Embed Size (px)
Citation preview

Review
Pathology and clinico-pathologic correlations in spondyloarthropathies
Bernard Fournié
Clinical Rheumatology Department, Purpan Teaching Hospital, Place du Docteur Baylac, 31059 Toulouse cedex 9, France
Received 18 September 2003; accepted 4 February 2004
Available online 22 March 2004
Abstract
The term “spondyloarthritis” encompasses a variety of conditions that manifest as inflammation of the synovial membranes and entheses.The synovial inflammation lacks specificity and shares many features with rheumatoid synovitis. The hallmark of spondyloarthritis isinflammation of the entheses, which manifests as a combination of hyperostosis, osteitis, and periostitis. The entheses include not only the siteswhere tendons, ligaments, and joint capsules attach to bone, but also other fibrous structures such as the amphiarthroses (pubic symphysis,manubriosternal symphysis, and discovertebral junctions) and the diarthro-amphiarthroses (sacroiliac area, chest wall joints, and tips of thefingers and toes). This vast entheseal territory is the target selectively involved in patients with spondyloarthropathy.© 2004 Published by Elsevier SAS.
Keywords: Spondyloarthritis; Enthesis; Enthesitis; Enthesopathy; Synovitis
The spondyloarthropathies are musculoskeletal diseasesthat share a number of characteristics, including inflamma-tion of the entheses, but also exhibit distinctive features.They should be viewed as a federation of related musculosk-eletal diseases, rather than as the shapeless mass of ill-defined conditions suggested by the classic term spondyloar-thropathy nebula.
The federation of spondyloarthropathies includes anky-losing spondylitis, psoriatic arthritis, SAPHO syndrome, en-teropathic arthropathies, and two less common conditions,sternocostoclavicular hyperostosis and chronic recurrentmultifocal osteomyelitis. However, this list is not universallyaccepted: thus, Kahn and Chamot [1] and others believe thatSAPHO syndrome (which includes sternocostoclavicularhyperostosis and multifocal osteomyelitis) is a separate en-tity that is related to, but not a member of, the spondyloar-thropathies.
1. Pathology
Enthesitis and synovitis are the fundamental pathologicalabnormalities in spondyloarthropathy. Both result from anonspecific inflammatory process, whose cause has not beenelucidated.
1.1. Enthesitis
The entheses fall into two groups [2]: the fibrous entheses,which attach to the diaphyseal periosteum, and the fibrocar-tilaginous entheses, which are the sites of tendon, ligament,and joint capsule attachment to bone. We will focus on thislast group, which is the main target in spondyloarthropathies.Fibrocartilaginous entheses are found throughout the skel-eton. Three anatomic characteristics are essential to a goodunderstanding of enthesitis [3]: (a) most of the enthesis islocated within the bone, and the tendon fibers merge with thebone trabeculae via gradual ossification; (b) the bone and theend of the tendon are separated by a cartilage plate that isperforated by the tendon fibers; (c) around the enthesis, theperiosteum blends with the peritenon.
Niepel et al. [4] and Ball [5] wrote the first detaileddescriptions of the mechanism underlying enthesitis. Theydescribed two phases: subchondral osteitis and reparativeossification. The inflammatory process starts in the in-traosseous part of the enthesis, under the cartilage plate,where an infiltrate of lymphocytes and plasma cells accumu-lates. The infiltrate is predominantly perivascular, althoughcell clusters are also present in the adjoining bone marrow.The granuloma eventually destroys the bone and the cartilageplate. The defect left by this destructive process is rapidlyfilled by newly formed woven bone then by lamellar bone.E-mail address: [email protected] (B. Fournié).
Joint Bone Spine 71 (2004) 525–529
http://france.elsevier.com/direct/BONSOI/
© 2004 Published by Elsevier SAS.doi:10.1016/j.jbspin.2004.02.002

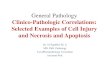
This ossification process extends to the terminal part of thetendon, producing an enthesophyte (Fig. 1).
Recent immunohistochemical studies of early enthesitislesions showed CD8+ T cell infiltrates in the bone marrowand CD68+ macrophages infiltrating the fibrocartilage [6–8].These cells may be central to the pathogenesis of enthesitis.
