Embed Size (px)
Citation preview

129
Journal of Neuropathology and Experimental Neurology Vol. 63, No. 2Copyright q 2004 by the American Association of Neuropathologists February, 2004
pp. 129 137
Multifocal Motor Neuropathy: Pathologic Alterations at the Site of Conduction Block
BRUCE V. TAYLOR, MD, P. JAMES B. DYCK, MD, JANEAN ENGELSTAD, HT, GREGORY GRUENER, MD,IAN GRANT, MD, AND PETER J. DYCK, MD
Abstract. The pathologic changes of nerves in multifocal motor neuropathy (MMN), a rare neuropathy with selective focalconduction block of motor fibers in mixed nerves, remain essentially unstudied. Fascicular nerve biopsy of 8 forearm or armnerves in 7 patients with typical MMN was undertaken for diagnostic reasons at the site of the conduction block. Abnormalitieswere seen in 7 of 8 nerves, including a varying degree of multifocal fiber degeneration and loss, an altered fiber sizedistribution with fewer large fibers, an increased frequency of remyelinated fiber profiles, and frequent and prominent regen-erating fiber clusters. Small epineurial perivascular inflammatory infiltrates were observed in 2 nerves. We did not observeovert segmental demyelination or onion bulb formation. We hypothesize that an antibody-mediated attack directed againstcomponents of axolemma at nodes of Ranvier could cause conduction block, transitory paranodal demyelination and remye-lination, and axonal degeneration and regeneration. Alternatively, the antibody attack could be directed at components ofparanodal myelin. We favor the first hypothesis because in nerves studied by us, axonal pathological alteration predominatedover myelin pathology. Irrespective of which mechanism is involved, we conclude that the unequivocal multifocal fiberdegeneration and loss and regenerative clusters at sites of conduction block explains the observed clinical muscle weaknessand atrophy and alterations of motor unit potentials. The occurrence of conduction block and multifocal fiber degenerationand regeneration at the same sites suggests that the processes of conduction block and fiber degeneration and regenerationare linked. Finding discrete multifocal fiber degeneration may also provide an explanation for why the functional abnormalitiesremain unchanged over long periods of time at discrete proximal to distal levels of nerve and may emphasize a need forearly intervention (assuming that efficacious treatment is available).
Key Words: Axonal degeneration; Multifocal motor neuropathy; Nerve fiber degeneration; Regenerating nerve clusters.
INTRODUCTION
Multifocal motor neuropathy with persistent conductionblock (MMN-PCB, or simply MMN) is a rare neuropathyclinically characterized by multiple pure motor mononeu-ropathies and electrophysiologically by persistent motorconduction block. It has a predilection for the upper limbs,particularly the forearm segments of mixed nerves, and of-ten results in asymmetrical painless wasting and weaknessof the hands. Sensory or autonomic nerve involvement andupper motor neuron signs or symptoms are atypical of thedisorder (1).
The regions of focal motor conduction block of limbnerves are not at common compression sites and these sitesdo not change over long periods of time. Sensory fibersremain unblocked. The exact criteria for conduction blockare somewhat controversial but there is agreement on gen-eral principles (2). We have proposed diagnostic criteria,
From Peripheral Neuropathy Research Center (PJBD, JE, PJD), De-partment of Neurology, Mayo Clinic and Mayo Foundation, Rochester,Minnesota. This report was initiated while Drs. Taylor, Gruener, andGrant were visiting clinicians or peripheral nerve fellows in the Periph-eral Neuropathy Research Center, Department of Neurology, MayoClinic and Mayo Foundation, Rochester, Minnesota. Their present af-filiations are Department of Neurology (GG), Loyola University Chi-cago, Maywood, Illinois; Department of Neurology (BVT), Royal Ho-bart Hospital, Hobart Tasmania, Australia; Division of Neurology (IG),QE II Health Sciences Center, Halifax, Nova Scotia, Canada.
