Embed Size (px)
Citation preview

APPLIED MICROBIOLOGY, Sept. 1972, p. 389-397Copyright 0 1972 American Society for Microbiology
Vol. 24, No. 3Printed in U.S.A.
Pathology of Exfoliated OropharyngealEpithelial Cells Infected with Wild-Type
AdenovirusDAVID P. McCORMICK, QUIRINO GALAPON, AND CARL BERLING
Virology Division, Naval Medical Field Research Laboratory, Camp Lejeune, North Carolina 28542
Received for publication 2 June 1972
Adenovirus disease was diagnosed in 2 hr by staining exfoliated infected oro-pharyngeal cells with fluorescein-tagged rabbit antisera to adenovirus types 4and 7. The method was as sensitive as the standard virus isolation procedures,but serological cross reactions were observed. Viral antigens were detected inboth the nucleus and cytoplasm of infected cells. Infection was accompanied bythe outpouring of large numbers of polymorphonuclear leukocytes and smallernumbers of mononuclear cells. The method provides a model for the study ofthe cellular response to viral upper respiratory disease.
With the advent of adenovirus vaccines andthe possibility of the use of chemotherapeuticagents for virus infections (5, 9, 10, 15), therapid diagnosis of infections causing acute re-spiratory disease becomes ever more impor-tant. Fluorescent antibody methods have beenused to detect in the tissues of patients a va-riety of viral agents including influenza virus(17), Herpesvirus hominis (1), and long-incu-bation hepatitis virus (8), not to mention thewidespread application of fluorescent-antibodytechniques for the rapid diagnosis of bacterialinfections in a clinical setting. Furthermore,fluorescent-antibody techniques have beenused to study the synthesis of adenovirus anti-gens in tissue culture preparations (2, 14).
Recurring epidemics of adenovirus disease ina Marine Corps population have enabled thislaboratory to prepare and test fluorescent-an-tibody reagents for the rapid detection of ade-novirus antigens infecting oropharyngeal cells.The fluorescent-antibody method described inthis report shortens the diagnosis time from aminimum of 7 days to 2 hr. The method is notexpected to replace the usual isolation tech-niques. However, it may find a use when thereis particular need for a rapid diagnosis in spe-cial situations: when chemotherapeutic agentsare used, when a rapid shift in virus type hasoccurred, or as a spot check in a populationwhere the standard virus isolation methods arenot available such as in small communities orat military bases having no virus laboratory.
MATERIALS AND METHODS
The methods for preparation and conjugation ofantisera have been described in detail (12).
Tissues. Continuous human epithelial (HEp-2)cells, HeLa-M cells, primary human embryonickidney (HEK), and human embryonic fibroblastcells (WI-38) were maintained in Eagle minimumessential medium supplemented with 2 to 5% heat-inactivated fetal calf serum.Virus prototypes. Adenovirus type 3 (strain
G.G.), adenovirus type 4 (strain RI-67), and adeno-virus type 7a (strain S-1058) were free from myco-
plasma contamination and were provided by SylviaCunningham, Medical Resources Branch, NationalInstitute of Allergy and Infectious Diseases, Na-tional Institutes of Health, Bethesda, Md.
Antisera. Adenovirus antigens were prepared inHEp-2 or HEK cells and specific antisera were pro-
duced in white rabbits (4). Preimmunization bleed-ings were obtained by cardiac puncture. On day 1,the rabbit was inoculated subcutaneously with 4.0 mlof undiluted adenovirus antigen emulsified in 4.0 mlof complete Freund's adjuvant (Difco); day 7, 1.0 mlof undiluted antigen was inoculated intravenouslyand 5.0 ml of antigen intraperitoneally; day 14, 1.5ml of antigen was inoculated intravenously and 5.0ml intraperitoneally; day 21, 2.0 ml of antigen wasinoculated intravenously and 5.0 ml intraperito-neally; day 28, trial bleeding. Antisera prepared inthis way titered 1:512 to 1:2048 against 100 mediantissue culture infective dose of type-specific adeno-virus by neutralization.
