Embed Size (px)
Citation preview

1
Parkinson’s Disease: what it is and how it is
managed.
An Allied Health Education Webinar
Chad Swank, PT, PhD, [email protected]
Objectives1) Discuss the pathology of Parkinson's disease.
2) Discuss the pharmacological and surgical management of people with PD.
3) Develop suitable physical therapy intervention strategy for people with PD.
Outline• Background
• Pathology of PD
• Medical Management of PD
• PT Management of PD
• Future Directions in PD

2
Background
Incidence of PD• 1 to 1.5 million cases in the US
o 60,000 new cases each year
• Typically develops after age 65
• Affects men and women equally
• No social, ethnic, economic boundaries
• More prevalent in industrial countries
PD facts:
• Direct and indirect costs associated with PD exceed $20 billion annually in United States(Weintraub et al., 2008)
o individual costs are 3.3 times higher for
people with PD with cognitive dysfunction (Vossius et al., 2011)
• With aging population, burden of PD continues to increase
o Number of PD cases in individuals ≥50 years predicted to reach 8.7 million worldwide in next 25 years (Dorsey et al., 2007)

3
Implications of PD
• People with Parkinson Disease are 5 times more likely to fall
• 70% of people fall more than once per year
• Within 10 years, 25% of people with PD will have a fractured hip
• Hip fractures constitute 47% of total fractures
Pathology of Parkinson’s Disease
PD - Video• PD - Video
• What do you notice about the person’s posture, gait, overall mobility?

4
What is PD?• Chronic, progressive, neurologic disorder
o Characterized by motor and nonmotor symptoms
o Pathogenesis involves degeneration of dopaminergicneurons in substantia nigra decreasing binding sites for DA.
Types:
• Idiopathic PD
o Most common (78%)
o Late-onset (> 40 yrs)
o Early-onset/ young-onset (< 40)
4-40%
• Secondary PD
o Caused by toxins
• Parkinson’s Plus Syndromeso Neurodegenerative diseases that cause PD-like symptoms
Basal Ganglia Anatomy
Input
Output •Maintains “readiness”•Modulates spacial orientation-time-force-tone•Cognitive, perceptual emotional, motivation (caudate nucleus)•Planning and programming movement through selection and inhibition of specific motor synergies
Substantia Nigra & the Extrapyramidal System

5
Dopamine synthesis
Dopamine pathways in human brain
Motor Features of PD
Resting tremor1,2
• 70% of patients
• “Pill-rolling” tremor in hands• Can involve lips, chin, jaw, legs
Bradykinesia1,3,4• 80-90% of patients
• Most disabling symptom of PD
Rigidity1,4
• >90% of patients
• “Cogwheel” (fluctuating) or “lead pipe” (continuous)
Postural instability1
• Indicative of advanced-stage PD
• Frequent cause of fallsPD, Parkinson’s disease.1. Jankovic. J Neurol Neurosurg Psychiatry. 2008;79(4):368-376. 2. Bhidayasiri. Postgrad Med J. 2005;81(962):756-762. 3. Berardelli et al. Brain. 2001;124(pt 111):2131-2146. 4. Weintraub et al. Am J Manag Care. 2008;14(2 suppl):S40-S48.

6
Balance &
Falls

7
Nonmotor Features of PDPsychiatric disorders1
• Depression in up to 40% of patients
• Anxiety in ~30% of patients
Cognitive disorders1,2
• Mild cognitive impairment
• Dementia in 15-40% of patients
Sleep abnormalities1,3• >70% of patients
• REM sleep behavior disorder
Autonomic dysfunction1-3
• Constipation
• Orthostatic hypotension
Sensory3 • Olfactory dysfunction
Miscellaneous1,2 • Fatigue and weight loss
PD, Parkinson’s disease; REM, rapid eye movement.1. Thanvi et al. Postgrad Med J. 2003;79(936):561-565. 2. Fahn and Sulzer. NeuroRx. 2004;1(1):139-154. 3. Jankovic. J Neurol Neurosurg Psychiatry. 2008;79(4):368-376.
Differential Diagnosis
• Idiopathic PDo No atypical sign
o No resistance to L-dopa in first 5 years of treatment
• Parkinsonism Syndromeso More symmetricalo Rapid progression (HY 3 in 3
years) o Early falls
o Earlier axial involvement
o Associated signs:• Oculomotor disorders• Pyramidal signs
• Cerebellar syndromes• Apraxia• Seizures• Early cognitive impairment• Dysautonomia

