Embed Size (px)
Citation preview
7/29/2017
1
Getting the Most Out of Skin BiopsiesTammie Ferringer, MD
Section Head and Fellowship Director of DermatopathologyDepts of Dermatology and Pathology
Danville, [email protected]
I have no relevant relationships with industry.
Pathologists are from MarsClinicians are from Venus
Maximizing Your Inflammatory Biopsy
Where to biopsy
Type of biopsy
Specific scenarios
Communication
Maximizing Your Inflammatory Biopsy
Where to biopsy
Type of biopsy
Specific scenarios
Communication
Choosing Biopsy Location In addition to considering….
site of scar
ease of post-op care
Most developed lesion
except
Early lesion if vesiculobullous, pustular, or vasculitis
Choosing Biopsy Location
Avoid necrosed, scratched, or traumatized areas
Avoid the site of the KOH
Avoid the lower leg
7/29/2017
2
Choosing Biopsy Location
Untreated lesion
More than one morphology, more than one biopsy
Incidental Lesion
Maximizing Your Inflammatory Biopsy
Where to biopsy
Type of biopsy
Specific scenarios
Communication
How would you biopsy this rash?
A) Punch
B) Shave
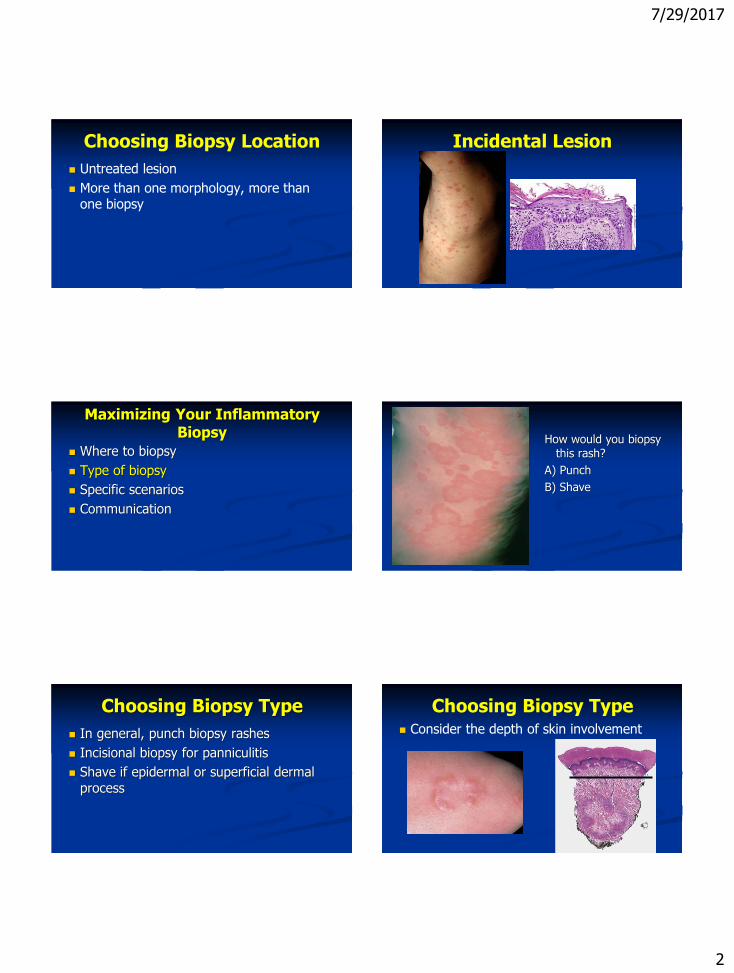
Choosing Biopsy Type
In general, punch biopsy rashes
