Embed Size (px)
Citation preview
PARTNER 3 Low-Risk Computed Tomography (CT) Sub-study: Subclinical Leaflet Thrombosis in Transcatheter and
Surgical Bioprosthetic Valves
Raj R. Makkar, MDon behalf of the PARTNER 3 Trial Investigators
Disclosures – Raj Makkar, MDTCT 2019; San Francisco, CA; September 25-29, 2019
Within the past 36 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below.
• Consultant and research grant from Edwards LifeSciences, Abbott, Medtronic, Boston Scientific
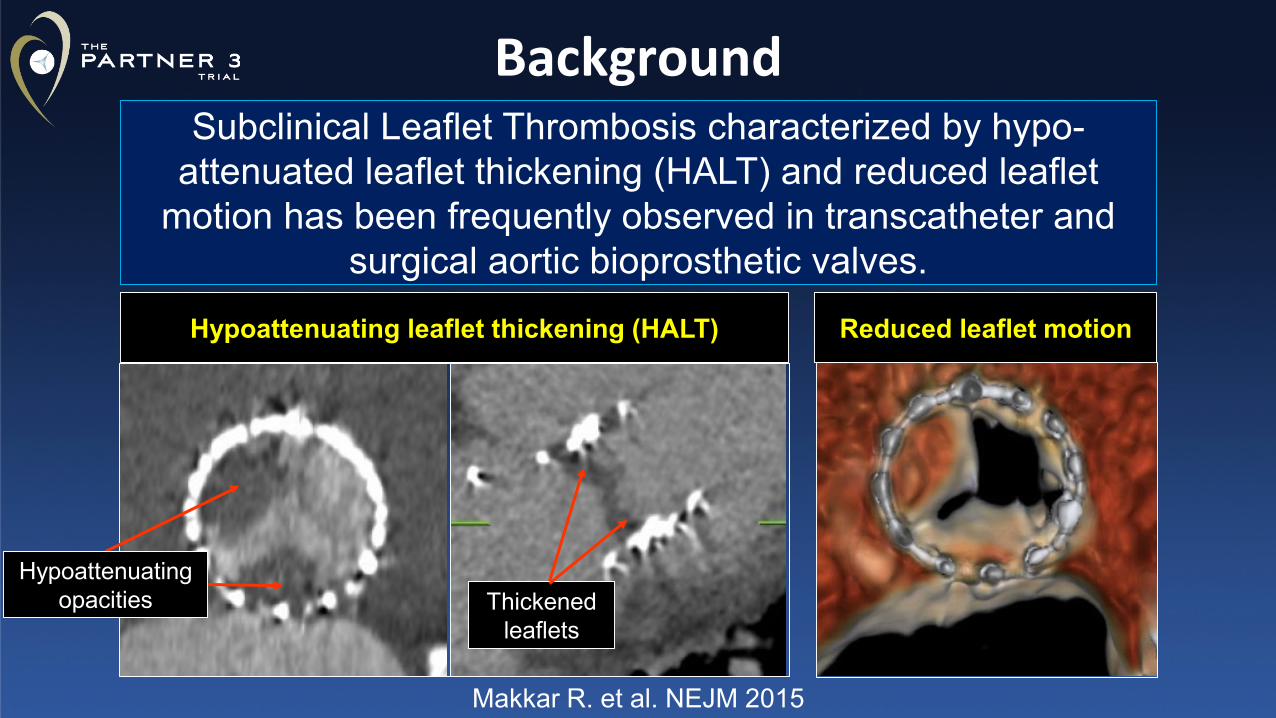
Subclinical Leaflet Thrombosis characterized by hypo-attenuated leaflet thickening (HALT) and reduced leaflet
motion has been frequently observed in transcatheter and surgical aortic bioprosthetic valves.
Background
Reduced leaflet motion
Makkar R. et al. NEJM 2015
Hypoattenuating leaflet thickening (HALT)
Thickened leaflets
Hypoattenuating opacities
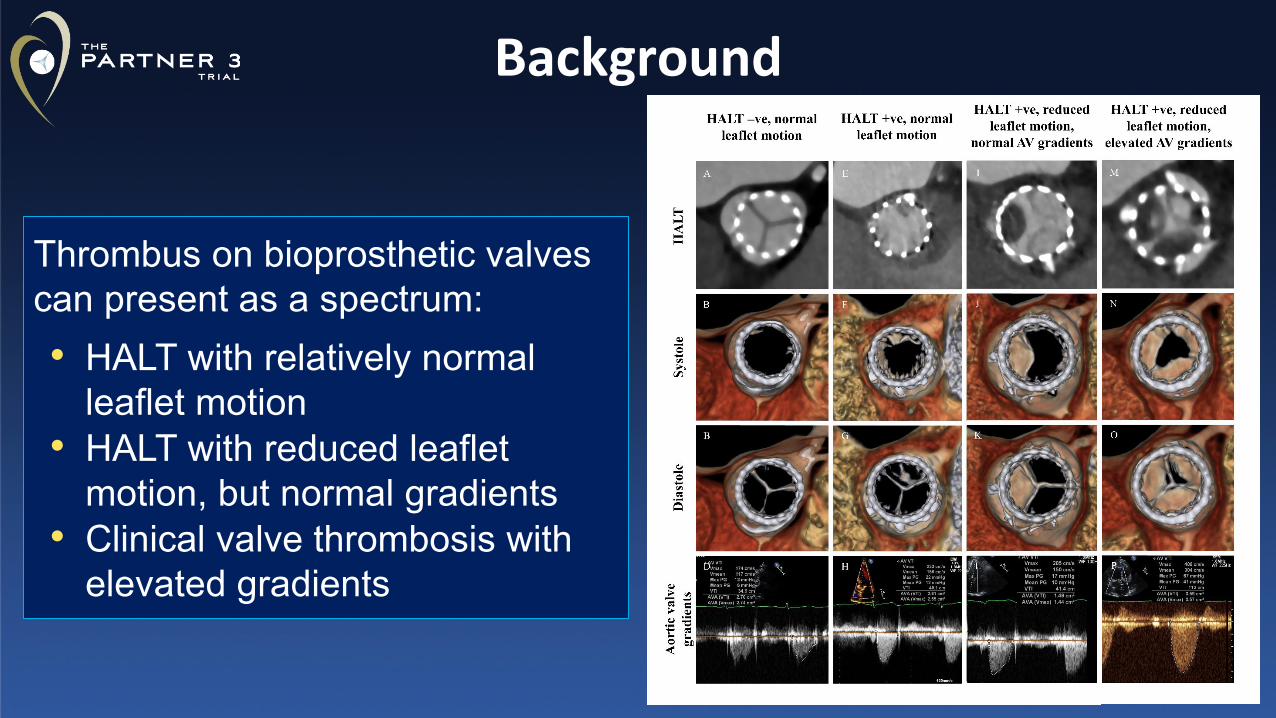
Thrombus on bioprosthetic valves can present as a spectrum:• HALT with relatively normal
leaflet motion• HALT with reduced leaflet
motion, but normal gradients• Clinical valve thrombosis with
elevated gradients
Background
• Randomized trial data on prevalence of Subclinical Leaflet Thrombosis between transcatheter and surgical bioprosthetic aortic valves, its natural history, and impact of this finding on valve hemodynamics and clinical outcomes are lacking.
• PARTNER 3 CT substudy was mandated by the FDA to study this finding in low-risk patients undergoing TAVR with SAPIEN 3 or surgery
Background
Study Objectives
The primary objective of the study was to evaluate HALT and reduced leaflet motion (RLM) in terms of:
• Differences in transcatheter and surgical bioprosthetic aortic valves in a randomized cohort
• Natural history of HALT and reduced leaflet motion in the absence of anticoagulation
• Impact on valve hemodynamics and clinical outcomes
Inclusion Criteria• Eligible for the PARTNER 3 Low-Risk Study• Ability to have a high quality multi-phasic, ECG-Gated CT
scans (i.e., 4D) with contrast
Exclusion Criteria• Condition requiring or planned use of anticoagulants
following index procedure• GFR < 50
Key Entry Criteria
Study Methodology
• Serial CTs at 30 days and 1 year post TAVR or SAVR• All CTs analyzed by a CT corelab blinded to patient
information or time of CTs (Jonathon Leipsic, MD, Philipp Blanke, MD University of British Columbia, Vancouver)
• Treating investigators blinded to the results of 30-day and 1-year CT scans
• Key clinical events were adjudicated by clinical events committee
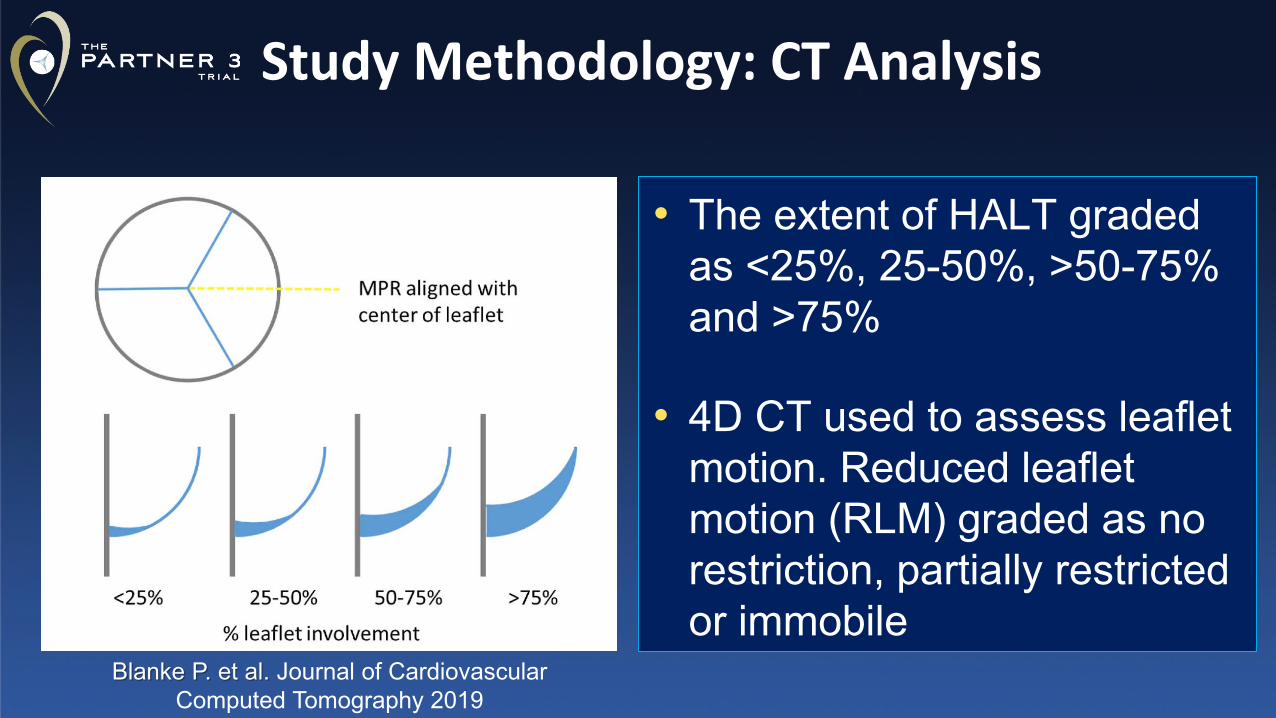
Study Methodology: CT Analysis
• The extent of HALT graded as <25%, 25-50%, >50-75% and >75%
• 4D CT used to assess leaflet motion. Reduced leaflet motion (RLM) graded as no restriction, partially restricted or immobile
