Embed Size (px)
Citation preview

Part C HIV Early Intervention Services New Geographic Service Areas
HRSA-12-171
Pre-Review Orientation Conference CallJune 8, 2012
Presented by: Department of Health and Human Services
Health Resources and Services AdministrationHIV/AIDS Bureau
Division of Community HIV/AIDS Programs
Director: Dr. Margarita Figueroa-Gonzalez
1
1

Agenda• Overview of Part C EIS Program• Program Narrative: Review Criteria
• Need• Epidemiology, unmet need, gaps in services,
barriers• Response
• Work Plan• Evaluation & Technical Support Capacity
• Clinical quality management, data collection system• Impact• Resources/ Capabilities
• Staffing Plan, Organizational Information• Support Requested
• Budget in relation to Proposed Project
• Funding Preference• Q &A
2
2

Purpose•President Obama’s 2011 World AIDS Day
Announcement•Provide HIV medical and psychosocial services
to:1. newly diagnosed/identified Persons Living
With HIV/AIDS (PLWHA) who are not in care;2. previously diagnosed PLWHA but never been in care;3. PLWHA who have dropped out of care; and,4. existing PLWHA clients
3
3

Part C EIS Overview• The purpose is to provide HIV primary care in the
outpatient setting. Applicants must propose a comprehensive continuum of outpatient HIV primary care services in the targeted area.
• Required Services include:• HIV Counseling, testing, and referral;• Medical evaluation and clinical care;• Other primary care services; and• Referrals to other health services.
• Applications should reflect a Medical Model of Care
• Budgets demonstrate allocations for providers who can Assess, Treat, and Refer PLWHA for HIV infection 4
4
Payer of Last Resort
• Part C programs are expected to use Ryan White funds as payer of last resort.
• Ryan White HIV/AIDS Program Part C funds cannot be used to supplant existing funding streams covering HIV primary care and other services.
• Part C funds cannot be used to pay for services when payment has been made or is expected from insurance or other health benefits program.
5
5

Eligible Applicants• Organizations in the United States and its
territories applying as new EIS applicants (not currently funded by Part C)--Note if applicant is a sub-contractor of a
current Part C grantee and the justification for additional Ryan White funding in the proposed service area
• Public or private nonprofit entities, including but not limited to
Federally Qualified Health Centers, Rural Health Centers, Health Centers under the Indian Health Service, University Medical Centers and affiliated clinics, Faith-based or community-based organizations 6
6
Part C Budget Categories
1. Early Intervention Services Costs (50%)
2. Core Medical Services Costs (75% after excluding CQM and Administrative)
3. Clinical Quality Management (CQM) Costs
4. Support Services Costs
5. Administrative Costs (10% of total annual request)
7
7

Part C Early Intervention Services
• Licensed medical providers who can assess, treat and refer
• Proportional medical support- nurses, med assistants
• Laboratory, immunizations and diagnostic tests
• Adherence monitoring/education
•Dental care•Mental health •Nutrition •Substance abuse•Specialty Care Services
•Travel to provide clinical care
8
8
EIS Funds cannot be used for:Services must be consistent with HAB Policy Notice 10-02 http://hab.hrsa.gov/manageyourgrant/pinspals/
eligible1002.html
Inpatient services Residential treatment Clinical research Nursing home care Cash payments to clients Purchase or improvement of real property Syringe Services programs Lobbying activities, advertising
9
9

Program Narrative
• Introduction• Needs Assessment• Methodology• Work Plan• Resolution of Challenges• Evaluation and Technical Support• Organizational Information
10
10