Incisional biopsy for panniculitis
Shave if epidermal or superficial dermal process
Consider the depth of skin involvement
Choosing Biopsy Type
7/29/2017
3
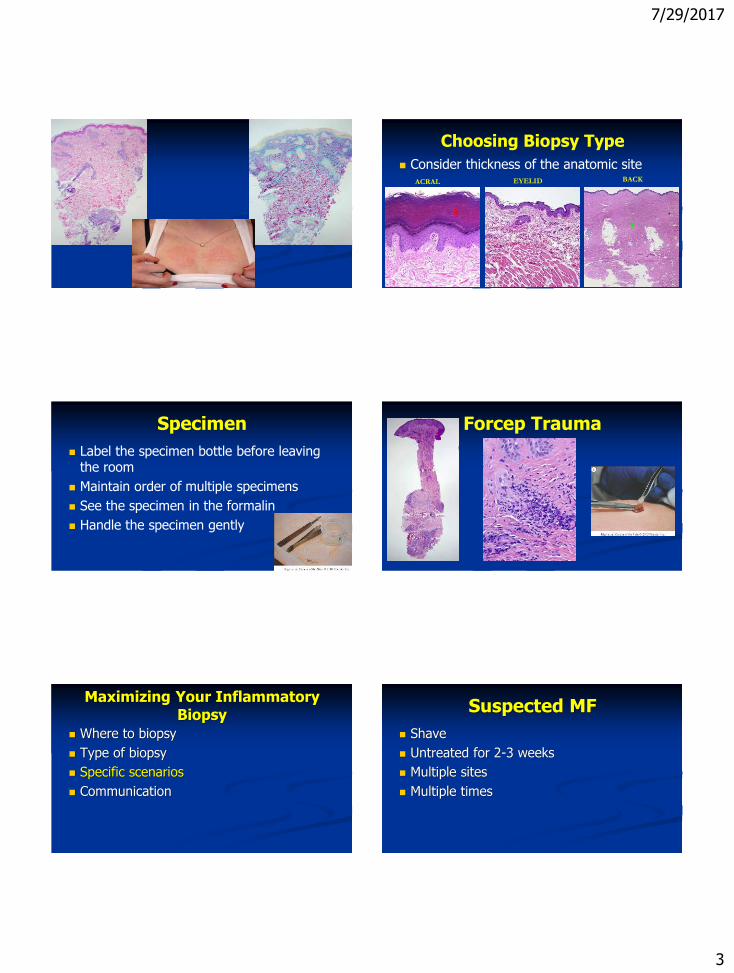
Choosing Biopsy Type
ACRAL BACKEYELID
Consider thickness of the anatomic site
Specimen
Label the specimen bottle before leaving the room
Maintain order of multiple specimens
See the specimen in the formalin
Handle the specimen gently
Forcep Trauma
Maximizing Your Inflammatory Biopsy
Where to biopsy
Type of biopsy
Specific scenarios
Communication
Suspected MF
Shave
Untreated for 2-3 weeks
Multiple sites
Multiple times
7/29/2017
4
“Invisible Dermatoses”
Pigment disorders, collagen and elastin disorders, etc…
Include labeled sample of normal skin for comparison
Panniculitis
Incisional
“Punch in a punch”
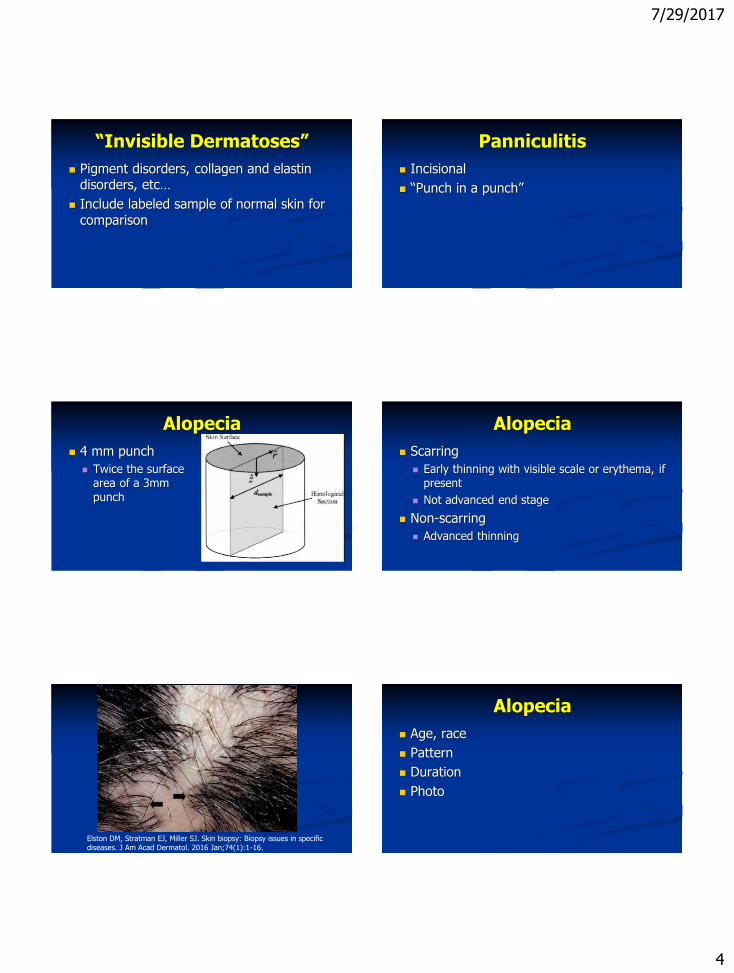
Alopecia
4 mm punch
Twice the surface area of a 3mm punch
Alopecia
Scarring
Early thinning with visible scale or erythema, if present
Not advanced end stage
Non-scarring
Advanced thinning
Elston DM, Stratman EJ, Miller SJ. Skin biopsy: Biopsy issues in specificdiseases. J Am Acad Dermatol. 2016 Jan;74(1):1-16.