Blanke P. et al. Journal of Cardiovascular Computed Tomography 2019
• This was a hypothesis-generating, observational study with no pre-specified statistical analysis plan
• Event rates are binary and p-values (when included) are based on Fisher’s Exact test
• P-values for continuous variables (when included) are based on t-test
Statistical Methods
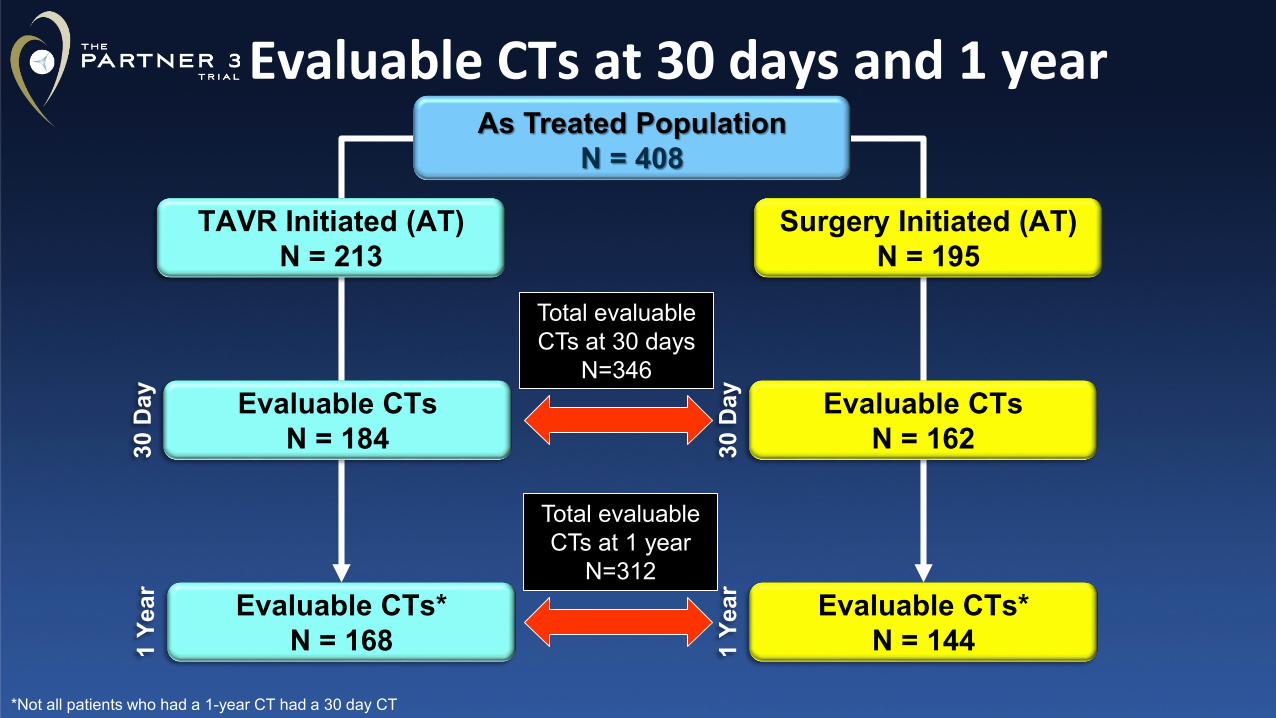
Evaluable CTs at 30 days and 1 yearAs Treated Population
N = 408
TAVR Initiated (AT) N = 213
Surgery Initiated (AT) N = 195
30 D
ay
30 D
ay
1 Ye
ar
1 Ye
ar
Evaluable CTsN = 184
Evaluable CTs*N = 168
Evaluable CTsN = 162
Evaluable CTs*N = 144
Total evaluable CTs at 30 days
N=346
Total evaluable CTs at 1 year
N=312
*Not all patients who had a 1-year CT had a 30 day CT
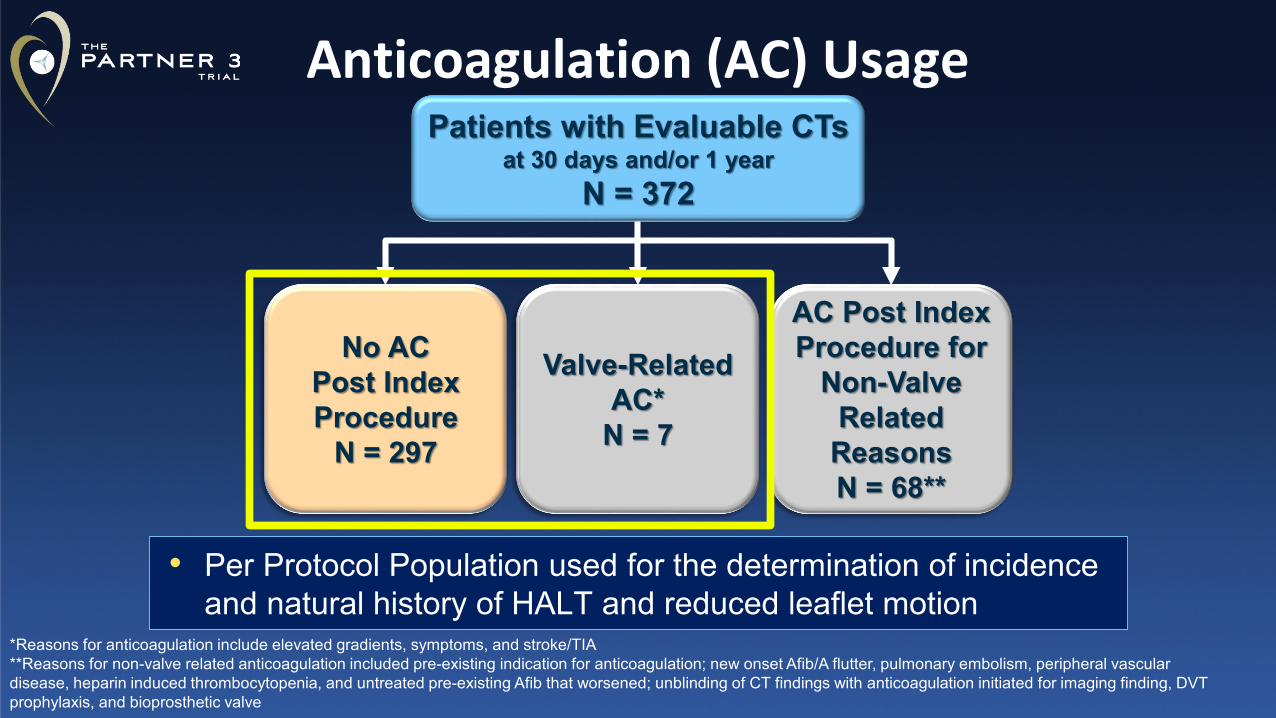
Anticoagulation (AC) Usage
No AC Post Index Procedure
N = 297
Valve-Related AC*
N = 7
*Reasons for anticoagulation include elevated gradients, symptoms, and stroke/TIA**Reasons for non-valve related anticoagulation included pre-existing indication for anticoagulation; new onset Afib/A flutter, pulmonary embolism, peripheral vascular disease, heparin induced thrombocytopenia, and untreated pre-existing Afib that worsened; unblinding of CT findings with anticoagulation initiated for imaging finding, DVT prophylaxis, and bioprosthetic valve
AC Post Index Procedure for
Non-Valve Related
ReasonsN = 68**
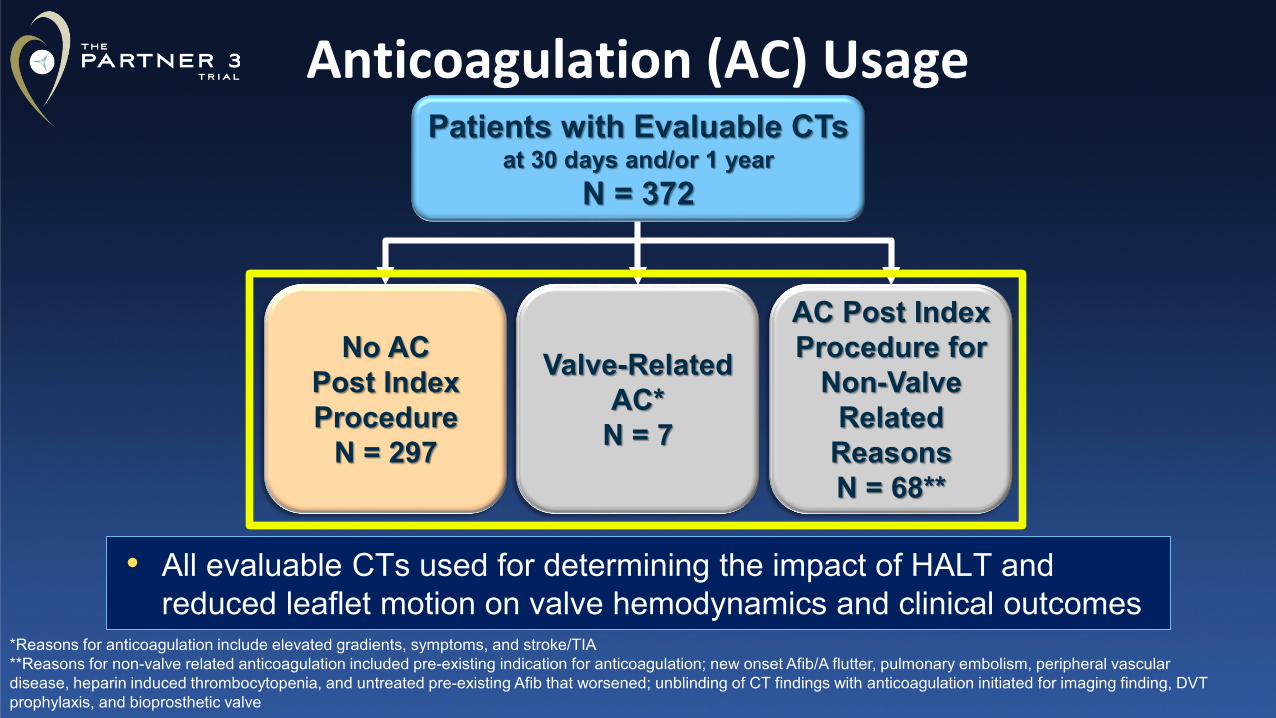
Patients with Evaluable CTs at 30 days and/or 1 year
N = 372
• Per Protocol Population used for the determination of incidence and natural history of HALT and reduced leaflet motion
No AC Post Index Procedure
N = 297
Valve-Related AC*
N = 7
*Reasons for anticoagulation include elevated gradients, symptoms, and stroke/TIA**Reasons for non-valve related anticoagulation included pre-existing indication for anticoagulation; new onset Afib/A flutter, pulmonary embolism, peripheral vascular disease, heparin induced thrombocytopenia, and untreated pre-existing Afib that worsened; unblinding of CT findings with anticoagulation initiated for imaging finding, DVT prophylaxis, and bioprosthetic valve
AC Post Index Procedure for
Non-Valve Related
ReasonsN = 68**
Patients with Evaluable CTs at 30 days and/or 1 year
N = 372
• All evaluable CTs used for determining the impact of HALT and reduced leaflet motion on valve hemodynamics and clinical outcomes
Anticoagulation (AC) Usage
Incidence of HALT at 30 Days and 1 Year
Outcomes (%)30 Days 1 Year
TAVR (N=165)
Surgery (N=119) P-value
TAVR (N=153)
Surgery (N=109) P-value
HALT 13.3 5.0 0.03 27.5 20.2 0.191 Leaflet 81.8 66.7 64.3 68.22 Leaflets 9.1 33.3 23.8 31.83 Leaflets 9.1 0 11.9 0
Event rates are binary and p-value is based on Fisher’s Exact test
TAVR vs SAVRPer Protocol Population
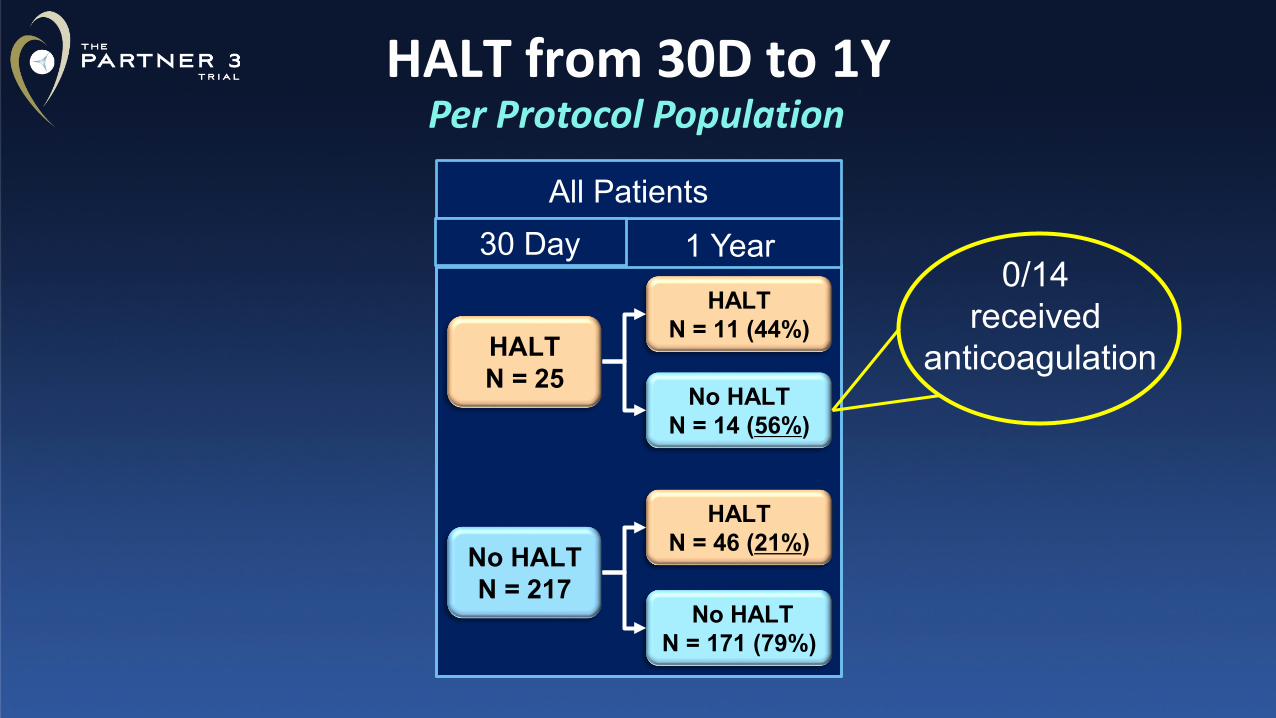