Needs Assessment: Four Major Sections
1. HIV Seroprevalence & Surrogate Markers – local HIV epidemiologic data from 2008 to 2010, unmet need calculation from Parts A/B
2. Social Context of HIV/AIDS— key community characteristics that support the need for Part C funding/services in the proposed area
3. Target Populations – are these consistent with those identified by the HIV epidemiologic data as new cases?
4. Local HIV Service Delivery System – are all HIV service providers, funding streams, and funded services described to assess current gaps and barriers?
11
11
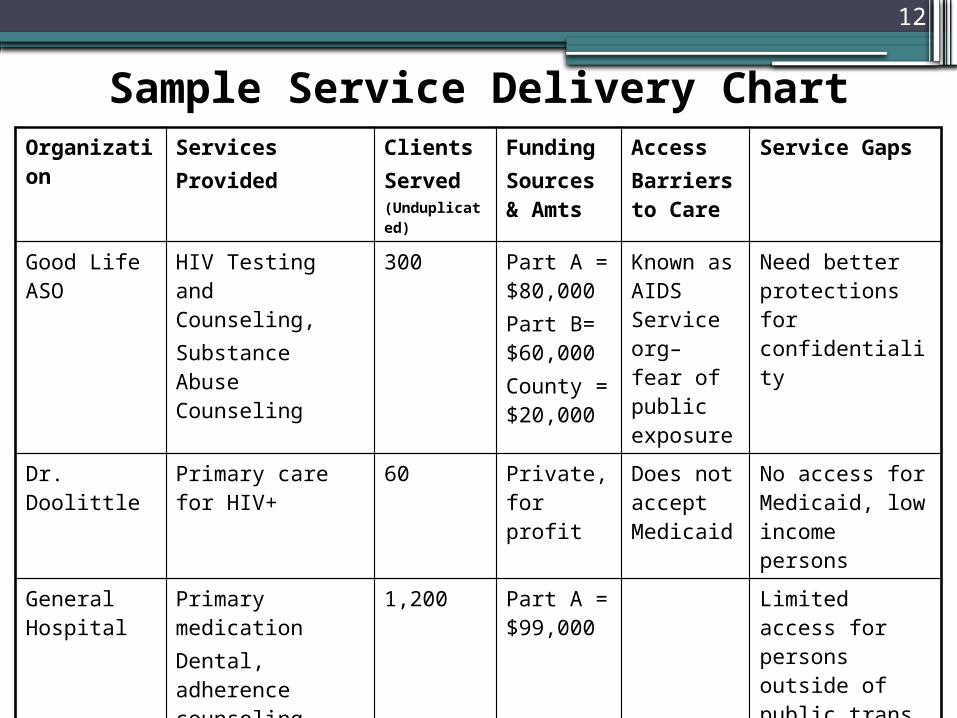
Organization ServicesProvided
ClientsServed(Unduplicated)
Funding Sources & Amts
AccessBarriers to Care
Service Gaps
Good Life ASO
HIV Testing and Counseling, Substance Abuse Counseling
300 Part A = $80,000Part B= $60,000County = $20,000
Known as AIDS Service org– fear of public exposure
Need better protections for confidentiality
Dr. Doolittle Primary care for HIV+
60 Private, for profit
Does not accept Medicaid
No access for Medicaid, low income persons
General Hospital
Primary medicationDental, adherence counseling, mental health, substance abuse treatment, nutritional services
1,200 Part A = $99,000
Limited access for persons outside of public trans limits
Average 5 week waiting period
Sample Service Delivery Chart
12

Review Criterion 1: Need• The extent to which the applicant provides clear and reliable data
showing an increased burden of HIV infection in the service area. The extent to which the applicant clearly describes the target population and the need for HIV-related health services in this population. This addresses the NHAS goal: to reduce HIV-related health disparities. The extent to which the applicant documents the public funding sources for HIV prevention and care in the proposed service area.
• The extent to which the applicant identifies unmet need, gaps in service and barriers to care.
• The extent to which the information shows a need for medical care paid by Part C for uninsured clients not covered by other Ryan White HIV/AIDS Parts.
• The extent to which the applicant demonstrates a need for Part C medical services based on epidemiological data, current HIV services, and funding available for the proposed service area.
13

Methodology: Scope of Work
1) HIV Counseling, Testing, Referral, Partner Counseling, and Linking to Care – targeted at high risk populations
2) Medical Evaluation and Clinical Care – description of the HIV medical care services consistent with HHS guidelines
3) Referral System – to other medical/specialty services
4) Other Core Medical Services – behavioral health, oral health, nutritional services, medical case management
5) Support Services – linked to medical/health outcomes
6) MAI
7) Coordination and Linkages with Other HIV Programs (scored under Impact) – reduces non-duplication of services
14
Review Criterion 2: Response• The strength of the medical evaluation and clinical care
systems (such as periodic medical evaluations, CD4 monitoring, viral load testing, antiretroviral therapy, prophylaxis and treatment of opportunistic infections). Evidence of adequate support for laboratory and pharmacy services, plans for staff education, and the involvement of consumers in decisions regarding their care. The extent to which the applicant describes a sound policy for after-hours and weekend coverage for urgent or emergency medical and dental care needs. The effectiveness of formal systems in place for referrals of individuals to health and support services that are not directly provided by the applicant. Evidence of mechanisms to follow-up on referrals and receive feedback from the providers of health and support services to which patients are referred. This addresses the NHAS goal: to increase access to care and optimize health outcomes for people living with HIV.
15

