Embed Size (px)
Citation preview

Part I – Triple-Negative Breast Cancer: The New BiologyTuesday, June 14, 20117:30 PM - 8:30 PM ET
RTP TV: An 8-Part Live CME Webcast Series

Joyce O’Shaughnessy, MD Co-Director, Breast Cancer Research ProgramBaylor-Charles A Sammons Cancer CenterTexas Oncology, PAUS OncologyDallas, Texas
Eric P Winer, MDThompson Investigator in Breast Cancer ResearchChief, Division of Women’s Cancers Dana-Farber Cancer InstituteProfessor of MedicineHarvard Medical SchoolBoston, Massachusetts
Neil Love, MDResearch To PracticeMiami, Florida

Disclosures for Moderator Neil Love, MD
Dr Love is president and CEO of Research To Practice, which receives funds in the form of educational grants to develop CME activities from the following commercial interests: Allos Therapeutics, Amgen Inc, AstraZeneca Pharmaceuticals LP, Aureon Laboratories Inc, Bayer HealthCare Pharmaceuticals/Onyx Pharmaceuticals Inc, Biogen Idec, Boehringer Ingelheim Pharmaceuticals Inc, Bristol-Myers Squibb Company, Celgene Corporation, Cephalon Inc, Daiichi Sankyo Inc, Dendreon Corporation, Eisai Inc, EMD Serono Inc, Genentech BioOncology, Genomic Health Inc, ImClone Systems, a wholly owned subsidiary of Eli Lilly and Company, Lilly USA LLC, Millennium — The Takeda Oncology Company, Mundipharma International Limited, Myriad Genetics Inc, Novartis Pharmaceuticals Corporation, OSI Oncology, Sanofi and Seattle Genetics.

Disclosures for Joyce O’Shaughnessy, MD
Advisory Committee
Biogen Idec, Bristol-Myers Squibb Company, Caris Diagnostics Inc, Eisai Inc, Genentech BioOncology, GlaxoSmithKline, GTx Inc, Johnson & Johnson Pharmaceuticals, Roche Laboratories Inc, Sanofi
Speakers BureauBristol-Myers Squibb Company, Celgene Corporation, Sanofi

Disclosures for Eric P Winer, MD
No financial interests or affiliations to disclose

Part I – Triple-Negative Breast Cancer: The New BiologyTuesday, June 14, 20117:30 PM - 8:30 PM ET
RTP TV: An 8-Part Live CME Webcast Series

Survey of 100 Practicing Oncologists
• 95% – fraction who see patients with TNBC
• 10 – median number of patients with metastatic TNBC currently in their practices

Survey of 100 Practicing Oncologists
Fraction with a patient who has received…
• Iniparib – 23%• Olaparib – 16%• Veliparib – 7%

Survey of 100 Practicing Oncologists
If you were to attend a CME conference on breast cancer, to what extent would you be interested in learning about the following topics?
• Response scale 0 – 10
0 = no interest
10 = very interested

TNBC: New Agents and Regimens
1%
2%
2%
2%
10%
9%
11%
18%
23%
22%
0% 5% 10% 15% 20% 25%
1
2
3
4
5
6
7
8
9
1045%

TNBC: PARP Inhibitors
0%
1%
2%
6%
5%
12%
18%
14%
20%
22%
0% 5% 10% 15% 20% 25%
1
2
3
4
5
6
7
8
9
1042%

Survey of 100 Practicing Oncologists
What question(s) would you like to pose to a clinical investigator with expertise in the management of TNBC?
• 97 questions/cases received

When will newer agents be integrated into earlier lines of treatment?

When is BRCA testing indicated in a patient with TNBC?

Under what conditions should metastatic sites be biopsied?