HALT from 30D to 1YPer Protocol Population
All Patients30 Day 1 Year
No HALTN = 217
HALTN = 25
HALTN = 11 (44%)
No HALTN = 14 (56%)
HALTN = 46 (21%)
No HALTN = 171 (79%)
0/14 received
anticoagulation
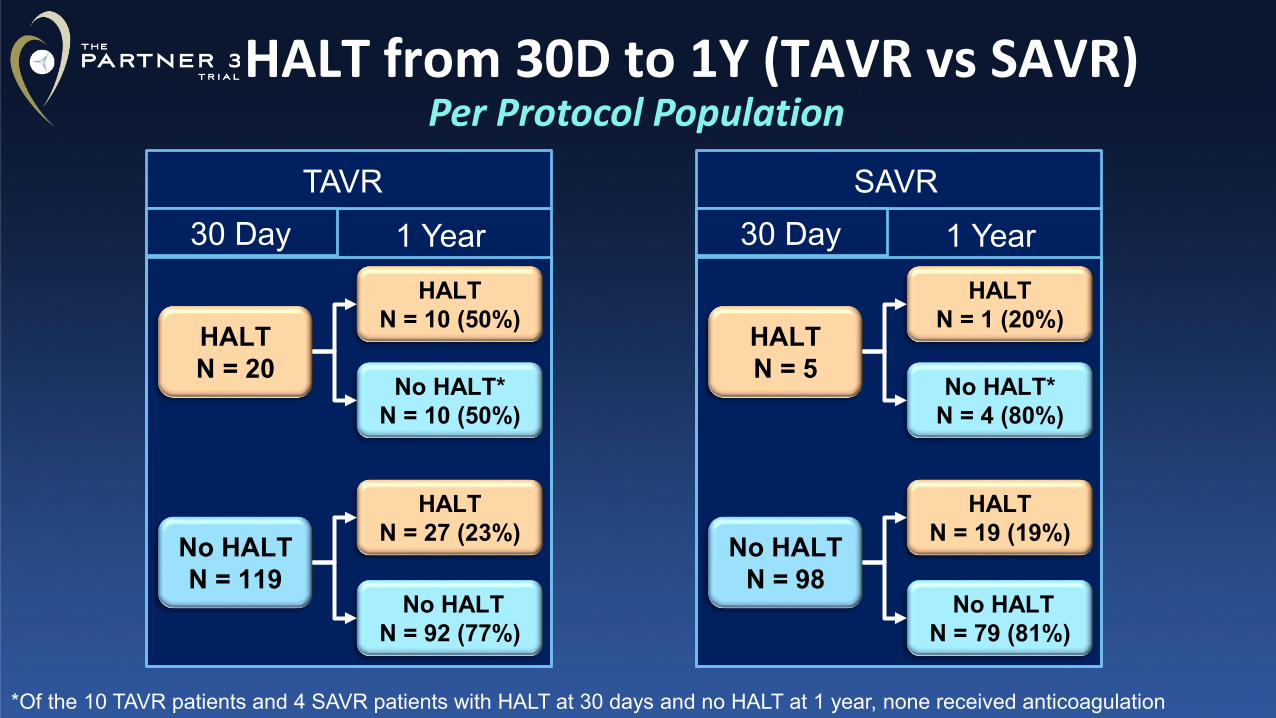
HALT from 30D to 1Y (TAVR vs SAVR)
*Of the 10 TAVR patients and 4 SAVR patients with HALT at 30 days and no HALT at 1 year, none received anticoagulation
Per Protocol PopulationTAVR
30 Day 1 Year
No HALTN = 119
HALTN = 20
HALTN = 10 (50%)
No HALT*N = 10 (50%)
HALTN = 27 (23%)
No HALTN = 92 (77%)
SAVR30 Day 1 Year
No HALTN = 98
HALTN = 5
HALTN = 1 (20%)
No HALT*N = 4 (80%)
HALTN = 19 (19%)
No HALTN = 79 (81%)
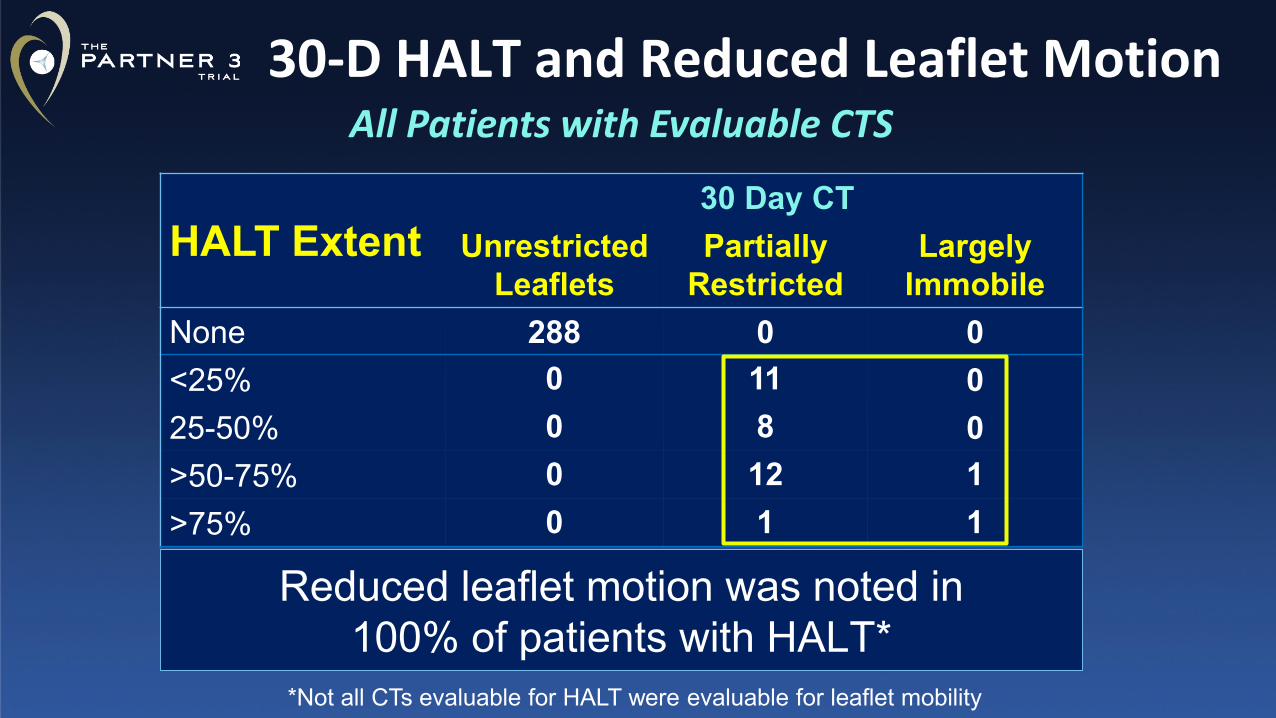
30-D HALT and Reduced Leaflet MotionAll Patients with Evaluable CTS
HALT Extent30 Day CT
Unrestricted Leaflets
Partially Restricted
Largely Immobile
None 288 0 0<25% 0 11 025-50% 0 8 0>50-75% 0 12 1>75% 0 1 1
Reduced leaflet motion was noted in 100% of patients with HALT*
*Not all CTs evaluable for HALT were evaluable for leaflet mobility
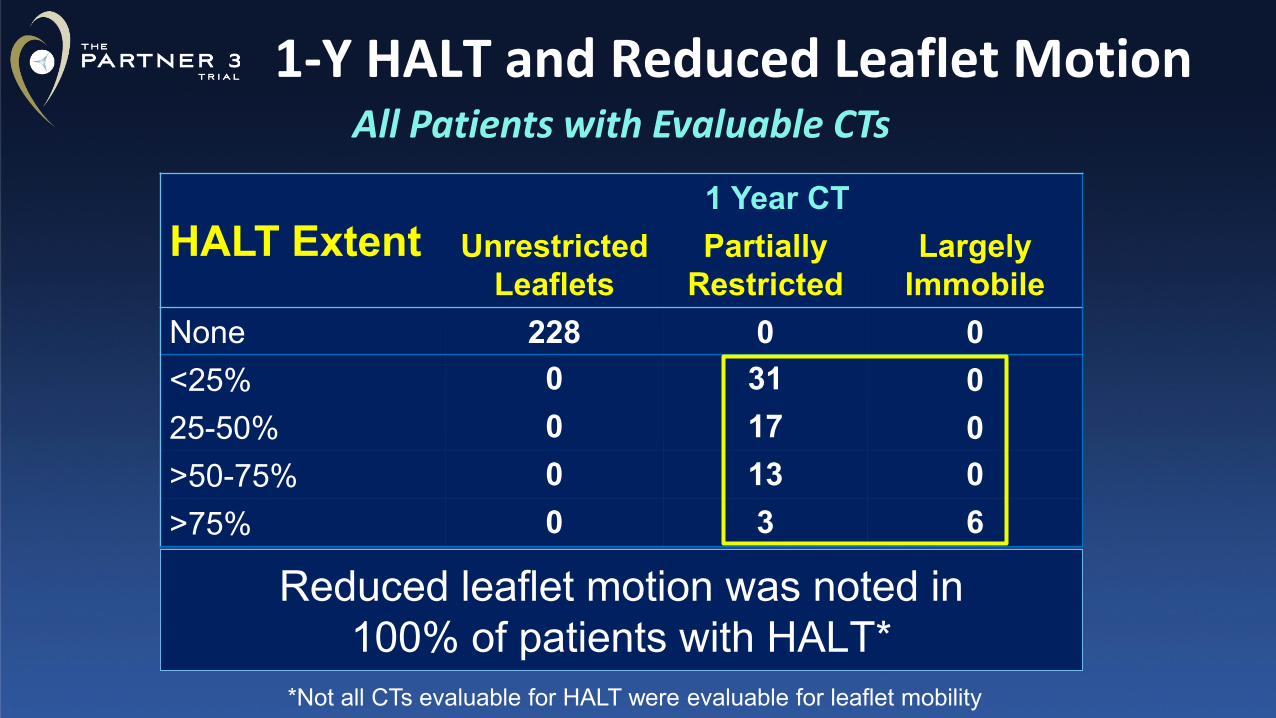
1-Y HALT and Reduced Leaflet MotionAll Patients with Evaluable CTs
HALT Extent1 Year CT
Unrestricted Leaflets
Partially Restricted
Largely Immobile
None 228 0 0<25% 0 31 025-50% 0 17 0>50-75% 0 13 0>75% 0 3 6
Reduced leaflet motion was noted in 100% of patients with HALT*
*Not all CTs evaluable for HALT were evaluable for leaflet mobility
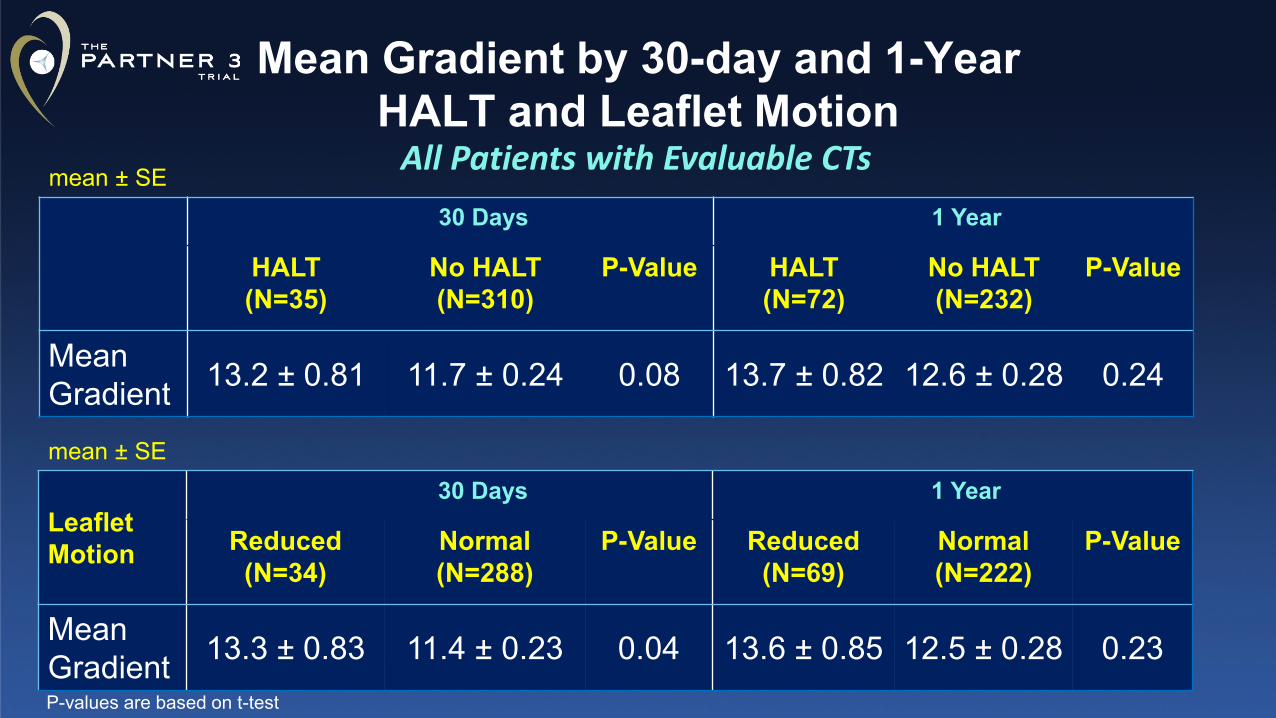
Mean Gradient by 30-day and 1-Year HALT and Leaflet Motion
30 Days 1 Year
HALT (N=35)
No HALT (N=310)
P-Value HALT (N=72)
No HALT (N=232)
P-Value
Mean Gradient 13.2 ± 0.81 11.7 ± 0.24 0.08 13.7 ± 0.82 12.6 ± 0.28 0.24
mean ± SE All Patients with Evaluable CTs
LeafletMotion
30 Days 1 Year
Reduced (N=34)
Normal (N=288)
P-Value Reduced (N=69)
Normal (N=222)
P-Value
Mean Gradient 13.3 ± 0.83 11.4 ± 0.23 0.04 13.6 ± 0.85 12.5 ± 0.28 0.23
mean ± SE
P-values are based on t-test
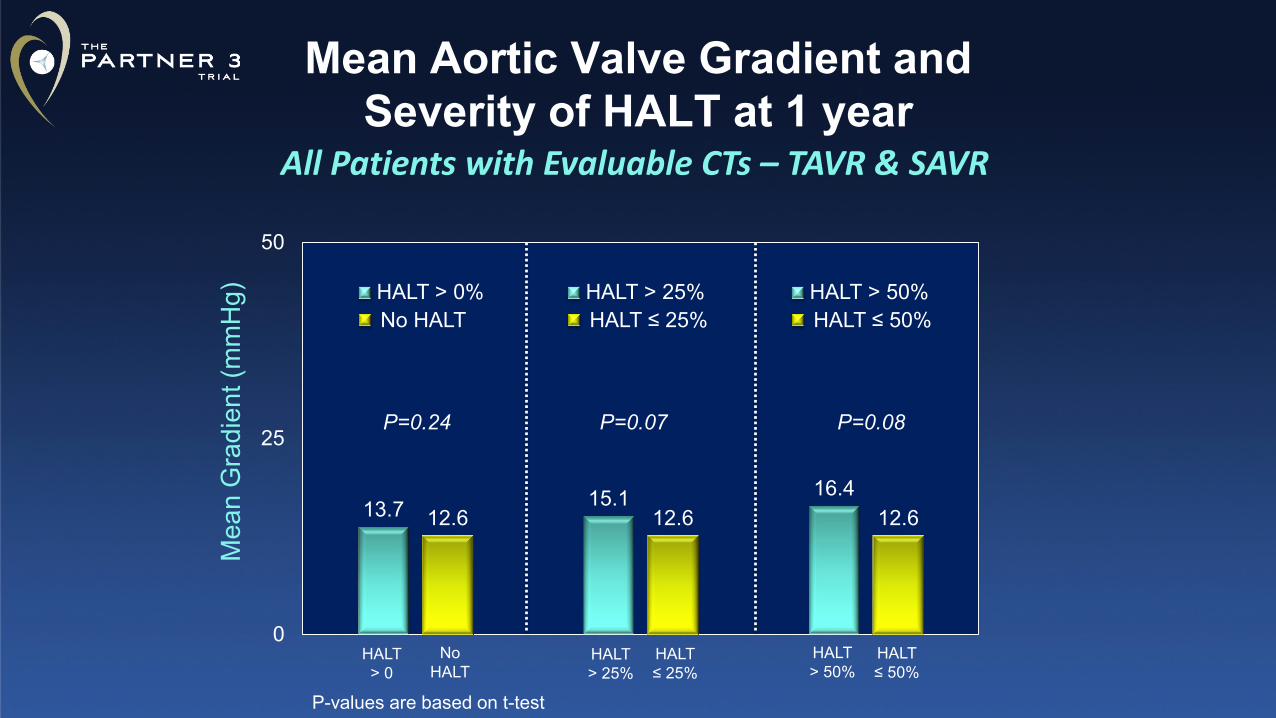
Mean Aortic Valve Gradient and Severity of HALT at 1 year
All Patients with Evaluable CTs – TAVR & SAVR
13.7 15.1 16.412.6 12.6 12.6
0
25
50
HALT > 25%HALT ≤ 25%
HALT > 50%HALT ≤ 50%
HALT > 25%
HALT ≤ 25%
P=0.07 P=0.08
HALT > 0
No HALT
HALT > 0%No HALT
P=0.24
HALT > 50%
HALT ≤ 50%
Mea
n G
radi
ent (
mm
Hg)
P-values are based on t-test
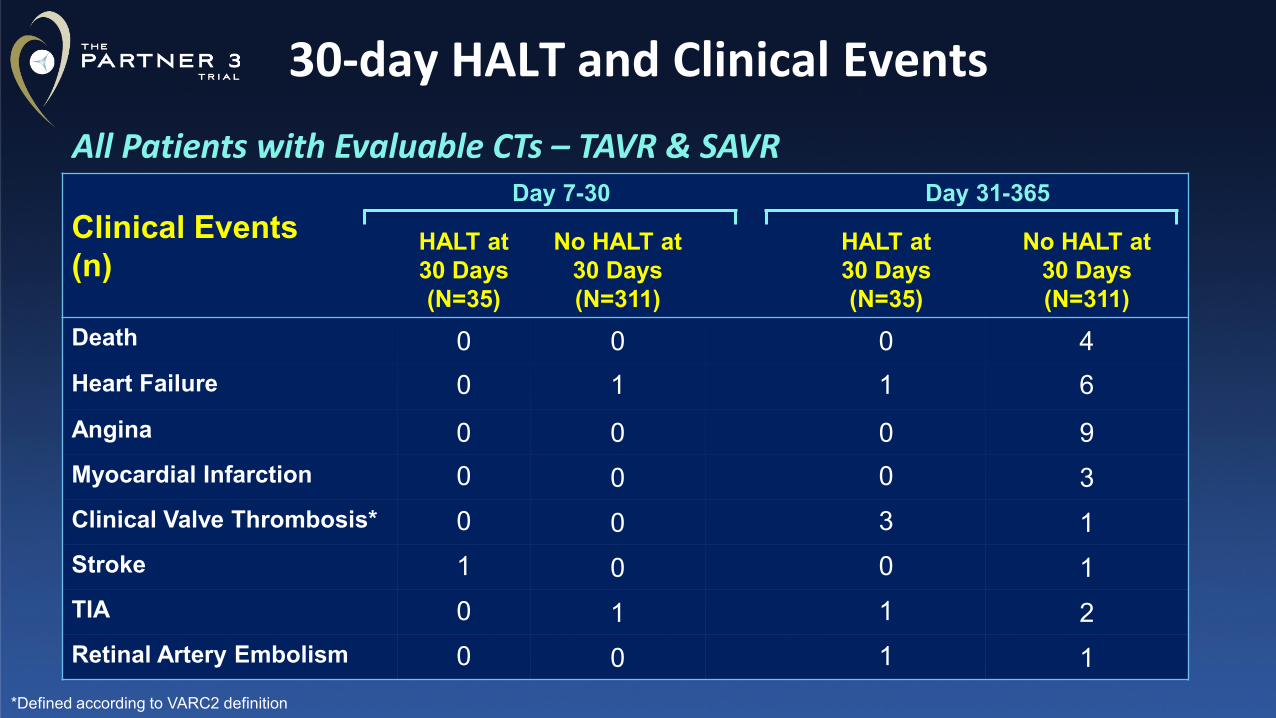
Clinical Events(n)
Day 7-30 Day 31-365
HALT at 30 Days (N=35)
No HALT at 30 Days (N=311)
HALT at 30 Days (N=35)
No HALT at 30 Days (N=311)
Death 0 0 0 4Heart Failure 0 1 1 6Angina 0 0 0 9Myocardial Infarction 0 0 0 3Clinical Valve Thrombosis* 0 0 3 1Stroke 1 0 0 1TIA 0 1 1 2Retinal Artery Embolism 0 0 1 1
30-day HALT and Clinical EventsAll Patients with Evaluable CTs – TAVR & SAVR
*Defined according to VARC2 definition
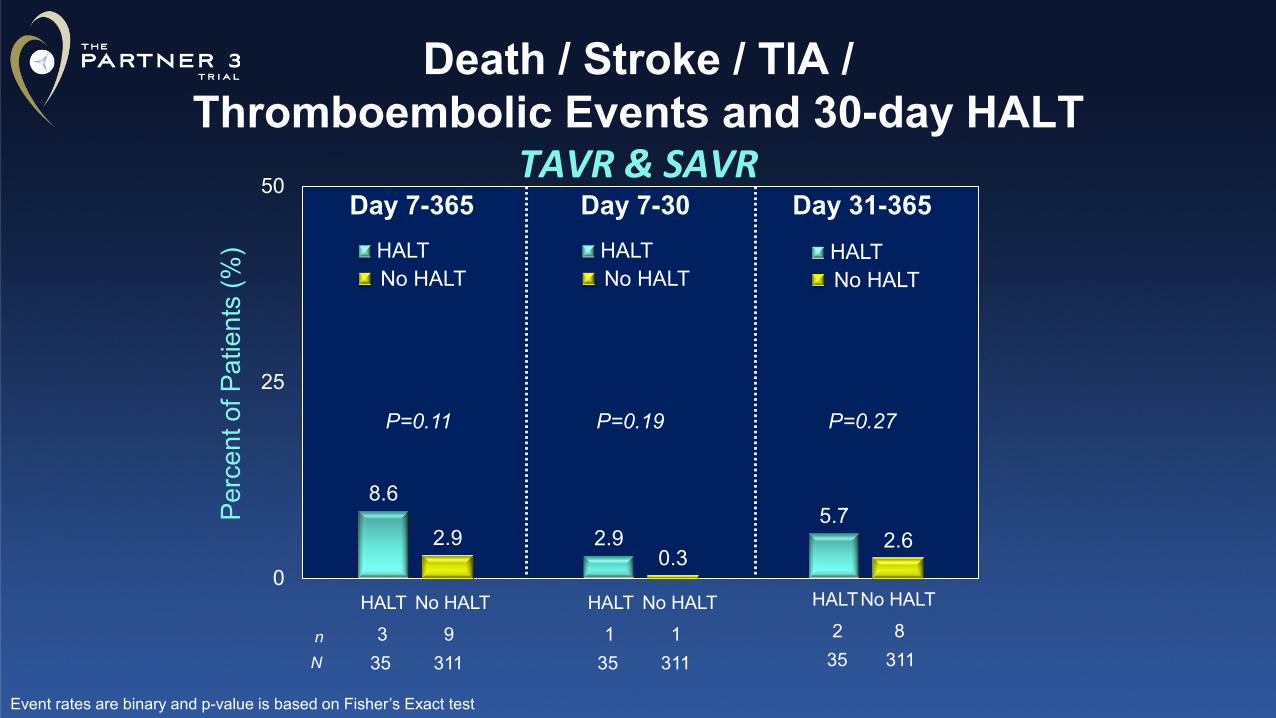
