Embed Size (px)
Citation preview

Patellofemoral Pain Syndrome

Anatomy

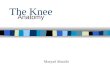
Anatomy – patellofemoral joint• Patella (convex) articulates with trochlea of femur (concave)
– Bony lesions may be present in PFPS e.g. degenerative/fracture• Patella is sesamoid bone, embedded within quadriceps/patella tendon• Associated soft tissue structures commonly affected in PFPS:
– Anterior synovial tissues– Anterior knee joint capsule– Suprapatellar plica– Fat pad– Bursae– Medial patellofemoral ligament– Retinaculum– Quadriceps/patella tendon– ITB

Pathophysiology
• Loss of osseous or peripatellar soft tissue homeostasis due to overload or high frequency of load to bone/soft tissues
• Potential neural involvement• Excessive pressure of lateral structures stimulates release
of substances that produce growth of new nerves and blood vessels e.g. Substance P, Vascular Endothelial Growth Factor (VEGF)
• Similar to tendinopathy?

What Causes Pain?Anatomical Source Description of Pain
Anterior synovial tissues, retinaculum, fat pad and capsules
Severe pain accurately localized
Capsular Margins, femoral condyles Poorly localized moderate pain
Articular cartilage of patella No pain (even with stage 2-3 chondramalacia patella)
(Dye et al., 1998)

Mechanism of Injury
• Traumatic– Compression – falling onto knee, impact of patella
into trochlea– Twisting – subluxation/dislocation of patella
• Overuse– Biomechanical overload– Biological overload (i.e not allowing tissue to
recover)

Classification1. Patellar Compression Syndrome
– Excessive Lateral Pressure Syndrome
– Global Patellar Pressure Syndrome
2. Patellar Instability– Chronic Patellar Subluxation– Acute Patellar Dislocation– Recurrent Patellar Dislocation
3. Biomechanical Dysfunction4. Direct Patellar Trauma
– Articular Cartilage Lesion (isolated)– Fracture– Fracture/dislocation– Articular Cartilage Lesion with
associated malalignment
5. Soft Tissue Lesions– Suprapatella Plica– Fat Pad Syndrome– Medial Patellomfemoral Ligament
Pain– Iliotibial Band Friction Syndrome– Bursitis
6. Overuse Syndromes– Tendinitis (tendinopathy)– Apophysitis
7. Osteochondritis Dessicans8. Neurologic Disorders
– Reflex Sympathetic Dystrophy– Sympathetically maintained pain

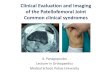
Patella Compression Syndrome- Excessive Lateral Pressure Syndrome
• Patella is squeezed by surrounding soft tissue
• If surrounding soft tissue is ‘tight’ the patella looses its mobility
• Excessive pressure of the lateral structures can cause lateral retinacular pain
• Pain can occasionally be medially as the structures are on constant stretch
• Can eventually lead to degeneration of the lateral facet of the patella
• Restriction in medial glide of patella resulting in lateral tilt

Patella Compression Syndrome- Excessive Lateral Pressure Syndrome

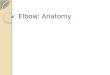
Patella Compression Syndrome- Global Patellar Pressure Syndrome
• Both Medial and Lateral retinaculum are tight• Develops due to fibrosis of tissues following
trauma or immobilization• Global restriction in patella range of
movement• Knee pain is reported globally around the
patella

Lower Extremity Biomechanical Dysfunction
• Biomechanical dysfunction at the low back, hip, tibia and ankle can change the kinematics of the knee
• This alters the patellofemoral joint stress and can cause pain

Do they happen in combination?
• Excessive lateral pressure syndrome can occur because of biomechanical dysfunctions
• The following presentation is going to assume this is the classification as treatment options will vary for all the different types
• See Wilk et al., 1998 for more information on the management of each classification

Subjective
• Insidious onset (generally, global patella compression syndrome is usually traumatic)
• History of overloading tissues (increase in activity/training duration, intensity, frequency and/or inadequate rest)
• Ill defined ache localized anterior knee• Sharp pain occasionally• Aggs: squatting, running, walking down slopes, sitting for
long periods (theatre goers knee), stairs• Giving way
– Pain inhibition of quads– Patella laterally dislocating

Objective
• Pain on palpation patella facets• Restricted ankle dorsiflexion• Continued pronation during gait• Restricted hip flexion/abduction/internal rotation• Restricted tibial internal rotation• Reduced quadriceps strength• Reduced hip extension/abduction strength• Painful squatting, stepping, lunge• Valgus collapse at knee

Special Tests
• Patella tracking and tilt is unreliable(Song et al., 2011)• Specific Tests are not useful(Nunes et al., 2013)• Assessing medio-lateral patellar position ONLY
reliable and valid test available(Smith et al., 2009)

Further Investigations
• Bone scintigraphy - can possibly detect changes in osseous metabolism.
• X-ray – not often useful, except if bony trauma• MRI – useful to guide treatment only in certain cases e.g.
joint effusion• Ultrasound – to detect soft tissue lesions?
Further investigation commonly ineffective at facilitating diagnosis or guiding treatment. Findings on investigation do not necessarily correlate with symptoms.

Management
• Multimodal • Physiotherapy is key• Mixture of manual therapy AND correct rehabilitation• Control of overloading to allow biological tissue to
repair e.g if running for 9 miles causes pain – only run 8 miles
• Ensure adequate time for recovery between training sessions
• Surgery should not be considered as lateral release has POOR outcomes

Management
Goal of therapy is to • Reduce overload to tissues, but maintaining sufficient
load to prevent deloading• Promote healing/restoration of homeostasis• Reduce pain and odema if present• Restore ROM • Restore motor control and strength• Improve biomechanics/address movement impairments • Improve neuromuscular control and proprioception• Prepare for return to sport/full function

Conservative Management
• Manual therapy – Reduce swelling/effusion, reduce pain, restore normal
mobility• Taping– Offload irritated tissues, alter muscle activity, change
arthrokinematics? Limited supporting evidence• Orthotics– Offload irritated tissues, alter biomechanics
• Barefoot running– Retrain running mechanics, reduce PFJ stress

Conservative Management
Exercise• Arguably the most important component of
physiotherapy management. • Manual therapy, taping, orthotics should be used to
facilitate pain free exercise.• Exercise selection based on assessment findings
1. Mobility – restore full ROM of ankle, knee, hip2. Restore motor control
• quads/VMO e.g. SQs, SLR, IRQ• Lumbopelvic control

Conservative Management
Exercise3. Strengthening (initially in ranges of minimum PFJ
stress• Quads
– leg press 0-45° knee flexion, leg ext 45-90° knee flexion, gradually increasing ROM
– Step up, step down, lateral step-up (without knee valgus)
• Glutes – external rotation/abduction– Clam, monster band walks
• Focus on concentric and eccentric strength• Gradually increase ROM and then load• Progress to squat, lunge, lateral lunge, deadlift

Conservative Management
Exercise4. Proprioception & neuromuscular control• Balance, change of direction, controlled jumping &
landing
5. Gait retraining• May be required to improve biomechanics/reduce PFJ
stress
6. Specific drills to prepare for return to normal activities/sport

Surgical - Management
• Not recommended due to poor outcomes e.g. lateral release