Embed Size (px)
Citation preview
Parent-Child Interaction Parent-Child Interaction Therapy (PCIT) with Therapy (PCIT) with
Puerto Rican families Puerto Rican families
Maribel Matos-Román, Ph.D.University of Puerto Rico
PCIT ConferenceJanuary 26-28, 2006
Gainesville, FL
Specific AimsSpecific Aims
To revise and culturally adapt PCIT for Puerto Rican preschool aged children with a diagnosis of ADHD who also present high rates of behavior problems.
To conduct a randomized controlled pilot study to evaluate the initial efficacy, feasibility, and acceptability of the refined PCIT for children with a diagnosis of ADHD and problem behaviors and their families.
Inclusion criteriaInclusion criteria 4 to 6 years – 11 months of age Parent complaints of significant
hyperactivity and behavior problems No evidence of neurological, pervasive
developmental disorders or significant handicaps
Be a child of a Puerto Rican mother No treatment with stimulant or
psychotropic medication No involvement in other forms of child
psychotherapy and/or pharmacotherapy
Inclusion criteriaInclusion criteria
IQ > 80 (PPVT) ADHD diagnosis, Combined or
Hyperactive-Impulsive Type - NIMH DISC-IV.
A score above the 93rd percentile on hyperactivity and ODD or aggression scales (DBRS or BASC)
Absence of domestic violence and chaotic family environment
No indicators of severe psychopathology on parents
Aim 1Aim 1 Translation of the PCIT manual and
handouts Linguistic adaptations Psychoeducational module about ADHD
and behavior problems– Description of hyperactivity and its
relationship to behavior problems
– Associated difficulties
– Risks and protective factors
– Possible etiologies
– Treatment options
Aim 1Aim 1 Nine families
– 9 children 7 M and 2 F; Mean age: 4.9 years; Mean IQ:
104.4, SD = 10.08
– 9 mothers 2 single parents, Mean age: 31.89, SD =
6.31 Range: 25 to 43
Education: 15.6 years (nearly a BA, SD =
1.59; Range: 14 to 19)
7 worked full-time, 1 part-time, 1 college
student
Aim 1Aim 1 Nine families
– 7 fathers (1 stepfather)
Mean age: 32.86, SD = 5.34 Range: 27 to
43
Education: 16.0 years (BA, SD = 3.79;
Range: 12 to 23
Full-time jobs
Aim 1Aim 1Procedures
– Screening and outcome measures (Pre-treatment assessment)
– Psychoeducational sessions (2 sessions)
– CDI and PDI Mean CDI sessions = 7.47 (6 - 9)
Mean PDI sessions= 7.79 (6 - 10)
– Post treatment assessment
– 3-month follow-up assessment
Screening MeasuresScreening Measures Disruptive Behavior Scale for Children
(DBRS)– 9 hyperactivity symptoms, 8 ODD symptoms
Behavioral Assessment System for Children-Parent Rating Scales (BASC-PRS)– Subscales of Hyperactivity and Aggression
Peabody Picture Vocabulary Test (PPVT-HAA)
NIMH DISC IV - Parent Version – ADHD, ODD, generalized anxiety disorder,
separation anxiety disorder, major depression, and disthymia modules
Outcome MeasuresOutcome Measures Eyberg Child Behavior Inventory (ECBI) Child Behavior Checklist (CBCL) BASC, DBRS Home Situations Questionnaire (HSQ) Family Experiences Inventory (FEI) Parent Practices Inventory (PPI) Beck Depression Inventory (BDI) Symptom Checklist – 36 (SCL-36) Treatment and Evaluation Survey (TES) Therapy Attitude Inventory (TAI)
ResultsResults
PCIT feasible to implement and acceptable
High level of satisfaction
– Mean TAI score: 48.67, SD=1.32
– Mothers’ reports of being felt understood,
confident, comfortable, and supported by their
therapists.