Death / Stroke / TIA / Thromboembolic Events and 30-day HALT
TAVR & SAVR
8.6
2.95.7
2.90.3
2.6
0
25
50
Perc
ent o
f Pat
ient
s (%
) HALTNo HALT
Day 31-365Day 7-30HALTNo HALT
n
HALT1
No HALT1
HALT2
No HALT8
N 35 311 35 311
P=0.19 P=0.27
HALT3
No HALT9
35 311
HALTNo HALT
Day 7-365
P=0.11
Event rates are binary and p-value is based on Fisher’s Exact test
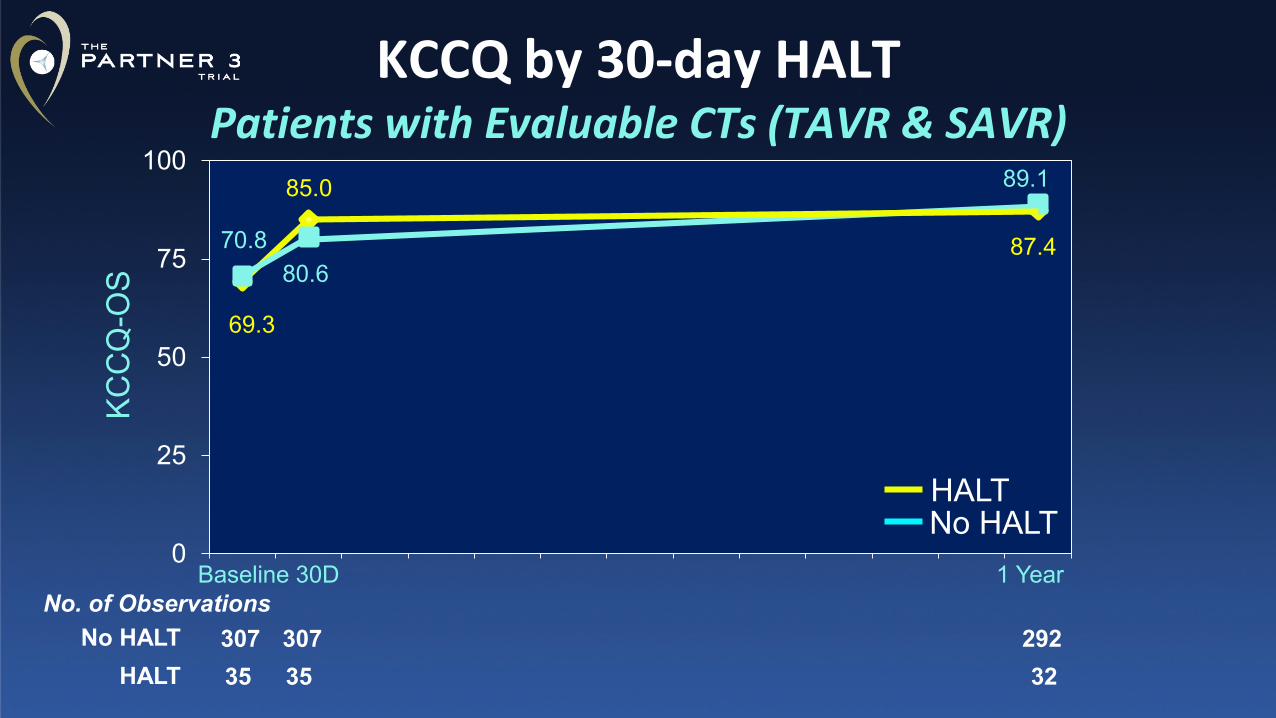
0
25
50
75
100
No HALTHALT
307 307 29235 35 32
KCC
Q-O
S
No HALTHALT
No. of ObservationsBaseline 30D 1 Year
69.3
85.0
87.470.880.6
89.1
KCCQ by 30-day HALT Patients with Evaluable CTs (TAVR & SAVR)
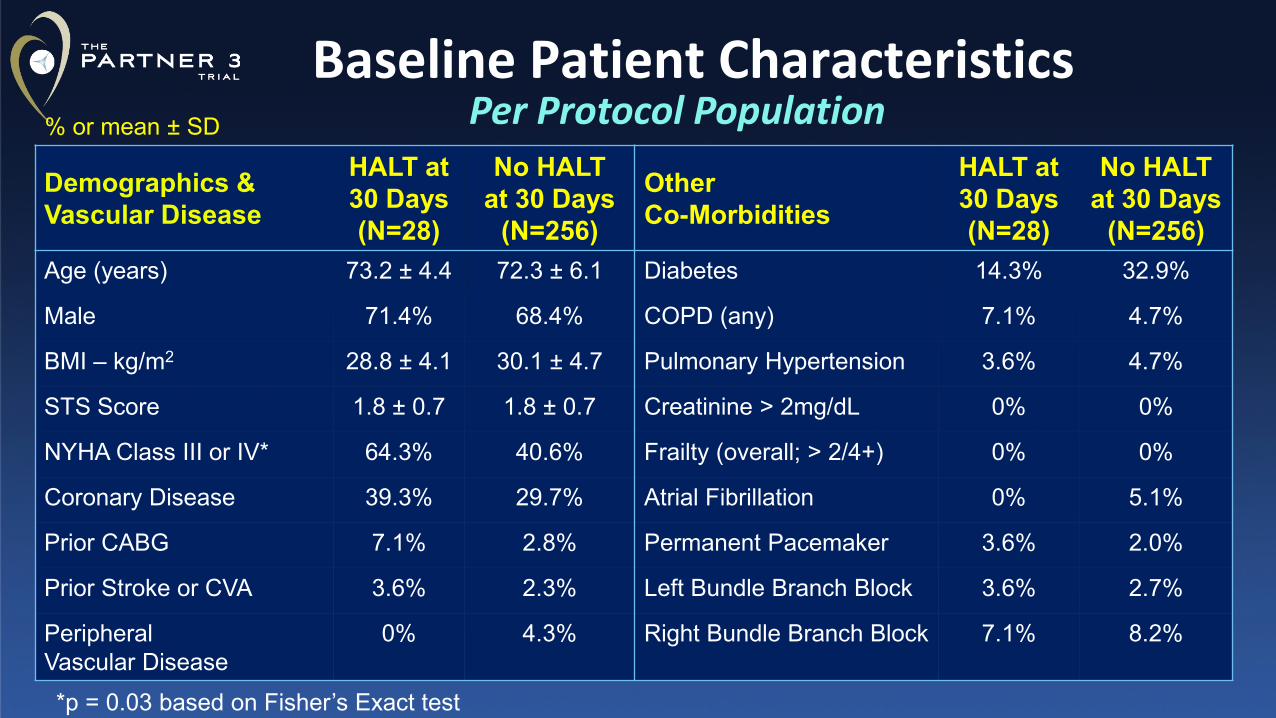
Baseline Patient Characteristics
Demographics & Vascular Disease
HALT at 30 Days(N=28)
No HALT at 30 Days
(N=256)
Other Co-Morbidities
HALT at 30 Days(N=28)
No HALT at 30 Days
(N=256)Age (years) 73.2 ± 4.4 72.3 ± 6.1 Diabetes 14.3% 32.9%
Male 71.4% 68.4% COPD (any) 7.1% 4.7%
BMI – kg/m2 28.8 ± 4.1 30.1 ± 4.7 Pulmonary Hypertension 3.6% 4.7%
STS Score 1.8 ± 0.7 1.8 ± 0.7 Creatinine > 2mg/dL 0% 0%
NYHA Class III or IV* 64.3% 40.6% Frailty (overall; > 2/4+) 0% 0%
Coronary Disease 39.3% 29.7% Atrial Fibrillation 0% 5.1%
Prior CABG 7.1% 2.8% Permanent Pacemaker 3.6% 2.0%
Prior Stroke or CVA 3.6% 2.3% Left Bundle Branch Block 3.6% 2.7%
Peripheral Vascular Disease
0% 4.3% Right Bundle Branch Block 7.1% 8.2%
% or mean ± SD
*p = 0.03 based on Fisher’s Exact test
Per Protocol Population
The PARTNER 3 CT Sub-StudyStudy Limitations
• Results reflect only 1-year outcomes. • Any potential impact of HALT on durability will be assessed in
the 10-year follow up of these low-risk patients• Study is not powered to draw conclusions regarding HALT,
leaflet mobility, and clinical events; results are hypothesis generating
Observations from CT sub-study with blinded assessment of serial CTs in randomized low risk patients undergoing TAVR with SAPIEN 3 or surgery:
• Incidence HALT and reduced leaflet motion are frequently present in the bioprosthetic valves. The incidence in the entire cohort was 10% at 30 days and increased to 24% at 1 year.
• TAVR vs. SAVR The prevalence of HALT and reduced leaflet motion was significantly higher in TAVR than SAVR at 30 days, but not at 1 year.
• Natural History HALT was dynamic and spontaneously resolved (50%) in the absence of anticoagulation; new HALT appeared in 20% of patients at 1 year.
The PARTNER 3 CT Sub-StudyConclusions 1
Observations from CT sub-study with blinded assessment of serial CTs in randomized low risk patients undergoing TAVR with SAPIEN 3 or surgery:
• Valve Hemodynamics HALT and reduced leaflet motion resulted in minimal increase in valve gradients, which can be considered clinically insignificant.