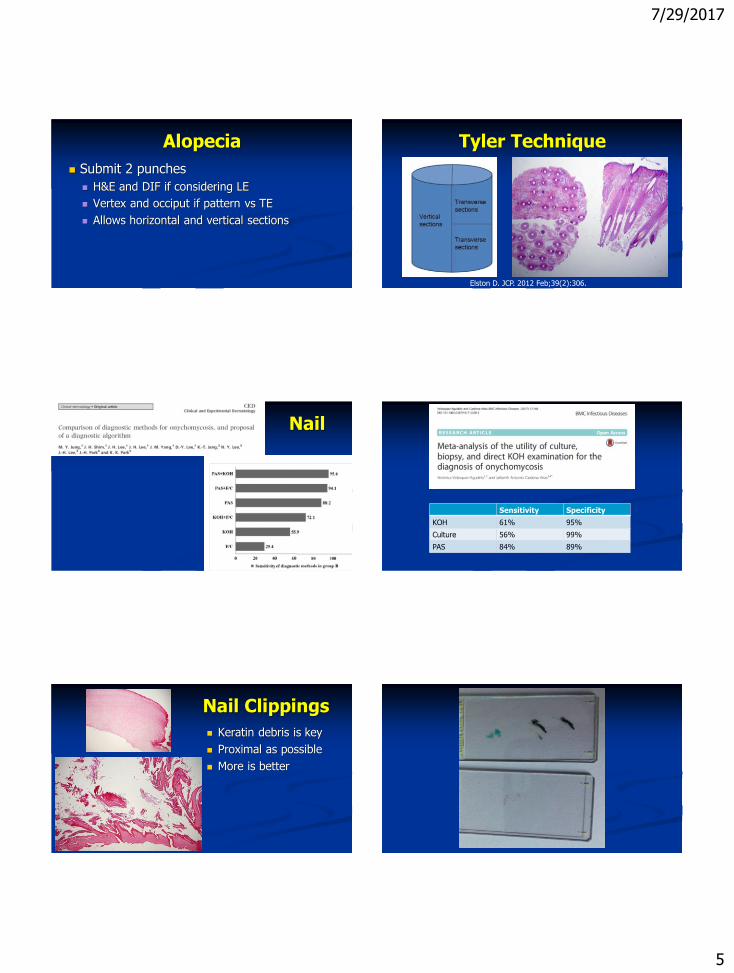
Alopecia
Age, race
Pattern
Duration
Photo
7/29/2017
5
Alopecia
Submit 2 punches
H&E and DIF if considering LE
Vertex and occiput if pattern vs TE
Allows horizontal and vertical sections
Tyler Technique
Elston D. JCP. 2012 Feb;39(2):306.
Nail
Sensitivity Specificity
KOH 61% 95%
Culture 56% 99%
PAS 84% 89%
Nail Clippings
Keratin debris is key
Proximal as possible
More is better
7/29/2017
6
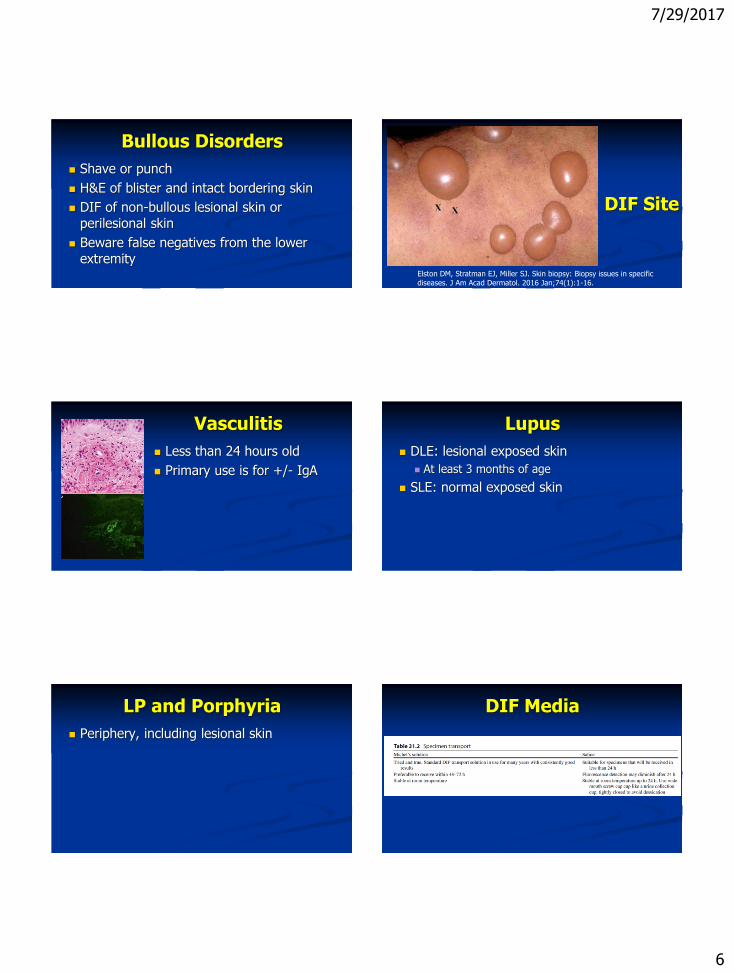
Bullous Disorders
Shave or punch
H&E of blister and intact bordering skin
DIF of non-bullous lesional skin or perilesional skin
Beware false negatives from the lower extremity
DIF Site
Elston DM, Stratman EJ, Miller SJ. Skin biopsy: Biopsy issues in specificdiseases. J Am Acad Dermatol. 2016 Jan;74(1):1-16.
Vasculitis
Less than 24 hours old
Primary use is for +/- IgA
Lupus
DLE: lesional exposed skin
At least 3 months of age
SLE: normal exposed skin
LP and Porphyria
Periphery, including lesional skin
DIF Media
7/29/2017
7
DIF from Formalin?
