Embed Size (px)
Citation preview
Pars Plicata Lensectomy and Vitrectomy in the Management of Congenital Cataracts GHOLAM A. PEYMAN, MD,* MOTILAL RAICHAND, MD,t CAROLYN OESTERLE, MD,* MORTON F. GOLDBERG, MD*
Abstract: Thirty-two eyes with congenital cataracts were surgically managed by pars plicata lensectomy and vitrectomy. All eyes have maintained clear media without pupillary membranes; no detached retina or cases of pupillary block have occurred during a follow-up period of up to 72 months. [Key words: congenital cataracts, lensectomy, pars plicata, vitrectomy.] Ophthalmology 88:437-439, 1981.
A major cause of blindness in childhood is congenital cataracts. 1
-3 Research in genetics, biochemistry,
and infectious disease has expanded our understanding of various etiologic possibilities. However, the management of congenital cataracts, such as the timing of surgical intervention, the type of surgical procedure, and the management of amblyopia, is still a challenge.
Previously, we presented our short-term experience with pars plicata lensectomy in the management of congenital cataracts in 18 eyes. 4 The purpose of this paper is to describe our surgical technique and to report on the long-term follow-up of our patients.
MATERIALS AND METHODS
Twenty-five patients (32 eyes) were referred to the Vitreous Service of the University of Illinois Hospital Eye and Ear Infirmary between 1974 and early 1980 (Table 1). In seven patients, bilaterallensectomy and
From the Department of Ophthalmology,* University of Illinois Hospital Eye and Ear Infirmary, and Cook County Hospital,t Chicago.
Presented at the Eighty-Fifth Annual Meeting of the American Academy of Ophthalmology, Chicago, November 2-7, 1980.
Supported in part by core grant 1 P30EY01792 from the National Institutes of Health, Bethesda; Research to Prevent Blindness, Inc., New York; and the Illinois Society for the Prevention of Blindness, Chicago.
Reprint requests to Gholam A. Peyman, MD, University of Illinois Hospital Eye and Ear Infirmary, 1855 W Taylor St, Chicago, IL 60612.
0161-6420/8110500/0437/$00.65 © American Academy of Ophthalmology
vitrectomy were performed; in the remainder, only one eye was treated with this technique.
Patients ranged in age from 1 month to 16 years. Two patients were twins. All but two patients had bilateral cataracts. In eight patients, the cataract could be attributed to maternal infection with rubella. In two patients, the family history suggested autosomal dominant inheritance. In the remainder, the cause could not be determined with certainty. In all eyes, a combined lensectomy and vitrectomy was performed with the vitrophage.
In addition to cataracts, many patients had other systemic problems. Five had heart disease that involved the valve of the pulmonary and/or aortic trees; one had Down's syndrome; four had mental retardation; and three had seizure disorders. Other associated findings were hypertension, eosinophilia, brachycephaly, and atropic dermatitis. Additional ocular findings included nystagmus, aniridia, microcornea, and esotropia.
Prior to surgery, both eyes were examined for corneal size, intraocular pressure, and clarity of ocular media. When possible, the fundus was examined with an indirect ophthalmoscope. All patients were operated on under general anesthesia.