Positive changes in children’s behavior
Reduction in family stress
Improvement in parent-child relationships
ResultsResults
Treatment gains maintained through 3-
month follow-up
Reliable change index (RCI)
– 89% in ECBI-Intensity and the ECBI-
Problem
– 62% in ADHD-Hyperactivity
– 88% in ODD
– 56% in the PPI
– 78% in the FEI
ModificationsModifications
8 sessions for CDI and 9 for PDI
Handout about pharmacological treatment for ADHD
Modification of time-out procedures – Loss of privileges
– Definition of silence
– Duration of time-out
Scripts for CDI and PDI
Aim 2 – Pilot StudyAim 2 – Pilot Study
32 families– Treatment group (TG); n=20– Wait-list group (WL); n= 12
No difference between groups – gender distribution– age– IQ– parents’ education– children’s impairment in adaptive
functioning– screening ratings of hyperactivity and
aggressive or ODD behaviors
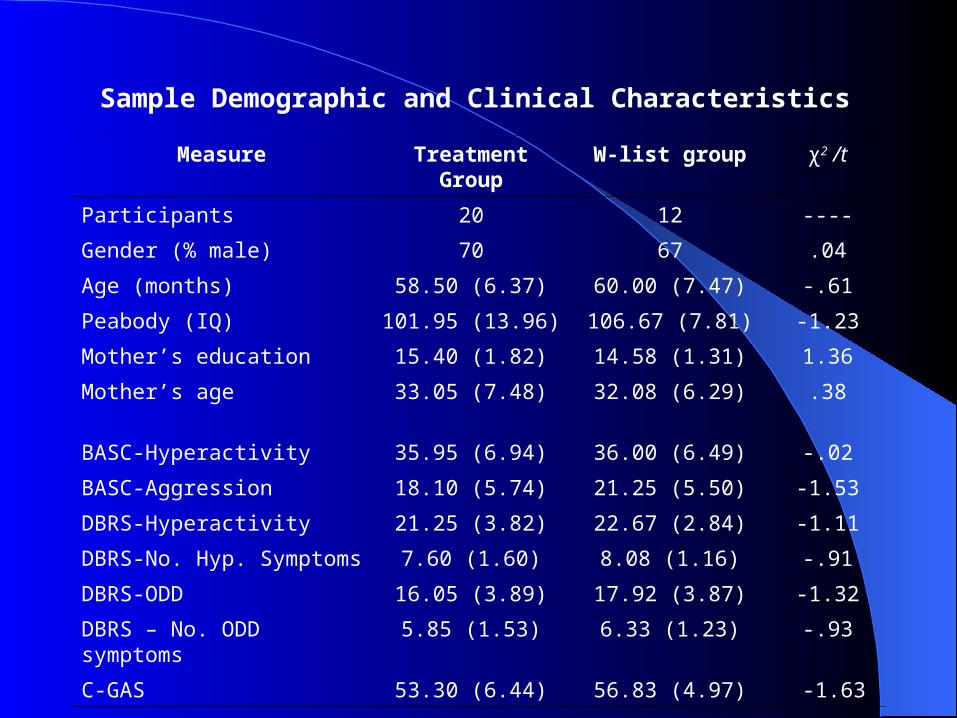
Measure Treatment Group
W-list group χ2 /t
Participants 20 12 ----
Gender (% male) 70 67 .04
Age (months) 58.50 (6.37) 60.00 (7.47) -.61
Peabody (IQ) 101.95 (13.96) 106.67 (7.81) -1.23
Mother’s education 15.40 (1.82) 14.58 (1.31) 1.36
Mother’s age 33.05 (7.48) 32.08 (6.29) .38
BASC-Hyperactivity 35.95 (6.94) 36.00 (6.49) -.02
BASC-Aggression 18.10 (5.74) 21.25 (5.50) -1.53
DBRS-Hyperactivity 21.25 (3.82) 22.67 (2.84) -1.11
DBRS-No. Hyp. Symptoms 7.60 (1.60) 8.08 (1.16) -.91
DBRS-ODD 16.05 (3.89) 17.92 (3.87) -1.32
DBRS – No. ODD symptoms
5.85 (1.53) 6.33 (1.23) -.93
C-GAS 53.30 (6.44) 56.83 (4.97) -1.63
Sample Demographic and Clinical Characteristics
Results – Pilot StudyResults – Pilot Study
Treatment Group (n=19)– Lower levels of hyperactivity
– Less aggressive and ODD behaviors
– Less externalizing behaviors
– Significant reduction in general behavioral problems (ECBI)
– Significant reduction in the behaviors they assessed as problematic (ECBI-Problems)
Results – Pilot StudyResults – Pilot Study– Reduction in the parenting stress
(FEI)
– Use of adequate parenting practices
– Mean CDI sessions: 7 (6 to 9)
– Mean PDI sessions: 8 (6 to 10)
– High level of consumer satisfaction Mean TAI scores: 47.77 (SD: 2.93)
Wait-list Group (n= 12)– No significant changes in any measure
ANCOVAs with pretreatment scores as covariates.