Not for pemphigus
Maybe for BP and DH
FP DIF
AJDP 2013;35:587-94.
Scabies
Orf
Herpes simplex
Varicella
Grover disease
Drug eruption
Maximizing Your Inflammatory Biopsy
Where to biopsy
Type of biopsy
Specific scenarios
Communication
Specimen Requisition5 D’s
Demographics Age, sex, race
Description Appearance, extent, distribution,
prior treatment
Duration/Change
Diseases/Drugs
Differential diagnosis
Barriers to Photos
Time
Consent, taking image, downloading, labeling, sending, saving
Computer storage
HIPAA compliance
Photos
100 cases
Correct diagnosis increased in 70
No change in diagnosis in 25
JAAD 2010;63:647-52.
7/29/2017
8
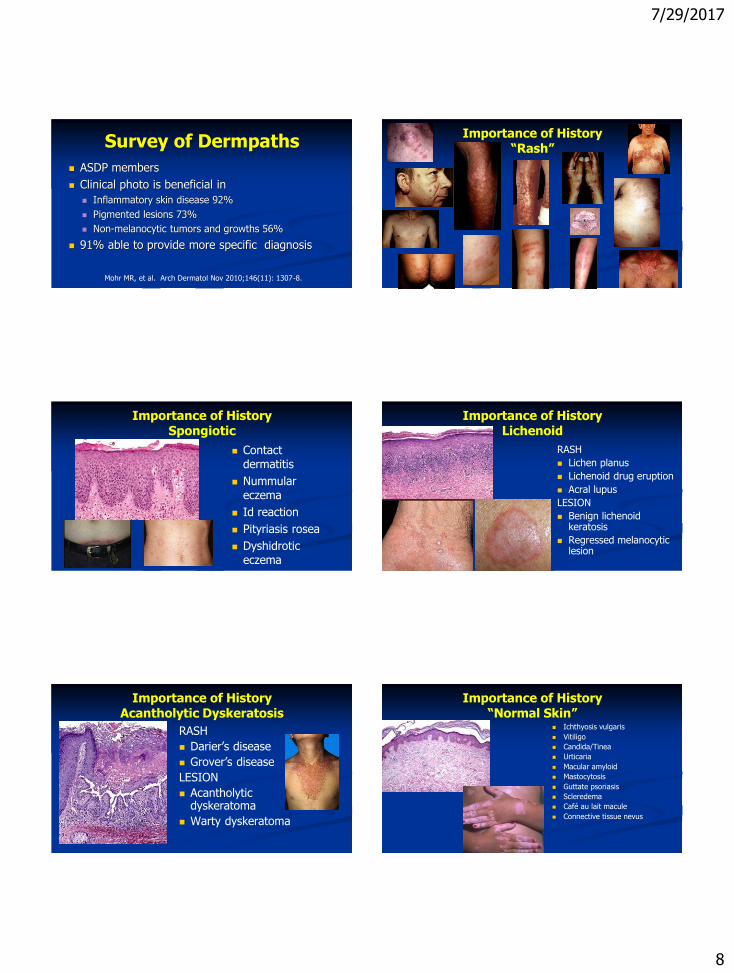
Survey of Dermpaths
ASDP members
Clinical photo is beneficial in
Inflammatory skin disease 92%
Pigmented lesions 73%
Non-melanocytic tumors and growths 56%
91% able to provide more specific diagnosis
Mohr MR, et al. Arch Dermatol Nov 2010;146(11): 1307-8.
Importance of History“Rash”
Importance of HistorySpongiotic
Contact dermatitis
Nummular eczema
Id reaction
Pityriasis rosea
Dyshidrotic eczema
Bite/scabies
Importance of HistoryLichenoid
RASH
Lichen planus
Lichenoid drug eruption
Acral lupus
LESION
Benign lichenoid keratosis
Regressed melanocytic lesion
Importance of HistoryAcantholytic Dyskeratosis
RASH
Darier’s disease
Grover’s disease
LESION
Acantholytic dyskeratoma
Warty dyskeratoma
Importance of History“Normal Skin”
Ichthyosis vulgaris
Vitiligo
Candida/Tinea
Urticaria
Macular amyloid
Mastocytosis
Guttate psoriasis
Scleredema
Café au lait macule
Connective tissue nevus
7/29/2017
9
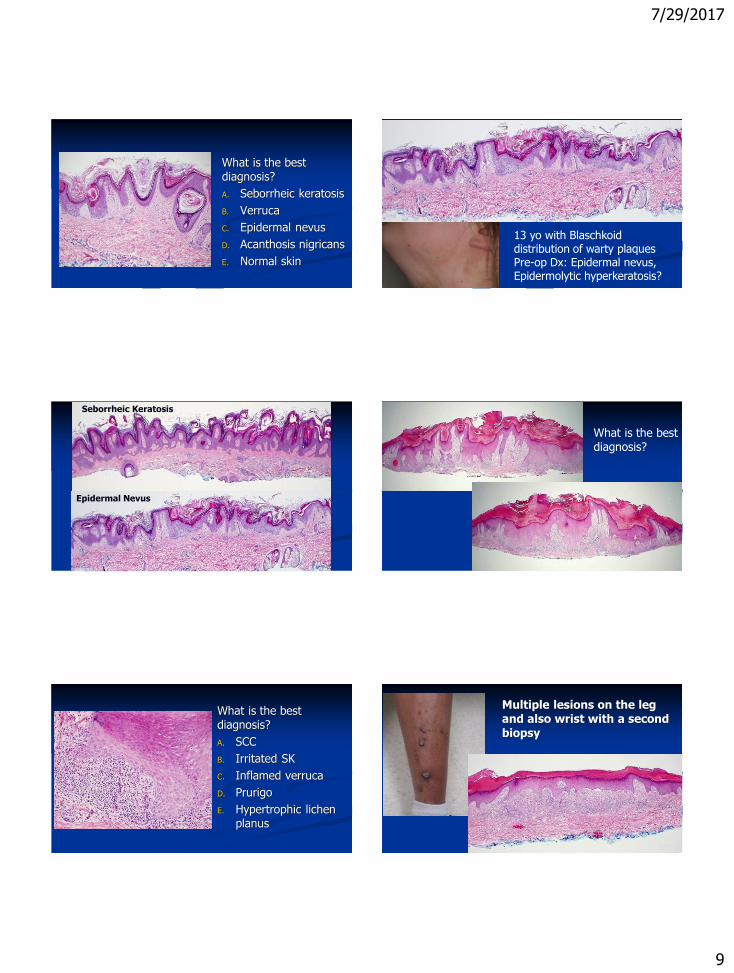
What is the best diagnosis?