PROCEDURE
Following surgical preparation and draping, 4-0 black silk sutures are used to retract the eyelids. Bridle sutures are placed underneath the four rectus muscles. After adequate exposure is obtained, a limbal peritomy (usually in the infero temporal quadrant),
437
OPHTHALMOLOGY • MAY 1981 • VOLUME 88 • NUMBER 5
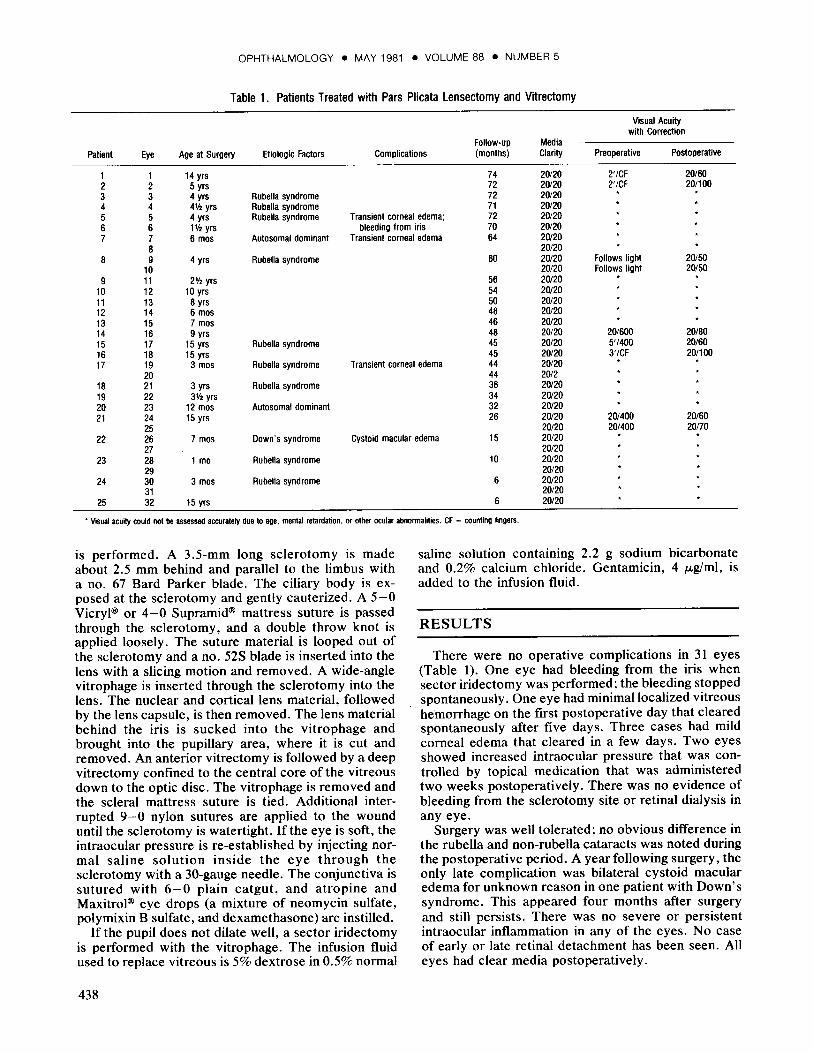
Table 1. Patients Treated with Pars Plicata Lensectomy and Vitrectomy
Follow-up Media
Visual Acuity with Correction
Patient Eye Age at Surgery Etiologic Factors Complications (months) Clarity Preoperative Postoperative
1 1 14 yrs 2 2 5 yrs 3 3 4 yrs 4 4 4'12 yrs
74 72
Rubella syndrome 72 Rubella syndrome 71
20/20 20/20 20/20 20/20
2'/CF 2'/CF
20/60 20/100
5 5 4 yrs Rubella syndrome Transient corneal edema; 72 20/20 6 6 1Y2 yrs bleeding from iris 70 20/20 7 7 6 mos Autosomal dominant Transient corneal edema 64 20/20
8 8 9 4 yrs
10 9 11 2V2 yrs
10 12 10 yrs 11 13 8 yrs 12 14 6 mos 13 15 7 mos 14 16 9 yrs 15 17 15 yrs 16 18 15 yrs
20/20 Rubella syndrome 60 20/20
20/20 56 20/20 54 20/20 50 20/20 48 20/20 46 20/20 48 20/20
Rubella syndrome 45 20/20 45 20/20
Follows light Follows light
*
20/600 5'/400 3'/CF
20/50 20/50
20/80 20/60 20/100
17 19 3 mos Rubella syndrome Transient corneal edema 44 20/20 * *
20 18 21 3 yrs 19 22 3'12 yrs 20 23 12 mos 21 24 15 yrs
25
44 Rubella syndrome 36
34 Autosomal dominant 32
26
20/2 20/20 20/20 20/20 20/20 20/20
20/400 20/400
20/60 20/70
22 26 7 mos Down's syndrome Cystoid macular edema 15 20/20 *
27 20/20 23 28 1 mo Rubella syndrome 10 20/20
29 20/20 24 30 3 mos Rubella syndrome 6 20/20
31 20/20 25 32 15 yrs 6 20/20
• Visual acuity could not be assessed accurately due to age, mental retardation, or other ocular abnormalities. CF = counting fingers.
is performed. A 3.5-mm long sclerotomy is made about 2.5 mm behind and parallel to the limbus with a no. 67 Bard Parker blade. The ciliary body is exposed at the sclerotomy and gently cauterized. A 5-0 Vicryl® or 4-0 Supramid® mattress suture is passed through the sclerotomy, and a double throw knot is applied loosely. The suture material is looped out of the sclerotomy and a no. 52S blade is inserted into the lens with a slicing motion and removed. A wide-angle vitrophage is inserted through the sclerotomy into the lens. The nuclear and cortical lens material, followed by the lens capsule, is then removed. The lens material behind the iris is sucked into the vitrophage and brought into the pupillary area, where it is cut and removed. An anterior vitrectomy is followed by a deep vitrectomy confined to the central core of the vitreous down to the optic disc. The vitrophage is removed and the scleral mattress suture is tied. Additional interrupted 9-0 nylon sutures are applied to the wound until the sclerotomy is watertight. If the eye is soft, the intraocular pressure is re-established by injecting normal saline solution inside the eye through the sclerotomy with a 30-gauge needle. The conjunctiva is sutured with 6-0 plain catgut, and atropine and Maxitrol® eye drops (a mixture of neomycin sulfate, polymixin B sulfate, and dexamethasone) are instilled.