Correspondence to: Peter J. Dyck, MD, Mayo Clinic, 200 First StreetSW, Rochester, MN 55905. E-mail: [email protected]
Supported in part by grants obtained from the National Institute ofNeurological Diseases and Stroke (NINDS 36797) and Mayo Founda-tion.
which we use for the identification of our cases (1). How-ever, lesser degrees or no conduction block could conceiv-ably occur in a subset of patients with the same disorder(3–5).
The pathologic changes underlying the muscle weak-ness and atrophy and motor unit potential change and theconduction block have been studied in only a few pa-tients, presumably because nerve tissue at sites of con-duction block was not available for study. The presenceof conduction block in motor fibers and the other clinicaland electromyographic findings have been taken by someauthors as evidence of demyelination with secondary ax-onal degeneration resulting in denervation and atrophy(6, 7). Other authors have speculated that a functionalblock at nodes of Ranvier results in block of saltatoryconduction (8). This finding has been supported by recentwork suggesting that the axon distal to the site of con-duction block in MMN is hyperpolarized with similarelectrical properties to that seen in ischemic axons andconsistent with dysfunction of the voltage gated Na1/K1
channels (9).It is generally felt that MMN is an autoimmune dis-
order based on the response to immunomodulating ther-apy (10–14) and an association with high titers of anti-ganglioside antibodies in a proportion of cases (15–17).
Two previous pathological studies of individual casesof MMN have been reported. Auer et al (18) reported apatient with onion bulbs and pure motor manifestations.Clinically, their patient probably had MMN. They biop-sied a proximal ulnar nerve and reported finding a chron-ic demyelinating process and onion bulbs. We note that
Downloaded from https://academic.oup.com/jnen/article-abstract/63/2/129/2916522by gueston 09 March 2018

130 TAYLOR ET AL
J Neuropathol Exp Neurol, Vol 63, February, 2004
frank demyelination was not seen and that a regenerativecluster is shown in one of their figures. The MMN caseof Kaji et al is informative in that focal segmental de-myelination and remyelination and onion bulbs are illus-trated (19). Neither of these reports provides an expla-nation for the obvious muscle weakness and atrophy andmotor unit potential changes that are characteristic ofmany chronic cases. Corse et al have reported minorchanges in the sural nerves of patients with MMN, butsince the sural nerve is not known to be affected inMMN, pathological inferences to MMN may not be jus-tified (20).
The present report focuses on the pathologic alterationsin fascicular biopsy specimens of forearm or arm nervesat the site of conduction block of a series of patients withwell-documented typical MMN.
MATERIALS AND METHODS
All patients met our previously published clinical and elec-trophysiological criteria for MMN (1). The clinical features ofpatients 2 through 6 have been included in previous reports (1).Fascicular biopsies of forearm or arm nerves were obtained atsites of conduction block for diagnostic and treatment consid-erations to ascertain whether a treatable pathologic alteration(e.g. inflammatory demyelination, necrotizing vasculitis, gran-uloma, a constrictive lesion, or tumor) was present. We sub-mitted and obtained permission from the Institutional ReviewBoard and from the patient to study the dossier medical recordsand tissues for research purposes.
Before biopsy the anatomical location of the nerve and thesite of the lower edge of the conduction block was determinedand marked on the skin. After surgical exposure of the nervethe epineurium was slit longitudinally to expose individual orsmall groups of fascicles. Intraoperatively, sutures were used tolightly elevate fascicles from the nerve bed so that individualor small groups of fascicles could be stimulated by microelec-trodes to identify fascicles with motor fibers and the distal siteof conduction block. Such fascicles, or preferably 2 to 3 fas-cicles (so as to have some intervening epineurial tissue), werebiopsied from a point approximately 2.5 cm above, to about2.5 cm below the distal edge of conduction block. The proce-dures we use for nerve fixation, histological processing, andevaluation have been described (21). As for all nerve biopsies,we maintained the proximal to distal identity of tissue blocksand the proximal to distal orientation of individual blocks. Inall cases where sufficient tissue was available, teased fibers andepoxy sections (for light and electron microscopy) were pre-pared from tissue blocks at several levels to assess proximal todistal changes.