1.2. Synovitis
The synovitis seen in patients with spondyloarthropathiesshares many similarities with rheumatoid synovitis. Despitethe less severe inflammation and earlier fibrosis, none of thehistological features is characteristic of spondyloarthropathy[9]. Data on synovitis are more extensive for psoriatic arthri-tis than for the other spondyloarthropathies [10–12]. In pso-riatic arthritis, synovitis may lead to tissue destruction, add-ing to the similarities with rheumatoid arthritis.
Three phases have been distinguished in the natural his-tory of synovitis. Severe and diffuse edema of the synovialfimbriae is the main feature in the early phase. Hyperplasia ofthe synovial cell layer is moderate. The lamina propria showscongestion with haphazardly distributed neovessels and aperivascular infiltrate of lymphocytes and plasma cells. Fi-brosis begins to develop. In the full-blown phase, the abnor-malities are more marked, but only rarely does the granulomaorganize into a synovial pannus. The blood vessel walls arethickened, infiltrated by inflammatory cells, and arranged inan onionskin pattern. Electron microscopy studies show en-dothelial cell hypertrophy with ergoplasm dilation, intercel-lular edema without rupture of the cell junctions, and thick-ening of the vascular basement membrane. There is noendothelial cell necrosis or immune complex deposition, andno viral particles are visible [13]. Immunofluorescenceshows IgG and IgA; IgM and C3 deposits are less common,whereas they are often present in the rheumatoid synovium[14]. The inflammatory infiltrate may be diffuse or arranged
in cell clusters; a nodular pattern is exceedingly rare. Lym-phocytes and plasma cells are the predominant cell types,macrophages are not consistently present, and polymorpho-nuclear neutrophils or basophils are uncommon. Lympho-cyte phenotype studies have shown a predominance of CD4+CD8+ T cells, a few B cells, and NK lymphocytes, with nodistinctive features as compared to other inflammatory jointdiseases [15]. Progression of the fibrosis manifests as fibro-blast division and development of collagen fiber bundlesaligned along the fimbriae. The edema resolves. Finally, thelast phase is characterized by residual abnormalities: thefibrosis replaces the synovial tissue and quenches the inflam-mation. The synoviocytes may stimulate fibroblast growth byoverproducing TNF-a and platelet-derived growth factor[16].
2. Clinical pathology
The entheses strictly speaking, or common entheses, arefound in joint structures characterized by limited mobility, asubstantial fibrous component, and little or no synovium.Poirier et al. [17] classified these structures among the am-phiarthroses and diarthro-amphiarthroses. Amphiarthrosesare interosseous ligaments and, therefore, are large entheses.They include the pubic symphysis, manubriosternal symphy-sis, and intervertebral disks (called “intervertebral liga-ments” by early pathologists). The diarthro-amphiarthrosescomprise the sacroiliac area, the chest wall joints, and the tipsof the fingers and toes. Although diarthro-amphiarthrosescontain some synovium, the amount of ligament or fibrocar-tilage is far greater, so that entheses predominate in thesejoints. In diarthroses, in contrast, the joint capsule is the onlyentheseal component.
2.1. The intervertebral disk and fibrous perispinal tissue
The intervertebral disk is composed of two distinct struc-tures, the annulus fibrosus and the disk center.
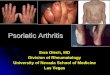
The annulus fibrosus is a ligament attached to the rim ofthe vertebral endplates, vertebral processes, or vertebral mar-gins. Rainer and Cotaescu [18] stated that the annulus waspart of the fibrous structure that surrounds the vertebralbodies and joins the vertebras to one another. This “perispi-nal structure” also includes the anterior vertebral ligament, inwhich Rainier differentiated two fiber types: short fibers thatbridge the intervertebral space and attach to the lateral andanterior aspects of the vertebral bodies, where they mergewith the periosteum; and superficial long fibers that consti-tute most of the anterior vertebral ligament (Fig. 2). Thisperispinal structure individualized by Rainier contains anabundance of entheses, both fibrocartilaginous (annulus) andfibrous (short fibers).