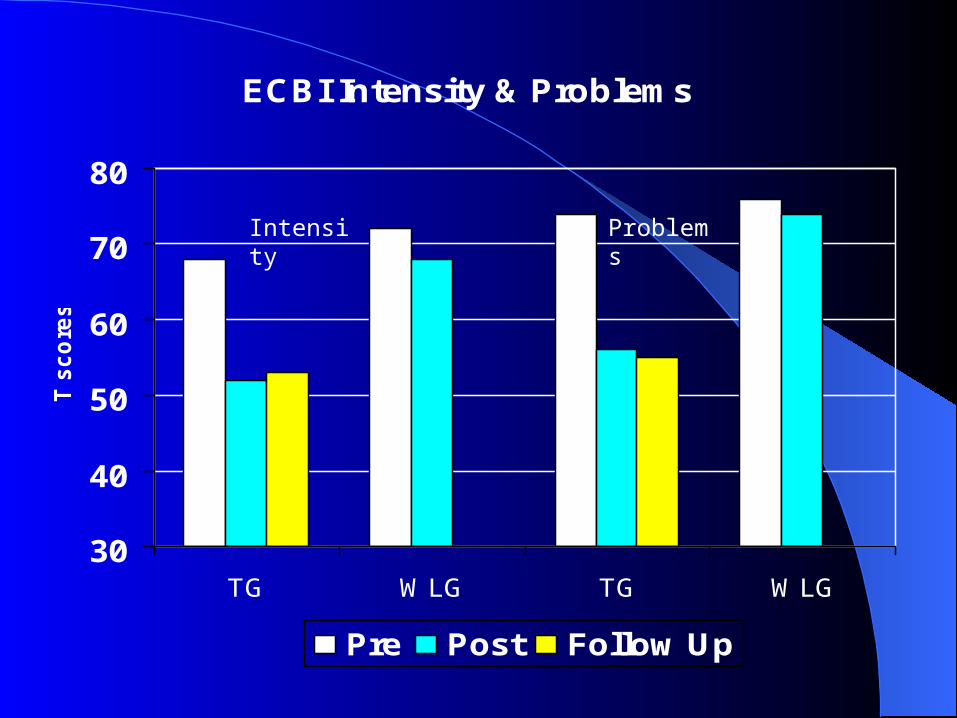
ECBI Intensity & Problems
30
40
50
60
70
80
TG WLG TG WLG
T s
co
res
Pre Post Follow Up
Intensity Problems

BASC Hyperactivity & Aggression
0
5
10
15
20
25
30
35
40
TG WLG TG WLG
Ra
w s
co
res
Pre Post Follow Up
Hyperactivity
Aggression
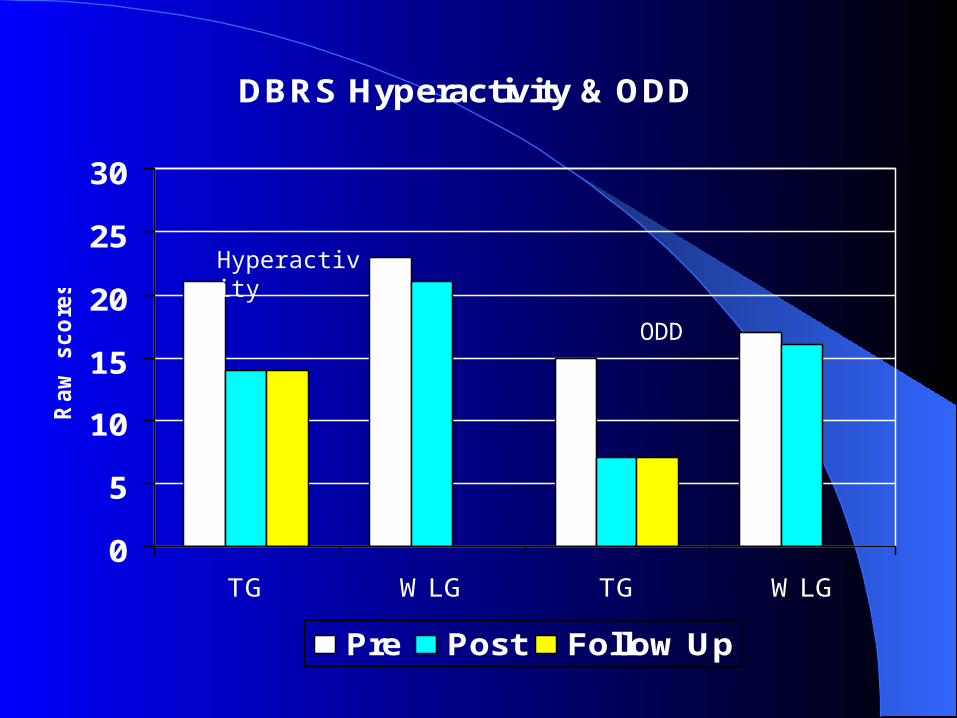
DBRS Hyperactivity & ODD
0
5
10
15
20
25
30
TG WLG TG WLG
Ra
w s
co
res
