Embed Size (px)
DESCRIPTION
Pathogenesis of Diseases of the Large Intestine. Dr Paul L. Crotty Department of Pathology AMNCH, Tallaght October 2008. Large intestine: by aetiology. Congenital : Anal anomalies, atresia, stenosis, Hirshsprung’s disease Acquired - PowerPoint PPT Presentation
Citation preview

Pathogenesis of Diseases of the Large
Intestine
Dr Paul L. Crotty
Department of Pathology
AMNCH, Tallaght
October 2008

Large intestine: by aetiology• Congenital: Anal anomalies, atresia, stenosis, Hirshsprung’s disease
• Acquired
• Infection: Infective enterocolitis (viral, bacterial, protozoal)
• Physical: Obstruction, Diverticular disease, Rectal mucosal prolapse
• Chemical/Toxic: NSAIDs
• Circulatory disturbances: Ischaemic bowel disease
• Immunological disturbance:
• Iatrogenic: (NSAIDs) Antibiotic-associated pseudomembranous colitis
• Idiopathic:: Crohn’s disease, ulcerative colitis
• Psychosomatic: :
• Pre-neoplastic/ Neoplastic: – Adenoma -> adenocarcinoma
– CIBD -> dysplasia -> adenocarcinoma

Fluid dynamics
Food intake: ~2 litres/d
Saliva: ~1 litre/d
Gastric secretions: ~2 litres/d
Bile: ~1 litre/d
Pancreas: ~2-3 litres/d
Small intestinal secretions: ~1 litre/d
Total 9-10 litres/d

Fluid dynamics
Re-absorption:
Small intestine: ~6 litres/d
Large intestine: normally ~2-3 litres/d
but with capacity to increase up to ~6 litres/d
Average stool weight 200-250g/d
of which 65-85% is water

Mechanisms of Diarrhoea
Secretory: increased secretions: persists after fasting. Examples: cholera, some viral infections
Osmotic: some solute present: osmotic retention of fluid in stool, resolves on fasting. Examples: disaccharidase deficiency; some viral infections
Exudative: pus present: ulceration in bowel. Examples: invasive bacterial infection: idiopathic chronic inflammatory bowel disease
Dysmotility-associated: Examples: Irritable bowel syndrome, hyperthyroidism
Malabsorption: Steatorrhoea

Chronic Inflammatory Bowel Disease
Most (but not all) can be separated into 1 of 2 patterns: (1) Crohn’s disease(2) Ulcerative colitis
based on clinical, endoscopic and pathological features

Features of both Crohn’s disease and ulcerative colitis
Idiopathic chronic inflammatory diseasesBoth have acute exacerbations and remissions
Typically onset 15-40 y: (small second peak ~ 65-70y)
- Active inflammation during acute exacerbation- Neutrophils in crypts (cryptitis, crypt abscesses)
- Over time: destruction of mucosal architecture

Crohn’s disease
- Granulomatous inflammation- May involve any part of bowel- Typically small intestine and/or colon (one third each)- Discontinuous: ‘skip lesions’ typically with rectal sparing - Aphthous ulcers early: linear ulcers later- Transmural inflammation- Wall thickening/strictures with luminal narrowing- Deep fissures/fistulas- Extra-intestinal disease- Probable small increased risk of colorectal carcinoma

Ulcerative colitis- NOT granulomatous- Colon only involved (no small bowel involvement)- Extends variable distance in continuity from rectum- Rectum always involved- Has well-defined proximal limit- No skip lesions- Broad-based ulcers with pseudo-polyps- Mucosal-based inflammation: NOT transmural- No wall thickening, no strictures,- No fissures , no fistulas- Extra-intestinal disease: also P.S.C.- Significant risk of dysplasia and carcinoma

Normal colonic mucosa

Crypt abscesses

Transmural inflammation, serosal granulomasCrohn’s colitis

Granulomas in Crohn’s disease

Fissure in Crohn’s disease

Normal

Crohn’s disease

Crohn’s disease
Crohn: 1932 [Morgagni: 1761: “ileal passion”]initially termed terminal/regional ileitis
- later identified could also have colonic involvement- later still recognised colonic-only pattern of disease
“Idiopathic”: but what do we know about its causes?