Are there other new noncytotoxic, targeted agents in TNBC in addition to PARP inhibitors?
— Naples, FL

1. Are there situations in which you would order BRCA testing for a 50-year-old woman with metastatic TNBC and no family history of breast or ovarian cancer?
12%
52%
36%
0% 10% 20% 30% 40% 50% 60%
No
Yes, sometimes
Yes, usually

Case 1 (Dr O’Shaughnessy)
• 50 yo woman with basal-like TNBC– Preoperative AC paclitaxel: pCR
• Tumor “melts away” after 1 cycle of AC– Locoregional RT
• 2 years later, very rapidly growing ipsilateral internal mammary node protruding from her chest and invading sternum and mediastinal LNs
• Patient enrolls on a trial of gem/carbo ± iniparib*– Major response for 8 cycles (6 months)
• Tissue harvested for total genome sequencing• Paclitaxel/bevacizumab
– Response for 6 months but progressing
* O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.

Progression with Regrowth of IpsilateralMammary Mass and Mediastinal Nodes

O’Shaughnessy J et al. Proc ASCO 2009;Abstract 3.
Phase II Study of Iniparib plus Gemcitabine/Carboplatin in mTNBC
Clinical Parameter Gem/Carbo
Gem/Carbo + Iniparib HR p-value
CBR 21% 62% – 0.0002
Median PFS 3.3 mo 6.9 mo 0.34 <0.0001
Median OS 5.7 mo 9.2 mo 0.348 0.0005

A Randomized Phase III Study of Iniparib (BSI-201) in Combination with Gemcitabine and Carboplatin in Metastatic Triple-Negative Breast Cancer (mTNBC)
O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.

Phase II Study of Iniparib plus Gemcitabine/Carboplatin in mTNBC
Clinical Parameter Gem/Carbo
Gem/Carbo + Iniparib HR p-value
CBR 34% 56% — 0.01
Median PFS 3.6 mos 5.9 mos 0.59 0.01
Median OS 7.7 mos 12.3 mos 0.57 0.01
• Based on promising Phase II results, Phase III trial of iniparib is conducted
O’Shaughnessy J et al. N Engl J Med 2011;364(3):205-14.

Metastatic Triple-Negative Breast Cancer (mTNBC)
• 15% of breast cancers; clinically defined as ER-negative, PR-negative and HER2-non-overexpressing
• Heterogeneous disease with generally virulent natural history
• Shares gene expression profiles with basal-like, claudin-low and other molecular subtypes
• No clinical implications of molecular subtypes at present
O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.

Iniparib (BSI-201)
A novel, investigational, anticancer agent• In triple-negative breast cancer cell lines:
– Induces cell cycle arrest in the G2/M phase – Induces double strand DNA damage ϒH2AX foci
but does not inhibit PARP1 and 2 at physiologic drug concentrations
– Potentiates cell-cycle arrest induced by DNA damaging agents, including platinum and gemcitabine
• Physiologic targets of iniparib and its metabolites are under investigation
O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.

Preclinical Pharmacodynamic and Pathway Analysis of 3 Presumed PARP Inhibitors: ABT-888, AZD2281, BSI-201
• ABT-888 and AZD2281 are mediated by PARP1 or PARP2.
• Iniparib (BSI-201) suppressed genes in the telomere pathway, suggesting PARP5/6 as potential targets.
Ji J et al. Proc AACR 2011;Abstract 4527.

