Embed Size (px)
Citation preview

Acta Chir. Aus t r iaca - Heft 4 • 1998 211
From the Department of Surgery, the *Department of Internal Medicine, Gastroenteroiogy/Hepatology, and the **Department of Radiodiagnostics, Virchow Clinic, Humboldt University, Berlin, Germany
Partial or Total Resection of the Biliary Tract - Surgical Strategies for Hilar Cholangiocarcinoma S. Jonas, W. O. Bechstein, H. Keck, W. Veltzke*, R. Hintze*, T. Vogl**, and P. Neuhaus
Key-words: Biliary tract, partial or total resection - cholangiocarci- noma - surgical strategies.
SchliisselwOrter: Gallenwege, partielle oder totale Resektion - Gal- lengangska~inom - chirurgische Behandlungsstrategien.
Summary: Background: Surgical resection provides the only chance of cure for patients suffering from hilar cholangiocarci- noma. Although appropriate procedures are not agreed upon, an increase in radicality has been observed during the past 20 years. Methods: The literature as well as our own experience after 80 resections of hilar cholangiocarcinomas were reviewed retro- spectively. Results: Tumor-free margins represent the most important pro- gnostic parameter. Hilar resections as least radical resective procedure will generate rates of formally curative resections of less than 50%. Curative resection and 5-year survival rates after additional hemihepatectomy generally do not exceed 65% and 25% in the more promising reports, respectively, in our series, the best 5-year survival rate was achieved after right trisegmen- tectomy with 59%. After conventional liver transplantation, 5-year survivors can only exceptionally be observed. Although extended bile duct resection or abdominal organ cluster trans- plantation may significantly increase the rate of formally cura- tive resections, long term survival is still disappointing. Conclusions: In our hands, right trisegmentectomy will provide the most pronounced benefit, if this procedure is applicable with respect to tumor extension and functioning hepatic reserve. Extended bile duct resections cannot be evaluated definitely at this stage. However, patterns of recurrence clearly demonstrate the need for adjuvant treatment protocols.
(Acta Chir. Austriaca 1998;30:211-214
PartieUe oder totale Resektion tier Gallenwege - ch i rur - gische Behandlungss t ra tegien beim zent ra len Gallen- gangskarz inom Zusammenfassung: Grundlagen: Resektionen stellen die einzi- gen potentiell kurativen Therapieoptionen beim zentralen Gal- lengangskarzinom dar. In den vergangenen 20 Jahren konnte eine Zunahme der Radikalitfit in der chirurgischen Therapie beobach- tet werden, ohne dag einheitliche Therapiekonzepte bestfinden.
Methodik: Retrospektive Untersuchung der Literatur sowie un- serer eigenen Erfahmng nach 80 Resektionen zentraler Gailen- gangskarzinome.
Ergebnisse: Formal kurative Resektabilit~,t stellt den wichtig- s~en Prognosefaktor dar. Hilusresektionen als Verfahre~ mit der geringsten Radikatit~it sind in weniger als 50% der F~ille formai kurativ. Die Raten formal kurativer Resektionen sowie des 5-Jah- res-Uberlebens nach zustitzlicher Hemihepatektomie tibersteigen auch in giinstigeren Serien in der Reget 65% bzw. 25% nicht. Im eigenen Krankengut wurde mit 59% die h/3chste 5-Jahres-15ber- lebensrate nach rechtsseitiger Trisegmentektomie beobachtet. Nach konventioneller Lebertransplantation kommt es nur in Aus-
Corresponding address: S. Jonas, M.D., Department of Surgery, Virchow Clinic, Humboldt University, Augustenburger Platz 1, D-13353 Berlin, Germany. Fax: ++49/30/450- 52900 E-mail: [email protected]
nahmef~illen zu einem Langzeittiberleben. Erweiterte Gallen- gangsresektionen sowie auch abdominelle ,,Cluster-Transplanta- tionen" ktinnen zwar die Rate formal kurativer Resektionen si- gnifikant steigern, fiJhren aber nicht zu einer h6heren 5-Jahres- Uberlebensrate.
Schlul3folgerungen-- Nach unserer Erfahrung krnnen die gtin- stigsten Ergebnisse nach Trisegmentektomien beobachtet wer- den, wenn Tumorausmat3 oder Parenchyrnreserve diese Verfah- renswahl zulassen. Erweiterte Gallengangsresektionen krnnen derzeit nicht abschliel3end beurteilt werden. Das Rezidivmuster verdeutlicht die Notwendigkeit adjuvanter Therapieans~itze.