Our interactive system for nerve morphometry (ISNM) wasused for morphometric studies of all fascicles and of sectionsof proximal to distal blocks to assess for proximal to distalchanges and to determine fiber density, fiber size distribution,number of regenerating clusters, and number of degeneratingnerve fiber profiles. The approaches used in the developmentof ISNM have been extensively described and validated andextensively employed in experimental and clinical studies (21–25).
Systematic sampling is used both for study of teased fibersand morphometric assessment so as to avoid biased selectionof fibers or frames for analysis. For teased fibers, the fascicularendoneurium is divided into 50 strands of nerve tissue andsmall strands of endoneurial tissue are teased from the righthand side of each of these 50 strands, whether the tissue con-tains fibers or not. By this approach we avoid selecting strandsof tissue with large-diameter fibers. Likewise in morphometricassessment, the transverse fascicular area is subdivided intorectangular frames. We begin by determining the frequency offrames to be evaluated (e.g. 1 in 3 frames). Then we traversethe endoneurial area in an x and y direction. The first frame tobe evaluated is chosen by chance and thereafter every thirdframe (partial or whole) is evaluated. This approach ensuressystematic sampling of the entire cross-sectional endoneurium.
No control biopsy tissue obtained at biopsy and processedby the same techniques was available for comparison. However,the histological features of paraffin sections and morphometryof myelinated fibers in semithin epoxy sections of 2 ulnar fore-arm nerves, taken within 6 hours of death from patients withoutneurologic disease, were studied for comparative purposes.
RESULTS
The demographic, clinical, and electrophysiologicalfeatures of the 7 patients are given in Table 1. Thesefeatures are typical for patients with MMN (21, 26). Themajor pathologic findings were a marked reduction of thenumbers of myelinated fibers (Fig. 1) in transverse sec-tions of nerve, focal, and multifocal regions. These re-gions were almost devoid of large fibers with mostlysmall fibers remaining. In some sections there appearedto be an increased number of intermediate-sized fiberswith thin myelin. By electron microscopy many of thesmall fibers were in regenerative clusters (Fig. 2), show-ing increased frequency of degenerating axons and smallperivascular lymphocyte infiltrates (Fig. 3). Paranodal orinternodal demyelination (absent myelin) or onion bulbformations were not seen. These changes are describedin more detail below.
Teased Fibers
Examination of teased nerve fiber preparations fromall nerves and in 5 nerves from at least 2 levels of thesame nerve revealed a low rate of axonal degeneration(median 4%, range 1%–10%) of classifiable fibers. Al-though we only have anecdotal information about the fre-quency of axonal degeneration from mixed nerves of theupper limbs in controls, we judge the frequency to beincreased in some of the nerves. Teased fibers with un-equivocal de- and remyelination were infrequent andprobably not more frequent than in controls. A proximalto distal gradient of teased fiber change was not observed.
Paraffin and Epoxy Sections
Light microscopy of transverse and longitudinal par-affin sections revealed no major alterations of nerve ar-chitecture. The most striking abnormality found in epoxy
Downloaded from https://academic.oup.com/jnen/article-abstract/63/2/129/2916522by gueston 09 March 2018

131CONDUCTION BLOCK ALTERATIONS IN MULTIFOCAL MOTOR NEUROPATHY
J Neuropathol Exp Neurol, Vol 63, February, 2004
TABLE 1Clinical Electrophysiological and Demographic Features of 7 MMN Cases
Case SexAge at timeof biopsy
Sites of definiteconduction blocks
Diseaseduration
NIS at timeof biopsy
Response totherapy Atypical features
1234567
FMMMMFF
51 years29 years29 years48 years47 years64 years51 years
RU, LPLU, LMLU, LP, LTRM, LR, LMLU, LMCRM, LM, RU, RPRM, RMC, LM, LU
6 Years5 Years2 Years6 Years
22 Years3 Years
20 Years
24.5295.5
19127.520.539
UncertainMarkedModerateMarkedMildMarkedModerate
NoneNoneType 1 DM 23 yearsNoneNoneNoneNo
All conduction blocks were graded as definite according to the criteria of Taylor et al (1). Disease duration is the time fromsymptom onset to biopsy. All nerve conduction studies and determination of sites of definite block were performed just prior tobiopsy. Abbreviations: RU, right ulnar; LU, left ulnar; LM, left median; RM, right median; LMC, left musculocutaneous; RMC,right musculocutaneous; LR, left radial; RP, right peroneal; LP, left peroneal; LT, left tibial; NIS, neuropathy impairment score;DM, diabetes mellitus.