Schema
Gem/carbo (GC)(N = 258)
Gemcitabine 1,000 mg/m2 IV d 1, 8carboplatin AUC 2 IV d 1, 8
21-day cycles
Gem/carbo (GC)(N = 258)
Gemcitabine 1,000 mg/m2 IV d 1, 8carboplatin AUC 2 IV d 1, 8
21-day cycles
Study design: Multicenter, randomized, open-label Phase III trial (N = 519)
Study Population:
• Stage IV TNBC• ECOG PS 0-1• Stable CNS metastases
allowed• 0-2 prior chemotherapies
for mTNBC
• Randomization stratified by prior chemotherapy in the metastatic setting:
• 1st-line (no prior therapy)
• 2nd/3rd-line (1-2 prior therapies)
Study Population:
• Stage IV TNBC• ECOG PS 0-1• Stable CNS metastases
allowed• 0-2 prior chemotherapies
for mTNBC
• Randomization stratified by prior chemotherapy in the metastatic setting:
• 1st-line (no prior therapy)
• 2nd/3rd-line (1-2 prior therapies)
Gem/carbo + iniparib (GCI)(N = 261)
Gemcitabine 1,000 mg/m2 IV d 1, 8carboplatin AUC 2 IV d 1, 8
iniparib 5.6 mg/kg IV d 1, 4, 8, 11
21-day cycles
Gem/carbo + iniparib (GCI)(N = 261)
Gemcitabine 1,000 mg/m2 IV d 1, 8carboplatin AUC 2 IV d 1, 8
iniparib 5.6 mg/kg IV d 1, 4, 8, 11
21-day cycles
Crossover allowed
to GCI following disease
progression (central review)
Crossover allowed
to GCI following disease
progression (central review)
RR
95% (n = 152) of progressing patients crossed over to GCI at time of primary analysis.
O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.

Study Objectives
Primary:
• Coprimary endpoints:
– Overall survival (OS)
– Progression-free survival (PFS)
– Study considered positive if either endpoint met
Secondary:
• Objective response rate (ORR)
• Safety, tolerability and pharmacokinetics of GCI
O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.

Treatment-Emergent Adverse EventsSafety Population (Prior to crossover, >5% Grade 3/4 in GCI arm)
AE
GC
N = 244
GCI
N = 255
All Grades
%
Grade 3/4
%
All Grades
%
Grade 3/4
%
Neutropenia 65 53 71 61
Febrile neutropenia 2 2 2 2
Anemia 62 22 64 18
Thrombocytopenia 54 24 54 28
Fatigue 64 6 71 8
Alanine aminotransferase increased
19 6 28 6
Dyspnea 27 4 29 6
O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.

1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
00 2 4 6 8 10 12 14 16
Pro
bab
ility
of
Pro
gre
ssi
on
-Fre
e S
urv
iva
l
Months Since Study Entry
PFSGC
(N = 258)GCI
(N = 261) HR p-value
Median PFS 4.1 mos 5.1 mos 0.79 0.027
Efficacy EndpointsProgression-Free Survival – ITT Population
Prespecified alpha = 0.01
O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.

OSGC
(N = 258)GCI
(N = 261) HR p-valueMedian OS
11.1 mos 11.8 mos 0.88 0.28
O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
00 2 4 6 8 10 12 14 16
Pro
bab
ility
of
Su
rviv
al
Months
Prespecified alpha = 0.04
Efficacy EndpointsOverall Survival – ITT Population

Exploratory Analysis 2nd/3rd-Line Progression-Free Survival – ITT Population
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
00 2 4 6 8 10 12 14 16
Pro
bab
ility
of
Pro
gre
ssi
on
-Fre
e S
urv
iva
l
Months Since Study Entry
2nd/3rd-line – 43% patients (222/519)
PFSGCI 43 mos
GC 29 mos
HR = 0.67, 169 events
O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.

2nd/3rd-line – 43% patients (222/519)
OS
GCI 108 mos
GC 91 mos
HR = 0.65, 132 events
O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.
Exploratory Analysis 2nd/3rd-Line Overall Survival – ITT Population
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
00 2 4 6 8 10 12 14 16
Pro
bab
ility
of
Su
rviv
al
Months

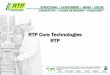
TNBC Comprised of Diverse Molecular Subtypes
With permission from O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.
Preliminary*R
elat
ive
Fre
qu
ency
in P
anel
0.3
0.25
0.2
0.15
0.1
0.05
0Basal Claudin-low ERBB2 Luminal A Luminal B
* Validation ongoingAffymetrix gene expression profiling of FFPE samplesIntrinsic subtypes assigned using Sorlie et al, PNAS, 2003 data set and claudin-low classifier(Prat et al, BCR, 2010) [courtesy of J. Theilhaber and D. Bergstrom, Sanofi]
Normal-like