• Clinical Outcomes There were no deaths or MIs in patients with HALT. The pooled rates of death/stroke/TIA/thromboembolic events were numerically higher in patients with HALT; however, given the low total number of events, the data are inconclusive and only hypothesis generating. Longer term follow-up and larger data set will further clarify the impact on clinical outcomes.
The PARTNER 3 CT Sub-StudyConclusions 2
Based upon these findings in surgical & transcatheter bioprosthetic valves:
• Despite the high incidence of HALT and reduced leaflet motion, lack of a clear association with serious clinical events such as death, MI and stroke does not justify the routine prophylactic use of anticoagulation in all patients.
• Routine post TAVR/SAVR CT scans, outside of research protocols are not indicated; CTs should be prompted by increased gradients or thromboembolic events.
• The effect of HALT and reduced leaflet motion on valve durability will be known during long-term follow-up.
The PARTNER 3 CT Sub-StudyClinical Implications
National Principal Investigators• Martin B. Leon, MD, Columbia University Medical Center, New York, NY• Michael J. Mack, MD, The Heart Hospital Baylor Plano, Plano, TX
Steering Committee• Howard Herrmann, Samir Kapadia, Susheel Kodali, Martin B. Leon, Michael J. Mack,
Raj Makkar, Craig R. Smith (chair), Wilson Szeto, Vinod Thourani, John WebbData & Safety Monitoring Board
• Cardiovascular Research Foundation, New York, NY; Joseph Carrozza, Jr., MD, chairClinical Events Committee
• Cardiovascular Research Foundation, New York, NY; Steven O. Marx, MD, chairCT Core Laboratory
• The University of British Columbia; Jonathon Leipsic, MD, chair; Philipp Blanke, MD, chair
Echocardiographic Core Laboratory• Quebec Heart & Lung Institute (Laval University); Philippe Pibarot, DVM PhD, chair• Cardiovascular Research Foundation, New York, NY; Rebecca Hahn, MD, chair
Sponsor• Edwards Lifesciences, Irvine, CA
Study Leadership
Thank you to the Partner 3 investigators

Back-Up Slides
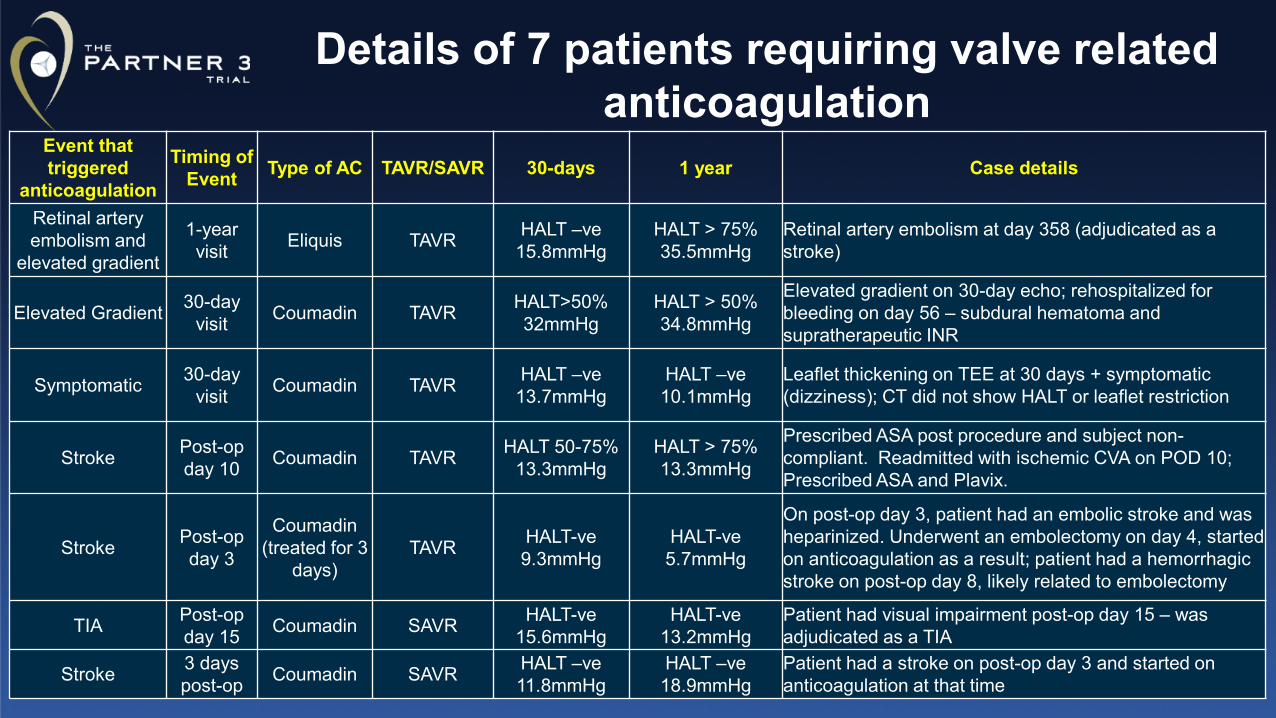
Details of 7 patients requiring valve related anticoagulation
Event that triggered
anticoagulation
Timing of Event Type of AC TAVR/SAVR 30-days 1 year Case details
Retinal artery embolism and
elevated gradient
1-year visit Eliquis TAVR HALT –ve
15.8mmHgHALT > 75%35.5mmHg
Retinal artery embolism at day 358 (adjudicated as a stroke)
Elevated Gradient 30-day visit Coumadin TAVR HALT>50%
32mmHgHALT > 50%34.8mmHg
Elevated gradient on 30-day echo; rehospitalized for bleeding on day 56 – subdural hematoma and supratherapeutic INR
Symptomatic 30-day visit Coumadin TAVR HALT –ve
13.7mmHgHALT –ve10.1mmHg
Leaflet thickening on TEE at 30 days + symptomatic (dizziness); CT did not show HALT or leaflet restriction
Stroke Post-op day 10 Coumadin TAVR HALT 50-75%
13.3mmHgHALT > 75%13.3mmHg
Prescribed ASA post procedure and subject non-compliant. Readmitted with ischemic CVA on POD 10; Prescribed ASA and Plavix.