If the pupil does not dilate well, a sector iridectomy is performed with the vitrophage. The infusion fluid used to replace vitreous is 5% dextrose in 0.5% normal
438
saline solution containing 2.2 g sodium bicarbonate and 0.2% calcium chloride. Gentamicin, 4 JLg/ml, is added to the infusion fluid.
RESULTS
There were no operative complications in 31 eyes (Table 1). One eye had bleeding from the iris when sector iridectomy was performed; the bleeding stopped spontaneously. One eye had minimal localized vitreous hemorrhage on the first postoperative day that cleared spontaneously after five days. Three cases had mild corneal edema that cleared in a few days. Two eyes showed increased intraocular pressure that was controlled by topical medication that was administered two weeks postoperatively. There was no evidence of bleeding from the sclerotomy site or retinal dialysis in any eye.
Surgery was well tolerated; no obvious difference in the rubella and non-rubella cataracts was noted during the postoperative period. A year following surgery, the only late complication was bilateral cystoid macular edema for unknown reason in one patient with Down's syndrome. This appeared four months after surgery and still persists. There was no severe or persistent intraocular inflammation in any of the eyes. No case of early or late retinal detachment has been seen. All eyes had clear media postoperatively.
PEYMAN, et al • CONGENITAL CATARACTS
Visual results were difficult to quantitate accurately in the majority of the patients because of amblyopia, nystagmus, or mental retardation, and age of the patients.
DISCUSSION
In the past, congenital cataracts have been managed by procedures such as simple discission,5- 7 which has an unacceptable rate of complications, such as lensinduced inflammation, glaucoma, and retinal detachment. Similarly, linear extraction8 has led to complications such as delayed formation of anterior chamber, occlusion of pupil, membrane formation, vitreous loss, and retinal detachment. 9 Although aspiration techniques have reduced some complications, 10- 12 vitreous loss and secondary membrane formation still continue to be problems. Phacoemulsification13 has greatly advanced the management of congenital cataracts; however, additional surgery for secondary membrane has been necessary in the majority of the cases. 14
•15
Two main approaches can be used with automated vitrectomy instruments for the management of congenital cataracts: one through the limbus16 and the other through the pars plicata. 4 We believe that the pars plicata approach has many advantages over other surgical techniques. We prefer the pars plicata to the pars plana because the pars plana is smaller in the young child than it is in the adult. Insertion of the vitrophage through the pars plicata allows for the maintenance of a safe distance from the vitreous base and ora serrata, thus reducing the chance of retinal dialysis. In addition, a large sclerotomy (3.5 mm) permits easy insertion of the vitrophage inside the eye, which eliminates unnecessary pressure on the ciliary body and prevents ciliary body detachment. Direct manipulation of the corneal endothelium is avoided. If lens particles or the nucleus fall accidentally into the vitreous, they can be visualized with the use of a fundus contact lens, and they can be retrieved with the vitrectomy instrument. Another advantage of the pars plicata approach is that the lens material can be easily removed in the axis of the instrument, whereas this is more difficult through the limbal approach. Any bleeding from the iris into the vitreous can be similarly dealt with. Cortical lens material behind the iris can be removed by applying suction alone. Removal of the anterior vitreous practically eliminates the chance of pupillary block.