semithin transverse sections was a reduction in fiber den-sity, which was distributed multifocally among and with-in fascicles in the nerve of case 5 (Fig. 1). These regionsof fiber decrease were also characterized by a remarkablealteration of fiber size (fewer large-diameter fibers andincreased numbers of small- and intermediate-diameterfibers). When these regions of decreased fiber densitywere viewed under light and electron microscopes, thedecrease in large fibers was evident but many of the smallfibers (;2–4 mm in diameter) were clustered close to-gether in a pattern of regenerating nerve sprouts (Fig. 2).In a few cases, they were surrounded by a common base-ment membrane, although in other cases the basementmembrane had disappeared but the close apposition offibers appeared to have been retained. There were trans-verse profiles of single, small- and intermediate-diametermyelinated fibers that could have represented remyeli-nated segments. No unequivocally demyelinated profilesor onion bulbs (indicators of myelin remodeling) wereseen. Apart from the small inflammatory collections seenin paraffin sections, no obvious interstitial pathologic ab-normality explained this fiber decrease. We did not findevidence other than multifocal fiber loss that could beinterpreted to be from ischemia. For example, we did notfind perineurial necrosis, necrotizing vasculitis, bleeding,injury neuroma, neovascularization, or accumulation ofaxonal organelles). Most nerves (7 of 8) showed changessimilar to, but less pronounced, than those described incase 5 (Fig. 1). Cases 1, 4R, 5, and 6 showed the mostprominent abnormalities, with increased numbers of re-generating clusters, more small- and intermediate-sizedfibers, and few large fibers. Some of the intermediate-sized myelinated fibers had thin myelin (Fig. 4, left mid-dle panel). The nerve of case 2 and 7 were relativelynormal.
Small perivascular lymphocytic infiltrates were ob-served in case 1 and 2 (Fig. 3). In case 1, it was seen inthe outer layers of the perineurium. In case 2, it was also
in the perineurium and extended into the endoneurium.Paraffin sections were reacted for common leukocyte an-tigen (CD 45) and for macrophages (CD 68), but affectedareas did not show additional inflammatory infiltrates tothose already described.
Morphometry
The studies are summarized in Table 2 and illustratedin Figure 4. Direct comparison with normative data wasnot possible because nerve taken at biopsy were unavail-able for comparison. The 2 postmortem nerves assesseddemonstrated no active fiber de- or regeneration and nofocal fiber density decrease (Table 2).
Similar to the light microscopy findings, morphometrydemonstrated abnormalities in 7 of 8 nerves studied, withrelative decrease of large myelinated fibers and relativeincrease in the number of small fibers. In the more se-verely affected nerves there was an increase in the indexof dispersion among frames consistent with multifocalfiber loss (Table 2). The fiber density in case 6 and case4R may be increased due to the large numbers of regen-erating clusters (groups of small, thinly myelinated fi-bers). Case 7 demonstrated changes only on nerve mor-phometry with an altered size distribution, increasedindex of dispersion, and increased numbers of regener-ating fiber clusters. The relative decrease of large mye-linated fibers and relative increase of small fibers is il-lustrated in Figure 4. Plots of the relationship of axondiameter to myelin thickness revealed differences amongnerves. Whereas case 2 had many large fibers with thickmyelin, the more severely affected nerves (case 4R, case6, and case 5) demonstrated smaller axons with thinnermyelin. A definitive electron microscopic study of axondiameter (from area) on number of myelin lamellae wasnot possible because only necropsy forearm controlnerves were available for study.