Spinal syndesmophytes reflect enthesitis of the annulusfibrosus and perispinal short fibers. The location and extentof the inflammatory process predicate the location and shape
Fig. 1. Enthesitis. (1) Marginal subchondral osteitis. (2) Secondary repara-tive ossification, which may produce an enthesophyte, a spur, a syndesmo-phyte, bony ankylosis, or hyperostosis. (3) “Reactive” periostitis at theperiphery of the enthesis. (4) Aseptic osteomyelitis may occur via directbone marrow contamination from the initial focus of osteitis.
526 B. Fournié / Joint Bone Spine 71 (2004) 525–529

of the syndesmophytes. A slender straight syndesmophytethat seems drawn with a ruler from one vertebral margin tothe next is located within the annulus. In contrast, syndesmo-phytes developed in the short fibers are coarser, with broadimplantation bases on the vertebral bodies and, in somecases, flowing-wax hyperostosis.
In enthesitis of the annulus fibrosus, anterior spondylitis[19] reflects the initial phase of osteitis and can manifest assquaring of the vertebral body, a marginal erosion, or mar-ginal sclerosis. Paravertebral ossifications [20] and “free”syndesmophytes, whose exact meaning is unclear, may belocated under the ligaments of the perispinal structure.
The disk center contains all the components that charac-terize entheses [21]: a distinctive system of fibers is arrangedconcentrically around the nucleus pulposus, cells are embed-ded within this system, and the fibers are inserted tangen-tially into the endplate cartilage, which is the equivalent ofthe cartilage plate at sites of tendon-to-bone attachment.Enthesitis of the disk center manifests as aseptic discitis withdisk space narrowing, irregular endplate sclerosis, and insome cases a geode within the vertebral body. Enthesitis ofthe disk center is independent from enthesitis of the annulusfibrosus [22], although the two can occur in combination.Disk center enthesitis should be distinguished from delayedbony metaplasia of the disk, which can occur in patients withspinal ankylosis, perhaps in part as a result of loss of mobil-ity.
2.2. The sacroiliac area and tips of the fingers and toes
The sacroiliac area comprises the anatomic structuresthat unite the sacrum to the pelvic bone, which can be divided
into two zones. The sacroiliac joint, which is small, containsonly a scant amount of synovium, and may be vestigial. It issurrounded by the anterior and posterior sacroiliac liga-ments. The supraarticular zone is a strong interosseousligament that is by far the largest enthesis in the body.
Three facts establish that the sacroiliitis seen in spondy-loarthropathies is, in fact, enthesitis of the sacroiliac area.First, although the lesions predominate in the joint, theyextend to the supraarticular ligament, involving the entiresacroiliac area. Second, the three stages of sacroiliitis de-scribed by Forestier [23] reflect the development of enthesitisof the joint space, with lysis followed by sclerosis (the ostei-tis phase) and finally bony ankylosis (the reparative ossifica-tion stage). Third, histological studies of biopsies from sac-roiliac joints of patients with early spondyloarthropathyshowed lesions identical to those seen in biopsies of tendon-to-ischium attachment sites, with inflammatory subchondralosteitis followed by fibrous proliferation and ultimately byossification responsible for ankylosis of the sacroiliac jointsand for ischial enthesophyte development [24].
The sacroiliac region shares striking similarities with thetips of the fingers and toes. The distal interphalangeal jointcontains a scant amount of synovium contrasting with anabundance of ligament fiber endings from the extensor andflexor tendons. In addition, the distal phalanx is joined to thenail and digit pad by a unique entheseal system composed ofconnective tissue septa that are inserted deep into the pha-langeal bone. This distinctive anatomic arrangement mayexplain why many patients with spondyloarthropathies havelesions in the fingers or toes, such as arthritis of the distalinterphalangeal joint, pulpitis, or osteoperiosteal remodelingof the distal phalanx, this last abnormality being seen chieflyin psoriatic arthritis [25].
2.3. The chest wall joints and symphyses
The chest wall joints unite the ribs to the vertebras andsternum and the sternum to the shoulder girdle via theclavicles. These joints have little or no mobility. They arecomposed primarily of fibrous or fibrocartilaginous tissuestrengthened by a network of ligaments near or around thejoint. The synovial component is small or absent.