A. Seborrheic keratosis
B. Verruca
C. Epidermal nevus
D. Acanthosis nigricans
E. Normal skin
13 yo with Blaschkoid distribution of warty plaquesPre-op Dx: Epidermal nevus, Epidermolytic hyperkeratosis?
Seborrheic Keratosis
Epidermal Nevus
What is the best diagnosis?
What is the best diagnosis?
A. SCC
B. Irritated SK
C. Inflamed verruca
D. Prurigo
E. Hypertrophic lichen planus
Multiple lesions on the leg and also wrist with a second
biopsy
7/29/2017
10
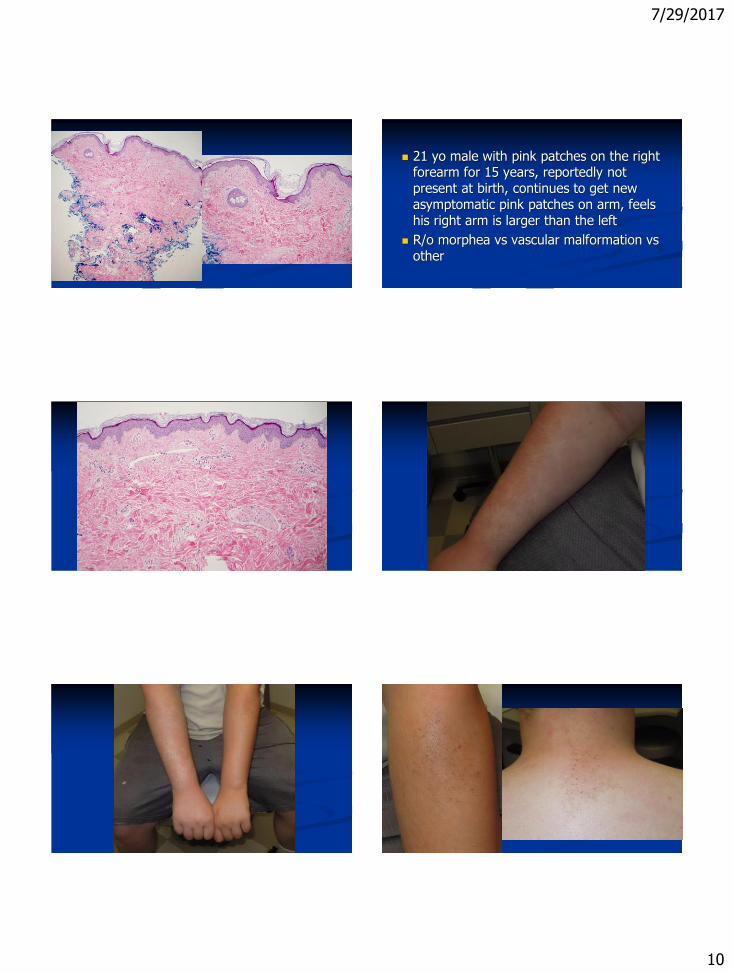
21 yo male with pink patches on the right forearm for 15 years, reportedly not present at birth, continues to get new asymptomatic pink patches on arm, feels his right arm is larger than the left
R/o morphea vs vascular malformation vs other
7/29/2017
11
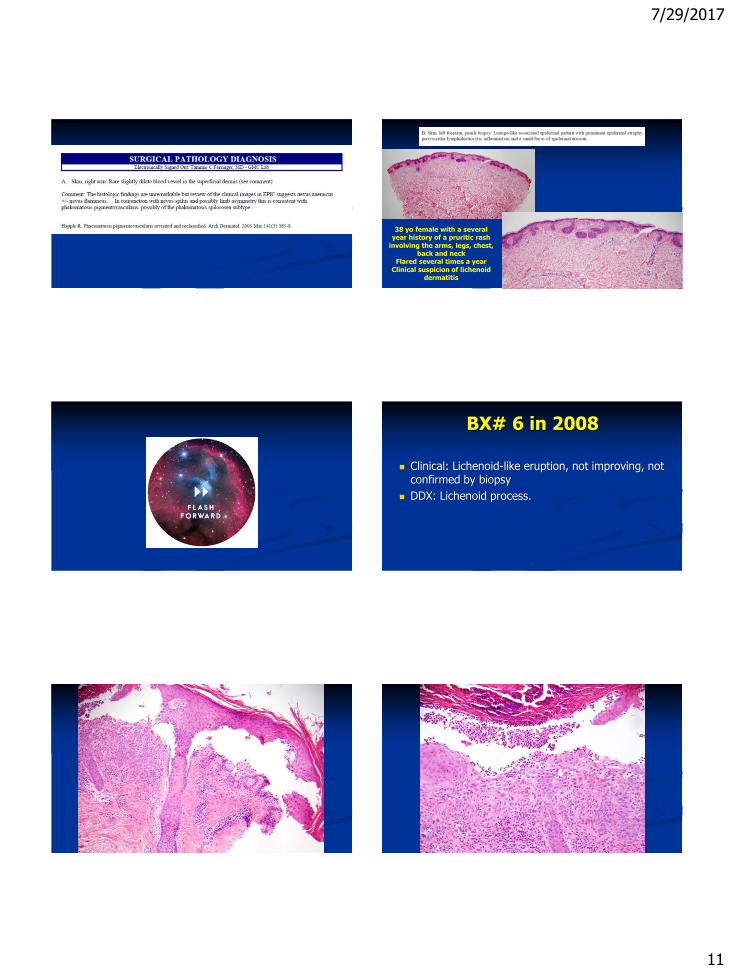
38 yo female with a several year history of a pruritic rash