Crohn’s disease
Genetic predisposition:Sibling risk: 15-40x risk of general populationMZ twin concordance: 40-50% DZ twin concordance: 3-7%
Linkage to loci on 16 (IBD1) also chromosome 3, 12

Crohn’s disease
linkage to locus on chromosome 16: high LOD score ~ 5.8
2001: NOD2 (nucleotide-binding oligomerisation domain)- normal function as signalling protein in macrophages- activates NFkB in response to bacterial LPS
- 40% of Crohn’s disease patients: NOD2 polymorphism- but polymorphism also in ~15% of general population
- heterozygous 2-4x risk/ homozygous 40x risk

Crohn’s disease
Smoking: 2-3X increased risk of Crohn’s diseasecounterbalanced by decrease in risk of ulcerative colitis
Urban > Rural“Good” hygiene > Poor
? Theory: Delayed exposure to antigens/bacteria

Crohn’s disease
Is there an infectious agent?
Animal models do not develop disease if kept in a strict germ-free environment
Candidates??Atypical mycobacteria??Measles virus

Crohn’s disease
Is there immune dys-regulation?
Is there a defect in the normal mechanisms of suppressionof the inflammatory response to normal gut flora?
New NOD2 data supportive of this theory

Crohn’s disease
Present with pain, variable diarrhoea, feverDiagnosis: Clinical, endoscopy, mucosal biopsies, barium
Complications:Strictures: obstructionFissures: abscessesFistulas: bladder, vagina, skin, entero-entericPeri-anal diseaseMalabsorption (terminal ileal disease, blind loops)Slight increased risk of cancer

Ulcerative colitis


Pseudopolyps in ulcerative colitis

Mucosal-based inflammation and ulcerationUlcerative colitis

Dysplasia in ulcerative colitis

Ulcerative colitis

Ulcerative colitis
Wilks: 1859 claim on first distinction from dysentery
1888: RSM in London debate on aetiology of the disease? Diet ? Infection ? Psychosocial
Genetic: MZ concordanceHLA association
? Infection ? Allergy ? Immune dys-regulation

Ulcerative colitis
Mucosal inflammation leading to ulcerationChronicity leads to mucosal destruction, regeneration
40% rectum/ recto-sigmoid only40% extends from rectum to point x20% pan-colonic
Presents with diarrhoea, pain, weight lossDiagnosis: Clinical, endoscopy, biopsy

Ulcerative colitis
Complications:
Fulminant colitis: Toxic megacolon
Extra-intestinal manifestationsIncluding primary sclerosing cholangitis
Significant risk of dysplasia and malignancyespecially with pan-colitis, long duration

Large intestine: by aetiology• Congenital: Anal anomalies, atresia, stenosis, Hirshsprung’s disease
• Acquired
• Infection: Infective enterocolitis (viral, bacterial, protozoal)
• Physical: Obstruction, Diverticular disease, Rectal mucosal prolapse
• Chemical/Toxic: NSAIDs
• Circulatory disturbances: Ischaemic bowel disease
• Immunological disturbance:
• Iatrogenic: (NSAIDs) Antibiotic-associated pseudomembranous colitis
• Idiopathic:: Crohn’s disease, ulcerative colitis
• Psychosomatic: :
• Pre-neoplastic/ Neoplastic: – Adenoma -> adenocarcinoma
– CIBD -> dysplasia -> adenocarcinoma

Infective organisms causing diarrhoeaWorld-wide: mortality 5 million /year, most children
Mechanisms by which infectious agents cause diarrhoea:(1) Pre-formed toxin in food
no live organisms ingested e.g. C botulinum, some S. aureus
(2) Live organisms: Non-invasive:
(a) organisms colonise gut and produces toxine.g. V. cholerae, C. difficile, some E. coli
(b) organisms bind to brush border e.g. Cryptosporidium
Invasive:(a) mucosal e.g. Shigella, most Salmonella, some E. coli
(b) deeper layers e.g. S. typhi, Yersinia

Viral enterocolitis
Rotavirusinfects enterocytes lining villi in small intestinenear-normal/minimal shortening of villimain effect is absence of lactase => osmotic diarrhoea
Norwalk virusAdenovirusAstrovirus