Work Plan Summary
• Access to Care• Comprehensive and Coordinated HIV
Primary Medical Care • Clinical Quality Management Program• Consumer Involvement activities
Include only the clients funded by Part C (as defined in the FOA).
Attachment 8
16

Sample Work Plan SummaryAccess to Care Objective FY 2012
Objective (# only)
1. # to be Counseled and Tested funded by award
2. # positive results
3. # New HIV infected patients to be enrolled in primary HIV medical care
Comprehensive, Coordinated Primary HIV Medical Care
FY 2012Objective
(# only)
1. # to be provided with Primary HIV medical care services
2. # to be provided with mental health screening
3. # to be provided with mental health treatment
4. # to be provided with substance abuse screening
5. #to be provided with substance abuse treatment
17

Sample Work Plan SummaryComprehensive, Coordinated Primary HIV Medical Care
FY 2012 Objective (# only)
6. # to be provided Hepatitis B screening
7. # to be provided Hepatitis C screening
8. # to be provided with care and treatment for Hepatitis C
9. # to be provided oral health care
10. # to be provided medical nutrition screening
11. # to be provided medical nutrition therapy by registered dietitian or licensed nutritionist
12. # to be provided treatment adherence services by qualified clinician
13. # to be provided medical case management by trained professional with IDSP
14. # to be provided specialty referrals
15. # to be provided support services to clients to meet their HIV medical outcomes.
18

Work Plan Summary: CQMClinical Quality Management Program FY 2012
Objective (# only)
Provide measures that the applicant organization has selected. Insert additional lines as needed.
For the HAB performance measures, see http://hab.hrsa.gov/special/qualitycare.htm
19

Work Plan Summary Consumer Involvement
Consumer Involvement FY 2012Objective
# consumers involved in planning, implementation and evaluation.
# of consumer meetings
# improvements made as a result of consumer involvement in evaluation
20

Review Criterion 2: Response• The extent to which the applicant demonstrates a lack of
resources for other core medical services, including outpatient oral health, adherence, mental health/substance abuse, and nutritional services and how this funding will be used to address the gaps. The extent to which HIV prevention services are incorporated into medical care. The extent to which the applicant explains how clients applying for financial support and services from other publicly funded programs will be assisted?
• The strength of the work plan summary as evidenced by measurable objectives that reflect, access to care, the comprehensive continuum of HIV care, quality improvement, and consumer involvement funded under the grant.
• Overall, the extent to which the applicant documents the ability of the organization to provide, internally and/or by contract, the full comprehensive continuum of HIV care, funded under the grant without duplication.
21

Evaluation and Technical Support
• The application should fully address the evaluation activities including quality management (QM) and information systems.
• QM should include:• Infrastructure• Performance Measurement• Quality Improvement
22
Information System• Describe the applicant’s current information system and
their ability to collect and report Part C required data to include the following:
The number of existing and new patients Demographic profile of patients Epidemiological data Exposure and diagnostic categories services The number of HIV infected individuals Third party program income Average costs of providing each service category
• Electronic Health Records• Office of National Coordinator for Health Information
Technology (ONC)www.hrsa.gov/healthit/ehrguidelines.html
• Department of Health and Human Services “Meaningful Use”www.cms.gov/ehrincentiveprograms
23

Review Criterion 3: Evaluation• The strength of the proposed quality management
infrastructure, including the key leaders and quality committee. The appropriateness of the role of consumers in the Quality Management program.
• The appropriateness of clinical indicators that will be used to measure performance. The extent to which the applicant describes how data will be used for quality improvement activities.
• The extent to which the applicant demonstrates how they will comply with reporting requirements of the program. The strength of the proposed data collection plan and process (e.g., frequency, key activities, and responsible staff). The strength of the process for reporting and disseminating future results and findings.
24