The costovertebral, acromioclavicular, and sternocosto-clavicular joints contain a synovial component, which issomewhat more abundant in the sternocostoclavicular jointsthan in the costovertebral and acromioclavicular joints. Thefibrous component is far larger, being present about the joint(sternoclavicular ligaments), near the joint (costoclavicularand interclavicular ligaments), and within the joint (menis-coid fibrocartilage). The chondrocostal and chondrosternaljoints are synarthroses composed of fibrocartilaginous tissue,with no joint cavity or synovial membrane. The manubri-osternal symphysis is made of fibrocartilage comparable tothe intervertebral disks, with a softer central part, sometimeshollowed out into a cleft resembling an ill-defined jointcavity.
Fig. 2. The intervertebral disk and fibrous perispinal structure. (1) Anteriorvertebral ligament. (2) Short fibers of the anterior vertebral ligament, atta-ched to the vertebral bodies. (3) Subligamentous space. (4) Annulus fibrosusattached to the vertebral body processes. (5) Central disk, whose fibers areinserted tangentially into the endplate cartilage.
527B. Fournié / Joint Bone Spine 71 (2004) 525–529

Enthesitis of the chest wall [26,27] predominantly affectsthe costovertebral joints, whose ligaments undergo ossifica-tion, the sternocostoclavicular joints, where osteitis domi-nates, and the manubriosternal symphysis, whose inflamma-tion can lead to ankylosis. Ankylosis may occur also at thepubic symphysis, which is an interosseous ligament.
2.4. Diarthroses
In contrast to the structures described above, diarthrosescontain a large amount of synovium. The joint capsule isusually the sole fibrous component. Inflammation of thediarthroses in patients with spondyloarthropathy is related toa dual process [28]: synovitis, which progresses to fibrousankylosis, and capsulitis, which tends to produce bony anky-losis of the joint.
Synovitis is particularly conspicuous in the large limbjoints, where involvement of the capsule often goes unno-ticed. At the hip, however, periarticular enthesophytes(pseudo-osteoarthritis) or even joint capsule ossification(sheathing hip disease) may occur. In contrast, capsular en-thesitis is visible clearly at the small joints such as the facetjoints, where it causes bony ankylosis, and at the interpha-langeal joints, where osteolysis followed by ankylosis ishighly suggestive of psoriatic arthritis [29].
3. Putting the facts together
The entheses are at the core of spondyloarthropathies, andenthesitis is widely believed to be the primary abnormalitythat gives rise to all the other lesions [21,27,30–34].
3.1. The entheses throughout the body
In addition to the classic entheses, amphiarthroses anddiartho-amphiarthroses can be classified as entheses becausethey are composed mainly of fibrous tissue, with little or nosynovium [21]. In addition, the mechanism underlying in-flammation of the amphiarthroses and diarthro-amphiarthroses is identical to that seen in enthesitis. Togetherwith the classic entheses, these joints constitute a vast terri-tory, which is the main target of the disease process inspondyloarthropathies. Inflammation of the entheseal terri-tory is the common denominator of spondyloarthropathiesand the sign that best distinguishes these conditions from theother inflammatory joint diseases, which manifest mainly assynovitis.
3.2. Hyperostosis-osteitis-periostitis syndrome
The radiological triad of hyperostosis-osteitis-periostitisreflects the main phases of enthesitis [21,34]. The initialosteitis manifests as pain, increased radionuclide uptake, andintraosseous changes visible by magnetic resonance imagingor ultrasonography followed by radiographic changes con-
sisting of focal osteolysis surrounded by a variable degree ofirregular bony sclerosis. Hyperostosis reflects the next stageof reparative ossification, which produces the classic imagesof enthesophytosis, spines, syndesmophytes, or ankylosis,according to the site of involvement. A periosteal reactionmay be visible around the enthesis.
3.3. Derived lesions
Enthesitis may induce inflammation of the adjacent struc-tures. Aseptic osteomyelitis, which occurs in several spondy-loarthropathies including psoriatic arthritis and SAPHO syn-drome, may be related to direct bone marrow contaminationfrom the initial focus of osteitis [21]. The synovitis may beinitiated by the inflammation of the adjacent joint capsule.These are unproven hypotheses, and most of the authors whoascribe the bone lesions to Propionibacterium acnes osteo-myelitis provide no explanation to the synovitis [35].
