Embed Size (px)
Citation preview

Paternal Transmission and Anticipationin Schizophrenia
Janice Husted,1 Laura E. Scutt,2 and Anne S. Bassett2,3*1Department of Health Studies and Gerontology, University of Waterloo, Waterloo, Ontario, Canada2Schizophrenia Research Program, Queen Street Mental Health Centre, Toronto, Ontario, Canada3Department of Psychiatry, University of Toronto, Toronto, Ontario, Canada
Recent studies have observed anticipation(earlier age at onset (AAO) or increased dis-ease severity in successive generations) infamilial schizophrenia. In other disorders,where the molecular mechanism (repeat ex-pansion) is known, anticipation varies in de-gree depending on the sex of the transmit-ting parent. We investigated parental sex ef-fects on anticipation in schizophrenia,using a familial sample of affected two-generation pairs in which anticipation hadpreviously been demonstrated using the me-dian intergenerational difference (MID) inAAO. A Wilcoxon rank sum test for indepen-dent samples was used to determine wheth-er MID in AAO was significantly differentfor paternal and maternal transmission. Re-sults suggested that in a sample of 127 par-ent-offspring pairs, anticipation wasgreater with paternal than with maternaltransmission (MID = 18 and 14 years, respec-tively, P = 0.05). Paternal effects werestrongest in 39 parent-offspring pairs withearly-onset offspring (<21 years) (MID = 22and 17 years, respectively, for paternal andmaternal transmission, P = 0.01). However,assessment of the effect of possible selectionbiases suggests that preferential ascertain-ment of late-onset fathers may have exertedimportant effects. While the results supportpossible paternal effects, further studies areneeded to draw firm conclusions about trueparent-of-origin effects on anticipation infamilial schizophrenia. Am. J. Med. Genet.(Neuropsychiatr. Genet.) 81:156–162, 1998.© 1998 Wiley-Liss, Inc.
KEY WORDS: schizophrenia; anticipation;imprinting; transmission; sexeffects
INTRODUCTION
Recent studies have observed anticipation (earlierage at onset (AAO) or increased disease severity in suc-cessive generations) in familial schizophrenia [Asher-son et al., 1994; Bassett and Honer, 1994; Lesch et al.,1994], consistent with the historical literature [Mott,1910; Bleuler, 1978]. Findings of significant anticipa-tion in schizophrenia persist even after adjusting forthe effects of ascertainment biases, which may simu-late anticipation [Gorwood et al., 1996; Bassett andHusted, 1997]. These studies have suggested anticipa-tion as a mechanism that may contribute to explainingcomplex modes of inheritance in schizophrenia [Asher-son et al., 1994; Bassett and Honer, 1994], a syndromewith variable phenotype involving psychotic symp-toms, marked social disabilities, and increased mortal-ity.
In several neuropsychiatric disorders with autoso-mal-dominant inheritance, anticipation is caused by adynamic mutation containing cytosine-guanine (CG)-rich trinucleotide repeats (TNR) that can expand insuccessive generations [Sutherland and Richards,1995]. Anticipation and the length instability of theassociated TNR expansion frequently vary in degree,depending on the sex of the transmitting parent. Forinstance, paternal transmission is associated withmore prominent anticipation of AAO in Huntingtondisease (HD) [Ranen et al., 1995], spinocerebellarataxia type I (SCA1) [Jodice et al., 1994], dentatoru-bral-pallidoluysian atrophy (DRPLA), Machado-Josephdisease (MJD) [Ikeuchi et al., 1996], and adult-onsetstages of myotonic dystrophy (DM) [Brunner et al.,1993]. As shown in Table I, the magnitude of theseparent-of-origin effects varies from disease to disease.
The observation of parental sex effects on anticipa-tion in other neuropsychiatric disorders raises ques-tions about such effects in schizophrenia. Evidence forthe presence of parental sex effects would provide fur-ther support for true anticipation in schizophrenia
Contract grant sponsors: Canadian Psychiatric Research Foun-dation, Medical Research Council of Canada.
*Correspondence to: Dr. Anne S. Bassett, Schizophrenia Re-search Program, Queen Street Mental Health Centre, 1001Queen Street West, Toronto, Ontario M6J 1H4, Canada.
