Embed Size (px)
Citation preview

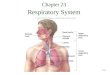
Part II - Respiratory Part II - Respiratory PhysiologyPhysiology

4 distinct events4 distinct events Pulmonary ventilationPulmonary ventilation: air is moved in and out : air is moved in and out
of the lungsof the lungs External respirationExternal respiration: gas exchange between : gas exchange between
blood and alveoliblood and alveoli Respiratory gas transportRespiratory gas transport: CV system : CV system
transports oxygen and carbon dioxide between transports oxygen and carbon dioxide between lungs & tissues (discussed in Blood chapter)lungs & tissues (discussed in Blood chapter)
Internal respirationInternal respiration: gas exchange between : gas exchange between blood & tissue cellsblood & tissue cells Definition: Cellular respirationDefinition: Cellular respiration: actual use of : actual use of
oxygen & production of carbon dioxide in the cellsoxygen & production of carbon dioxide in the cells (this is why we have to breathe!!)(this is why we have to breathe!!)

Pulmonary VentilationPulmonary Ventilation

External Respiration External Respiration

Resp. Gas TransportResp. Gas Transport

Internal RespirationInternal Respiration

Cellular RespirationCellular Respiration

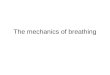
Mechanics of BreathingMechanics of Breathing

Pulmonary Ventilation: Event #1 Pulmonary Ventilation: Event #1
Pulmonary ventilation: - Moving air into Pulmonary ventilation: - Moving air into and out of the lungsand out of the lungs Depends on pressure changesDepends on pressure changes BreathingBreathing
Inspiration = moving air into the lungsInspiration = moving air into the lungs Expiration = moving air out of lungsExpiration = moving air out of lungs

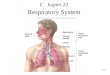
Pressure RelationshipsPressure Relationships
Intrapulmonary pressureIntrapulmonary pressure Pressure within the alveoli (lungs)Pressure within the alveoli (lungs) Changes with phases of breathingChanges with phases of breathing Always equalizes itself with atmospheric Always equalizes itself with atmospheric
pressurepressure Intrapleural pressureIntrapleural pressure
Pressure within intrapleural space (between Pressure within intrapleural space (between the pleural membranes )the pleural membranes )
Always 4 mmHg less than intrapulmonary Always 4 mmHg less than intrapulmonary pressurepressure


AtalectasisAtalectasis
Any conditions that causes intrapulmonary Any conditions that causes intrapulmonary pressure to equal intrapleural pressure will pressure to equal intrapleural pressure will cause the lungs to collapsecause the lungs to collapse
This means they lose the ability This means they lose the ability to move air since there is NO to move air since there is NO more pressure differencemore pressure difference

AtelectasisAtelectasis
term for lung collapseterm for lung collapse

PneumothoraxPneumothoraxAir in the intrapleural Air in the intrapleural
space due to trauma – space due to trauma – causes lung collapsecauses lung collapse

Pulmonary ventilationPulmonary ventilation
Question: Why does breathing happen?Question: Why does breathing happen? ONLY acceptable answer: The RULE: ONLY acceptable answer: The RULE:
Volume changes lead to pressure changes Volume changes lead to pressure changes which lead to the flow of gases to equalize which lead to the flow of gases to equalize the pressurethe pressure

Diaphragm StructureDiaphragm Structure
Boyle’s Law = Pressure & Volume have an INVERSE relationship.

Pressure differences cause gas to flow from Pressure differences cause gas to flow from high to lowhigh to low

When the diaphragm contracts, the When the diaphragm contracts, the muscle fibers shorten – so muscle muscle fibers shorten – so muscle
comes downcomes down

InspirationInspiration
Main inspiratory musclesMain inspiratory muscles Diaphragm & external intercostalsDiaphragm & external intercostals
Thoracic dimensions change to increase Thoracic dimensions change to increase volume of thoracic cavity by 0.5 litersvolume of thoracic cavity by 0.5 liters
Intrapulmonary pressure drops 1-3 mmHg Intrapulmonary pressure drops 1-3 mmHg and air rushes info normal quiet inspirationand air rushes info normal quiet inspiration
A deep forced (active) inspiration requires A deep forced (active) inspiration requires activation of accessory muscles – see activation of accessory muscles – see diagram in notesdiagram in notes

ExpirationExpiration
A passive process dependent on natural A passive process dependent on natural lung elasticitylung elasticity
lungs recoil when inspiration stops – so lungs recoil when inspiration stops – so alveoli compress –which leads to a volume alveoli compress –which leads to a volume
decreases -causing intrapulmonary pressure decreases -causing intrapulmonary pressure to rise - gas outflows to equalize the to rise - gas outflows to equalize the pressure with atmospheric pressurepressure with atmospheric pressure
Forced (active) expiration requires Forced (active) expiration requires contraction of abdominals, etc – see diagramcontraction of abdominals, etc – see diagram


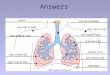
What doctors listen forWhat doctors listen for
Bronchial sounds: produced by air rushing Bronchial sounds: produced by air rushing through trachea & bronchithrough trachea & bronchi
Vesicular sounds: produced by air filling Vesicular sounds: produced by air filling alveolialveoli

Respiratory SoundsRespiratory Sounds
WheezingWheezing: whistling : whistling soundsound
Rales: Rales: rasping rasping soundsound

Hear the soundsHear the sounds
Basic Lung Sounds – Bronchial Auscultating The Lungs - Reference Guide

Physical factors influencingPhysical factors influencing
Pulmonary ventilation can be influenced Pulmonary ventilation can be influenced by 4 physical factorsby 4 physical factors Respiratory passage resistanceRespiratory passage resistance Lung complianceLung compliance Lung elasticityLung elasticity Alveolar surface tension forcesAlveolar surface tension forces