Review Criterion 4: Impact• The extent to which the work plan summary provides
objectives which are appropriate for the level of unmet need and gaps in services for the target population in the proposed service area, as described in the Needs Assessment.
• The extent to which the applicant describes how its proposed program will increase the number of (1) newly diagnosed PWLHA, (2) previously diagnosed PLWHA who have never been in care, and; (3) PLWHA who have dropped out of care that are linked to HIV medical care without duplication of services in the proposed service area. This addresses the President’s initiative stemming from World AIDS Day 2011 to increase access to primary HIV medical care and support services.
25

Organizational Information
• Describe the applicant organization’s capacity and expertise to provide primary care by describing the administrative, fiscal, and clinical operations.
• How does a Part C EIS project fit within the scope of the organization’s mission?
• The structure of the organization.
• Attachment 9: Project Organizational Chart –should demonstrate the placement of the proposed Part C program within the entire organization
26

Budget: Staffing Plan• Should include all staff being funded under Part C and
key staff not funded by the grant.
• Should demonstrate that project personnel are qualified by education/training, HIV experience and expertise to provide early intervention services under the grant.
• Should demonstrate language fluency and cultural competence
• Should provide the staff time/effort (FTE) and ALL funding sources for the HIV program
• Key personnel include:• Lead for quality management activities • Program coordinator• Staff managing and overseeing grant activities • Staff monitoring activities of contractors• Medical Director 27
27

Review Criterion 5: Resources• Evidence of the organization’s ability to implement the
proposed project. The strength of the organization’s mission, structure and experience which support the provision of HIV Primary care services as evidenced by the clinic licensure information and organizational chart.
• Overall, the strength of the organization’s fiscal and MIS capacity to manage this grant, and meet program requirements including monitoring grant expenditures, a discounted fee schedule, annual cap on patient charges, and collecting, tracking and using program income to support the HIV program. If applicable, the applicant’s demonstration of the ability to manage and monitor subcontractor performance and compliance with Part C EIS requirements.
28
Review Criterion 6: Support Requested
• The appropriateness of the requested funding level for each year of the project period in comparison to the level of effort, performance, and total number of patients served. The reasonableness of the average cost of care for each service category. The number of patients to be served, the number of patients with AIDS versus HIV, and the number of patients with no form of third party reimbursement or funding from Part A or B.
29

Part C Budget Requirements
• Shows only Federal Part C EIS funds
• At least 50% of Part C budget must be allocated for EIS/Primary care costs.
• At least 75% of the Part C budget, after CQM and Administrative costs are subtracted, must be allocated for Core Medical Services
• Administrative costs are capped at 10.0% of the total
EIS award amount
• Calculations for all items in the budget justification should include unit cost, number of units, and number of persons to be served
32

Budget: Points
• Budget Period is ONE YEAR
(July 1, 2012 to June 30, 2013)
• Organizations were instructed to submit three separate program specific line item budgets and one budget justification (which lists the changes in subsequent years reflected in the line-item budget).
• Section B of SF-424A: • Years 1 to 3 line item budget summary
33

Budget: Sample Line-Item
34

Salary Limitations
• This is a new HRSA requirement resulting from the Appropriations Act for 2012, that salaries charged to
grants are capped at $179,700 annually.
• This amount reflects an individual’s base salary, exclusive of fringe benefits and income earned outside of the applicant organization.
• The limitation also applies to subcontracts.
35
35