Stroke Post-op day 3
Coumadin (treated for 3
days)TAVR HALT-ve
9.3mmHgHALT-ve5.7mmHg
On post-op day 3, patient had an embolic stroke and was heparinized. Underwent an embolectomy on day 4, started on anticoagulation as a result; patient had a hemorrhagic stroke on post-op day 8, likely related to embolectomy
TIA Post-op day 15 Coumadin SAVR HALT-ve
15.6mmHgHALT-ve
13.2mmHgPatient had visual impairment post-op day 15 – was adjudicated as a TIA
Stroke 3 days post-op Coumadin SAVR HALT –ve
11.8mmHgHALT –ve18.9mmHg
Patient had a stroke on post-op day 3 and started on anticoagulation at that time
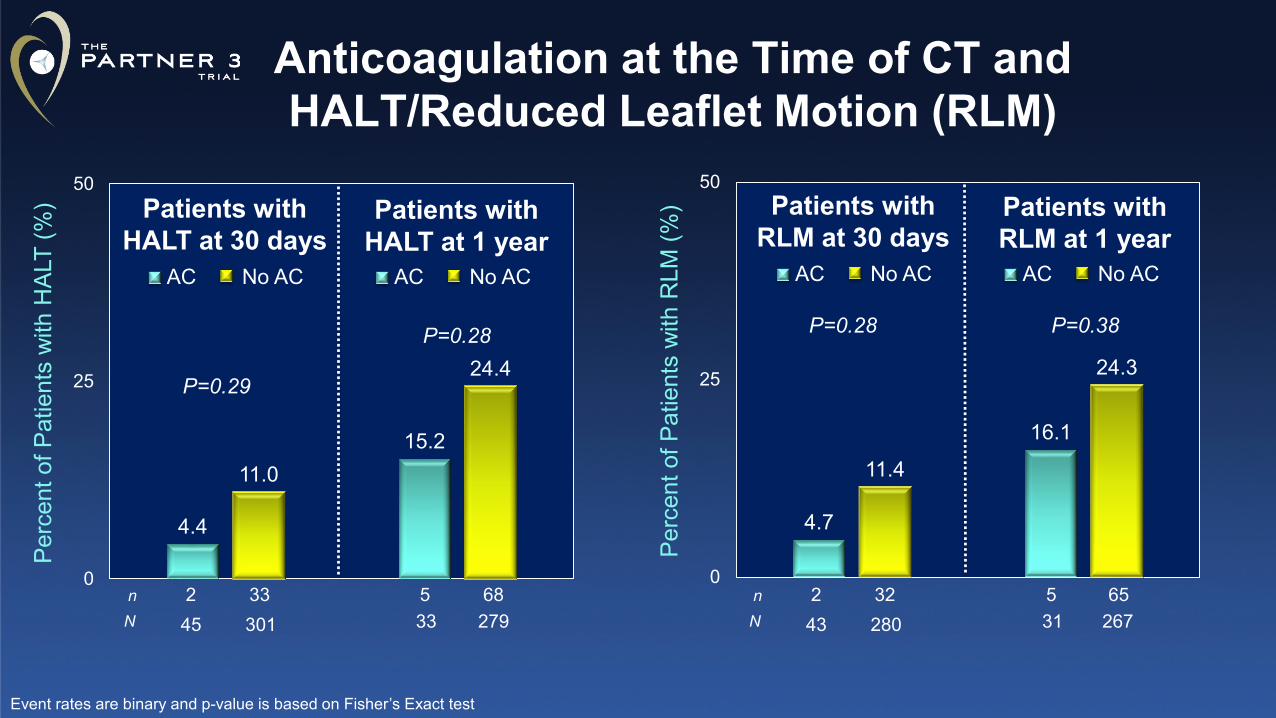
Anticoagulation at the Time of CT and HALT/Reduced Leaflet Motion (RLM)
4.4
15.211.0
24.4
0
25
50
Perc
ent o
f Pat
ient
s w
ith H
ALT
(%)
AC
Patients with HALT at 30 days
n 2 33 5 68N 45 301 33 279
P=0.29
P=0.28
4.7
16.1
11.4
24.3
0
25
50
Perc
ent o
f Pat
ient
s w
ith R
LM (%
)
n 2 32 5 65N 43 280 31 267
P=0.28 P=0.38
Patients with HALT at 1 year
No AC AC No AC AC
Patients with RLM at 30 days
Patients with RLM at 1 year
No AC AC No AC
Event rates are binary and p-value is based on Fisher’s Exact test
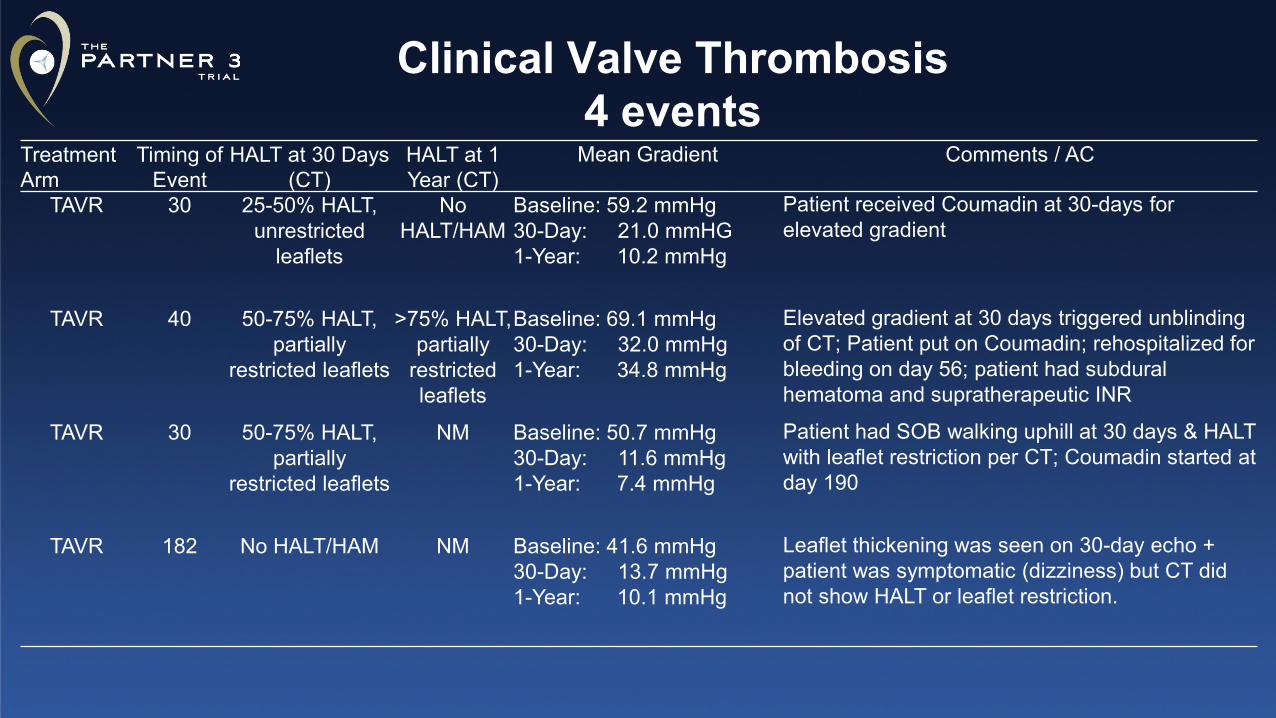
Treatment Arm
Timing of Event
HALT at 30 Days (CT)
HALT at 1 Year (CT)
Mean Gradient Comments / AC
TAVR 30 25-50% HALT, unrestricted
leaflets
No HALT/HAM
Baseline: 59.2 mmHg30-Day: 21.0 mmHG1-Year: 10.2 mmHg
Patient received Coumadin at 30-days for elevated gradient
TAVR 40 50-75% HALT, partially
restricted leaflets
>75% HALT, partially
restricted leaflets
Baseline: 69.1 mmHg30-Day: 32.0 mmHg1-Year: 34.8 mmHg
Elevated gradient at 30 days triggered unblinding of CT; Patient put on Coumadin; rehospitalized for bleeding on day 56; patient had subdural hematoma and supratherapeutic INR
TAVR 30 50-75% HALT, partially
restricted leaflets
NM Baseline: 50.7 mmHg30-Day: 11.6 mmHg1-Year: 7.4 mmHg
Patient had SOB walking uphill at 30 days & HALT with leaflet restriction per CT; Coumadin started at day 190
TAVR 182 No HALT/HAM NM Baseline: 41.6 mmHg30-Day: 13.7 mmHg1-Year: 10.1 mmHg
Leaflet thickening was seen on 30-day echo + patient was symptomatic (dizziness) but CT did not show HALT or leaflet restriction.