Received 26 August 1997; Revised 31 October 1997
American Journal of Medical Genetics (Neuropsychiatric Genetics) 81:156–162 (1998)
© 1998 Wiley-Liss, Inc.

[Ranen et al., 1995] and could help in the search forcausal mutations, none of which have yet been identi-fied. Few studies, however, have examined parent-of-origin sex effects on transmission in familial schizo-phrenia, and sample sizes have been small [Ashersonet al., 1994; Bassett and Honer, 1994; Gorwood et al.,1996]. Only one study has reported anticipation of AAOseparately for paternal and maternal transmission inschizophrenia [Gorwood et al., 1996]. No evidence forparental sex effects on anticipation was found; how-ever, relatively small numbers of offspring of affectedfathers (n 4 24) and of affected mothers (n 4 19) mayhave decreased the power of this study to detect subtleeffects. For instance, in HD the detection of subtle pa-ternal anticipation required a large sample of affectedparent-offspring pairs (n 4 1,693) and the investiga-tion of a relatively large subsample of offspring withvery young AAO (<21 years) (n 4 169) to determinesignificant effects [Ridley et al., 1988].
The objective of the current study was to investigateparent-of-origin sex effects on anticipation in schizo-phrenia using a familial sample of affected two-generation pairs in which anticipation had previouslybeen demonstrated [Bassett and Husted, 1997]. In thisstudy we assumed that parental sex effects on antici-pation in schizophrenia would be large enough to beobserved despite factors complicating all genetic stud-ies of schizophrenia, i.e., decreased reproductive fit-ness, especially in males [Bassett et al., 1996], andlikely locus heterogeneity.
PATIENTS AND METHODSPenrose Archival Data
Samples used in the current study were drawn fromarchival data collected for Lionel Penrose’s study en-titled ‘‘Survey of Cases of Familial Mental Illness’’[Penrose, 1991], which was published posthumously[Crow, 1991]. Subject recruitment and assessmenthave been described in detail elsewhere [Bassett andHusted, 1997]. Briefly, Penrose ascertained a large rep-resentative sample of familial mental illness by survey-ing all individuals who had been admitted to Ontariopsychiatric hospitals between 1926–1944, reviewingtheir medical records, and identifying those with one ormore family members who had ever been hospitalizedwith a mental illness or who had committed suicide.The total sample, comprising approximately 10% of the
total psychiatric inpatient population in Ontario, con-sisted of 7,339 individuals from 3,109 families. Foreach individual in the sample, Penrose recorded infor-mation on diagnostic category, year of birth, year offirst psychiatric hospitalization, and how the indi-vidual was related to the relative(s) in the data set(e.g., father, daughter, niece). Penrose used the medicalchart diagnoses to form 13 broad categories of mentalillness, with the majority of individuals in the samplebeing diagnosed with either schizophrenia (30.8%) oraffective disorder (29.8%). In our previous study [Bas-sett and Husted, 1997], we addressed concerns aboutthe heterogeneity within Penrose’s 13 diagnostic cat-egories by examining the original chart diagnosis withPenrose’s recorded diagnosis in a subset of the sample(n 4 2,176). This comparison showed that approxi-mately 94% of subjects in the schizophrenia categoryhad diagnoses of schizophrenia alone or schizophreniaof the catatonic, paranoid, hebephrenic, or mentally de-fective type. In the affective disorder category, 99.0% ofsubjects had depressive, manic, manic-depressive, mel-ancholic, or schizoaffective diagnoses. Other findingssuggested that the diagnostic categorization of severepsychiatric illnesses was comparable to that of contem-porary studies [Crow, 1991]. These included a similarproportion of subjects with schizophrenia and affectivedisorders in the total sample, separate diagnostic cat-egories for medical disorders, and an earlier medianAAO for schizophrenia (31 years) than for affective dis-order (44 years).
For the current study we used two samples (I and II)of affected relative pairs after excluding families withbilineal transmission [Bassett and Husted, 1997]. Inthe cases where there were two or more affected pairsper family (8.6% of sample I and 23.9% of sample II), asingle pair per family was randomly selected. Becausethe diagnosis of schizophrenia after age 60 years isrelatively rare [Gorwood et al., 1996], we felt less con-fident about the validity of the diagnosis in this sub-group. Therefore, families with a member who had avery late AAO (ù60 years) (n 4 10, sample I; n 4 10,sample II) were excluded.