In t roduct ion
Surgical strategies in the therapy of hilar cholangiocarcinoma afford patients the best chance for significant survival. Radi- cal resections are currently considered as optimal treatment. but less than 20% of patients are estimated to be amenable to a formally curative approach (9, 11). Although these tumors usually have a low propensity for metastases and tend to grow slowly, curative attempts are impaired by a longitudinally and laterally advanced local infiltration, as the diagnosis is gene- rally not made until a patient is jaundiced (7, 39). The deter- gent properties of bile facilitate its passage through tiny gaps in an obstructed lumen long before it becomes clinically appa- rent (31).
The type of growth provides another condition for technically difficult or even impossible resections in the vicinity of vital hilar structures. The nodular type with a well demarcated tumor is ra- rely found in cholangiocarcinoma and a fibrous capsule, which can frequently be detected in hepatocellular carcinoma, is almost always absent. Conversely, the periductal type, with infiltration and proliferation along thickened bile duct walls with minimal mass formation, is exclusively observed in the hilar type of cholangiocarcinoma (13, 38). The resection rate of this subset of tumors approximates only 10%. Apart from a local spread via lymphatic vessels, microscopic tumor extension can inde- pendently be observed through perineural spaces, predomi- nantly in hepatofugal direction due to the intrahepatic narro- wing of the perineurium (6, 41). Thereby, the already difficult diagnosis of hilar cholangiocarcinoma including its differen- tiation from benign fibrosing diseases at the hepatic confluen- ce, especially primary sclerosing cholangitis, primary biliary cirrhosis and Caroli's disease, is further complicated by an even intraoperatively hardly definable tumor extension, which may easily reach beyond its palpable confines. Moreover, hi- stologic carcinomatous invasion of surrounding vessels may occur, but is less common and macroscopically indistinguishable from adherence and perivascv.ia- fibrosis (2).
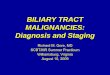
Fig. l. Modified Bismuth-Corlette classification ofhilar cholangiocar- cinoma according to the tumor extension at the bifurcation of the biliam., tree.

212 Acta Chir. Austriaca. Heft 4 . 1998
Table 1. Pattern of cholangiocarcinoma recurrence after formally curative hilar resections (according to [25]).
Site of recurrence Overall frequency of recurrence
Liver 62%
'Tumor bed 42%
Regional lymph nodes
Peritoneum
Lungs
Bone
Subcutaneous tissue
20%
16%
71%
31%
7%
Frequency of primary recurrence
76%
24%
Loca l r e s e c t i o n
The type of resection that may be indicated for hilar cholangio- carcinoma depends on the site and extent of the tumor. The loca- tion of a carcinoma within the biliary tree and its relation to the hepatic confluence is practically standardized in the modified Bismuth-Corlette classification (Fig. 1).
Local or hilar resections including the extrahepatic, suprapan- creatic biliary tract represent the least extended resective proce- dures and have been shown to be safe, the operative mortality rate being even less than 1% in selected series (4). Theoretically, patients suffering from Bismuth-Corlette type I or type II tumors could undergo hilar resections in a curative intent. However, the pattern of failure after formally curative extrahepatic bile duct re- sections demonstrated a high percentage of patients (76%) with locoregional recurrence (25). Distant metastases developed in most patients exhibiting a locoregional recurrence but were the site of first failure in only 24% (Table 1). The liver was identified as the most frequent site of recurrence, either by direct parenchy- real invasion or along the segmental duct draining the caudate lobe (segment 1) (26). A 97% rate of segment 1 ramifications at the hepatic confluence or within a distance of less than 10 mm into the main left or right hepatic duct is likely to result in an early tumor involvement and led to the postulate to generally in- clude caudate lobe resections into the surgical strategy, if cure is intended (5, 20, 27).
Patient longevity after hilar resection remains poor and single- center experiences achieving 5-year-survival rates of 30% have to be considered as favorable (12, 32). Moreover, it could not be demonstrated that an additional caudate lobe resection had a be- neficial impact on survival (26, 32). Prime targets of tumor recur- rence were still locoregional within the former tumor bed, liver parenchyma and pancreatic lymph nodes.
