Embed Size (px)
Citation preview

Particularities of Treating HIV Positive Women
Latin American and Caribbean HIV Symposium March 1-2, 2013
Dr. Isabel CassettiHelios Salud
Buenos Aires-Argentina

Outline
• Clinical Case Discussion
• Gender Differences
• Particularities of Treating HIV Positive Women

Case 1. ART Naive Patient
• 42 year old woman, HIV positive since 1997, through heterosexual trasmission
• No symptoms for many years• No HCV neither HBV• Her physician recommended to start therapy when
her CD4 count fell < 350 cells/mm3, but she refused to do so
• In March 2010 she iniciated treatment. CD4 count: 240 cells/mm3 (15%) and VL: 320000 c/ml (5.2 log)

• March 2010 : She started HAART with AZT+3TC+ATV/r, but 9 days later she developed rash. The treatment was discontinued and later switched to AZT+3TC+LPV/r
• In April, after 2 weeks on this regimen, she started having mild nausea and diarrhea
• Three months later the treatment was changed to AZT+3TC+EFV. However, dreams, nightmares and dizziness, became frequent

Date CD4 cells/mm3(Abs, %)
RNA-HIV 1 Viral Load(c/ml, log)
Antiretroviral Treatment
1997 560 (29%) 35.200 (log 4.2)
March/ 2010 240 (15) 320.000 (5.2) AZT+3TC+ATZ/rDay 10 th: rash, stop ARV´s
April/2010 AZT+3TC+LPV/rGI intolerance. 3 months later stop therapy
Sep/2010 210 (13) 360.000 (5.4) AZT+3TC+EFZDizziness, nightmares. Mild GI intolerance
Dec/2010 Stop ARV´s

• HIV Resistance Test: no resistance mutations• HIV Tropism Test: Virus CCR5 tropic
• What treatment would you recommend at this point?

What treatment would you recommend at this point?
1. TDF/FTC or 3TC + DRV/r2. ABC/3TC + FPV/r 3. TDF/FTC or 3TC + RAL4. AZT/3TC + MVC

Date CD4 cells/mm3(Abs y %)
RNA HIV 1 Viral Load(c/ml, log)
AntiretroviralTreatment
Jan/2011 195 ( 12 %) 360.000 (5.4) TDF/FTC+RAL
April /2011
Oct/2011
290 (16%)
350 (21)
1400 (3.2)
<20 (<1.5)
Feb/2012 420 (25) <20
Jul/2012 510 (28) <20
Oct/2012 590 (31) <20
Jan 2013 650 (34) <20

Women and ART Complications/Adverse Effects
Compared to Men:
• Women seem to be overall, at higher risk of ART-associated complications
• Women are more likely to discontinue or change their ART regimen because of treatment-related side effects
• Women seem to experience different GI side effects than men: (more nausea and less diarrhea)
• Women seem to present increased levels of serum triglycerides, leptin and low-density lipoprotein cholesterol
Aziz M and Smith K. Current HIV/AIDS Rep, 2012, 9:171-178

Adverse Reactions to Antiretroviral Therapy More Common in Women
NRTIs• Lactic Acidosis• Reaction to ddI: 2.7 times higher (RR:2.7,p:0.03)• Hepatotoxicity and AZT associated anemia
NNRTIs• NVP: Severe rash and more discontinuation (3-5 times greater)
– Hepatitis: particularly with CD4 counts > 250. Severe hepatic failure was seen, causing mortality, concluding that NVP in female patient with elevated CD4 counts is discouraged
Ofotokun I. and Pomeroy C. Topics In HIV Med, 2003 Mar/Apr. Aziz M and Smith K. Current HIV/AIDS Rep, 2012, 9:171-178