• Triple-negative eligibility enriches for subtype of biologic interest (basal-like) but will misclassify some.
• However, we have no reason to think this happened in a differential manner across the 2 trials.
Triple Negative is Biologically Heterogeneous
Prat A and CM Perou. Mol Oncol 2011;5(1):5-23.
2%13%13%
71%
0%
20%
40%
60%
80%
100%
ER+/HER2+ER+/HER2-ER-/HER2+ER-/HER2-
Claudin-low Basal-like
HER2-enriched Luminal B Luminal A
2% 7% 8%
83%
0%
20%
40%
60%
80%
100%
15%16%
51%
18%
0%
20%
40%
60%
80%
100%
20%
72%
1%7%
0%
20%
40%
60%
80%
100%
7%
87%
2% 5%
0%
20%
40%
60%
80%
100%

TNBC Comprised of Diverse Molecular Subtypes
With permission from O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.
Preliminary*R
elat
ive
Fre
qu
ency
in P
anel
0.3
0.25
0.2
0.15
0.1
0.05
0Basal Claudin-low ERBB2 Luminal A Luminal B
* Validation ongoingAffymetrix gene expression profiling of FFPE samplesIntrinsic subtypes assigned using Sorlie et al, PNAS, 2003 data set and claudin-low classifier(Prat et al, BCR, 2010) [courtesy of J. Theilhaber and D. Bergstrom, Sanofi]
Normal-like

Prat A, Perou CM.
Mol Oncol 2011;5(1):5-23.
Deconstructing the molecular portraits of breast cancer

Prat A and CM Perou. Mol Oncol 2011;5(1):5-23.
Luminal
HER2
Basal
Immune
Cell Adhesion
Mesenchymal/ECM
Proliferation
Normal Breast-like (NBL)Luminal A and B (LA and LB)
Claudin-low (CL)Basal-like (BL)HER2-enriched (H2)
+2 +1 0 -1 -2

• Triple-negative eligibility enriches for subtype of biologic interest (basal-like) but will misclassify some.
• However, we have no reason to think this happened in a differential manner across the 2 trials.
Triple Negative is Biologically Heterogeneous
Prat A and CM Perou. Mol Oncol 2011;5(1):5-23.
2%13%13%
71%
0%
20%
40%
60%
80%
100%
ER+/HER2+ER+/HER2-ER-/HER2+ER-/HER2-
Claudin-low Basal-like
HER2-enriched Luminal B Luminal A
2% 7% 8%
83%
0%
20%
40%
60%
80%
100%
15%16%
51%
18%
0%
20%
40%
60%
80%
100%
20%
72%
1%7%
0%
20%
40%
60%
80%
100%
7%
87%
2% 5%
0%
20%
40%
60%
80%
100%


2. What is the most common pattern of receptor status shift from primary tumor to metastatic disease?
11%
16%
3%
70%
0% 20% 40% 60% 80%
ER-positive ER-negative
ER-negative ER-positive
HER2-positive HER2-negative
HER2-negative HER2-positive

Case 2 (Dr Winer)
• 48 yo premenopausal, BRCA1/2-negative woman presents 6 years ago with weakly ER+, PR- T2N1 breast cancer– Neoadjuvant AC paclitaxel– Excision/re-excision plus RT– Tamoxifen
• Ipsilateral breast recurrence 1 year later– Mastectomy
• Waxing and waning supraclavicular adenopathy over next 18 months until diagnosed with local recurrence
• Needle biopsy reveals metastatic TNBC, with small pulmonary nodule
• Enrolled on TBCRC009: Phase II study of cisplatin or carboplatin for metastatic TNBC*– Clinical CR after 7 cycles of cisplatin– Treatment discontinued due to toxicity (fatigue, neuropathy)
• No further therapy for past 2 years, 4 months
* Isakoff SJ et al. ASCO 2011;Abstract 1025.