L i v e r r e s e c t i o n
Resections are considered curative if tumor-free margins are ob- tained on pathologic examination of a resected specimen. The true extent of a periductular infltrating carcinomatous lesion cannot be recognized by the surgeon and even pathologic deter- mination of intraoperative frozen-section biopsies may be diffi- cult, especially in the setting of concomitant cholangitis, hepato- lithiasis or biliary obstruction. Retrospective analyses of speci- mens from hilar resections showed tumor-free margins in less than 50% of the patients, concluding an increased risk of residual cancer after hilar resections when compared to additional liver resection (2). Therefore, adequate clearance and the chance of long-term survival may only be preserved after hepatic resections (5, 20, 33, 42).
Hilar cholangiocarcinomas involving either the right or left he- patic duct (Bismuth-Corlette types IIIa/IIIb) are generally propo- sed to require resection of the respective hemiliver in order to achieve cleared margins. Recent studies on prognostic parame- ters after resection identified only tumor-free margins as a com- mon predictor of postoperative survival in multivariate analyses, while histopathologic differentiation and tumor-stage showed a clear correlation only in single studies (32, 37). The improved equipment and understanding of techniques requisite for liver surgery allow performance of extended resections without major concessions to perioperative safety. In a French multicentric sur- vey of 278 patients suffering from hilar cholangiocarcinoma, pe- rioperative mortality was highest after surgical exploration (58%) or palliative decompression by transtumoral intubation (27%) and biliary digestive anastomosis (26%) (35). The mortality rates after resective surgery were significantly lower with 17% after local resections and 14% after hepatectomies, which in part may have been due to the fact that many of the participating institu- tions treated only few patients while the majority of hepatecto- mies was performed in centers. In addition, these results also re- vealed a selection of patients with more favorable tumor stages for major surgery. In our experience, hepatic resections of hilar cholangiocarcinoma had a postoperative mortality of 10% which is reflected in other recently reported series of experienced cen- ters (22, 32, 37).
Combined tumor and hepatic resections could increase not only the rate of curative resections which in our experience of 80 resected hilar cholangio¢arcinomas rose from 44% after hilar re- sections to 65% after additional hepatic resections but also the
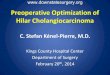
Fig. 3. CT scan 1 month after decompression of the left hepatic duct and embolization of the right hepatic arte~ showing atrophy of the right and hypertrophy of the left hemiliver. The radiologic density of the right segments has decreased following arterial embolization.
Fig. 2. Endoscopic retrograde cholangiography showing dilation of the left biliar 3' system in a patient suffering from hilar cholangiocar- cinoma (~,pe llla according to the modified Bismuth-Corlette classi- fication). Prior to right trisegmentectomy, left hepatic hypertrophy and right hepatic atrophy are induced b.v decompression of the left hepatic duct via transhtmoral stenting and embolization of the right hepatic arte~, by angiographically inserted platinum coils (arrows). The long distance between obstracted confluence and ramification of the left lateral segments is obvious, allowing for a wide rumor-free resection margin.

Acta Chir. Aust r iaca • Heft 4 • 1998 213
total number of patients amenable to surgery. Over the long term, these surgical approaches could not be associated with favorable survival figures, although a number of survivors are reported in many series. 5-year survival rates range from 40% in the most optimistic reports to 10% in other accounts (22, 29, 30, 32, 37, 43).
In our series, the most favorable outcome was observed among the subset of patients undergoing right trisegmentectomy. The rate of formally curative resections in this group was 75% (9 of 12 patients) with a 5-year survival rate of 59%. Although only 1 tumor in this group presented with a poor histopathological dif- ferentiation, anatomical considerations may as well account for this superior figure. With respect to the hepatic hilum, a more distant segmental ramification of the left hepatic duct which va- ries in size from 1 to 5 cm is likely to allow more radical right- sided than left-sided resections. Conversely, the anterior and po- sterior right ducts, which are formed by the segmental ducts 5/8 and 6/7, respectively, combine at a confluence constituting the right hepatic duct which rarely exceeds a length of 1 cm (10). In addition, the common bile duct is located on the right side of the hepatoduodenal ligament with the right hepatic artery behind its proximal portion. In order to comply with the basic principle of surgical oncology to achieve wide tumor-free margins, it may be appropriate to perform right trisegmentectomies even for some hilar cholangiocarcinomas infiltrating the left hepatic duct.