Downloaded from https://academic.oup.com/jnen/article-abstract/63/2/129/2916522by gueston 09 March 2018

132 TAYLOR ET AL
J Neuropathol Exp Neurol, Vol 63, February, 2004
Downloaded from https://academic.oup.com/jnen/article-abstract/63/2/129/2916522by gueston 09 March 2018

133CONDUCTION BLOCK ALTERATIONS IN MULTIFOCAL MOTOR NEUROPATHY
J Neuropathol Exp Neurol, Vol 63, February, 2004
←
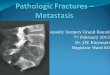
Fig. 1. Transverse sections of a fascicular biopsy of ulnar nerve from case 5 showing striking foci of myelinated fiber decrease(upper frames). The rectangles in upper frames are shown at greater magnification in lower frames. In addition to decreaseddensity of myelinated fibers, there is a striking alteration of size distribution (fewer large fibers) and prominent regeneratingclusters (arrowhead).
Fig. 2. Low-power scanning electron micrograph of an area of nerve with decreased density of myelinated fibers (case 5).The clusters of closely applied small myelinated fibers are indicative of there being regenerating fibers. The significance of thisfinding is discussed in the text.
Electron Microscopy
Electron microscopy of regions of large myelinated fi-ber decrease (e.g. case 5) demonstrated the presence ofunmyelinated fibers, stacks of Schwann cell processes,and regenerating clusters of small, thinly myelinated fi-bers (Fig. 4). There were no intracellular inclusions seenand no abnormal organelles seen within Schwann cellnuclei or axons. The myelin sheaths of unaffected mye-linated fibers appeared morphometrically normal with noalteration in spacing of lamellae.
DISCUSSION
The findings presented here are of importance becausethey focus on the pathological alterations at or near themost common sites of conduction block in forearm orarm nerves of patients with MMN. The principle findingsof our studies are somewhat at variance with these earlierfindings, but the differences may be explained by differ-ences in the acuteness of the pathologic lesions—our cas-es perhaps being more chronic. Unlike the findings of
earlier investigators of single cases, we found focal andmultifocal regions of fiber decrease (especially of largefibers), an altered size distribution, regenerating fiberclusters, and a low frequency of fiber degeneration. Thedecrease in fiber density (especially of large fibers) infocal or multifocal regions, alteration in size distribution,the presence of regenerating clusters, and low-grade ax-onal degeneration was seen to varying degrees in 7 of 8nerves. Although we did not find paranodal or internodalsegmental demyelination or onion bulbs, some interme-diate-sized fibers with thin myelin were seen, perhapsindicative of previous remyelination.
Our results provide an improved understanding of theclinically observed muscle atrophy and fibrillation andmotor unit potential change in MMN. Degeneration ofmotor axons of limb nerves appears to account for theseclinical and electrophysiologic changes. This conclusionis inferred from intraoperative electrophysiologic record-ings, showing that fascicles that were biopsied containedmotor fibers and demonstrated conduction block. The bi-opsied fascicles appeared to have an increased frequency
Downloaded from https://academic.oup.com/jnen/article-abstract/63/2/129/2916522by gueston 09 March 2018

134 TAYLOR ET AL
J Neuropathol Exp Neurol, Vol 63, February, 2004
Downloaded from https://academic.oup.com/jnen/article-abstract/63/2/129/2916522by gueston 09 March 2018

135CONDUCTION BLOCK ALTERATIONS IN MULTIFOCAL MOTOR NEUROPATHY
J Neuropathol Exp Neurol, Vol 63, February, 2004
←
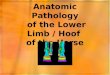
Fig. 3. Upper panel: Transverse paraffin section stained with hematoxylin and eosin to show a minute perivascular inflam-matory cell infiltrate near the inner aspect of the perineurium (case 2). Lower panel: Transverse epoxy section stained withmethylene blue and showing a small perivascular inflammatory cell infiltrate just outside the perineurium (case 1). The significanceis unclear but may be in keeping with an autoimmune process. The findings are discussed in text.
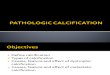
Fig. 4. Representative sections from nerves of patients with multifocal motor neuropathy. The panels on the left show lesssevere changes than those shown in Figure 1. The panels on the right show no change. Although the density of fibers (left) isprobably normal, there is a marked alteration of the diameter distribution (more small- and intermediate-sized fibers and fewlarge fibers). The nerve shown on the right appears to have a normal distribution of fiber diameters. The nerve shown on theright was from case 2, the one on the left from case 6.