References
[1] Kahn MF, Chamot AM. SAPHO syndrome. Rheum Dis Clin NorthAm 1992;18:225–46.
[2] Benjamin M, Kumai T, Milz S, Boszczyk BM, Boszczyk AA, Ral-phs JR. The skeletal attachment of tendons—tendon “entheses”.Comparative biochemistry and physiology. Mol Integrative PhysiolPart A 2002;133:931–45.
[3] Dolgo-Saburoff B. Ursprung und insertion der skelettmusculatur.Anat Anz 1929;68:80.
[4] Niepel GA, Kostka D, Kopecky S, Manca S. Enthesopathy. ActaRheum Balneol Pistiniana 1966;1:9–64.
[5] Ball J. Enthesopathy of rheumatoid and ankylosing spondylitis. AnnRheum Dis 1971;30:213–23.
[6] Bollow M, Fischer T, Reisshauer H, Backhaus M, Sieper J,Hamm B, et al. Quantitative analyses of sacroiliac biopsies inspondyloarthropathies: T cells and macrophages predominate in earlyand active sacroiliitis. Cellularity correlates with the degree ofenhancement detected by magnetic resonance imaging. Ann RheumDis 2000;59:135–40.
[7] Laloux L, Voisin MC, Allain J, Martin N, Kerboull L, Cheva-lier X, et al. Immunohistological study of entheses inspondyloarthropathy: comparison in rheumatoid arthritis and osteoar-thritis. Ann Rheum Dis 2001;60:316–21.
[8] Mc Gonagle D, Marzo-Ortega H, O’Connor P, Gibbon W, Hawkey P,Henshaw K. Histological assessment of the early enthesitis lesion inspondyloarthropathy. Ann Rheum Dis 2002;61:534–7.
[9] Cooper NS, Soren A, Mc Ewan C, Rosenberger JL. Diagnosis speci-ficity of synovial lesions. Human Pathol 1981;12:314–28.
[10] Sherman MS. Psoriatic arthritis. Observation on the clinical, roent-genographic and pathological changes. J Bone Joint Surg 1952;34A:821–52.
[11] Laurent MR. Psoriatic arthritis. Clin Rheumatic Dis 1985;11:61–85.[12] Grossin M, Hayem G. Anatomopathologie synoviale et liquide articu-
laire dans le rhumatisme psoriasique. Rev Rhum 2002;69:624–9.[13] Espinoza LR, Vasey FB, Espinoza CG, Bocanegra TS, Germain BF.
Vascular changes in psoriatic synovium. A light and electron micro-scopic study. Arthritis Rheum 1982;25:677–84.
[14] Fyrand O, Mellbye OJ, Natvig JB. Immunofluorescence studies forimmunoglobulins and complement C3 in synovial joint membranes inpsoriatic arthritis. Clin Exp Immunol 1977;29:422–7.
[15] Taccari F, Fattorossi A, Moretti S, Riccieri V, Fasani M, Zopini A.Phenotypic profile of major synovial cell populations in longstandingpsoriatic arthritis. J Rheumatol 1987;14:525–30.
528 B. Fournié / Joint Bone Spine 71 (2004) 525–529

[16] Zachariae H, Aslam HM, Bjerring P, Sogaard H, Zachariaf E, Hieck-endorff F, et al. Serum aminoterminal propeptide of type III procol-lagen in psoriasis and psoriatic arthritis: relation to liver fibrosis andarthritis. J Am Acad Rheumatol 1991;25:50–3.
[17] Poirier P, Charpy A, Nicolas A. Traité d’anatomie humaine, Tome 1.Paris: Arthrologie; 1911 Masson, Cie, editors.
[18] Rainer FJ, Cotaescu I. Contribution à l’étude de l’appareil fibreux dela colonne vertébrale. In: Milcu SM, editor. L’œuvre scientifique deRainer FJ, 2. Bucarest: Imprimerie Nationale; 1945. p. 33–46.
[19] Romanus R,Yden S. Destructive and ossifying spondylitic changes inrheumatoid ankylosing spondylitis (pelvo-spondylitis ossificans).Acta Orthop Scand 1952;22:88–99.