The main obstacle to this approach is frequently represented by the preoperative anticipation of a limited functioning hepatic remnant due to the small size of the left lateral segments in some patients or to an insufficient postoperative compensatory enlar- gement due to cholestasis-associated liver damage. A preoperati- ve hypertrophy of the future remnant liver, induced by unilateral portal vein embolization, has been shown to minimize the asso- ciated risk of postoperative liver failure (24). Decompression of the biliary system may also be indicated to improve hepatocellu- lar function. Former randomized trials did not demonstrate an ad- vantage associated with preoperative external biliary drainage (17). However, older studies mainly comprised bypass surgery and suffer from a low share of hepatectomies. We use a modified approach with internal stent decompression of the remnant left lobe and arterial platinum-coil embolization of the fight liver ar- tery (Fig. 2). In our experience, insidious arterial embolization by coiling is comparable to portal embolization with respect to safe- ty and extent of contralaterally induced hypertrophy (Fig. 3). Moreover, the deleterious effects of a decreased arterial supply to bile ducts are well-known from ischemic type biliary lesions (ITBL) after liver transplantation and may be more appropriate as an antitumoral concept than portal embolization.
Total hepatectomy Unresectable tumors and functional restrictions, but also the as- sumption that greater exstirpative procedures might provide an increased chance for cure, resulted in the more radical concept of resecting the entire intrahepatic biliary tree by combining hilar resection, total hepatectomy and liver transplantation. Arguments in favor of this approach included a putative rise in rates of for- mally curative resections, the simultaneous therapy of underlying or associated diseases, e.g. primary sclerosing cholangitis, as well as the prevention of de novo and recurrent tumors, since multifocal lesions within the biliary tract may be identified in as many as 10% of patients (16). Moreover, tumor stage and poly- centricity are likely to be assessed with higher reliability by hi- stopathological staging after total hepatectomy when compared to radiological visualization of the hepatic remnant after partial resections.
Postoperative mortality was even expected to decrease as liver transplants in a patient population not suffering from complica- ting portal hypertension can be performed rather straighttbrward. However, postoperative and long term survival figures have been disappointing. In a review of 56 patients originating from 13 stu- dies, 90-day mortality and 5-year survival rates after total hepa- tectomy and liver transplantation for hilar cholangiocarcinoma
were approximately 25% and 5%, respectively (14). Cancer re- currence predominated as cause of death in 85% of the patients surviving more than 90 days posttransplant. Many of these pa- tients underwent operation in the 1980s, when the initial surgical endeavour was made to establish liver transplantation as a wide- spread treatment option for liver diseases in general. Therefore, postoperative mortality rates are likely to be cut at least in half some ten years later. However, the major obstacle to patient lon- gevity remains the unpredictable risk caused by a potentially ac- celerated growth of residual tumor cells during chronic immuno- suppression, which has been shown after hepatectomy and liver transplantation for hepatocellular carcinoma (44).
Another lesson learned from liver transplantation for hepato- cellular carcinoma in cirrhosis is that the formerly adopted attitu- de to resect when resection is feasible and perform transplanta- tion for those tumors being unresectable represented a complete misconception. If successful outcome is observed posttransplant, it will be in patients suffering from resectable lesions, whereas total hepatectomy and liver transplantation will not confer a sur- vival benefit to those suffering from otherwise unresectable he- patocellular carcinomas (8, 21). At least, the latter principle may hold true for hilar cholangiocarcinoma as well, while a poor pro- gnosis is not an exception but the rule in the small subset of pa- tients in whom diagnosis of a hilar cholangiocarcinoma is made at an early stage or incidentally (15, 32). Therefore, most trans- plant centers have abandoned the policy to consider hilar cholan- giocarcinomas as an indication for liver transplantation.
To t a l r esec t ion of the b i l i a ry t r a c t 3 mechanisms are likely to serve as an explanation for long term failure after total hepatectomy and liver transplantation for hilar cholangiocarcinoma: unrecognized distant metastases, intra- or preoperative tumor cell seeding, e.g. via biopsy needle tracts, and peripancreatic tumor extensions in lymphatic vessels or perineu- ral sheathes along the distal residual bile duct.