Pairs were formed using one relative from the paren-tal generation (parent or aunt/uncle) and one from theindex generation (offspring or niece/nephew). Sample I,consisting of 127 parent-offspring pairs with schizo-phrenia, permitted a direct test of the hypothesis ofparental sex effects on anticipation as measured by a
TABLE I. Parental Sex Effects on Anticipation of AAO for Selected Autosomal-Dominant Diseases
Huntington’s diseaseaDentatorubralpallidoluysian
atrophybMachado-Joseph
diseaseb Myotonic dystrophyc
Paternal Maternal Paternal Maternal Paternal Maternal Paternal Maternal
Anticipation inyears (SD) 6.73 (9.2) 1.35 (8.49) 25.6 (2.4) 14.0 (4.0) 15.4 (2.5) 6.9 (2.0) 30 27
TNR instability Paternal > maternal Paternal > maternal Paternal > maternal Paternal > maternald
aRidley et al., 1988; Ranen et al., 1995.bIkeuchi et al., 1996.cLopez de Munain et al., 1994.dWith paternal transmission, instability increases but the rate of transmission decreases with increasing TNR size; transmission of congenital DM isalmost exclusively maternal.
Paternal Transmission and Anticipation 157

generational difference in AAO, which was defined asage at first psychiatric hospitalization. Although onlyan approximation of AAO of illness, age at first psychi-atric hospitalization provides a reliable estimate of theAAO of acute and serious psychiatric symptoms of ma-jor mental disorders such as schizophrenia [DeLisi,1992; Beiser et al., 1993]. In addition, it has beenshown that age at first treatment is highly correlatedwith age at first diagnosis, defined as the age at whichpatients first met DSM-III-R diagnostic criteria forschizophrenia based on medical records and interviews[Gorwood et al., 1996]. Sample II consisted of 92 aunt/uncle-niece/nephew pairs in which both members werediagnosed with schizophrenia and transmitting par-ents were unaffected (not hospitalized). This samplepermitted an assessment of parental sex effects on an-ticipation where confounding influences of reduced re-productive fitness and environmental adversity result-ing from parent’s affected status were minimized.
Analyses
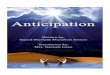
Since the distribution of AAO was asymmetrical(Fig. 1), we used the median to compare AAO between
the parental and offspring generations within eachsample [Bassett and Husted, 1997]. We first deter-mined anticipation of AAO by subtracting offspringgeneration AAO from parental generation AAO foreach pair. The Wilcoxon sign-rank paired-sample testwas used to determine whether pairwise intergenera-tional AAO differences were significantly >0, testingthe null hypothesis of no anticipation. To examinewhether there was a parental sex effect on anticipa-tion, we used the Wilcoxon rank sum test for indepen-dent samples to determine whether pairwise intergen-erational AAO differences were significantly differentfor paternal and maternal transmission. In addition, toassess the effect of preferential selection of late-onsetfathers, we examined parental sex effects on anticipa-tion in early-AAO (ø34 years) parents. Our definitionof early and late AAO is consistent with that used byPenrose and with mean AAO values for first-admissionschizophrenia samples in 1943 [Penrose, 1991; Bassettand Husted, 1997]. Consistent with the HD literature,we also investigated parental sex effects in very young-onset offspring, defined as offspring with AAO ø21years. All analyses were performed using the SAS Sys-tem for Windows, Release 6.11 (Cary, North Carolina).
Fig. 1. Histograms of age at onset (AAO) for parents (black bars) and offspring (white bars) in sample I (n 4 127). AAO values are grouped into 5-yearcohorts for both the paternally transmitted pairs (n 4 39) and the maternally transmitted pairs (n 4 88). Median, mean, and mode, respectively, for AAOof subjects were as follows: fathers (top, black bars): 41.0, 42.6 (SD 4 9.9), and 36.0; offspring of fathers (top, white bars): 23, 26.2 (SD 4 8.7), and 17;mothers (bottom, black bars): 39, 39.6 (SD 4 8.7), and 35; offspring of mothers (bottom, white bars): 25, 27.4 (SD 4 9.1), and 22.