Isakoff SJ et al.
Proc ASCO 2011;Abstract 1025. (Poster Discussion)
TBCRC009: A Multicenter Phase II Study of Cisplatin or Carboplatin for Metastatic Triple-Negative Breast Cancer and Evaluation of p63/p73 as a Biomarker of Response

Phase II Study of Cisplatin or Carboplatin for mTNBC
• 86 patients enrolled to physician's choice of either cisplatin or carboplatin
• Overall RR: 30.2%, including 4 CR (4.7%) and 22 PR (25.6%)
• RR by treatment (exploratory): 37% cisplatin
23% carboplatin
• p63/p73 analysis is ongoing
Isakoff SJ et al. Proc ASCO 2011;Abstract 1025.

Submitted CaseDr Frances de la Serna, Philippines
• 40 yo woman with axillary lymphadenopathy in 1/2010– Excisional biospy: Ductal carcinoma consistent with
breast primary in 4 nodes– Ultrasound: 2 solid masses in breast (15.1 and
20.9 mm) • Neoadjuvant anthracycline/taxane-based therapy x
2 cycles surgery– No residual tumor or LVI in the breast– 7/9 nodes positive– ER/PR-, HER2 1-2+ (FISH positive)
• Receives chemotherapy/trastuzumab

Submitted Case (Continued)
• 12/2010: Neck mass– FNB: Metastatic carcinoma– Multiple enlarged lymph nodes in supraclavicular
and jugular chains– Excisional biopsy: ER/PR/HER2-negative
adenocarcinoma• Patient receives cisplatin/gemcitabine
– Resolution of enlarged nodes• 5/2011: Neck mass
– Biopsy: Metastatic carcinoma– Multiple nodules on the skin flap
• Plan: Continue cisplatin

Local versus Central Laboratory Discrepancies in TNBC Status (CIBOMA/2004-01/GEICAM/2003-11)
• N = 1,441 patient samples sent for central laboratory confirmation
• In 130 cases (9%) tumors were found to not be TNBC by central determination
• 71% of discrepant results involved ER or PR status
• 22% of discrepant results involved HER2 status
Ruiz-Borrego M et al. Proc ASCO 2011;Abstract 1022.

von Minckwitz G et al. J Clin Oncol 2011;29(16):2150-57.
Cytoplasmic Poly(Adenosine Diphosphate-Ribose) Polymerase Expression Is Predictive and Prognostic in Patients with Breast Cancer Treated with Neoadjuvant Chemotherapy

Retrospective Analysis of Cytoplasmic PARP (cPARP) Expression in Patients Treated with Neoadjuvant Chemotherapy• N = 638 tumor samples from patients enrolled in
GeparTrio study of neoadjuvant TAC therapy
• High cPARP expression detected in all tumor subtypes, but highest in more aggressive cancer phenotypes
– 35.5% of TNBC
– 26.4% of HER2-positive
– 18.0% of HR-positive/HER-negative
• In TNBC tumors, high cPARP expression is linked to pCR rate but not to survival after therapy
von Minckwitz G et al. J Clin Oncol 2011;29(16):2150-57.


TBCRC 018: Phase II Study of Iniparib plus Chemotherapy to Treat Triple-Negative Breast Cancer (TNBC) Brain Metastases (BM)
Anders CK et al.
Proc ASCO 2011;Abstract TPS127: Trials in Progress.