Nodal infiltration may occur in as many as one-third of patients whereas blood born metastases are distinctly unusual (23, 40). Indeed, careful follow-up frequently disclosed postoperative fai- lure of tumor control with recurrence at the pancreatic head and local peritoneal carcinosis (3). Therefore, it may be doubted that distal radicality can be achieved by partial bile duct resections, all the more considering tumor-free margins of less than 10 mm, which are not uncommon in oncological biliary surgery, as insuf- ficient for all other gastrointestinal cancers. Similarly, intraabdo- minal tumor seeding probably confronts the surgeon with an even more important problem, as it is common practice in some cen- ters to establish tumor diagnosis by open biopsies. Dissection of tumor or peritumor is considered obsolete for other carcinomas. In rectal cancer for example, not only perforation of the tumor but even dissection of the mesorectum, which is considered a "holy plane", has been identified as main reason for local recur- rence (18, 19). The "holy plane" in oncological surgery of the ex- trahepatic biliary tract may be represented by the hepatoduodenal ligament which is regularly dissected during preparation of the hepatic artery and portal vein for conventional liver transplanta- tion.
In order to comply with these roles of oncological surgery, we have described the "extended bile duct resection", i.e. en bloc eradication of the entire biliary ~ee by a no-touch technique com- bining total hepatectomy, partial pancreatoduodenectomy, exten- ded lymphadenectomy and liver transplantation (28). Moreover, an attempt was made to select patients suffering from less advan- ced tumors, because it is known from other cancers that there is limited chance of cure at an advanced stage even if the surgical technique is excellent.
In spite of an attempted selection, only 4 of 14 patients presen- ted with UICC I/II tumors (UICC IVa: n -- 9; UICC IVb: n = 1). After 14 extended bile duct resections, formally curative resec- tions were achieved in all but 1 patient, in whom a metastasis at the right ovary was not apparent until the procedure had already reached an irreversible stage. During the postoperative course, 2

214 Acta Chir. Austriaca. Heft 4 -1998
patients (14%) were lost due to complications associated with the pancreatic tail. After a change in the protocol to administer oc- treotide routinely, we did not observe any more severe complica- tions. Currently, the 4-year survival rate including the postopera- tive mortality is 30%. An analysis of the late failures disclosed implantation metastases in about half of the patients with tumor recurrence. The pathway is not fully apparent, though an exfolia- tion of tumor cells into the bile running freely into the operative field via gastric or jejunal succus, is likely to be operative.
Comparably disappointing results are reported after abdominal organ cluster transplantation performed by Starzl et al. in Pitts- burgh (1, 36). This procedure was designed to resect the whole complexity of visceral organs deriving during embryonal life from the portion of the foregut which later in life differentiates into duodenum, liver and pancreas. In the subset of patients suf- fering from cholangiocarcinoma, postoperative mortality and 5- year survival rates were 20% and 14%, respectively. Most of the- se patients underwent additional transplantation of the pancreas and all postoperative fatalities could be related to the pancreatic graft. Transplantation of the liver alone was advocated for some patients despite creating a hardly adjustable diabetes mellitus, in order to avoid the considerable morbidity and mortality associa- ted with the pancreas graft.
Conc lus ions Even highly extended resective procedures do not achieve the ex- pected survival benefit in the treatment of hilar cholangiocarci- noma, although the observed advantage after formally curative resections can be confered to a significantly increased share of patients. The pathways of recurrence are not fully investigated, but clearly demonstrate the need for adjuvant treatment proto- cols. So far, chemotherapy and radiation have failed to contribute to improved survival figures (34).
In our hands, right trisegmentectomy will provide the most pronounced benefit, if this procedure is applicable with respect to tumor extension and functioning hepatic reserve. Extended bile duct resections cannot be evaluated definitely at this stage and must be applied with considerable caution regarding tumor seeding. As most issues concerning an optimal treatment of hilar cholangiocarcinoma remain unsolved, it should be emphasized that the evaluation of these patients has to be concentrated in spe- cialized institutions.
