid patterned uniform neuro-endocrine cells(circle) which are separated with dilated vascularstructures (thin small arrows), cystic structures
(big, black arrows) and hematoma areas(green arrows) (Hematoxylin and Eosin Staining,
Original magnification x100)

neuroendocrine character of the tumor cells. Thehistopathological diagnosis was paraganglioma.
Four and a half months after the operation, the pa-tient stated that her facial edema had decreasedin intensity by 90% one month after the operation[Figure 4]. She gained 5 kilos and was well with-out any sign of recurrence.
DiscussionIn the differential diagnosis of chronic orofa-cial edema, various disorders should be keptin mind [1]. All of them are entities that actlocally as a space occupying lesion or are theresult of local edema because of various localacting disease processes. For the presentcase detailed examination disclosed aretroperitoneal mass and a retrocaval nodu-lar calcification that had not any superiorvena cava compromise. After the operation forthe retroperitoneal mass, she experienced adecrease of intensity by 90% in the upper ex-tremity and facial edema in the first postop-erative month. This observation led us to theconclusion that the edema of our patient wasrelated to the retroperitoneal mass lesion.
The adrenal medulla and sympathetic nerv-ous system ganglia are derived from the neu-ral crest and synthesize and secretecatecholamines. PGLs are rare tumors thatarise from the chromaffine cells. Pheochro-mocytomas are rare tumors arising from cate-
cholamine producing cells in the adrenalmedulla – an intraadrenal PGL. Adrenal andextraadrenal PGLs produce significantamounts of catecholamines and give rise to theclinical picture of pheochromocytoma. PGLsare classified as sympathetic or parasympa-thetic PGLs according to their origin.
Sympathetic PGLs are derived from the sym-pathetic chain of chest, abdomen or pelvis andproduce clinical symptoms as a consequenceof either the secretion of catecholamines or thesize of the tumors with consequent impinge-ment on neighboring structures. On the otherhand, parasympathetic PGLs are tumors ofparasympathetic ganglia that are usually lo-cated in the head and neck region and usuallybiochemically silent.
As in our case, nine percent of PGLs were di-agnosed incidentally during the imaging forother diseases. Retroperitoneal PGLs aremost likely to be malignant and present witha mass effect or pain. They metastasize tolungs, lymph nodes or bones or locally extendto vertebral column. In our patient, anymetastases or either local extension was notdetected.
The clinical presentation of PGLs is usually alocal mass effect or rarely of classic cate-cholamine excess characterized by headaches,palpitations, perspiration, pallor, orthostasisand hypertension. About 8% of patients maybe completely asymptomatic. We did not ob-serve any symptoms caused by catecholamineexcess in our patient with retroperitoneal PGLbut only weight loss and upper body edemawere present.
Our patient did not have any family history.As the age of the patient was older and shedid not fulfill the other several clinical crite-ria, a genetic testing was not ordered. Genetictesting is recommended in young adults, es-pecially for those having von-Hippel-Lindaudisease [4].
PGLs secrete catecholamines (hypertension),neuropeptide Y (hypertension), PTHrP (hyper-calcemia), ACTH (Cushing's syndrome), ery-thropoietin (erythrocytosis), and IL-6 (fever)[4]. Obviously, our patient's clinical picturewas not a Cushing's syndrome. As our patientdid not have any clinical symptoms men-tioned and not have a histopathological diag-nosis before operation, we did not perform
J Turk Acad Dermatol 2010; 4 (1): 04101c. http://www.jotad.org/2010/1/jtad04102c.pdf
Page 3 of 4(page number not for citation purposes)
Figure 4. The appearance of the patient four anda half months following the operation. Her facial edema
has decreased in intensity by 90% and she hasalso gained 5 kilos.

any biochemical analysis. Afterwards, wehave clinically concluded that none of thesepeptides could cause this clinical picture inour patient so as none of them are known tocause edema. However, the possibility of neu-ropeptide Y, causing vasoconstruction, couldbe an etiologic factor for edema remained.
In conclusion, we present a case of aretroperitoneal PGL with chronic facial andupper extremity edema. The edema decreasedin intensity by about 90% within one monthafter operation. The chronic facial and upperextremity edema was thought to be a parane-oplastic phenomenon in the presented case.
Acknowledgements
This manuscript was poster presented in the “22.National Dermatology Congress, 14-18 October2008, Konya, Turkey”; We gratefully thank to Fuat
Atalay, Nesrin Turhan, Hüseyin Üstün and HasanMete Aksoy for their great contribution.
References
1. Litvyakova LI, Bellanti JA. Orofacial edema: a diagnos-tic and therapeutic challenge for the clinician. Ann Al-lergy Asthma Immunol 2000; 84: 188-92. PMID:10719775
2. Dragan LR, Baron JM, Stern S, Shaw JC. Solid facialedema preceding a diagnosis of retro-orbital B-celllymphoma. J Am Acad Dermatol 2000; 42(5 Pt 2):872-874. PMID: 10767691
3. Nadruz W Jr, Carvalheira JBC, Brenelli SL. A man
with chronic facial swelling. Lancet 2000; 355: 1516.
PMID: 10801174
4. Karagiannis A, Mikhailidis DP, Athyros VG, HarsoulisF. Pheochromocytoma: an update on genetics and ma-nagement. Endocrine-Related Cancer 2007; 14: 935-956. PMID: 18045948
J Turk Acad Dermatol 2010; 4 (1): 04102c. http://www.jotad.org/2010/1/jtad94102c.pdf
Page 4 of 4(page number not for citation purposes)