8
• Idiopathic PDo Most common at 65%o 2nd cause of motor disability after stroke
• Progressive Supranuclear Palsy (PSP)o 5% of parkinsonism syndromeso Dx made after 3 years; mean survival = 6 years
• Multiple System Atrophy (MSA)o 10% of parkisonism syndromes; mean survival = 9 yearso Atypical progressive presentation
• Corticobasal Degeneration (CBD)o 1% prevelance; onset in 6th decade
• Dementia with Lewy Bodies (DLB)o Combo of cognitive disorders, hallucinations & falls
Prevalence
UK brain bank criteria to Diagnose PD
I: Is Bradykinesia (slowness of movement) present?II: Are two of the below present?
___ Rigidity (Stiffness in arms, leg, or neck)___ 4-6 Hertz resting tremor___ Postural instability not caused by primary visual,
vestibular, cerebellar, proprioceptive dysfunctionIII: Are at least 3 of the below present?
___ Unilateral onset___ Rest tremor present___ Progressive disorder___ Persistent asymmetry affecting side of onset most___ Excellent response (70-100%) to levodopa
___ Severe levodopa induced dyskinesia___ Levodopa response for 5 years or more___ Clinical course of 5 years or more
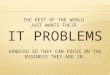
FMT-PET images of a healthy individual and PD patients. FMT uptake declines asymmetrically in the early stages, mostly in the posterior putamen.
FMT-PET (6-[18F]fluoro-L-m-tyrosine)
Asari et al. BMC Neurology 2011, 11:35

9
National Parkinson’s Association: An update on DAT Scanning for Parkinson’s Disease Diagnosis April 2014
DaTscan
Measures of Severity in PD
Hoehn & Yahr Stages of PD
• Stage I: unilateral
• Stage II: bilateral without impaired balance
• Stage III: bilateral - recovery on pull test
• Stage IV: highly disabled; can still walk
• Stage V: totally disabled

10
Modified Hoehn and Yahr Staging for Parkinson’s Stage 0 No signs of disease
Stage 1 Unilateral disease
Stage 1.5 Unilateral plus axial involvement
Stage 2 Bilateral disease, without impairment of balance
Stage 2.5 Mild bilateral disease, with recovery on pull test
Stage 3 Mild to moderate bilateral disease; some postural
instability; physically independent
Stage 4 Severe disability; still able to walk or stand unassisted
Stage 5 Wheelchair bound or bedridden unless aided
UPDRS
• Unified Parkinson’s Disease Rating Scale• Developed by an international group of
neurologists
o UPDRS
- Mentation
- ADL’s, medical complications
- Motor impairment
- Modified HY scale
- Schwab and England ADL Scale
• Interrater reliability: r = 0.8
• Part III correlates well with the HY (r = 0.8)
• Part III can be converted to an HY stage
Parkinson Disease QuestionnairePDQ-39
• 39 questions• 8 aspects of QOL
o Mobilityo Activities of daily livingo Emotionso Stigmao Social supporto Cognitiono Communicationo Bodily discomfort
• Cronbach’s alpha 0.72–0.95
• Test–retest 0.76–0.93
Hagell & Nygren 2007
PDQ-8
• 8 questions• Relates with PDQ-39
o Pearson's r=0.96, ICC=0.95
Tan et al 2004

11
Medical Management of Parkinson’s Disease
Use of levodopa
Late 1950s: L-dihydroxyphenylalanine (L-DOPA; levodopa),
a precursor of dopamine that crosses the blood-brain barrier,
could restore brain dopamine levels and motor functions in
animals treated with catecholamine depleting drug
(reserpine)
First treatment attempts in PD patients with levodopa
resulted in dramatic but short-term improvements; took years
before it became an established and successful treatment
Still today, levodopa cornerstone of PD treatment; virtually
all patients benefit
Limitations of levodopa
Efficacy tends to decrease as the disease progresses
Chronic treatment associated with adverse events
(motor fluctuations, dyskinesias and
neuropsychiatric problems)