involving the arms, legs, chest, back and neck
Flared several times a yearClinical suspicion of lichenoid
dermatitis
BX# 6 in 2008
Clinical: Lichenoid-like eruption, not improving, not confirmed by biopsy
DDX: Lichenoid process.
64|
|
Patient #1
66|

7/29/2017
12
BX# 6 Skin, left arm: Impetiginized crust with areas of
superficial epidermal acantholysis and sparse
dyskeratosis. (See comment)
Comment: The histologic differential diagnosis
includes bullous impetigo or impetiginized Grover’s disease. The presence of sparse dyskeratotic cells militates against an acantholytic process such as pemphigus. There is no evidence of a lichenoid infiltrate.
67|
BX# 9 in 2013 BX# 9 in 2013Final Pathologic Diagnosis:
Skin, right posterior neck, shave biopsy: lentigo-like epidermal pattern and
some
additional broader buds of epithelium.
Derm Grand Rounds 2015
Skin, left arm: Impetiginized crust with areas of superficial epidermal acantholysis and sparse dyskeratosis.
No family history and normal nails but… Darier’s????
7/29/2017
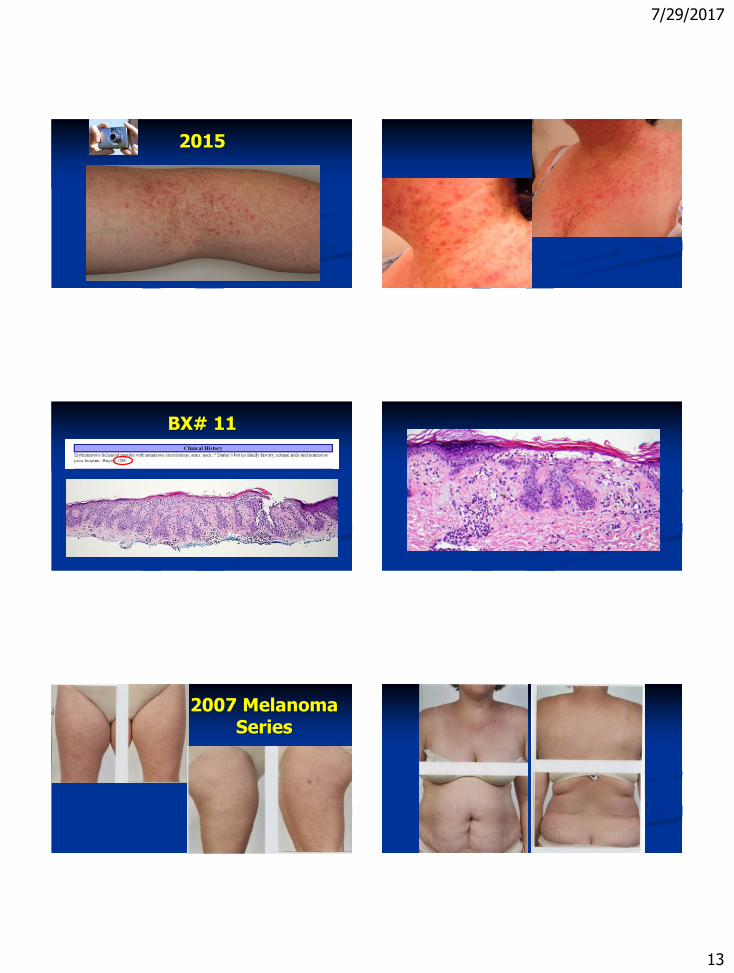
13
2015
BX# 11
2007 Melanoma Series
7/29/2017
14
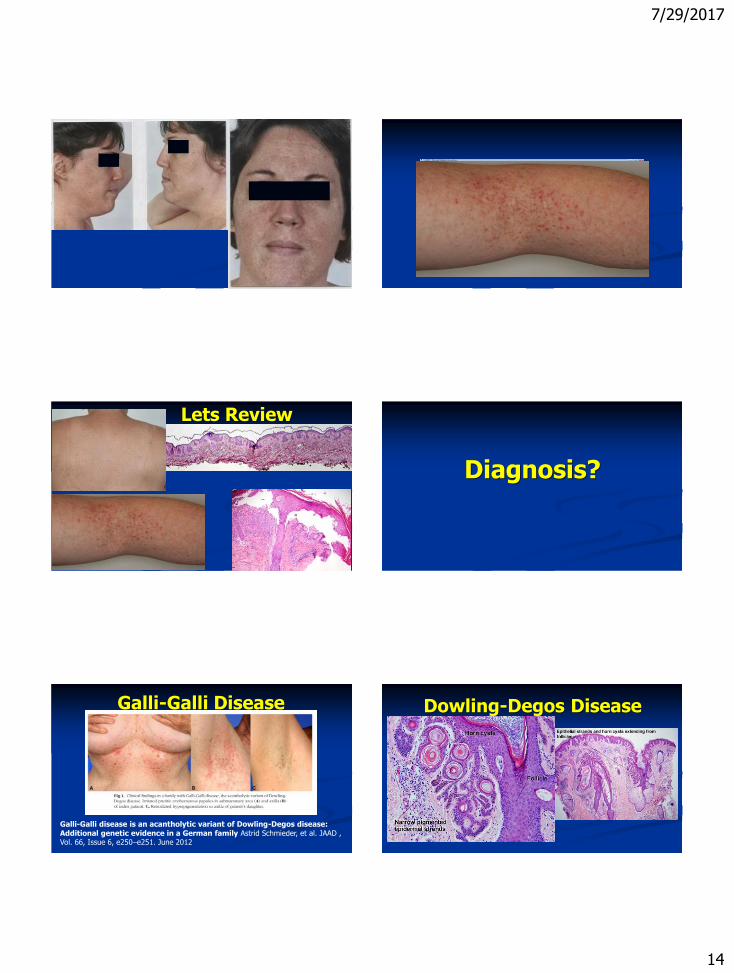
Lets Review
Diagnosis?
Galli-Galli disease is an acantholytic variant of Dowling-Degos disease: Additional genetic evidence in a German family Astrid Schmieder, et al. JAAD , Vol. 66, Issue 6, e250–e251. June 2012
Galli-Galli Disease Dowling-Degos Disease
7/29/2017
15
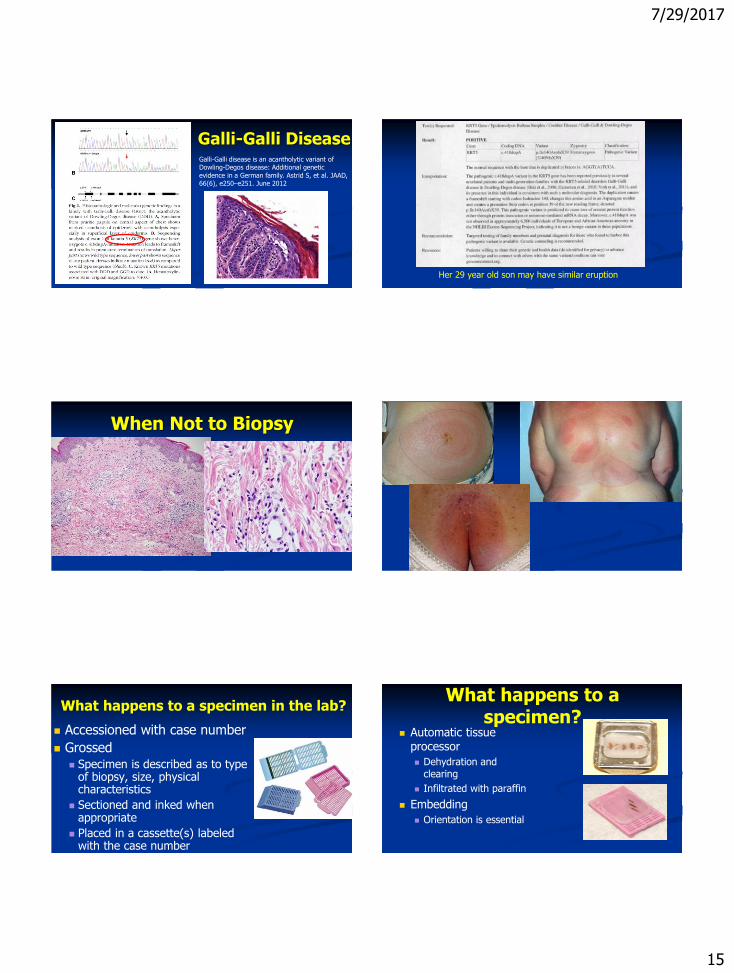
Galli-Galli disease is an acantholytic variant of Dowling-Degos disease: Additional genetic evidence in a German family. Astrid S, et al. JAAD, 66(6), e250–e251. June 2012
Galli-Galli Disease
Her 29 year old son may have similar eruption
When Not to Biopsy
What happens to a specimen in the lab?