Respiratory passage resistanceRespiratory passage resistance
Resistance due to Resistance due to increased friction as increased friction as air moves through air moves through passagespassages Smooth muscle Smooth muscle
bronchoconstriction bronchoconstriction Disorders such as Disorders such as
asthmaasthma – when – when bronchi constrict bronchi constrict
Local accumulations Local accumulations of mucus, infectious of mucus, infectious material, and tumors – material, and tumors – also block air passagealso block air passage

Asthma Asthma

Lung complianceLung compliance
The ease with which lungs can readily The ease with which lungs can readily expandexpand
Affected by the elasticity of the lungs and Affected by the elasticity of the lungs and the thoracic cage which can be diminished the thoracic cage which can be diminished by 2 main factors:by 2 main factors: FibrosisFibrosis of the lung tissue of the lung tissue Ossification and/or muscle paralysis impairs Ossification and/or muscle paralysis impairs
flexibility of the thoracic cageflexibility of the thoracic cage

Lung fibrosisLung fibrosis

Lung ElasticityLung Elasticity
Essential for normal expirationEssential for normal expiration
EmphysemaEmphysema: tissue becomes less : tissue becomes less elastic and more fibrouselastic and more fibrous loss of elasticity & increase in fibrous tissue loss of elasticity & increase in fibrous tissue
causes enormous effort to exhale – at end causes enormous effort to exhale – at end stages, alveolar walls break down and surface stages, alveolar walls break down and surface area is lost for gas exchangearea is lost for gas exchange


Alveolar Surface Tension forcesAlveolar Surface Tension forces
Surface tension is caused by the tendency Surface tension is caused by the tendency of polar molecules such as water to stick to of polar molecules such as water to stick to each other with hydrogen bondseach other with hydrogen bonds
this can cause the walls of the alveoli to this can cause the walls of the alveoli to stick together like plastic wrap every time stick together like plastic wrap every time you exhale.you exhale.
Large amounts of energy /effort will be Large amounts of energy /effort will be required to simply re-expand the lungs and required to simply re-expand the lungs and allow you to inhale (allow you to inhale (IRDSIRDS))

Alveolar Surface Tension ForcesAlveolar Surface Tension Forces
Surfactant – interferes with cohesion of Surfactant – interferes with cohesion of water molecules so less energy needed to water molecules so less energy needed to expand lungs – this is one of the things expand lungs – this is one of the things that keeps our lungs partially expanded at that keeps our lungs partially expanded at all times. (the other thing is the pressure all times. (the other thing is the pressure difference previously discussed)difference previously discussed)
Secreted by Type II cells in lungsSecreted by Type II cells in lungs

Alveoli & Surface TensionAlveoli & Surface Tension

IRDSIRDS – Infant Respiratory Distress – Infant Respiratory Distress SyndromeSyndrome
AKA: Hyaline AKA: Hyaline Membrane DiseaseMembrane Disease
Caused by lack of Caused by lack of surfactant due to surfactant due to prematurity prematurity
28 weeks of gestation is 28 weeks of gestation is consideredconsidered

Nonrespiratory Air ManeuversNonrespiratory Air Maneuvers
Reaction or reflex responseReaction or reflex response
• Cough Cough
• Sneeze –travels up to 40 miles per hourSneeze –travels up to 40 miles per hour
• Hiccup – phrenic nerve irritation causes Hiccup – phrenic nerve irritation causes diaphragm to spasmdiaphragm to spasm
• Yawn – saturates alveoli with fresh airYawn – saturates alveoli with fresh airNeed for increased oxygenNeed for increased oxygen

Control of BreathingControl of Breathing
NeuralNeural
Medulla oblongata sets rate of breathingMedulla oblongata sets rate of breathing
Pons fine-tunes rate and transition Pons fine-tunes rate and transition

Hering-Breuer ReflexesHering-Breuer Reflexes
Stimulation is sentStimulation is sent
Inflation reflex- prevents overexpansion Inflation reflex- prevents overexpansion via receptors around bronchiolesvia receptors around bronchioles
Deflation reflex – inhibits expiratory centers Deflation reflex – inhibits expiratory centers and stimulates inspiratory centers. and stimulates inspiratory centers.
Receptors in alveolar wallsReceptors in alveolar walls
Usually during forced activityUsually during forced activity

Control of Breathing Chemical Control of Breathing Chemical FactorsFactors
Central chemoceptors monitor pH levels in Central chemoceptors monitor pH levels in cerebrospinal fluid.cerebrospinal fluid.
High levels of CO2 increase hydrogen level in High levels of CO2 increase hydrogen level in blood – therefore pH decreases.blood – therefore pH decreases.
Peripheral chemoreceptors located in aorta and Peripheral chemoreceptors located in aorta and carotid arteries monitor blood oxygen level.carotid arteries monitor blood oxygen level.
Mechanoreceptors located in muscles and Mechanoreceptors located in muscles and joints detect muscle contraction and force joints detect muscle contraction and force increased ventilation.increased ventilation.

Lung VolumeLung Volume
Static Lung VolumeStatic Lung Volume
Instructed to perform following breathing Instructed to perform following breathing maneuversmaneuvers
Tidal volume – amount inhaled during Tidal volume – amount inhaled during normal breathingnormal breathing
Vital capacity – breath in maximum, followed Vital capacity – breath in maximum, followed by maximum expirationby maximum expiration

Lung VolumeLung Volume
Residual volume – Residual volume – volume of air that volume of air that never leaves the never leaves the lungslungs
Important for continual Important for continual gas exchangegas exchange

Lung VolumeLung Volume
Dynamic Lung VolumeDynamic Lung Volume

End of Quiz #2 MaterialEnd of Quiz #2 Material