12
Pharmacologic Therapies for PD
Pharmacological Management o Levodopa (L-dopa) – act on D1 receptor
• For motor disability
• Sinemet, Parcopa, Sinemet CR, Stalevo
o Dopamine agonist – act on D2 receptor• Stimulates DA receptors
• Lessens motor complications
• May delay use of levadopa
• Miripex, Requip
o MAO-B Inhibitors• Selegiline, Azilect
o COMT-inhibitors• taken with levodopa that can help levodopa work longer and better
• Comtan, Tasmar
o Anticholinergics• Artane, Cogentin
o Others• Amantadine
Side Effects: dyskinesias, nausea, orthostatic hypotension, confusion, hallucinations, headache, agitation, psychosis.
Surgical Treatment
• Deep Brain Stimulation (DBS)o Thalamic (Vim DBS): reduces tremor
o Pallidal (GPi DBS): reduces tremor, rigidity, bradykinesia, and gait disorder
o Subthalamic nucleus (STN DBS): reduces tremor, rigidity, bradykinesia, and gait disorder

13
Physical Therapy Management of Parkinson’s
Disease
Intervention Framework
Parkinson’s Disease
Indirect Impairments
-Musculoskeletal
-CardiovascularDirect Impairments-Rigidity
-Tremor
-Bradykinesia
-Postural Instability Disability
-Decreased mobility
-Decreased quality of life
-Decreased ADL’s
Medicine
Rehabilitation
What is the Evidence?
• Patients with Parkinson’s disease benefit from PT in addition to standard medications. de Goede et al. Arch Phys Med Rehabil
2001
• Current literature suggests benefits of physical intervention, but results are not conclusive. Deane KHO et al,
Cochrane Review, 2001
• Exercise, treadmill training, balance training, cued activities probably effective to improve functional
outcomes, but results not lasting. Suchowersky et al, Neurology 2006
• PT unlikely to influence disease itself but can improve daily functioning and may influence secondary health problems. Keus et al. Movement Disorders 2007.

14
Limitations To Current Evidence
• Most studies are for individuals in earlier stages of PD
• Little evidence exists regarding the best approach for individuals later in the disease
• Recruitment for these studies can be a challenge due to the progressive nature of the disease.
Given the Current Evidence ...
• For which patients is physical intervention appropriate?
• How should the intervention be structured?
• Should the intervention be tailored differently for patients in different stages of PD?
• What results should be expected from physical intervention and in each stage?
Theoretical Framework Across Continuum
Disease Stage
Evaluation Findings
Intervention Strategies
Additional Roles and
Interventions
Early Stage Middle Stage Late Stage
•Minimal impairments•Minimal activity
limitations•No participation restrictions
•Increasing severity of impairments
•Min/Mod activity limitations
•Min/Mod participation
restrictions
•Severe impairments•Severe activity
limitations•Severe participation restrictions
1. Preventative2. Restorative
3. Compensatory?
1. Compensatory2. Preventative
3. Restorative?
1. Compensatory2. Preventative
Patient/family/caregiver training and educationPsychological support
Referral to other health care professionals

15
Early Stage Physical Therapy Interventions
Benefits of Exercise• 2 years of supervised and structured exercise is
effective at improving functional performance outcomes in individuals with moderate PD (Prodoehl et al., 2015)
o Clinicians should include structured and supervised exercise in the long-term plan of care for individuals with PD.
• PRE can significantly improve muscle size, muscle strength, muscle endurance, and neuromuscular function and can significantly impact bradykinesia, postural instability, and patient-perceived quality of life (David et al., 2012)

16
Benefits of Exercise• Intensive rehabilitation might slow down the
progression of motor decay, delaying the need for increasing drug treatment demonstrating a possible
neuroprotective effect (Frazzitta et al., 2015)
Agility Program
Boxing Video
http://www.punchingoutparkinsons.org/

17
Middle Stage Physical Therapy Interventions
Treadmill Training for Gait
• Miya et al. 2000o Results: Significantly improved UPDRS total & # steps for BWSTT
• Skidmore et al 2008
o Precautions must be taken to prevent falls & monitor blood pressure instability during exercise
o Treadmill training is feasible, may reduce
symptom severity, & improve fitness.
Cycling
• Man with bicycle
• Comparing the effects of voluntary exercise (VE)
and forced exercise (FE) on PD symptoms, motor function, and bimanual dexterity
o Aerobic fitness improved in PD patients following both VE and FE interventions.
o Only FE resulted in improvements of motor function and bimanual dexterity.
o FE may lead to a shift in motor control strategy, from
feedback to a greater reliance on feedforward processes, suggesting FE may be altering central motor control processes.