HRSA’s Scoring Rubric
•Available in the EHB-ARM system as a reference
•Good tool for gauging appropriate scoring of sections based upon analysis of the applicant’s response to the entire FOA and the Review Criteria
36
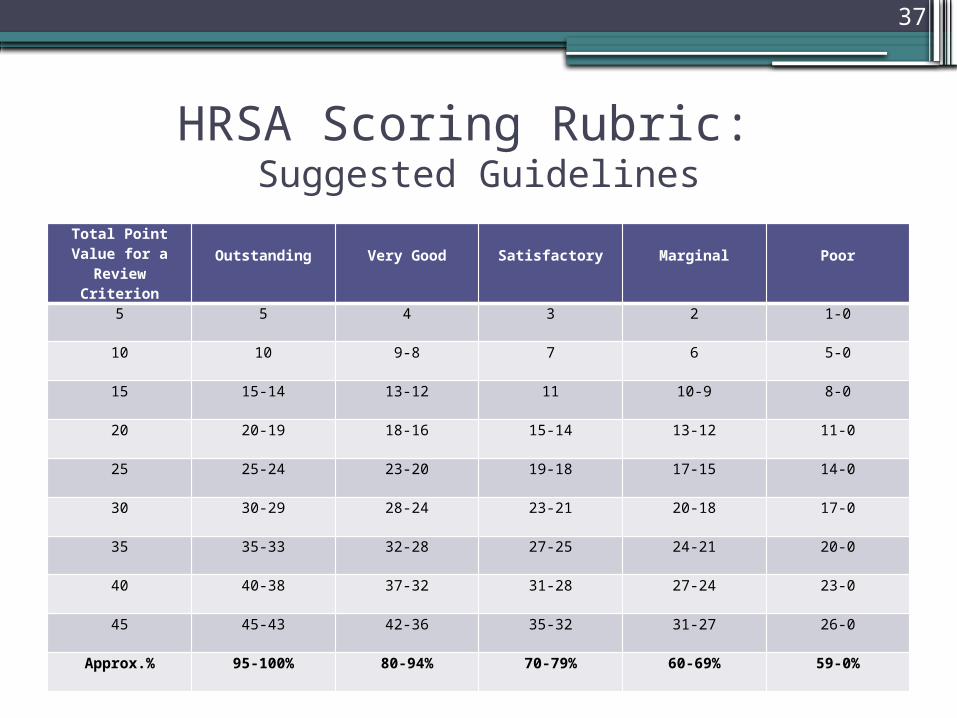
HRSA Scoring Rubric: Suggested Guidelines
Total Point Value for a Review
CriterionOutstanding Very Good Satisfactory Marginal Poor
5 5 4 3 2 1-0
10 10 9-8 7 6 5-0
15 15-14 13-12 11 10-9 8-0
20 20-19 18-16 15-14 13-12 11-0
25 25-24 23-20 19-18 17-15 14-0
30 30-29 28-24 23-21 20-18 17-0
35 35-33 32-28 27-25 24-21 20-0
40 40-38 37-32 31-28 27-24 23-0
45 45-43 42-36 35-32 31-27 26-0
Approx.% 95-100% 80-94% 70-79% 60-69% 59-0%
37

HRSA Scoring Rubric (cont.)• Outstanding All elements are clearly addressed, well conceived,
thoroughly developed, and well supported. Documentation and required information are specific and comprehensive. Weaknesses identified will likely have no effect on the applicant’s proposed project.
• Very Good Elements are clearly addressed with necessary detail and adequate support. Most documentation and required information are specific and sufficient. Weaknesses identified will likely have minor effect on the applicant’s proposed project.
• Satisfactory Elements are addressed, although some do not contain necessary detail and/or support. Most documentation and required information are present and acceptable. Weaknesses identified will likely have moderate effect on the applicant’s proposed project.
• Marginal Some elements are not addressed, and those addressed do not contain necessary detail and/or support. Some documentation and required information are missing or deficient. Weaknesses identified will likely have significant effect on the applicant’s proposed project.
• Poor Few, if any, elements are addressed. Documentation and required information are deficient or omitted. Weaknesses identified will likely have substantial effect on the applicant’s proposed project.
38

Funding Preference
• Must meet all factors in Qualification #1 for 2009 and 2010 to qualify for Increased Burden, then if applicable, can apply for rural areas or underserved. Document in detail- Attachment 12
• Qualification 1: Increased Burden
▫ Increased number and increased rate of HIV/AIDS Cases▫ Lack of EIS services, from Parts A, B and C▫ Increased number and increased rate of
Other sexually transmitted diseases TB Drug Abuse Co-infection of HIV and Hepatitis B or C
▫ Lack of primary care providers, other than the applicant▫ Distance to service area with adequate HIV providers▫ Patient travel time to that area
• Qualification a: Rural Areas• Qualification b: Underserved (from all EIS resources
including Parts A/B/C) 37
39
Your questions are welcome
Bob Settles
HAB TARGET Websitehttp://careacttarget.org/webcasts.asp
40