TBCRC 018: A Phase II Study of Iniparib plus Chemotherapy for TNBC Brain Metastases (BM)
Anders CK et al. Proc ASCO 2011;Abstract TPS127.
• Target accrual: 40
• Eligibility: TNBC BM >0.5 cm, no limit to prior therapies, no diffuse leptomeningeal disease
• Regimen: Iniparib + irinotecan
• Primary endpoint: Intracranial or extracranial TTP

3. A woman in her midfifties with locally advanced and metastatic TNBC: What is your most likely treatment regimen?
27%
14%
13%
23%
23%
0% 5% 10% 15% 20% 25% 30%
Gemcitabine/platinum
Taxane/platinum/bevacizumab
Taxane/platinum
Taxane/bevacizumab
Anthracycline/taxane

Case 3 (Dr O’Shaughnessy)
• A woman in her mid-50s with locally advanced and metastatic TNBC
– Enrolled in a study of total genome sequencing
– Determined to have a high level BRAF amplicon
• Enrolled on a Phase I trial of MEK plus AKT inhibitors*
– Significant response in a very large, fungating breast
* Tolcher AW et al. ASCO 2011;Abstract 3004.

4. An 83-year-old woman with TNBC and a known BRCA mutation develops nodal and lung metastases two years after TC x 4. What is your most likely treatment regimen?
51%
33%
16%
0% 10% 20% 30% 40% 50% 60%
Single-agentchemotherapy
Gemcitabine/platinum
Taxane/bevacizumab

Case 4 (Dr Winer)
• 83 yo woman presented 6 years ago with ER+ breast cancer– Radiation and hormonal therapy given
• Contralateral TNBC 3 years later– BRCA1 mutation– The patient is treated with TC x 4
• Nodal and lung metastases 2 years later– Phase III trial of GC ± iniparib*– Good response but brain metastases after
5 cycles
* O’Shaughnessy J et al. Proc ASCO 2011;Abstract 1007.


Tolcher AW et al.
Proc ASCO 2011;Abstract 3004.
A Phase I Dose-Escalation Study of Oral MK-2206 (Allosteric AKT Inhibitor) with Oral Selumetinib (MEK Inhibitor) in Patients with Advanced or Metastatic Solid Tumors

Phase I Dose-Escalation Study of Oral AKT Inhibitor MK-2206 Combined with MEK Inhibitor Selumetinib• N = 33 patients treated at 5 dose levels
• Preliminary antitumor activity and durable SD observed
– Confirmed PR: Ovarian cancer
NSCLC (KRAS mutant)
– SD: Pancreatic cancer (KRAS wild type and mutant)
Squamous NSCLC (EGFR wild type, KRAS
wild type)
Adenocarcinoma of appendix
• Main DLTs were skin rash, diarrhea, stomatitis and ocular events
• No drug-drug interactions observed
Tolcher AW et al. Proc ASCO 2011;Abstract 3004.


Schedule of Events
Tuesday, June 21 MelanomaKeith T Flaherty, MDJeffrey Weber, MD, PhD
Tuesday, June 28 Non-Small Cell Lung CancerLucian R Chirieac, MD Thomas J Lynch Jr, MDLecia V Sequist, MD, MPH
Tuesday, July 5Multiple MyelomaNikhil C Munshi, MDA Keith Stewart, MBChB
Tuesday, July 12Gastric CancerCharles S Fuchs, MD, MPHDavid H Ilson, MD, PhDLaura H Tang, MD, PhD
Tuesday, July 19Triple-Negative Breast Cancer: Current Clinical Management
Harold J Burstein, MD, PhDCharles E Geyer Jr, MD
Tuesday, July 26Non-Hodgkin’s Lymphoma/Chronic Lymphocytic LeukemiaStephanie A Gregory, MDJohn P Leonard, MD
Tuesday, August 2Chronic Myeloid LeukemiaSusan M O’Brien, MDNeil P Shah, MD, PhD



























![[MS-RTP]: Real-time Transport Protocol (RTP) …...Release: July 24, 2018 [MS-RTP]: Real-time Transport Protocol (RTP) Extensions Intellectual Property Rights Notice for Open Specifications](https://img.pdfslide.net/doc/110x75/5ecb4ebafdd0d04e1c3c1812/ms-rtp-real-time-transport-protocol-rtp-release-july-24-2018-ms-rtp.jpg)