18
ALBERTS, J.L., S.M. LINDER, A.L. PENKO, M.J. LOWE, and M. PHILLIPS. It is not about the bike, it is about the pedaling: forced exercise and parkinson’sdisease.
Exerc. Sport Sci. Rev., Vol. 39, No. 4, pp. 177Y186, 2011.
Training BIGoAmplitude of movement important
o Intensity of training
oUses auditory & cognitive cuing
External Cues• External cues are effective for improving the
gait parameters and psychomotor performance of PD patients (Rocha et al., 2014)
• Types of cues:o Visual
o Auditory
o Sensorial
o Cognitive

19
Examples of Cueing• Proprioceptive - practice recognizing limb positions with eyes
closed
• Somatosensory – tactile or vibratory
• Cognitive
o Mental simulation
o Rehearsal of movement
• Visual
o Feedback regarding body position using mirrors
o Lines drawn on the floor
o Flashing lights, targets
• Auditory
o Rhythmic acoustic feedback
o Music
o Metronome
Functional Tips/Tricks
• EPDA | COPING STRATEGIES
http://epda.eu.com/copingstrategies/en/category.htm
Example - Getting Up From A Seated Position
• Consider starting position
• Determine efficient strategy
– Use of arms
– To rock or not?
– Counting
• Modify environment
– Chair with higher seat
– Lift chairs
– Chair with handles

20
Late Stage Physical Therapy Interventions
Clinical Decisions
• As patients approach later stages of PDo Emphasis shifts from
• correction to compensation
• Patient, family, and care-giver training
o Preventive strategies should be incorporated to minimize sequelae (e.g., hip fracture, pneumonia)
o The role of the caregiver is critical• training for caregiver
• impact on the caregiver should be considered
• strategies should be included to assist the caregiver to meet his/her own needs.
PD-specific Assistive Devices• Things to consider
o Need to address variety of functional l imitations
o Need to be practical!
• 2 references: o Assistive devices alter gait patterns in Parkinson disease: Advantages of the
four-wheeled walker. Kegelmeyer, et al., Gait & Posture 38 (2013) 20-24
o A review of assistive technologies for people with Parkinson’s disease. Cunningham et al., Technology and Health Care 17 (2009) 269-279.

21
Measures of Function in PD
NeuroEDGE PD
• http://www.neuropt.org/professional-resources/neurology-section-outcome-measures-recommendations/parkinson-disease
Future Directions in Parkinson’s Disease

22
Case Example• A 78-year-old man presented with a 15-year
history of chronic constipation. At age 68, he experienced a near complete loss of his
sense of smell. Recently, he has developed an unusual sleep disorder, characterized by
abrupt and at times combative behavior during the night that has resulted in injury to
his spouse on two separate occasions; he is referred to a sleep disorders clinic.

23
Pharmacological Approach
• Levodopa/carbidopa intestinal gel (LCIG, marketed as Duodopa®)o developed to minimize the fluctuation in levodopa plasma levels
seen in oral administration by providing a continuous influx of
steady levels of levodopa
o personal pump directly administers the LCIG into the duodenum,
the main site of intestinal absorption
• Proposed benefits include a significant “off” time reduction and dyskinesia along with a
significant improvement in gait disorders and quality of life
Non-invasive Brain Stimulation
Community Based Exercise Programs
• Development of collaborative interventions (i.e. people with PD, physicians, caregivers, researchers) to manage PD

24
Resources for PDNational Parkinson Foundation (www.parkinson.org)
American Parkinson Disease Association
(www.apdaparkinson.org)
Davis Phinney Foundation (www.davisphinneyfoundation.org)
Michael J. Fox Foundation (www.michaeljfox.org)
Parkinson’s Disease Foundation (www.pdf.org)
• Know your community resources!o support groups for patient and family, free exercise classes, information sessions,
respite care, and other organizations involved within caring for this population in your area.
http://www.youtube.com/watch?v=pL_LZgAEsnM