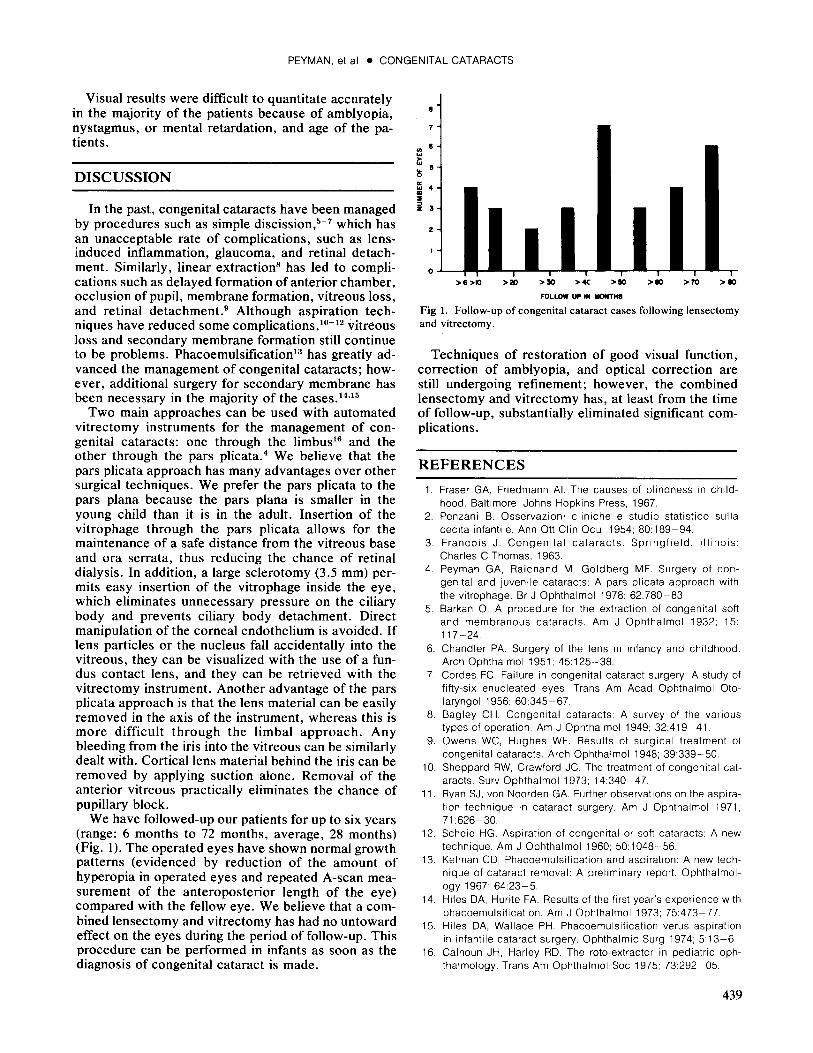
We have followed-up our patients for up to six years (range: 6 months to 72 months, average, 28 months) (Fig. 1). The operated eyes have shown normal growth patterns (evidenced by reduction of the amount of hyperopia in operated eyes and repeated A-scan measurement of the anteroposterior length of the eye) compared with the fellow eye. We believe that a combined lensectomy and vitrectomy has had no untoward effect on the eyes during the period of follow-up. This procedure can be performed in infants as soon as the diagnosis of congenital cataract is made.
8
7
"' "' 4 ID :II
i 3
0
>6>10 >20 >30 >4C >110 >110 >70 >110
FOLLOW UP IN -THS
Fig 1. Follow-up of congenital cataract cases following lensectomy and vitrectomy.
Techniques of restoration of good visual function, correction of amblyopia, and optical correction are still undergoing refinement; however, the combined lensectomy and vitrectomy has, at least from the time of follow-up, substantially eliminated significant complications.
REFERENCES
1. Fraser GA, Friedmann AI. The causes of blindness in childhood. Baltimore: Johns Hopkins Press, 1967.
2. Penzani B. Osservazioni cliniche e studio statistico sulla cecita infantile. Ann Ott Clin Ocul 1954; 80:189-94.
3. Francois J. Congenital cataracts. Springfield, Illinois: Charles C Thomas, 1963.
4. Peyman GA, Raichand M, Goldberg MF. Surgery of congenital and juvenile cataracts: A pars plicata approach with the vitrophage. Br J Ophthalmol 1978; 62:780-83.
5. Barkan 0. A procedure for the extraction of congenital soft and membranous cataracts. Am J Ophthalmol 1932; 15: 117-24.
6. Chandler PA. Surgery of the lens in infancy and childhood. Arch Ophthalmol 1951; 45:125-38.
7. Cordes FC. Failure in congenital cataract surgery: A study of fifty-six enucleated eyes. Trans Am Acad Ophthalmol Otolaryngol 1956; 60:345-67.
8. Bagley CH. Congenital cataracts: A survey of the various types of operation. Am J Ophthalmol 1949; 32:419-41
9. Owens WC, Hughes WF. Results of surgical treatment of congenital cataracts. Arch Ophthalmol 1948; 39:339-50.
10. Sheppard RW, Crawford JC. The treatment of congenital cataracts. Surv Ophthalmol 1973; 14:340-47.
11. Ryan SJ, von Noorden GA. Further observations on the aspiration technique in cataract surgery. Am J Ophthalmol 1971, 71:626-30.
12. Scheie HG. Aspiration of congenital or soft cataracts: A new technique. Am J Ophthalmol 1960; 50:1048-56.
13. Kelman CD. Phacoemulsification and aspiration: A new technique of cataract removal: A preliminary report. Ophthalmology 1967; 64:23-5.
14. Hiles DA, Hurite FA. Results of the first year's experience with phacoemulsification. Am J Ophthalmol 1973; 75:473-77.
15. Hiles DA, Wallace PH. Phacoemulsification verus aspiration in infantile cataract surgery. Ophthalmic Surg 1974; 5:13-6.
16. Calhoun JH, Harley RD. The rotc-extractor in pediatric ophthalmology. Trans Am Ophthalmol Soc 1975; 73:292-05.
439