Downloaded from https://academic.oup.com/jnen/article-abstract/63/2/129/2916522by gueston 09 March 2018

136 TAYLOR ET AL
J Neuropathol Exp Neurol, Vol 63, February, 2004
TABLE 2Interactive System for Nerve Morphometry Results for 8 MMN Nerves and 2 Control Ulnar Nerves of Forearm
Obtained at Necropsy
Nerve andlevel (L)
Number offascicles
Index ofdispersion
DensityMF/mm2 Clusters mm2 DPs mm2 MF diameter
Control 1Control 2Case 1Case 2 L1L2L3Case 3
6211111
1.411.851.381.351.101.241.66
7003872787957177732377879342
00
1640409
00
30044
2085
6.3906.3514.6449.0449.4167.7756.059
Case 4 L1Right L2Case 4 L1Left L2Case 5Case 6 L1L2L3Case 7
232132115
1.602.821.670.763.204.631.442.122.72
10,63510,663
785179104933
11,89310,334
96238095
1922291474
128159530
28
26131930
12320867
1210
4.8485.6968.0607.3806.0374.8376.0295.5845.375
* Median values.Clusters are groups of small thinly myelinated fibers presumably originally contained in a common basement membrane
remaining after degeneration of a myelinated fiber. All densities are per mm2 of endoneurium. Abbreviations: MF, myelinatedfiber; DP, degenerating profile (nerve fiber undergoing active degeneration).
of degenerating fibers and, perhaps more dramatically,had multifocal regions of fiber decrease with many re-generating sprouts in them. Our histologic studies, there-fore, provide unequivocal evidence of a multifocal pro-cess affecting motor fibers of limb nerves resulting infiber degeneration. In addition, abortive nerve regenera-tion was prominent in these regions of fiber loss.
The issue of whether any of these regenerated sproutscan or do regrow and re-innervate muscle target remainsunclear, although the alteration of motor unit potentialsuggests that some do. Although there is information onthe characteristic features of regenerative sprouts, little isknown about the time course of development and dis-appearance of regenerative nerve clusters. It is assumedthat some regenerating axons re-innervate previously de-nervated muscle.
The degree of focal fiber loss and regenerative sprout-ing may also provide an explanation for why patientswith MMN tend to be refractory to treatment. In our ex-perience, despite intensive treatment with intravenousgamma globulin or cyclophosphamide for long periodsof time, patients with this disease may show only partialimprovement, being left with considerable clinical deficit.
Our studies provide unequivocal evidence that thepathologic lesions of forearm nerves are focal and mul-tifocal and are at fixed proximal to distal levels of nerve.Finding discrete regions of fiber decrease, altered sizedistribution, and regenerative clusters suggests that thesefoci are near the proximal level of the lesions because ifthey were not, a greater spread of pathologic abnormal-ities would have been seen. It is further noted that these
foci occur in the general region of conduction block, pro-viding a linkage between conduction block and fiber de-generation and regeneration (see below). Conductionblock may be an earlier and milder alteration than theobvious axonal degeneration, fiber loss, and regenerativesprouting we have observed here. Apart from the knownselective vulnerability of motor fibers (i.e. the mid-fore-arm location of many of the lesions), the reason for sitesof involvement remains unexplained.
Can the findings of conduction block, segmental de-myelination, and remyelination by Auer et al (18) andKaji et al (19) be reconciled with our studies showingmultifocal fiber loss and abortive regeneration? We hy-pothesize that an antibody-mediated attack directedagainst components of the axolemma of nodes of Ranvier,if mild, could explain the conduction block and, if moresevere, could induce transitory demyelination (and vary-ing degrees of remyelination) and axonal degeneration(and regeneration, perhaps mainly abortive). Alternative-ly, an attack on components of paranodal myelin couldalso explain both segmental demyelination and axonaldegeneration and regeneration. We favor the first hypoth-esis because anti-ganglioside antibodies are thought to bedirected at components of axolemma and because wefound prominent fiber loss and abortive regenerationwithout finding overt segmental demyelination or onionbulbs.