158 Husted et al.

RESULTSSex Effects of Affected Transmitting Parents
on Anticipation
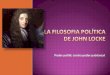
Of the 127 parent-offspring pairs with schizophreniain sample I, 39 pairs had an affected father and 88 hadan affected mother (Table II). This ratio is consistentwith male reproductive fitness, which is about half thatof females with schizophrenia [Bassett et al., 1996].Ninety-five percent of paternally transmitted pairs and84% of maternally transmitted pairs showed anticipa-tion, with significant median intergenerational AAOdifferences of 18 and 14 years, respectively (Table II).Figure 2 shows the distribution of anticipation. Therewas an abnormal skew for paternal transmission(−0.37) and for maternal transmission (−0.40). The me-dian AAO was 40 years for the parental generation(fathers and mothers) and 24 years for the offspringgeneration. These values bracket the mean AAO of 34years observed in a random sample of first admissionsin Ontario in 1943 [Penrose, 1991], and likely reflectthe effects of ascertaining affected parent-offspringpairs [Bassett and Husted, 1997]. There were no sig-nificant sex differences in median AAO within genera-tions (see Table II).
As shown in Table II, anticipation was significantlygreater in paternal transmission than maternal trans-mission (Wilcoxon two-sample Z statistic 4 1.93, P 40.05). Further analyses revealed that the sex of off-spring (son or daughter) did not modify the observedpaternal effect on anticipation (data not shown). Asimilar pattern of results was observed when the diag-nosis was broadened to include one affected relativewith either schizophrenia or a major affective disorder,a related group of illnesses that forms the major differ-ential diagnosis for schizophrenia (n 4 289 parent-offspring pairs; data not shown). The subgroup analy-sis of early-AAO parents (ø34 years) (Table II), how-ever, showed no significant difference in anticipationbetween paternal and maternal transmission. A pater-nal effect on anticipation remained in the larger sub-sample of late-AAO parents (>34 years) (median antici-
pation 4 20 years and 16 years for paternal andmaternal transmission, respectively; Wilcoxon two-sample Z statistic 4 1.88, P 4 0.06), suggesting late-onset fathers as a major source of the effect.
Early-Onset Offspring (<21 Years) and SexEffects of Transmitting Parents on Anticipation
Of the 127 pairs with schizophrenia in sample I, 39pairs had an affected offspring with very young AAO(ø21 years) (Table II). The proportion of very early-AAO offspring of affected fathers (38.5%) and of af-fected mothers (27.3%) did not differ significantly (chi-square statistic 4 1.59, df 4 1, P 4 0.21). Among thevery early-AAO offspring, AAO ranged from 16–21 forpaternal transmission and 13–21 for maternal trans-mission; AAO for fathers ranged from 29–56, and AAOfor mothers ranged from 22–47. Anticipation was sig-nificantly greater with paternal transmission thanwith maternal transmission in very early-AAO off-spring (see Table II). However, the median AAO of fa-thers of very early-onset offspring was significantlyolder than that of mothers (40 years vs. 35 years, Wil-coxon two-sample Z statistic 4 2.88, P 4 0.004). Toattempt to adjust for this difference in parental AAO,we examined parental sex effects on anticipation inparents with an AAO ø40 years (8 fathers and 19mothers) and in parents with an AAO >40 years (7fathers and 5 mothers). In both subgroups, median an-ticipation was 4–5 years greater with paternal trans-mission than with maternal transmission; however,the observed paternal effect was not statistically sig-nificant in either group, probably due to small samplesizes.