Clinical Valve Thrombosis4 events
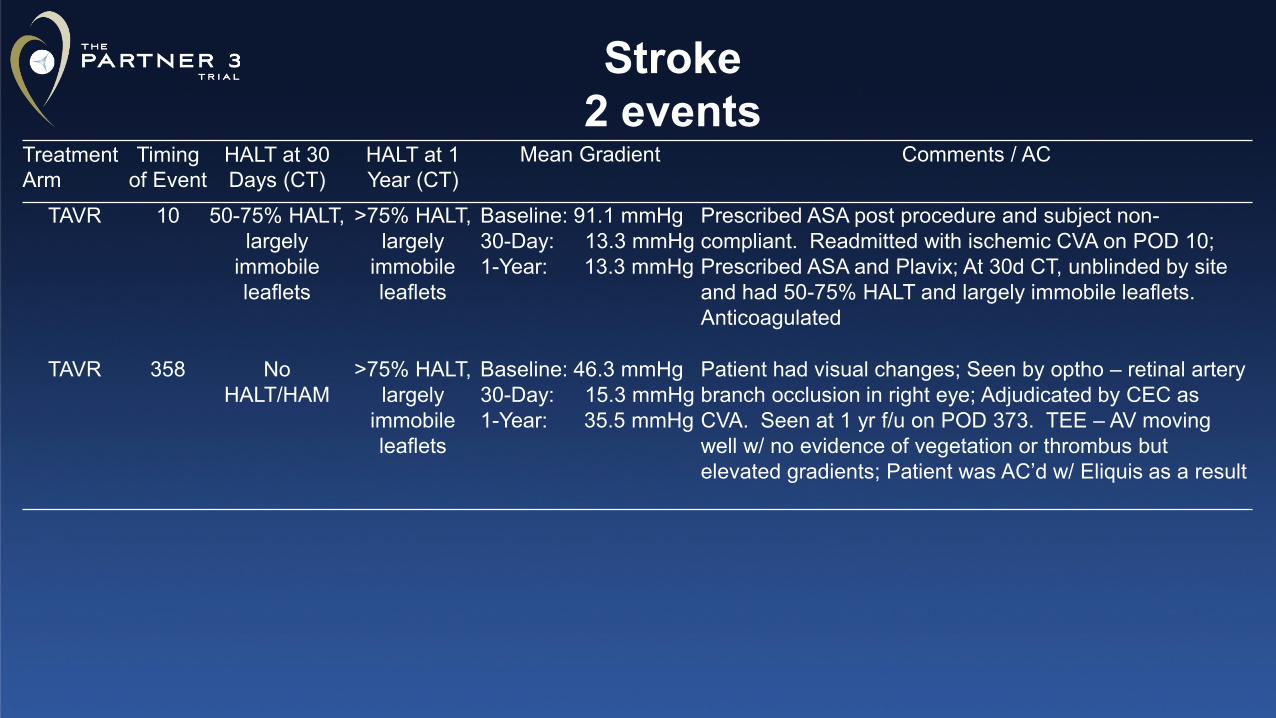
Treatment Arm
Timing of Event
HALT at 30 Days (CT)
HALT at 1 Year (CT)
Mean Gradient Comments / AC
TAVR 10 50-75% HALT, largely
immobile leaflets
>75% HALT, largely
immobile leaflets
Baseline: 91.1 mmHg30-Day: 13.3 mmHg1-Year: 13.3 mmHg
Prescribed ASA post procedure and subject non-compliant. Readmitted with ischemic CVA on POD 10; Prescribed ASA and Plavix; At 30d CT, unblinded by site and had 50-75% HALT and largely immobile leaflets. Anticoagulated
TAVR 358 No HALT/HAM
>75% HALT, largely
immobile leaflets
Baseline: 46.3 mmHg30-Day: 15.3 mmHg1-Year: 35.5 mmHg
Patient had visual changes; Seen by optho – retinal artery branch occlusion in right eye; Adjudicated by CEC as CVA. Seen at 1 yr f/u on POD 373. TEE – AV moving well w/ no evidence of vegetation or thrombus but elevated gradients; Patient was AC’d w/ Eliquis as a result
Stroke2 events
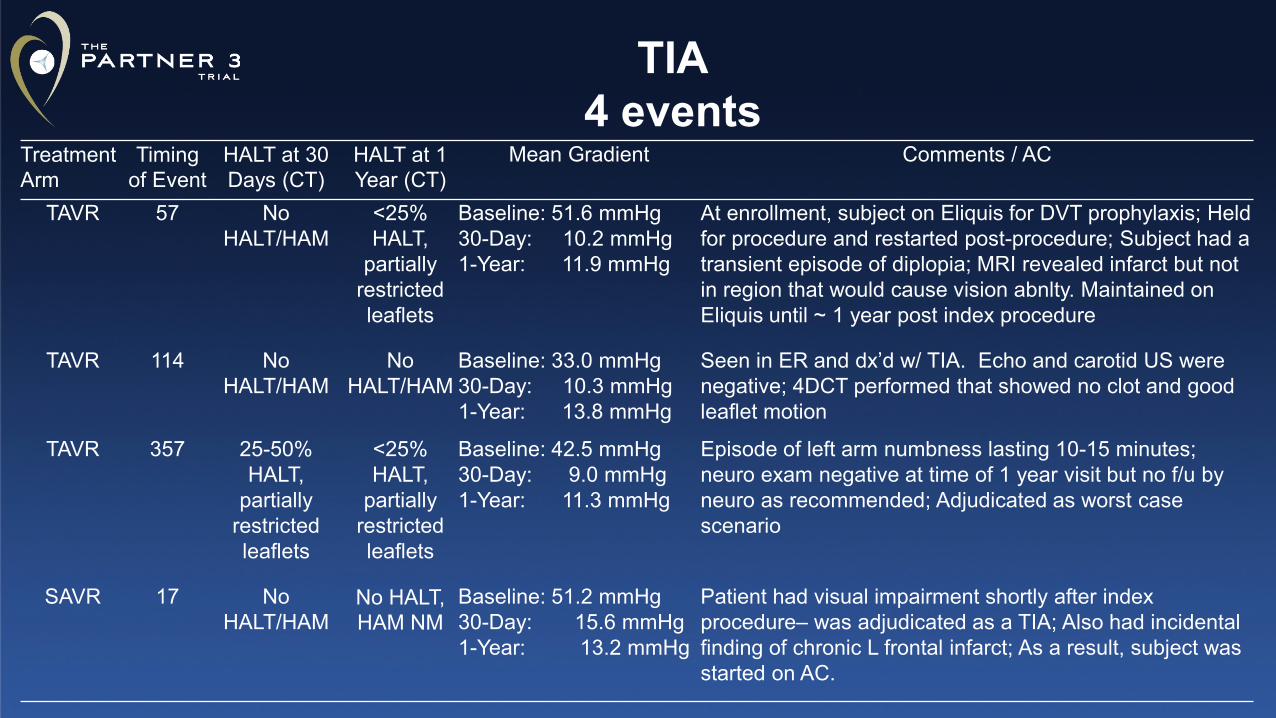
Treatment Arm
Timing of Event
HALT at 30 Days (CT)
HALT at 1 Year (CT)
Mean Gradient Comments / AC
TAVR 57 No HALT/HAM
<25% HALT,
partially restricted leaflets
Baseline: 51.6 mmHg30-Day: 10.2 mmHg1-Year: 11.9 mmHg
At enrollment, subject on Eliquis for DVT prophylaxis; Held for procedure and restarted post-procedure; Subject had a transient episode of diplopia; MRI revealed infarct but not in region that would cause vision abnlty. Maintained on Eliquis until ~ 1 year post index procedure
TAVR 114 No HALT/HAM
No HALT/HAM
Baseline: 33.0 mmHg30-Day: 10.3 mmHg1-Year: 13.8 mmHg
Seen in ER and dx’d w/ TIA. Echo and carotid US were negative; 4DCT performed that showed no clot and good leaflet motion
TAVR 357 25-50% HALT,
partially restricted leaflets
<25% HALT,
partially restricted leaflets
Baseline: 42.5 mmHg30-Day: 9.0 mmHg1-Year: 11.3 mmHg
Episode of left arm numbness lasting 10-15 minutes; neuro exam negative at time of 1 year visit but no f/u by neuro as recommended; Adjudicated as worst case scenario
SAVR 17 No HALT/HAM
No HALT, HAM NM
Baseline: 51.2 mmHg30-Day: 15.6 mmHg1-Year: 13.2 mmHg
Patient had visual impairment shortly after index procedure– was adjudicated as a TIA; Also had incidental finding of chronic L frontal infarct; As a result, subject was started on AC.
TIA4 events
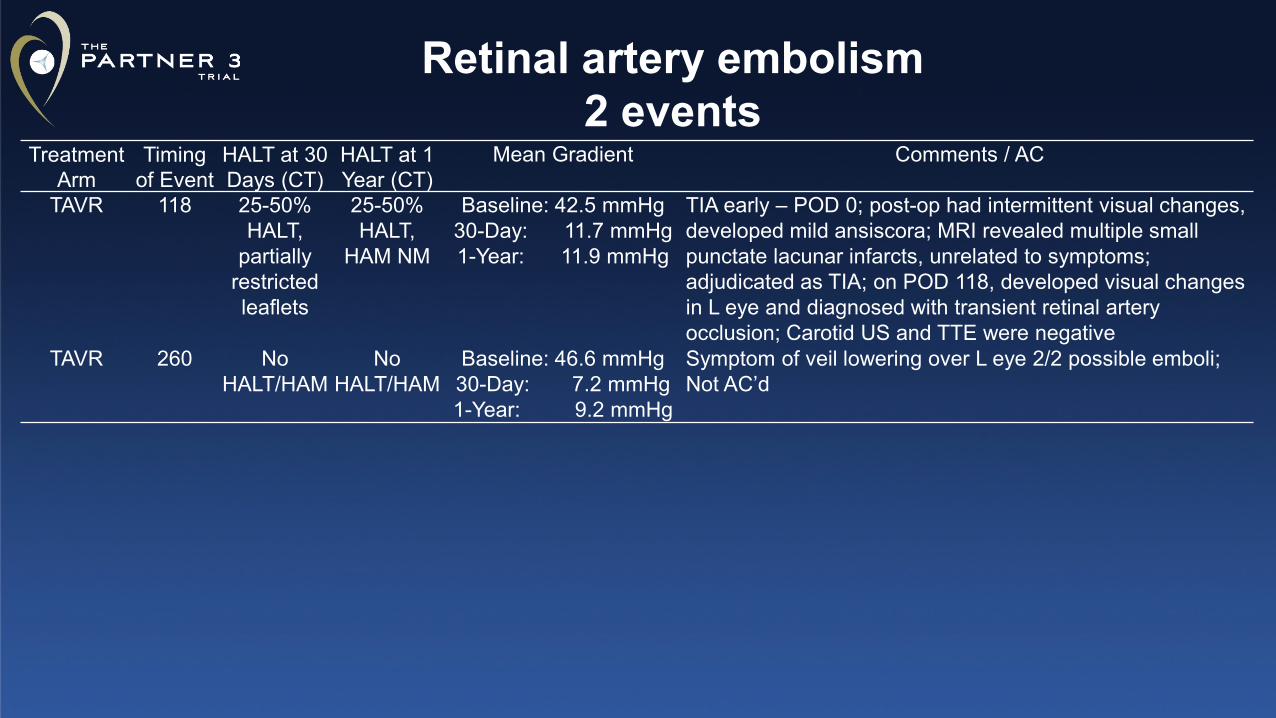
Treatment Arm
Timing of Event
HALT at 30 Days (CT)
HALT at 1 Year (CT)
Mean Gradient Comments / AC
TAVR 118 25-50% HALT,
partially restricted leaflets
25-50% HALT,
HAM NM
Baseline: 42.5 mmHg30-Day: 11.7 mmHg1-Year: 11.9 mmHg