The small inflammatory infiltrates seen in 2 cases areof unclear pathological significance but may suggest aninflammatory or immune component. Although we ac-cept Kaji et al’s evidence for the occurrence of segmental
Downloaded from https://academic.oup.com/jnen/article-abstract/63/2/129/2916522by gueston 09 March 2018

137CONDUCTION BLOCK ALTERATIONS IN MULTIFOCAL MOTOR NEUROPATHY
J Neuropathol Exp Neurol, Vol 63, February, 2004
demyelination and remyelination in MMN, it appears thatit is not a prominent feature in chronic cases.
A physiological block of motor axons based on an an-tibody-mediated blockade or damage of Na1, K1 chan-nels at the nodes of Ranvier could explain conductionblock in MMN. Takigawa et al (8) demonstrated alter-ations in K1 currents at nodes of Ranvier using a voltageclamp technique of isolated single myelinated rat nervefibers using anti-ganglioside (GM1) antibodies and com-plement. They concluded that anti-GM1 antibodies maybe able to uncover potassium channels in the paranodalregions, while GM1 antibodies in the presence of com-plement may form antibody complexes that block sodiumchannels and disrupt the membrane at the nodes of Ran-vier. The findings by Kiernan (9) of hyperpolarization ofthe axon distal to the site of conduction block in MMNpatients are also supportive of a functional block. Ac-cording to his view, functional conduction block, if moresevere or prolonged, could cause axonal degeneration.The fact that others (18, 19), and now we, have shownmorphologic changes at sites of conduction block sug-gests that more than a functional block develops.
An antibody-mediated channelopathy could explain theinitial response to therapy seen with immunomodulatingtherapy, particularly IVIg, where neutralization of neu-romuscular blocking antibodies by IVIg has been dem-onstrated in GBS, and a similar mechanism may be op-erative in MMN (27). The subsequent pathologicalteration of fibers (segmental remodeling and axonal de-generation and regeneration) could then explain the de-creasing responses to treatment with time with the de-velopment of irreversible muscle atrophy.
The pathologic changes we have described have ther-apeutic implications. Our findings suggest that functionalalterations precede fiber degeneration and faulty regen-eration. Therefore, if available, early and adequate treat-ment would be preferable to delayed treatment.
REFERENCES
1. Taylor BV, Wright RA, Harper CM, Dyck PJ. Natural history of 46patients with multifocal motor neuropathy with conduction block.Muscle Nerve 2000;23:900–908
2. Olney RK. Consensus criteria for the diagnosis of partial motorconduction block. Muscle Nerve 1999;22(Suppl 8):S225–S229
3. Cappellari A, Nobile-Orazio E, Meucci N, Levi Minzi G, ScarlatoG, Barbieri S. Criteria for early detection of conduction block inmultifocal motor neuropathy (MMN): A study based on controlpopulations and follow-up of MMN patients. J Neurol 1997;244:625–30
4. Felice KJ, Goldstein JM. Monofocal motor neuropathy: Improve-ment with intravenous immunoglobulin. Muscle Nerve 2002;25:674–78
5. Pakiam AS, Parry GJ. Multifocal motor neuropathy without overtconduction block. Muscle Nerve 1998;21:243–45
6. Katz JS, Wolfe GI, Bryan WW, Jackson CE, Amato AA, BarohnRJ. Electrophysiological findings in multifocal motor neuropathy.Neurology 1997;48:700–707
7. Chaudhry V. Multifocal motor neuropathy. Seminars in Neurology1998;18:73–81