[20] Bywaters EGL, Dixon ASJ. Paravertebral ossification in psoriaticarthritis. Ann Rheum Dis 1965;24:313–31.
[21] Fournié B. Enthesopathy and hyperostosis–osteitis–periostitis syn-drome. A nosological radioclinical approach to inflammatory spondy-larthropathies. Rev Rhum [Ed Fr] 1993;60:485–8.
[22] François RJ. Le rachis dans la spondylarthrite ankylosante. Bruxelles:Arscia SA; 1976. p. 79–91.
[23] Forestier J. The importance of sacro-iliaque changes in the earlydiagnosis of ankylosing spondylarthritis. Radiology 1939;33:389–402.
[24] Schichikawa K, Tsujimoto M, Nishioka J, Nishibayashi Y, Matsu-moto K. Histopathology of early sacroiliitis and enthesitis in ankylos-ing spondylitis. In: Ziff M, Cohen SB, editors. Advances in inflamma-tion research The spondyloarthropathies, 9. New York: Raven Press;1985. p. 14–24.
[25] Fournié B, Viraben R, Durroux R, Lassoued S, Gay R, Fournié A.Psoriatic onycho-pachydermo-periostitis of the big toe. Anatomo-clinical study and physiopathogenic approach apropos of 4 cases. RevRhum Mal Osteoartic 1989;56:579–82.
[26] Fournié B, Boutes A, Dromer C, Sixou L, Le Guennec P,Granel J, et al. Prospective study of anterior chest wall involvement inankylosing spondylitis and psoriasic arthritis. Rev Rhum Engl Ed1997;64:22–5.
[27] Gaucher A, Pere P, Regent D, Grandhaye Ph, Aussedat R, Vivard Ph.Spondylarthropathies or ossifying polyenthesitis. Scintigraphic andscanographic evidence. Rev Rhum Mal Osteoartic 1987;54:243–8.
[28] Fassbender HG. Morphological aspects of rheumatoid arthritis andpsoriatic arthritis. In: Wagenhuser FG, editor. Chronic forms of pol-yarthritis. City: Publisher; 1976. p. 917–26.
[29] Fournié B, Granel J, Bonnet M, Dromer C, Pages M, Billey T, et al.Incidence of signs indicating psoriatic rheumatism in radiologicalinvolvement of fingers and toes. Apropos of 193 cases of psoriaticarthropathy. Rev Rhum Mal Osteoartic 1992;59:177–80.
[30] Paolaggi JB, Strutz P, Goutet MC, Le Parc JM, Siaud JR, Auquier L.Systematic research on enthesopathies in chronic rheumatism.Results and pathological significance. Relation to erosive spondylitisand other tendinous or synovial lesions. Rev Rhum Mal Osteoartic1984;51:451–6.
[31] Paolaggi JB, Goutet MC, Strutz P, Siaud JF, Le Parc JM, Auquier L.Enthesopathy in inflammatory spondylarthropathy. Incidence, clini-cal, radiological and anatomical descriptions. Current status of thequestion. Apropos of 37 cases. Rev Rhum Mal Osteoartic 1984;51:457–62.
[32] Gaucher A, Péré P. Les enthésiopathies ossifiantes. De la maladie deForestier à la spondylarthrite ankylosante. Rev Rhum Mal Osteoartic1987;54:537–8.
[33] Gillet P, Banwarth B, Netter P, Morel O, Péré P, Gaucher A. Experi-mental auto-immune spondylodiscitis associated with type II collageninduced arthritis. J Rheumatol 1987;14:856–8.
[34] Fournié A, Bouvier M, Fournié B, Colson F, Ayrolles C, Labre JP.Hyperostosis–osteitis–periostitis: a radiological triad of enthesopa-thies. Remarks apropos of 2 unusual femoral localizations. Rev RhumMal Osteoartic 1989;56:763–6.
[35] Edlund E, Johnsson U, Lidgren L, Petterson H, Sturfelt G, Svens-son B, et al. Palmoplantar pustulosis and sternocostocalvicular arthro-osteitis. Ann Rheum Dis 1988;47:809–15.
529B. Fournié / Joint Bone Spine 71 (2004) 525–529