Pre Post Follow Up
Hyperactivity
ODD
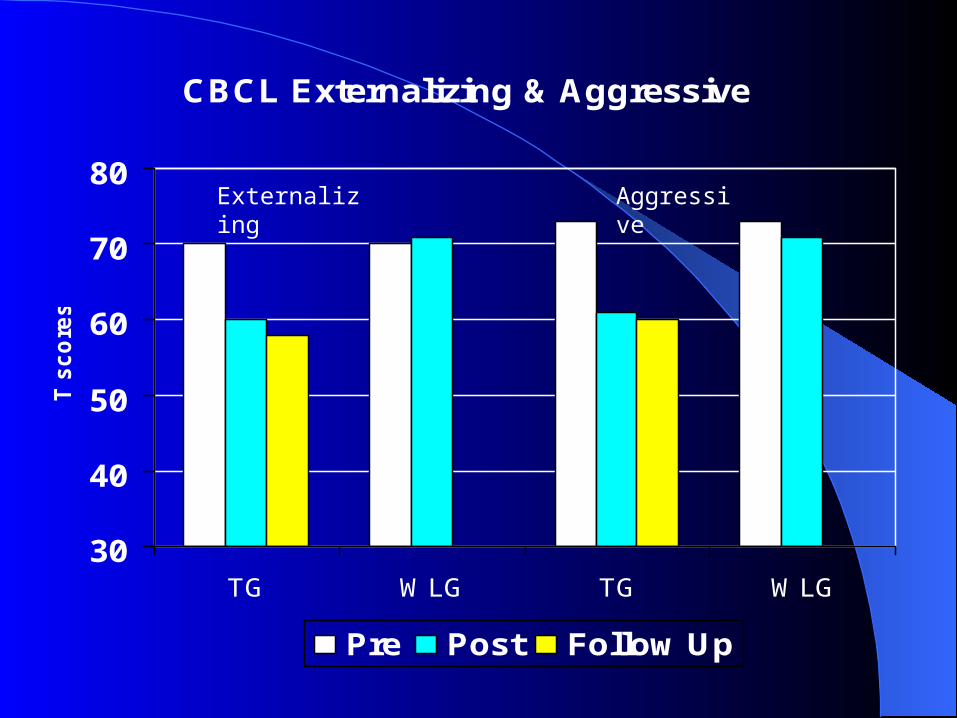
CBCL Externalizing & Aggressive
30
40
50
60
70
80
TG WLG TG WLG
T s
co
res
Pre Post Follow Up
Externalizing Aggressive
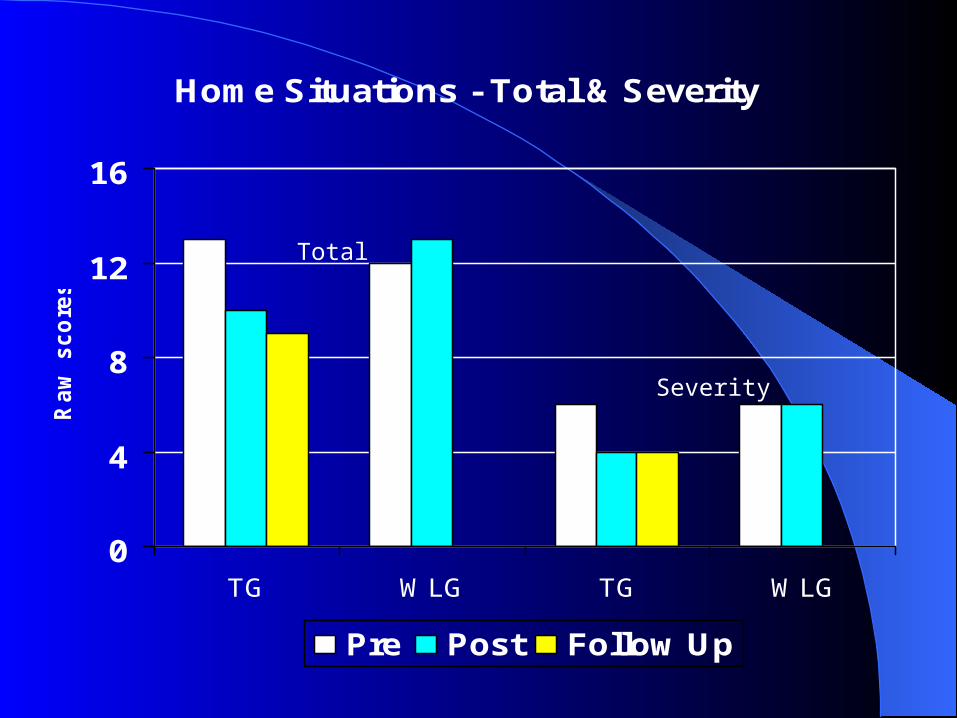
Home Situations - Total & Severity
0
4
8
12
16
TG WLG TG WLG
Ra
w s
co
res
Pre Post Follow Up
Total
Severity
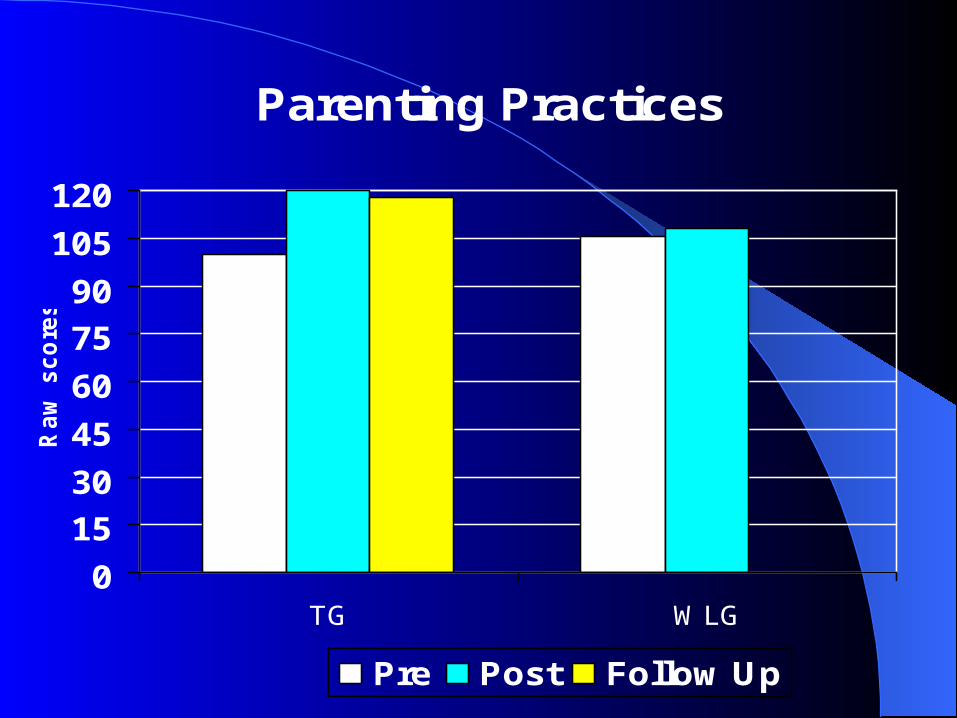
Parenting Practices