8. Takigawa T, Yasuda H, Kikkawa R, Shigeta Y, Saida T, KitasatoH. Antibodies against GM1 ganglioside affect K1 and Na1 cur-rents in isolated rat myelinated nerve fibers. Ann Neurol 1995;37:436–42
9. Kiernan MC, Guglielmi JM, Kaji R, Murray NM, Bostock H. Ev-idence for axonal membrane hyperpolarization in multifocal motorneuropathy with conduction block. Brain 2002;125:664–75
10. Azulay JP, Rihet R, Pougert J, et al. Long-term follow-up of mul-tifocal motor neuropathy with conduction block under treatment. JNeurol Neurosurg Psychiatry 1997;62:391–94
11. Leger JM, Chassande B, Musset L, Meininger V, Bouche P, Bau-mann N. Intravenous immunoglobulin therapy in multifocal motorneuropathy: A double-blind, placebo-controlled study. Brain 2001;124:145–53
12. Carpo M, Allaria S, Scarlato G, Nobile-Orazio E. Marginally im-proved detection of GM1 antibodies by Covalink ELISA in mul-tifocal motor neuropathy. Neurology 1999;53:2206–7
13. Van den Berg LH, Franssen H, Wokke JHJ. The long-term effectof intravenous immunoglobulin treatment in multifocal motor neu-ropathy. Brain 1998;121:421–28
14. Federico P, Zochodne DW, Hahn AF, Brown WF, Feasby TE. Mul-tifocal motor neuropathy improved by IVIg: Randomized, double-blind, placebo-controlled study. Neurology 2000;55:1256–62
15. Pestronk A, Choksi R. Multifocal motor neuropathy. Serum IgManti-GM1 ganglioside antibodies in most patients detected suingcovalent linkage of GM1 to ELISA plates. Neurology 1997;49:1289–92
16. Taylor BV, Gross L, Windebank AJ. The sensitivity and specificityof anti-GM1 antibody testing. Neurology 1996;47:951–55
17. Willison HJ. Antiglycolipid antibodies in peripheral neuropathy:Fact or fiction. J Neurol Neurosurg Psychiatry 1994;57:1383–87
18. Auer RN, Bell RB, Lee MA. Neuropathy with onion bulb forma-tions and pure motor manifestations. Can J Neurol Sci 1989;16:194–97
19. Kaji R, Oka N, Tsuji T, et al. Pathological findings at the site ofconduction block in multifocal motor neuropathy. Ann Neurol1993;33:152–58
20. Chaudhry V, Corse A, Cornblath D, et al. Maintenance immuneglobulin therapy for multifocal motor neuropathy: Results of long-term follow-up. Ann Neurol 1996;40:513–14
21. Dyck PJ, Giannini C, Lais A. Pathologic alterations of nerves. In:Dyck PJ, Thomas PK, Low PA, Griffin JW, Poduslo JF, eds. Pe-ripheral neuropathy, 3rd ed. Philadelphia: W.B. Saunders, 1993:514–95
22. Karnes J, Robb R, O’Brien PC, Lambert EH, Dyck PJ. Comput-erized image recognition for morphometry of nerve attribute ofshape of sampled transverse sections of myelinated fibers whichbest estimates their average diameter. J Neurol Sci 1977;34:43–51
23. Zimmerman IR, Karnes JL, O’Brien PC, Dyck PJ. Imaging system fornerve and fiber tract morphometry: Components, approaches, perfor-mance, and results. J Neuropathol Exp Neurol 1980;39:409–19
24. Dyck PJ, Karnes J. Morphometry of neuron columns and fibertracts in neurobiology and pathology using computer imaging.Trends Neurosci 1981;4:138–41
25. Dyck PJ, Dyck PJB, Giannini C, Sahenk Z, Windebank AJ, En-gelstad J. Peripheral Nerves. In: Graham DI, Lantos PL, eds. Green-field’s neuropathology. London: Arnold Publishing, 2002: 551–675
26. Nobile-Orazio E. Multifocal motor neuropathy. J Neuroimmunol2001;115:4–18
27. Buchwald B, Ahangari R, Weishaupt A, Toyka KV. Intravenousimmunoglobulins neutralize blocking antibodies in Guillain BarreSyndrome. Ann Neurol 2002;51:673–80
Received July 10, 2003Revision received October 14, 2003Accepted October 16, 2003
Downloaded from https://academic.oup.com/jnen/article-abstract/63/2/129/2916522by gueston 09 March 2018