Sex Effects of Unaffected Transmitting Parentson Anticipation
In sample II, consisting of 92 aunt/uncle-niece/nephew pairs with schizophrenia, there were 37 pairswith paternal transmission, and 55 pairs with mater-nal transmission (Table II). The paternal:maternal
TABLE II. Parental Sex Effects on Anticipation in Schizophrenia
Sample I: Affected parents
Subgroup analyses
All offspringEarly AAO parents
(ø34 years)Very early onset
offspring (ø21 years)Sample II: unaffected parents
all niece/nephews
Median AAO (years)Paternal(n 4 39)
Maternal(n 4 88)
Paternal(n 4 7)
Maternal(n 4 24)
Paternal(n 4 15)
Maternal(n 4 24)
Paternal(n 4 37)
Maternal(n 4 55)
Parental generationa 41 39 29 31 40b 35 35 32Offspring generationa 23 25 23 23.5 19 18.5 25 24Anticipationc 18* 14* 6*** 6** 22* 17* 9* 7*Paternal vs. maternal
difference in anticipationd Z 4 1.93 (P 4 0.05) Z 4 0.50 (P 4 0.62) Z 4 2.50 (P 4 0.01) Z 4 0.90 (P 4 0.37)
aNo significant differences found between paternal and maternal AAO for both the parental and offspring generations (Wilcoxon two-sample statistic),except as indicated in next footnote.bZ 4 2.88 (P 4 0.004).cMedian years of anticipation. The corresponding Wilcoxon matched-pairs sign-rank statistic, showing significance level of difference in median AAO from0 (null hypothesis), is indicated in the next three footnotes.dWilcoxon two-sample Z-statistic showing significance of difference in anticipation between paternal and maternal transmission.
*P 4 0.0001.**P 4 0.0335.
***P 4 0.50.
Paternal Transmission and Anticipation 159

transmission ratio of 2:3 is consistent with a degree ofreduced reproductive fitness previously observed inmen who did not have schizophrenia but who were atincreased risk of being gene carriers [Bassett et al.,1996]. Seventy-eight percent of paternally transmittedpairs and 71% of maternally transmitted pairs showedanticipation. As reported previously, the overall mag-nitude of anticipation was less than that for parent-offspring pairs [Bassett and Husted, 1997] owing to areduced role of ascertainment bias in the aunt/uncle-niece/nephew sample. In this sample, median anticipa-tion was not significantly greater for paternal than ma-ternal transmission (see Table II). This finding did notchange when the sex of the offspring generation (niece/nephew) was taken into consideration or when the sexof both the paternal and offspring generations weresimultaneously controlled for in the analyses (e.g., pa-ternal aunt-nephew pairs compared with maternalaunt-nephew pairs; data not shown). In a subsampleselected for very early-AAO nieces/nephews (ø21years), median anticipation was 14 years and 9.5 years,respectively, for paternal (n 4 9) and maternal (n 416) transmission, a nonsignificant difference (Wilcoxontwo-sample Z statistic 4 0.85, P 4 0.40).
DISCUSSION
Parental sex effects on anticipation have been ob-served for several diseases which involve a dynamicmutation containing CG-rich trinucleotide repeats(TNR) [Sutherland and Richards, 1995]. In schizophre-nia, evidence for parental sex effects would provide fur-ther support for the observed anticipation being a truephenomenon with a comparable molecular genetic ba-sis [Ranen et al., 1995]. As observed in past studies[Asherson et al., 1994; Lesch et al., 1994; Gorwood etal., 1996; Bassett and Husted, 1997], results from thecurrent study suggest that anticipation in schizophre-nia is present in transmission from both sexes. Thisstudy is, however, the first to report significantlygreater anticipation with paternal transmission thanmaternal transmission, in a relatively large sample ofparent-offspring pairs with schizophrenia. The pater-nal-maternal differences in anticipation of AAO weresubtle, in the range of 4–5 years, which could explainabsence of the finding in smaller samples [Gorwood etal., 1996]. As in HD [Ridley et al., 1988], paternal ef-fects were strongest in a subgroup of the sample withvery early-onset offspring (ø21 years). Anticipation
Fig. 2. Histograms of anticipation of AAO data (median intergenerational difference in 10-year groups) for 127 parent-offspring pairs with schizo-phrenia. Frequency of distribution (top) and percentage of cases (bottom) for paternal (black bars) and maternal (white bars) transmission are shown.
160 Husted et al.

differences were of the same magnitude but not signifi-cant in a small subsample of very early-onset niecesand nephews. Compared to single major locus disor-ders with anticipation (Table I), the results appear tobe most consistent with DM, DRPLA, and MJD, andless so with HD, where significant anticipation is aphenomenon restricted to paternal transmission [Rid-ley et al., 1988; Ranen et al., 1995]. The results are alsoconsistent in direction with a recent study of bipolar Idisorder [Grigoroiu-Serbanescu et al., 1997], a majorpsychotic disorder where anticipation has previouslybeen reported [McInnis et al., 1993].