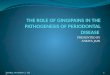
Vibrio cholerae
Toxin productionincludes binding units, catalytic unit
=> binds to glycolipid on surface of enterocyte=> catalytic unit taken up into enterocyte
=> activated intracellularly=> stimulates G-protein=> increases intracellular cAMP=> actively stimulates secretion of Na, Cl, water

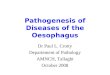
Shigella
=> stimulates its own endocytosis
=> proliferates within cell
=> rapid cell death, lysis
=> infects adjacent cells

Large intestine: by aetiology• Congenital: Anal anomalies, atresia, stenosis, Hirshsprung’s disease
• Acquired
• Infection: Infective enterocolitis (viral, bacterial, protozoal)
• Physical: Obstruction, Diverticular disease, Rectal mucosal prolapse
• Chemical/Toxic: NSAIDs
• Circulatory disturbances: Ischaemic bowel disease
• Immunological disturbance:
• Iatrogenic: (NSAIDs) Antibiotic-associated pseudomembranous colitis
• Idiopathic:: Crohn’s disease, ulcerative colitis
• Psychosomatic: :
• Pre-neoplastic/ Neoplastic: – Adenoma -> adenocarcinoma
– CIBD -> dysplasia -> adenocarcinoma

Antibiotic-associated (pseudomembranous) colitis
• Clostridium difficile in normal flora
• When other bacteria eradicated by antibiotics, C. difficile proliferates
• Selection of toxin-producing forms
• Enterotoxin (A) and cytotoxin (B)
• Disrupt cytoskeleton, inflammation
• Cell death, confluent ulceration

Antibiotic-associated (pseudomembranous) colitis

Large intestine: by aetiology• Congenital: Anal anomalies, atresia, stenosis, Hirshsprung’s disease
• Acquired
• Infection: Infective enterocolitis (viral, bacterial, protozoal)
• Physical: Obstruction, Diverticular disease, Rectal mucosal prolapse
• Chemical/Toxic: NSAIDs
• Circulatory disturbances: Ischaemic bowel disease
• Immunological disturbance:
• Iatrogenic: (NSAIDs) Antibiotic-associated pseudomembranous colitis
• Idiopathic:: Crohn’s disease, ulcerative colitis
• Psychosomatic: :
• Pre-neoplastic/ Neoplastic: – Adenoma -> adenocarcinoma
– CIBD -> dysplasia -> adenocarcinoma

Ischaemic bowel disease
• SMA, IMA -> mesenteric arcades
• collateral supply
• watershed areas: splenic flexure
• venous drainage
• acute, subacute, chronic

Ischaemic bowel disease
• Arterial thrombosis– atherosclerosis, dissection, hypercoagulation
• Arterial embolism– atherosclerosis, arrhythmias, SBE
• Venous thrombosis– hypercoagulation
• Generalised hypoperfusion– hypotensive shock, CCF

Ischaemic bowel disease• Transmural infarction
– acute occlusion (arterial or venous, thrombotic or embolic) -> acute abdomen
– perforation/gangrene if untreated
• Mucosal/submucosal infarction– acute/subacute hypoperfusion– can mimic acute colitis
• Fibrosis and mucosal atrophy– chronic, strictures: can mimic Crohn’s




Large intestine: by aetiology• Congenital: Anal anomalies, atresia, stenosis, Hirshsprung’s disease
• Acquired
• Infection: Infective enterocolitis (viral, bacterial, protozoal)
• Physical: Obstruction, Diverticular disease, Rectal mucosal prolapse
• Chemical/Toxic: NSAIDs
• Circulatory disturbances: Ischaemic bowel disease
• Immunological disturbance:
• Iatrogenic: (NSAIDs) Antibiotic-associated pseudomembranous colitis
• Idiopathic:: Crohn’s disease, ulcerative colitis
• Psychosomatic: :
• Pre-neoplastic/ Neoplastic: – Adenoma -> adenocarcinoma
– CIBD -> dysplasia -> adenocarcinoma

Diverticular disease
• Diverticulum: blind pouch off GI tract
• Incidence: 40-50% in >60 years in West
• Diet low in fibre -> decreased stool volume
• Chronic increased intraluminal preseeure
• Acquired ‘blow-out’ diverticuli– at points of focal weakness in wall of colon
where vessels cross muscle layer

Diverticular disease
• Complications
• Inflammation
• Abscess formation
• Perforation
• Bleeding