Women Adverse Reactions to Antiretroviral Therapy
PIs:– More prevalent in women, including nausea and vomiting
due to intolerance mainly to ritonavir– Women demonstrate more central fat accumulation with
PIs
Integrase Inhibitors:
– To date there is no evidence of sex/gender differences in adverse eventes associated with Raltegravir
Ofotokun I. and Pomeroy C. Topics In HIV Med, 2003 Mar/Apr. Aziz M and Smith K. Current HIV/AIDS Rep, 2012, 9:171-178;

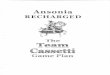
STARTMRK: Time to Discontinuation Due to Adverse Event
Rockstroh J, et al, 19th IAC; Washington, DC; July 22-27, 2012; Abst. LBPE19.
0 16 32 48 60 72 84 96 120 144 168 192 216 2400
2
4
6
8
10
12
14
16
18
20Cu
mul
ative
Dis
conti
nuati
on R
ate
Due
to A
E (%
)
Log-rank P-value = 0.023
Weeks
Raltegravir 400 mg BID
Efavirenz 600 mg QHS
Number of Contributing Patients
282 272 257 254 245 235 221 213 203 200 196 183
281 272 265 262 255 246 236 231 227 223 217 190

Case 2. Recently diagnosed Pregnant Patient
• 24 year old woman, 34 week of pregnancy• Multiple sexual partners, unsafe sex• First visit to a public hospital, with a positive
HIV Elisa test• First pregnancy 3 years ago, HIV negative at
that time, newborn was HIV negative• Not having the confirmatory Western Blot
test, the physician orders the RNA-HIV Viral Load (VL), CD4 count and HIV resistance test

What would you do?
1. Wait the confirmatory WB and VL result before starting therapy2. Start ARV therapy with AZT+3TC+NVP3. Start ARV therapy with AZT+3TC+LPV/r 4. Instuct the patient to return to the clinic when labor begins

• Starting with AZT+3TC+LPV/r, RAL was added to the previous regimen
• The result of baseline VL came 10 days after initiating treatment showing 2.234 c/ml (log 3.3); CD4 count: 334/mm3 (24%)
• Elective C Section was performed at 38 week pregnancy
• HIV VL sample was obtained at delivery• We received the VL results 10 days after delivery:< 50
c/ml (undetectable)• Healthy newborn, received prophylaxis with
AZT+3TC+NVP • Baby´s PCRs: were negative

DHHS Guidelines, February 2013When to Start
Initiating Therapy in Pregnancy Regardless of CD4 count: DHHS, IAS-USA
2012, European, British, Spanish, Latinamerican Guidelines 2012

Antiretroviral Agents and PregnancyNRTI NNRTI PI Entry
InhibitorIntegrase Inhibitor
Recommended LamivudineZidovudine
Nevirapine* Lopinavir/RTVAtazanavir/RTV (2012)
Alternate AbacavirEmtricitabine
Tenofovir‡
Darunavir/RTV (2012)Saquinavir/RTV
Special circumstances
Didanosine(2012) Stavudine (2012)
Efavirenz¶ Indinavir/RTV (2012)Nelfinavir (2012)
Raltegravir
Insufficient data EtravirineRilpivirine
(2012)
Fosamprenavir/RTVTipranavir/RTV
EnfuvirtideMaraviroc
DHHS Perinatal Guidelines. Nov 2012 – Feb 2013
*Not recommended with CD4+ counts > 250 cells/mm3 due to increased risk of hepatotoxicity, unless benefits outweigh risks.‡Recommended to be used in combination with emtricitabine or lamivudine for HIV/HBV coinfection when therapy for HBV is indicated.¶Evidence of human fetal risk; pregnancy category D. May be used after first trimester if other options not available.

http://www.bhiva.org/PublishedandApproved.aspx


Progress Report 2011



ICAAC 2012

1,0
6,0
11,0
16,0
21,0
26,0
31,0
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Mortality From AIDS-related and Non-AIDS-related Deaths
French AL, et al. J Acquir Immune Defic Syndr. 2009.
Women’s Interagency Health Survey (WIHS), N=2792
Non-AIDS DeathsAIDS DeathsAll Deaths
Standardized Mortality Ratios