TIA early – POD 0; post-op had intermittent visual changes, developed mild ansiscora; MRI revealed multiple small punctate lacunar infarcts, unrelated to symptoms; adjudicated as TIA; on POD 118, developed visual changes in L eye and diagnosed with transient retinal artery occlusion; Carotid US and TTE were negative
TAVR 260 No HALT/HAM
No HALT/HAM
Baseline: 46.6 mmHg30-Day: 7.2 mmHg1-Year: 9.2 mmHg
Symptom of veil lowering over L eye 2/2 possible emboli; Not AC’d
Retinal artery embolism2 events
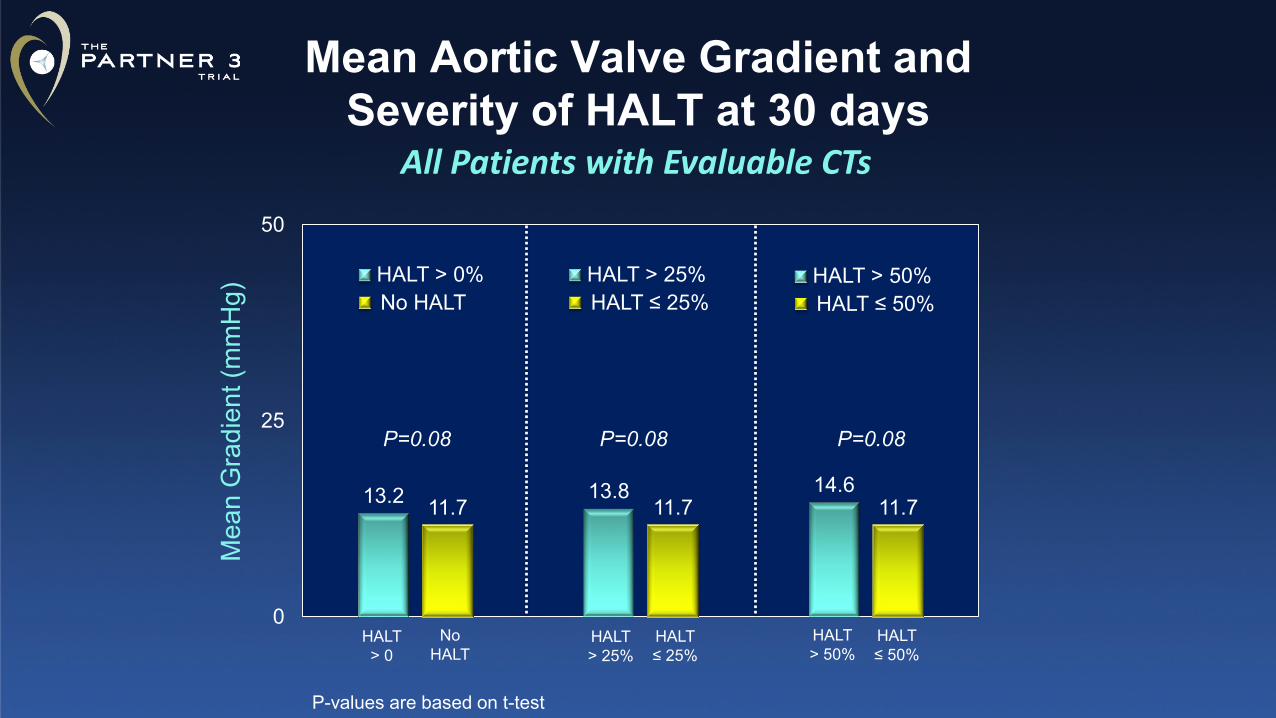
Mean Aortic Valve Gradient and Severity of HALT at 30 days
All Patients with Evaluable CTs
13.2 13.8 14.611.7 11.7 11.7
0
25
50M
ean
Gra
dien
t (m
mH
g)HALT > 25%HALT ≤ 25%
HALT > 50%HALT ≤ 50%
HALT > 25%
HALT ≤ 25%
P=0.08 P=0.08
HALT > 0
No HALT
HALT > 0%No HALT
P=0.08
HALT > 50%
HALT ≤ 50%
P-values are based on t-test
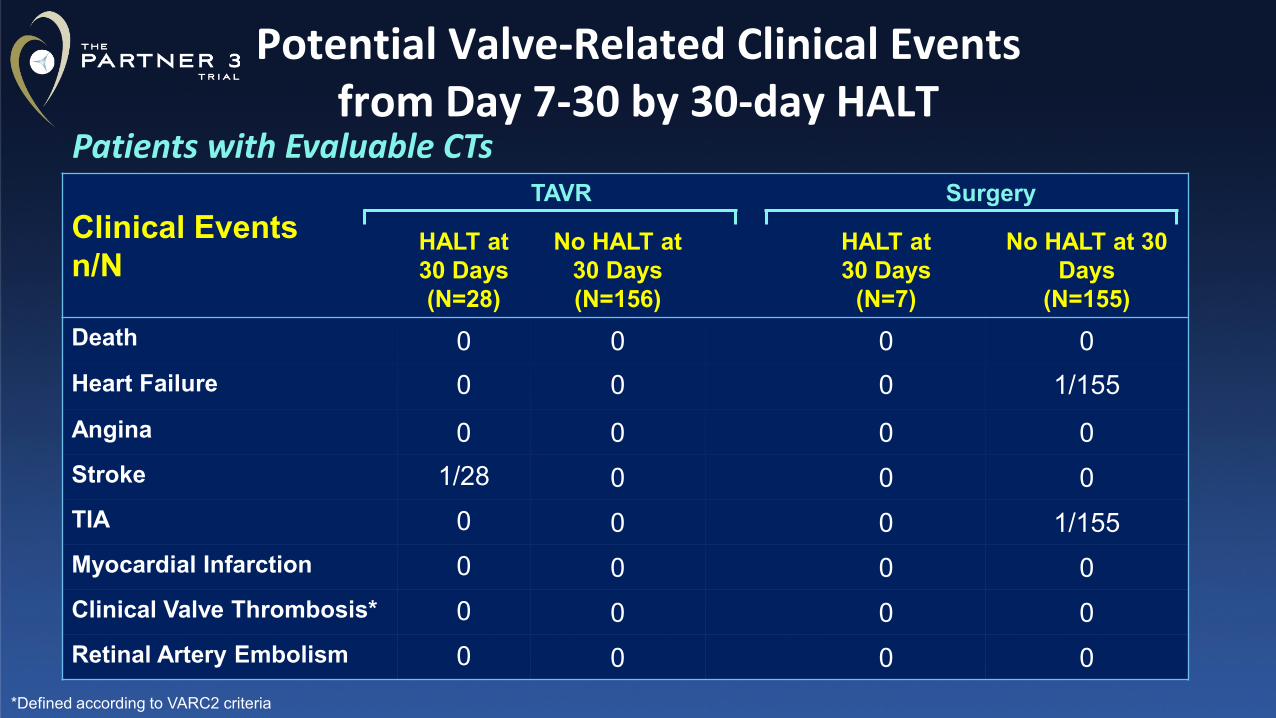
Clinical Eventsn/N
TAVR Surgery
HALT at 30 Days (N=28)
No HALT at 30 Days (N=156)
HALT at 30 Days
(N=7)
No HALT at 30 Days
(N=155)Death 0 0 0 0Heart Failure 0 0 0 1/155Angina 0 0 0 0Stroke 1/28 0 0 0TIA 0 0 0 1/155Myocardial Infarction 0 0 0 0Clinical Valve Thrombosis* 0 0 0 0Retinal Artery Embolism 0 0 0 0
Potential Valve-Related Clinical Events from Day 7-30 by 30-day HALT
Patients with Evaluable CTs
*Defined according to VARC2 criteria
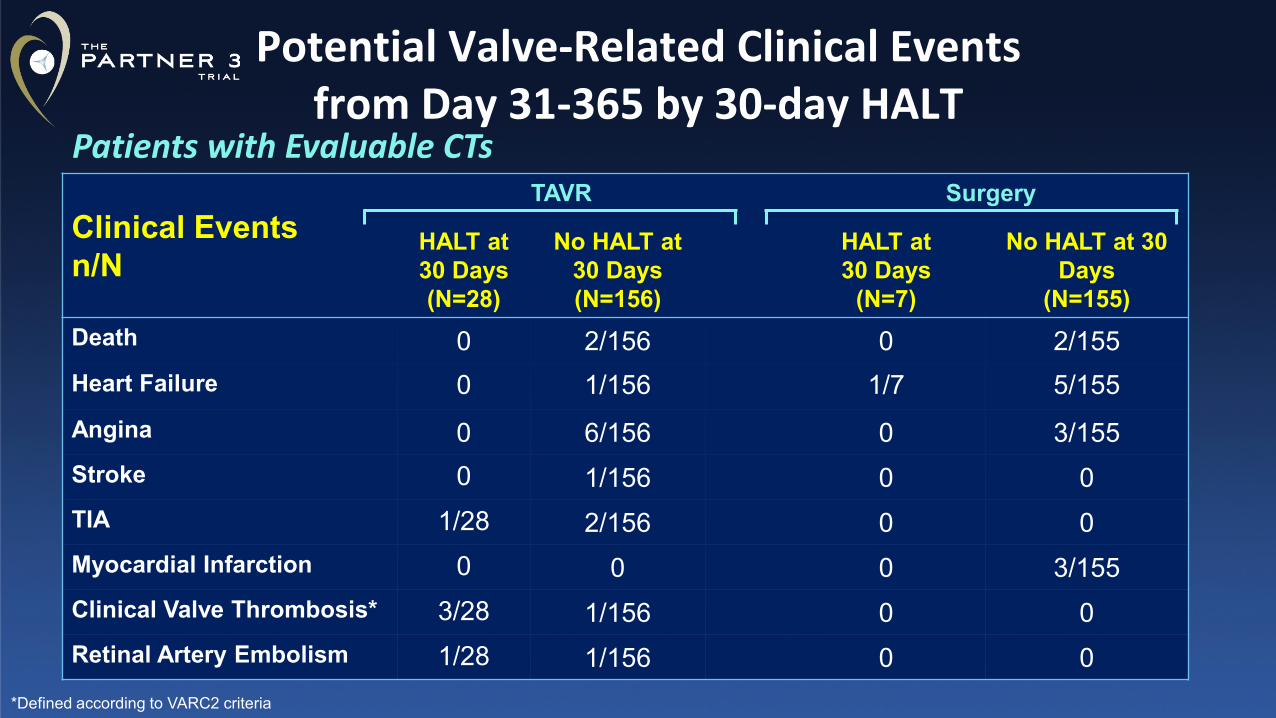
Clinical Eventsn/N
TAVR Surgery
HALT at 30 Days (N=28)
No HALT at 30 Days (N=156)
HALT at 30 Days
(N=7)
No HALT at 30 Days
(N=155)Death 0 2/156 0 2/155Heart Failure 0 1/156 1/7 5/155Angina 0 6/156 0 3/155Stroke 0 1/156 0 0TIA 1/28 2/156 0 0Myocardial Infarction 0 0 0 3/155Clinical Valve Thrombosis* 3/28 1/156 0 0Retinal Artery Embolism 1/28 1/156 0 0
Potential Valve-Related Clinical Events from Day 31-365 by 30-day HALT
*Defined according to VARC2 criteria
Patients with Evaluable CTs
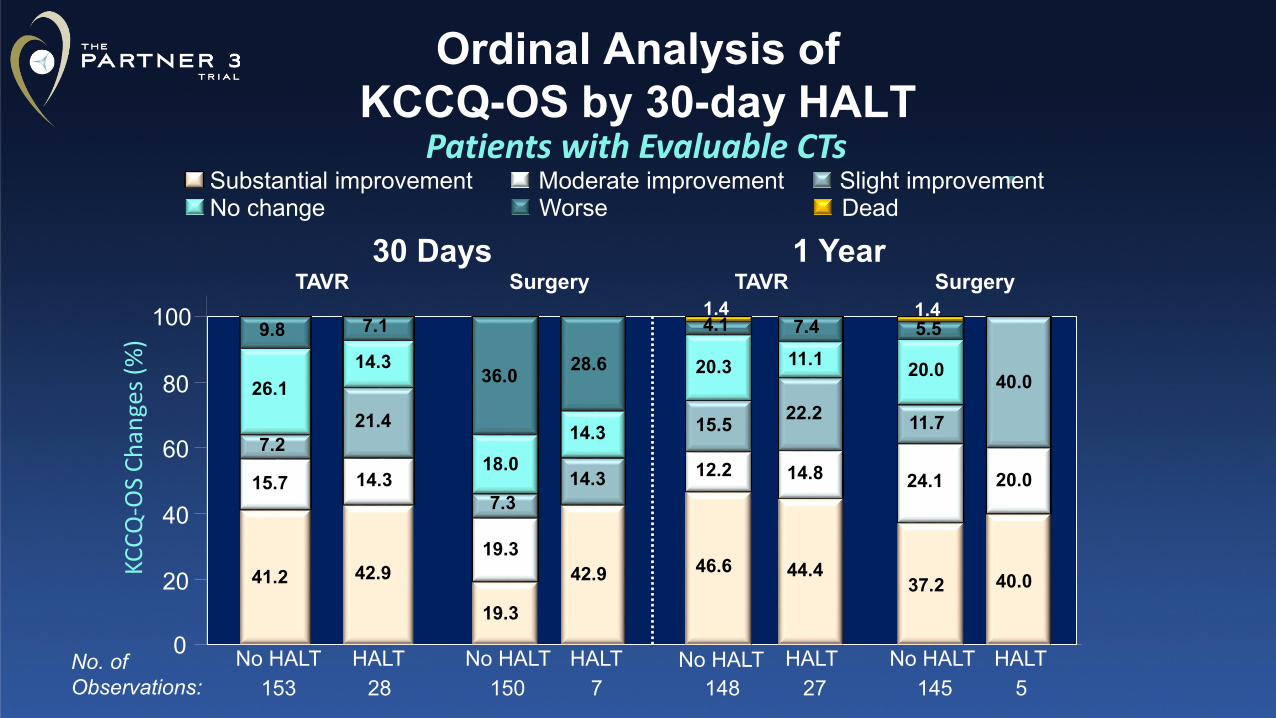
Ordinal Analysis of KCCQ-OS by 30-day HALT
Patients with Evaluable CTsDeadWorseNo changeSlight improvementModerate improvementSubstantial improvement
KCCQ
-OS
Chan
ges (
%)
37.2
24.1
11.7
20.0
5.51.4
40.0
20.0
40.0
No HALT HALT
46.6
12.2
15.5
20.3
4.11.4
44.4
14.8
22.2
11.17.4
No HALT HALT
19.3
19.3
7.3
18.0
36.0
42.9
14.3
14.3
28.6
No HALT HALT
41.2
15.7
7.2
26.1
9.8
42.9
14.3
21.4
14.3
7.1
No HALT HALT0
20
40
60
80
100
30 DaysTAVR Surgery TAVR Surgery
153 28 150 7 148 27 145 5No. of Observations:
1 Year
![Fundamentals of cone beam computed tomography for a ...Cone beam computed tomography (CBCT, also referred to as C-arm computed tomography [CT], cone beam volume CT, or flat panel CT)](https://img.pdfslide.net/doc/110x75/611ad245d6c77f53c63c9117/fundamentals-of-cone-beam-computed-tomography-for-a-cone-beam-computed-tomography.jpg)