Refe rences (1) Alessiani M, Tzakis A, Todo S, Demetris A J, Fung JJ, Starzl TE: Assessment of five-year experience with abdominal cluster transplantation. J Am Coil Surg 1995;180:1-9. (2) Beazley RM, Hadjis N, Benjamin IS: Clinicopathological subjects of high bile duct cancer: experience with resection and bypass surgical treatments. Ann Surg 1984; 199:623-636. (3) Beckurts KTE, H61scher AH, Bauer TH, Siewert JR: Maligne Tumoren der Hepaticusgabel - Ergehnisse der chimrgischen Therapie and Prognosefaktoren. Chirurg 1997;68:378-384. (4) Bengmark S, Blumgart LH, Launois B: Liver resection in high bile duct tumors, in Bengmark S, Blumgart LH (eds): Liver surgery. Edinburgh, Churchill Livingston, t986, pp 81-87. (5) Bengmark S, Ekberg H, Evander A, Klofver-Stahl B, Tranberg KG: Major liver resection for hilar cholangiocarcinoma. Ann Surg 1988;207:120-125. (6) Bhuiya MR, Nimura Y, Kamiya J, Kondo S, Fukata S, Hayakawa N, Shionnya S: Clinicopathnlogic studies on perineural invasion of bile duct carcinoma. Ann Surg 1992;215:344-349. (7) Bismuth H, Castaing D, Traynor O: Resection or palliation: priority of surgery in the treatment of hilar cancer. World J Surg i988;12:39-47. (8) Bismuth H, Chiche L, Adam R, Castaing D, Diamond T, Dennison A: Liver resection versus transplantation for hepatocellutar carcinoma in cirrhotic patients. Ann Surg 1993;218:145-151. (9) Bismuth H, Nakache R, Diamond T: Management strategies in resection for hilar eholangiocarcinoma. Ann Surg 1992;215:31-38. (i0) Bismuth H: Surgical anatomy and anatomical surgery of the liver. World J Surg 1982;6:3-9.
( I 1 ) Blumgart LH, Benjamin IS: Liver resection for bile duct cancer. Surg Clin North Am 1989;69:323-337. (12) Childs T, Hart M: Aggressive surgical therapy for Klztskin tumors. Am J Surg 1993;165:554-557. (13) Colombari R, Tsui WMS: Biliary tumors of the liver. Semin Liv Dis 1995;15:402-413. (14) Curley SA, Levin B, Rich TA: Management of specific malignancies: liver and bile ducts, in Abeloff MD, Armitage JO, Lichter AS, Niederbuber JE (eds): Clinical Oncology. New York, Churchill Livingstone, 1995, pp 1305-1372. (15) Delcore R, Eisenach JE, Payne KM, Bhatia P, Forster J: The risk of occult carcinomas in patients undergoing orthotopic liver transplantation for end-stage liver disease secondary to primary sclerosing cholangitis. Transplant Proc 1983;23:1883- 1884. (16) Gertsch P, Thomas P, Baer H, Lerut J, Zimmermann A, Blumgart H: Multiple tumors of the biliary tract. Am J Surg 1990;158:386-388. (17) Hatfield ARW, Tobias R, Terblanche J, Girdwood AH, Fataar S, Hat-ties-Jones R, Kernoff L, Marks IN: Preoperative external biliary drainage in obstructive jaundice: a prospective controlled clinical trial. Lancet 1982;11:896-899. (18) Heald RJ, Ryall R: Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1986;I:1479-1482. (19) Heard RJ: The "holy plane" of rectal surgery. J Roy Soc Med 1988;81:503-508. (20) Iwasaki Y, Okamura T, Ozaki A, Todoroki T, Takase Y, Ohara K, Nishimura A, Otsu H: Surgical treatment for carcinoma at the confluence of the major hepatic ducts. Surg Gynecol Obst 1986;162:457-464. (21) Jonas S, Bechstein WO, Kling N, Guckelberger O, Neuhaus P: Therapie des prim~en hepatozellul~'en Karzinoms. Dtsch Med Wschr 1997; 122:617-620. (22) Jonas S, Bechstein WO, Kting N, Neuhaus P: Das Resektionsausmag in der chirurgischen Therapie zentraler Gallengangskarzinome. Langenbecks Arch Chir Suppl 1997;2:1075-1077. (23) Kirshbaum JD, Kosoll DD: Carcinoma of the gallbladder and extrahepatic bite ducts. Surg Gynecol Obstet 1941 ;93:740-754. (24) Makuuchi M, Thai BL, Takayasu K, Takayama T, Kosuge