Although the findings in the sample of parent-offspring pairs are suggestive of paternal transmissioneffects on anticipation in schizophrenia, they requirecautious interpretation. Several alternate explanationsshould be considered. One plausible explanation is thatthe slightly greater anticipation in father-offspringpairs vs. mother-offspring pairs may arise from uncon-trolled ascertainment biases. Specifically, the signifi-cant paternal effect in parent-offspring pairs may be aresult of preferential selection of late-AAO fathers, be-cause reduced reproductive fitness in men with severe,early-AAO illness led to their exclusion from study.This possibility is suggested by the absence of a signifi-cant paternal transmission effect in both the aunt/uncle-niece/nephew sample, where reproductive fitnessbiases were less, and in the subgroup of parents withearly AAO (ø34 years), although the sample size offather-offspring pairs was small (n 4 7). However,preferential ascertainment of late-AAO fathers doesnot appear to explain results for the very young AAOoffspring subsample, where there was a 4–5-year dif-ference in anticipation of AAO, whether parents had anAAO that was younger or older than the parental me-dian.
Another possibility is that if assortative mating oc-curs more frequently among affected fathers than af-fected mothers with schizophrenia, this could lead tothe finding of slightly greater anticipation for paternaltransmission. However, there is some evidence sug-gesting that the frequency of assortative mating is rela-tively rare and, when present, tends to be more fre-quent in affected mothers [Gottesman and Shields,1976]. This, along with the inclusion of only unilinealfamilies in the current study, argues against assorta-tive mating explaining the results. A third possibility isthat the sex of the affected parent influenced the like-lihood of hospitalization, and therefore entry in thesample. Men may be more likely to be hospitalized thanwomen of equal disease severity because of differencesin social expectations and symptom expression be-tween the sexes [Goldstein and Tsuang, 1990]. If thiswere the case, anticipation in maternal transmissionmay have been underestimated. While this form of as-certainment bias was unmeasured, the vast majority ofindividuals with a serious psychotic disorder are hos-pitalized, minimizing the influence of this particularbias [Link and Dohrenwend, 1980]. Alternately, gendermay influence the timing of hospitalization, particu-larly for late-AAO cases. However, there is no evidenceto suggest that late-AAO males experience a delayedhospitalization compared with late-AAO females. A
fourth limitation relates to our measure of anticipa-tion. The current study did not investigate parental sexeffects on disease severity across generations. Thismay be important, since there is conflicting evidencewith respect to parental sex effects on genetic risk ofschizophrenia. Past studies have reported that off-spring of affected mothers have a higher risk of schizo-phrenia than the offspring of affected fathers; however,other studies found no such maternal effect [Gottes-man and Shields, 1976].
Finally, since two-generation families were studied,results of this study would likely apply to familialschizophrenia with an inheritance pattern consistentwith autosomal-dominant transmission and would notpertain to all schizophrenia in the general population.Notably, the results are not consistent with either X-linked or mitochondrial transmission, which have beensuggested for bipolar disorder [Gelernter, 1995; McMa-hon et al., 1995]. The nonsignificant results for parent-of-origin effects on anticipation in aunt/uncle-niece/nephew pairs may be compatible with oligogenic inher-itance, which is likely to be the most common mode ofinheritance in schizophrenia, and with genetic hetero-geneity. Also, intrafamilial variability of AAO has beenobserved in other anticipating disorders [Howeler etal., 1989], and this may have been another factor in thediffering results between the aunt/uncle-niece/nephewand the parent-offspring samples.