HIV Integrase Inhibitors Have Different Metabolic Pathways
Drug Metabolism Comment
Raltegravir UGT1A1 Not CYP 3A4 Substrate
ElvitegravirCYP 3A4 - Major
UGT1A1- Minor
CYP 3A4 Inhibition increases bioavailability
and half life
DolutegravirUGT1A1- MajorCYP 3A4 - Minor
Investigational Drug
Raltegravir does not utilize CYP 3A4


Tricot L. et al
Bickel M.et al
Moreno A. et al
Outcome of HCV/HIV-coinfected Liver Transplant Recipients: A Prospective andMulticenter Cohort Study Miró JM et al. Am J Transplant Jul 2012, 12(7): 1866-76

HIV+ Women Experienced Higher Rates of Stress, Depression, and Anxiety Than Their Male Counterparts (N=409)
0123456789
10
Stress Depression Anxiety Family/FriendsEmotionalSupport
Partner EmotionalSupport
Me
an
Sc
ore
s f
or
Ps
yc
ho
log
ica
l We
ll-b
ein
g
HIV+ Men (n=307) HIV+ Women (n=102)
Gordillo V, et al. J Behav Med. Published online June 19, 2009.
P <0.001
P <0.01
P <0.01P <0.05
P <0.05


Curran A. et al. AIDS 2011, 25

VER
• After W24, no statistically differences in any AT (adipose tissue) parameter were observed between women switching to RAL vs continued PI or NNRTI, although a slight decrease in VAT (3.6%) was observed in the RAL group compared to a 1.9% increases in subjects continuing PI or NNRTI
• Statistically significant improvements in median total and LDL cholesterol were observed in subjects switching from PI to RAL
Lake J et al. AIDS Patient Care and STDs, 2012, 26:532-540

Bone loss greater in postmenopausal than premenopausal HIV+ women
Premenopausal
HIV- (N=68)
HIV+ (N=100)
% c
han
ge
in B
MD
/yr
1. Yin et al. JAIDS, 2010. 2. Yin et al JCEM, 2011
Postmenopausal
HIV- (N=58)
HIV+ (N=82)

ART and Risk of Fracture in the Veterans’ Administration HIV Database
Bedimo R, et al AIDS. 2012;26:825-831.

Curran A et al. AIDS 2011
Bloch M et al. Poster 878, CROI 2012

Issues related to HIV women
• Be aware of all the clinical issues • HIV Screening to pregnant woman´s partner• Don´t forget about depression and anxiety. Work
with mental health-care team to try to solve them
• Perform periodical PAP and colposcopy (HPV)• Provide counseling (including family plan and
contraception) • Treatment challenges: competing priorities,
gender norms, domestic violence, economic factors

• Women experience more treatment related complications or adverse reactions, (gastrointestinal intolerance on PIs; psychiatric disorders on EFV)
• Risk for potentially birth defects with EFV (first trimester of pregnancy)
• Reduces the effectiveness of hormone-based contraception
• Depression• Body fat changes• Menopause (aging: renal problems, cardiovascular risk and
bone alterations)
Issues related to womenART Initiation

Could Raltegravir contained regimen be appropriate for women ?
• Favorable tolerability profile (use in patients with tolerability issues on NNRTI and PI regimens)
• Rapid and sustained control of plasma HIV RNA levels for prevention of vertical transmission
• No drug-interactions (´hormonal contraception’)• Good safety profile• Lipid friendly • Potential improvement of lipodystrophy after switching
(further studies need to be confirmed) • Potential beneficial bone effects ( further studies need to be
performed)



Aknowledgements
• Staff Helios Salud: Dra. Claudia Vecchio, Dra. Fernanda Rombini, Dra. Romina Mauas, Dra. Paula Rodríguez
• Dra. Griselda Hernández, Pablo Marotta

Muchas gracias !!!