T, Gunven P, Yamazaki S, Hasegawa H, Ozaki H: Preoperative portal embolization to increase safety of major hepatectomy for hilar bile duct carcinoma: a preliminary report. Surgery 1990;107:521-527. (25) Mittal B, Deutsch M, Iwatsuki S: Primary cancers of the extrahepatic biliary passages. Int J Radiat Oncol Biol Phys 1985; 11:849-855. (26) Mizumoto R, Kawarada Y, Suzuki H: Surgical treatment of hilar carcinoma of the bile duct. Surg Gynecol Obst 1986; 162:153- t 58. (27) Mizumoto R, Suzuki H: Surgical anatomy of the hepatic hilum with special reference to the caudate lobe. World J Surg 1988;12:2-10. (28) Neuhaus P, Blumhardt G: Extended bile duct resection - a new oncological approach to the treatment of central bile duct carcinomas? Description of method and early results. Langenbecks Arch Chir 1994;379:123-128. (29) Nimura Y, Hayakawa N, Kamiya J, Kondo S, Shionoya SH: Hepatic segmen- tectomy with caudate lobe resection for bile duct carcinoma of the hepatic hilus. World J Surg 1990;14:535-544. (30) Nimura Y, Hayakawa N, Kamiya J, Maeda S, Kondo S, Yasui A, Shionoya S: Hepatopancreatoduodenectomy for advanced carcinoma of the biliary tract. Hepato- gastroenterology 1991;38:170-175. (31) Okuda K, Kubo Y, Okazaki N, Arishima T, Hashimoto M: Clinical aspects of intrahepatic bile duct carcinoma including ,hilar carcinoma: a study of 57 autopsy- proven cases. Cancer 1977;39:232-246. (32) Pichlmayr R, Weimann A, Klempnauer J, Oldhafer KJ, Maschek H, Tusch G, Ringe B: Surgical treatment in proximal bile duct cancer. A single-center experience. Ann Surg 1996;224:628-638. (33) Pinson CW, Rossi RL: Extended right hepatic lobectomy, left hepatic lobectomy, and skeletonization resection for proximal bile duct cancer. World J Surg 1988; 12:52- 59. (34) Pitt HA, Nakeeb A, Abrams RA, Coleman J, Piantadosi S, Yet C J, Lillemoe KD, Cameron JL: Perihilar cholangiocarcinoma. Postoperative radiotherapy does not improve survival. Ann Surg 1995;221:788-798. (35) Reding R, Buard JL, Lebeau G, Lannois B: Surgical management of 552 carcinomas of the extrahepatice bile ducts (gallbladder and periampullary tumors excluded). Results of the French association survey. Ann S urg 1991 ;219:236-241. (36) Starzl TE, Todo S, Tzakis A, Podesta L, Mieles L, Demetris A, Teperman L, Selby R, Stevenson W, Stieber A, Gordon R, Iwatsuki S: Abdominal organ cluster transplantation for the treatment of upper abdominal malignancies. Ann Surg 1989;210:374-386. (37) Su CH, Tsay SH, Wu CC, Shyr YM, King KL, Lee CH, Lui WY, Liu TJ, P'eng FK: Factors influencing postoperative morbidity, mortality, and survival after resec- tion for hilar cholangiocarcinoma. Ann Surg 1996;223:384-394. (38) Sugihara S, Kojiro M: Pathology of cholangiocarcinoma, in Okuda K, Ishak KG (eds): Neoplasms of the liver. Tokyo, Springer, 1987, pp 236-30 l. (39) Suzuki M, Takahashi T, Ouchi K, Matsuno S: The development and extension of hepatohilar bile duct carcinoma. Cancer 1989;64:658-663. (40) Tsuzuki T, Ogata Y, Iida S, Nakanishi I, Takenaka Y, Yoshii H: Carcinoma of the bifurcation of the hepatic ducts. Arch Surg 1983; 118: l 147-t 151. (41) Weinbren K, Mutum SS: Pathological aspects of cholangiocarcinoma. J Pathol !983;I39:217-238. (42) White TT: Skeletization resection and central hepatic resection in the treatment of bile duct cancer. World J Surg 1988;12:48-51. (43) Yet CJ, Pitt HA, Cameron JL: Cholangiocareinoma. Surg Clin North Am 1990;70:1429-1447. (44) Yokoyama I, Cart B, Saitsu H, Iwatsuki S, Starzl TE: Accelerated growth rates of recurrent hepatocellular carcinoma after liver transplantation. Cancer 199!;68: 2095-2100.