Accessioned with case number
Grossed Specimen is described as to type
of biopsy, size, physical characteristics
Sectioned and inked when appropriate
Placed in a cassette(s) labeled with the case number
What happens to a specimen?
Automatic tissue processor
Dehydration and clearing
Infiltrated with paraffin
Embedding
Orientation is essential
7/29/2017
16
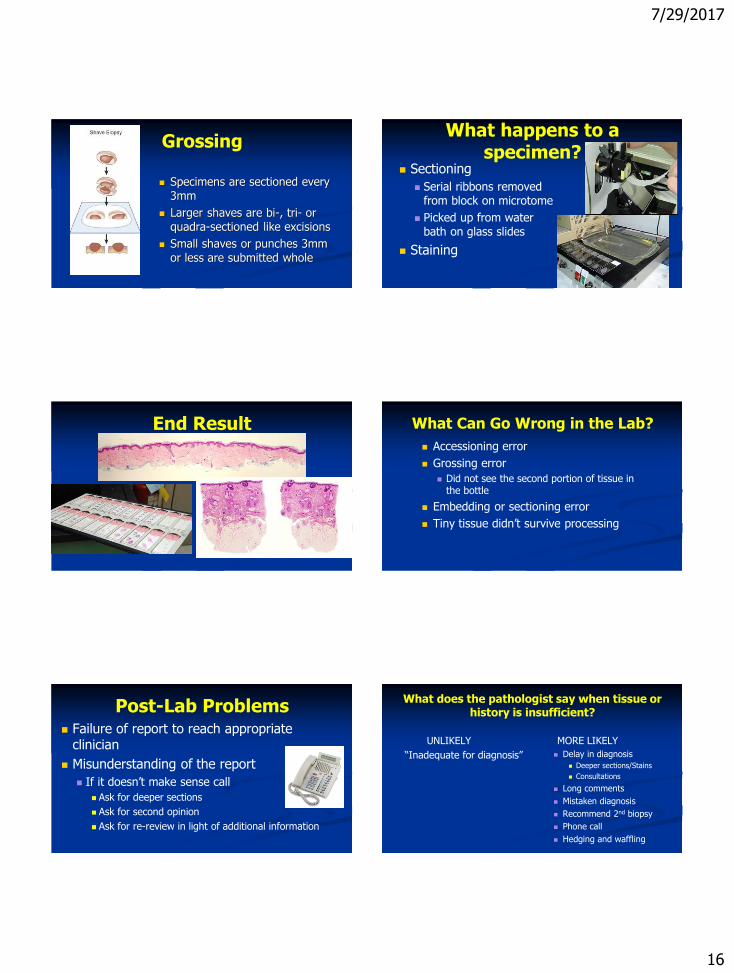
Grossing
Specimens are sectioned every 3mm
Larger shaves are bi-, tri- or quadra-sectioned like excisions
Small shaves or punches 3mm or less are submitted whole
What happens to a specimen?
Sectioning
Serial ribbons removed from block on microtome
Picked up from water bath on glass slides
Staining
End Result What Can Go Wrong in the Lab?
Accessioning error
Grossing error
Did not see the second portion of tissue in the bottle
Embedding or sectioning error
Tiny tissue didn’t survive processing
Post-Lab Problems Failure of report to reach appropriate
clinician
Misunderstanding of the report
If it doesn’t make sense call
Ask for deeper sections
Ask for second opinion
Ask for re-review in light of additional information
What does the pathologist say when tissue or history is insufficient?
UNLIKELY
“Inadequate for diagnosis”
MORE LIKELY
Delay in diagnosis
Deeper sections/Stains
Consultations
Long comments
Mistaken diagnosis
Recommend 2nd biopsy
Phone call
Hedging and waffling
7/29/2017
17
Hedges and Waffles
Consistent with or compatible with….
Clinical correlation required
Know your pathologist
Multiple personalities
Cowboy: Black or white
Agnostic: No unusual case is diagnosable with absolute certainty and the biologic behavior cannot be determined
Meek: Consistent with or compatible with
Upgrader: Unusual or atypical, may be malignant
BEST: COMBINATION OF ALL
Know your pathologist
Know his/her style
Read the microscopic and the comments
Open lines of communication
If it doesn’t make sense call
Ask for deeper sections
Be accessible to discuss unusual cases
Thank You
















![Position-based modeling of lesion displacement in ... · Image-guided breast biopsy is the standard procedure to evaluate symptomatic and screening-detected suspicious lesions [1]](https://img.pdfslide.net/doc/110x75/6064b89f3a466f05ad65ec83/position-based-modeling-of-lesion-displacement-in-image-guided-breast-biopsy.jpg)