If paternal transmission were truly associated withgreater anticipation for familial schizophrenia with au-tosomal-dominant-like inheritance, what implicationscould this have for the molecular genetics of schizo-phrenia? First, the finding would strengthen the evi-dence for genetic anticipation in schizophrenia and thepossibility that unstable (TNR) mutation mechanismsmay play a role in etiology. Second, the similarity tosome aspects of anticipation in DRPLA, MJD, and DMsuggests that the mechanisms proposed for those dis-orders [Brunner et al., 1993; Ikeuchi et al., 1996] maybe more applicable to schizophrenia than those impli-cated in other anticipating disorders. If adult-onset DMwere used as a model for familial schizophrenia, unaf-fected obligate carriers may be more likely to be malethan female [Brunner et al., 1993], and the chance offinding large changes in repeat size would be maxi-mized by examining father-offspring pairs. There isalso a possible relationship between mechanisms foranticipation and those proposed for genomic imprint-ing, or monoparental methylation, which causes geneinactivation [John and Surani, 1996]. The possibilitythat mechanisms related to imprinting may be actingin schizophrenia is intriguing [Flint, 1992], particu-larly given the likelihood that imprinted genes mayplay a key role in regulating development of both thebrain and behavior [Keverne et al., 1996].
In summary, the current study is unique in that itinvestigated parental sex effects on anticipation usinga relatively large and representative sample of familialschizophrenia. While the findings in the affected par-ent-offspring sample are suggestive of a paternal effecton anticipation in familial schizophrenia, it is unclearto what extent the observed phenomenon reflects atrue parental sex effect or ascertainment bias. Further
Paternal Transmission and Anticipation 161

studies of parental sex effects on anticipation, usinglarge samples and measures of both disease severityand AAO, are clearly warranted. However, it is likelythat conclusive evidence concerning parental sex ef-fects on genetic anticipation will evolve only from iden-tifying disease-causing mutations and investigatingthe molecular mechanisms of anticipation in schizo-phrenia.
ACKNOWLEDGMENTS
The authors thank Susana Correia, Brian Watada,M.D., and Suzan Williams for their work on this study.The authors are grateful to two anonymous reviewersand to Cyril Greenland, Ph.D., and Joseph Berg, M.D.,for their assistance and long-standing interest in thework of Lionel Penrose. This work was supported inpart by funding from the Canadian Psychiatric Re-search Foundation and the Medical Research Councilof Canada.
REFERENCESAsherson P, Walsh C, Williams J, Sargeant M, Taylor C, Clements A, Gill
M, Owen M, McGuffin P (1994): Imprinting and anticipation: Are theyrelevant to genetic studies of schizophrenia? Br J Psychiatry 164:619–624.
Bassett AS, Honer WG (1994): Evidence for anticipation in schizophrenia.Am J Hum Genet 54:864–870.
Bassett AS, Husted J (1997): Anticipation or ascertainment bias in schizo-phrenia? Penrose’s familial mental illness sample. Am J Hum Genet60:630–637.
Bassett AS, Bury A, Hodgkinson KA, Honer WG (1996): Reproductive fit-ness in familial schizophrenia. Schizophr Res 21:151–160.
Beiser M, Erickson D, Fleming JA, Iacono WG (1993): Establishing theonset of psychotic illness. Am J Psychiatry 150:1349–1354.
Bleuler M (1978): ‘‘The Schizophrenic Disorders: Long-term Patient andFamily Studies.’’ New Haven: Yale University Press.
Brunner HG, Bruggenwirth HT, Nillesen W, Jansen G, Hamel BCJ, HoppeRLE, de Die CEM, Howeler J, van Oost BA, Wieringa B, Ropers HH,Smeets HJM (1993): Influence of sex of the transmitting parent as wellas of parental allele size on the CTG expansion on myotonic dystrophy(DM). Am J Hum Genet 53:1016–1023.
Crow TJ (1991): A note on ‘‘Survey of cases of familial mental illness’’ byL.S. Penrose. Eur Arch Psychiatry Clin Neurosci 240:314–315.
DeLisi LE (1992): The significance of age of onset for schizophrenia.Schizophr Bull 18:209–215.
Flint J (1992): Implications of genomic imprinting for psychiatric genetics(editorial). Psychol Med 22:5–10.
Gelernter J (1995): Genetics of bipolar affective disorder: Time for anotherreinvention? Am J Hum Genet 56:1262–1266.
Goldstein JM, Tsuang MT (1990): Gender and schizophrenia: An introduc-tion and synthesis of findings. Schizophr Bull 16:179–183.
Gorwood P, Leboyer M, Falissard B, Jay M, Rouillon F, Feingold J (1996):
Anticipation in schizophrenia: New light on a controversial problem.Am J Psychiatry 153:1173–1177.