0
15
30
45
60
75
90
105
120
TG WLG
Ra
w s
co
res
Pre Post Follow Up
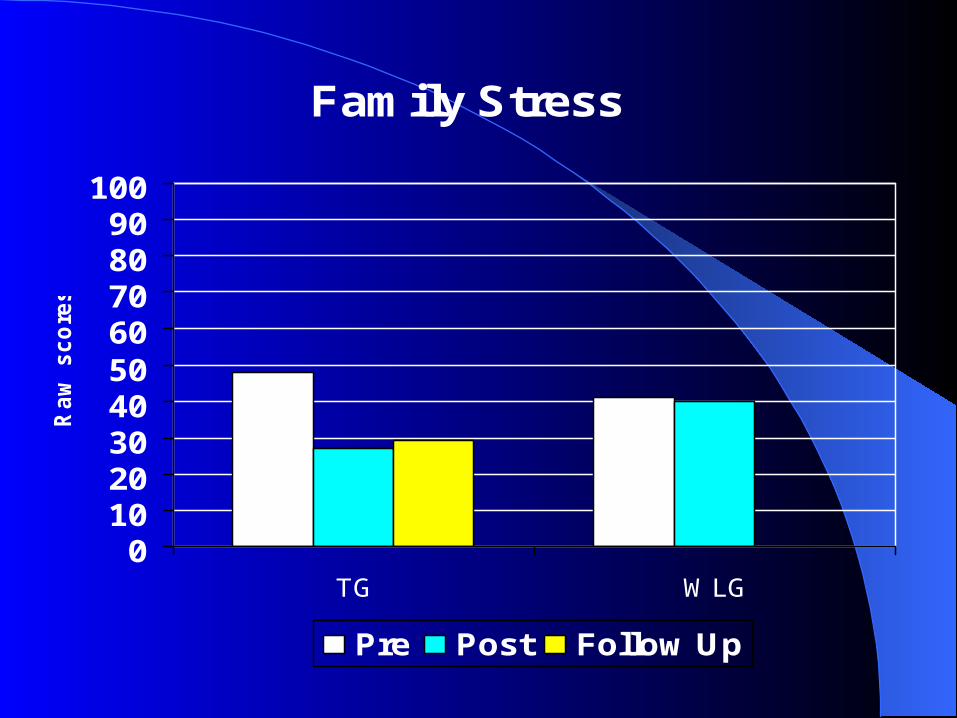
Family Stress
0102030405060708090
100
TG WLG
Ra
w s
co
res
Pre Post Follow Up
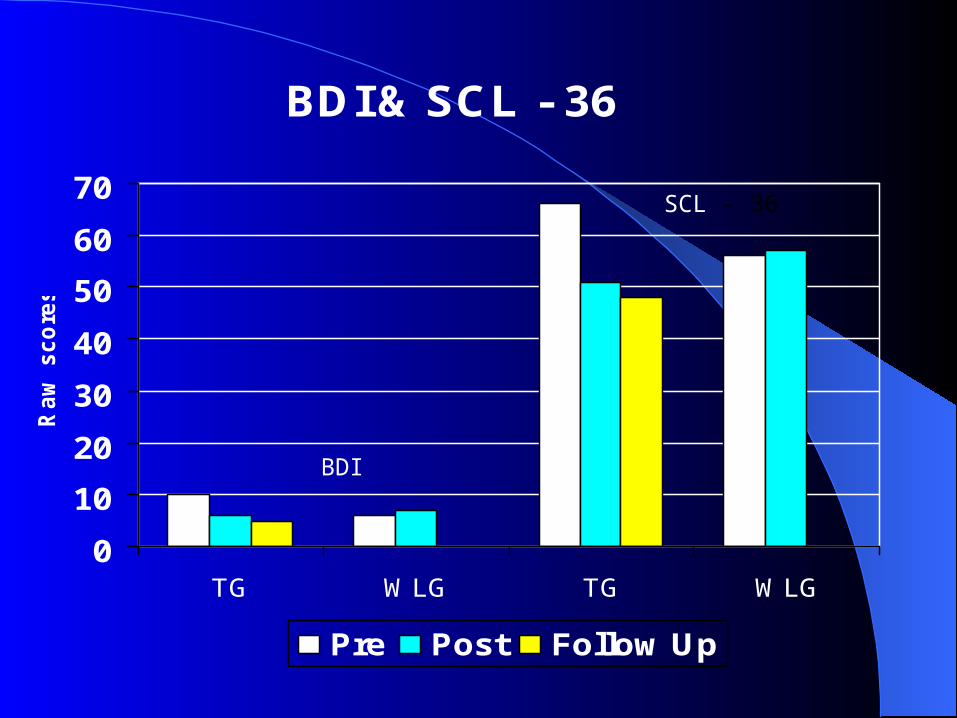
BDI & SCL - 36
0
10
20
30
40
50
60
70
TG WLG TG WLG
Ra
w s
co
res
Pre Post Follow Up
BDI
SCL - 36
ConclusionsConclusions
PCIT seems to be:
– A responsive family intervention for Puerto Rican families who have preschool- age children with significant behavior problems.
– An acceptable and effective treatment for Puerto Rican parents.
– Efficacious to reduce significantly the behavior problems associated with ADHD and ODD.
.
Research TeamResearch Team
Co-investigators– José J. Bauermeister, Ph.D.– Guillermo Bernal, Ph.D.
Data Analysis– José V. Martínez, Ph.D.– Eduardo Cumba, Ph.D.
Research AssistantsGraduate students•Rosalie Torres•Rocheli Santiago•Ixa Rodriguez•Liliana Torres•Michelle Jurado•Elisabet Avilés•Kenneth Junco
Undergraduate students•Marisol De Jesús•Damaris Cordero•Wilmarie Ríos•Arlene Román
AcknowledgmentsAcknowledgments
Funded by NIMH 5R24MH-49368-11
Dr. Maribel Matos E-mail: [email protected]

¡Gracias!¡Gracias!





