Gottesman II, Shields J (1976): A critical review of recent adoption, twin,and family studies of schizophrenia: Behavioral genetics perspectives.Schizophr Bull 2:360–401.
Grigoroiu-Serbanescu M, Wickramaratne PJ, Hodge SE, Milea S, Mihai-lescu R (1997): Genetic anticipation and imprinting in bipolar I illness.Br J Psychiatry 170:162–166.
Howeler CJ, Busch HFM, Geraedts JPM, Niermeijer MF, Staal A (1989):Anticipation in myotonic dystrophy: Fact or fiction? Brain 112:779–797.
Ikeuchi T, Igarashi S, Takiyama Y, Onodera O, Oyake M, Takano H, KoideR, Tanaka H, Tsuji S (1996): Non-Mendelian transmission in denta-torubral-pallidoluysian atrophy and Machado-Joseph disease: The mu-tant allele is preferentially transmitted in male meiosis. Am J HumGenet 58:730–733.
Jodice C, Malaspina P, Persichetti F, Novelletto A, Spadaro M, Giunti P,Morocutti C, Terrenato L, Harding AE, Frontali M (1994): Effect oftrinucleotide repeat length and parental sex on phenotypic variation inspinocerebellar ataxia I. Am J Hum Genet 54:959–965.
John RM, Surani MA (1996): Imprinted genes and regulation of gene ex-pression by epigenetic inheritance. Curr Opin Cell Biol 8:348–353.
Keverne EB, Fundele R, Narasimha M, Barton SC, Surani MA (1996):Genomic imprinting and the differential roles of parental genomes inbrain development. Dev Brain Res 92:91–100.
Lesch KP, Stober G, Balling U, Franzek E, Li SH, Ross CA, Newman M,Beckmann H, Riederer P (1994): Triplet repeats in clinical subtypes ofschizophrenia: Variation at the DRPLA (B37 CAG repeat) locus is notassociated with periodic catatonia. J Neural Transm Genet Sect 98:153–157.
Link B, Dohrenwend B (1980): Formulation of hypothesis about the ratio ofuntreated to treated cases in the true prevalence studies of functionalpsychiatric disorders in adults in the United States. In DohrenwendBP, Dohrenwend BS, Schwartz Gould M, Link B, Neugebauer R, Wun-sch-Hitzig R (eds): ‘‘Mental Illness in the United States: EpidemiologicEstimates.’’ New York: Praeger.
Lopez de Munain A, Blanco A, Emparanza JI, Marti Masso JF, Cobo A,Basauri B, Martorell L, Baiget M, Martinez Lage JM (1994): Anticipa-tion in myotonic dystrophy: A parental-sex-related phenomenon. Neu-roepidemiology 13:75–78.
McInnis MG, McMahon FJ, Chase GA, Simpson SG, Ross CA, DePaulo JRJr (1993): Anticipation in bipolar affective disorder. Am J Hum Genet53:385–390.
McMahon FJ, Stine OC, Meyers DA, Simpson SG, DePaulo JR (1995):Patterns of maternal transmission in bipolar affective disorder. Am JHum Genet 56:1277–1286.
Mott FW (1910): Hereditary aspects of nervous and mental diseases. BrMed J 2:1013–1020.
Penrose LS (1991): Survey of cases of familial mental illness. Eur ArchPsychiatry Clin Neurosci 240:315–324.
Ranen NG, Stine OC, Abbott MH, Sherr M, Codori AM, Franz ML, ChaoNI, Chung AS, Pleasant N, Callahan C, Kasch LM, Ghaffari M, ChaseGA, Kazazian HH, Brandt J, Folstein SE, Ross CA (1995): Anticipationand instability of IT-15 (CAG)N repeats in parent-offspring pairs withHuntington disease. Am J Hum Genet 57:593–602.
Ridley RM, Frith CD, Crow TJ, Conneally PM (1988): Anticipation in Hun-tington’s disease is inherited through the male line but may originatein the female. J Med Genet 25:589–595.
Sutherland GR, Richards RI (1995): Simple tandem DNA repeats and hu-man genetic disease. Proc Natl Acad Sci USA 92:3636–3641.
162 Husted et al.