Serology. Rabbit serum-neutralizing adenovirusantibodies were titered in microplates by the methodof Rosenbaum, Edwards, and Sullivan (Amer. Pub.Health Ass. 97th Annu. Meeting, Philadelphia,
389
on May 25, 2020 by guest
http://aem.asm
.org/D
ownloaded from

McCORMICK, GALAPON, AND BERLING
1969). Dilutions of serum and virus were incubatedat room temperature for 2 hr and applied with asuspension of HEp-2 cells to the wells of a microtiterplate (U-shaped wells, Cooke Engineering). Neu-tralizing antibody titers were read after 3 days ofincubation.
Adenovirus complement-fixing antibodies weredetected in acute and convalescent sera from MarineCorps trainees by the micromethod of Sever using 4to 6 units of antigen and 2 units of complement (16).
Fluorescent-antibody conjugates. Globulinswere prepared from the hyperimmune rabbit serumby precipitation with cold 3.52 M (NH4),SO4 (6).Ammonium sulfate was removed by dialysis against0.15 M sodium chloride. Total protein, albumin, andglobulin were assayed by the biuret method.
Purified globulin suspended in 0.15 sodium chlo-ride was diluted in 0.5 M pH 9.0 carbonate-bi-carbonate buffer so as to contain 10 mg of proteinglobulin/ml of solution. Fluorescein isothiocyanateisomer I (FITC, BioQuest, Division of Becton, Dick-inson, and Company) was added to the globulin sus-pension at a ratio of 0.02 mg of FITC/mg of proteinglobulin. After incubation of the reaction mixture,excess unconjugated FITC was removed by dialysis.
Fluorescent-antibody conjugates cross-reactedwith other adenovirus types in vitro unless they werefirst absorbed with HeLa-M cells at a concentrationof 1 ml of packed cells/3 ml of FITC-conjugated an-tisera as was done. Preincubation of antigen withunconjugated specific antisera blocked specificstaining by fluorescein-tagged antisera.
Fluorescein-tagged antisera were titered in theusual fashion by the direct fluorescent-antibodystaining method. Target antigens were HeLa-M cellsinfected with the appropriate adenovirus type. In-fected cells were removed to cover slips, stained, andmounted on microscope slides in Elvanol (Du Pont)(12). Stained cells were examined for fluorescence ona Zetopan research microscope using a 3.0-mm BG12 exciter filter and a GG 9 or GG 13 barrier filter.
Trainees. A total of 37 Marine Corps traineeswere studied with oropharyngeal scrapings and athroat gargle for virus isolation. Acute sera were ob-tained from all trainees; however, because of con-flicts in training, convalescent sera were studiedfrom only 10 trainees. The group on which studieswere essentially complete included four traineeshospitalized for acute respiratory disease and eighttrainees seen as outpatients for acute respiratorydisease (ARD) (Table 1).
Trainees were studied between 13 and 23 March1972 during the final stages of an adenovirus type 4epidemic. From 6 March until 31 March 1972, 27trainees were admitted to the hospital for acute re-spiratory disease and adenovirus type 4 was isolatedfrom 15 of these men. During the same period oftime, 175 trainees were seen at the dispensary forARD, and adenovirus type 4 was isolated from 25 ofthese men. The Virology Division isolated adeno-virus type 7 from only one man during the periodfrom 13-23 March.
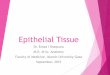
Isolation and identification of adenovirus from theinfected trainees have been described (18). Orophar-yngeal cells were removed by scraping with a
wooden coffee stirrer (Fig. 1; Forster Mgf. Co., Wil-ton, Maine). Epithelial cells were smeared on coverslips, fixed for 60 sec in cold acetone, and stained bythe direct method with fluorescein-tagged antisera toadenovirus strains. Fluorescein-tagged antisera wereused at dilutions of 1: 20 to 1: 30. As an alternative,
TABLE 1. Results of staining adenovirus-infectedoropharyngeal cells with fluorescein-tagged
adenovirus antiserum
ThroatAdenovirus scraping
Hospi- complement- stained withtal (H) Vir fixation conjugate
Patient patient isolation against:(0) Con- Adeno- Adeno-
Acute vales- virus viruscent type 4 type 7
GSK H Ad 7 N.T.a N.T. N.T. +CQF 0 Ad 4 <1:2 1:64 + _RJS 0 Ad 4 1:8 1:8 - +MM 0 Ad 4 N.T. N.T. + -
JML 0 Ad 4 <1:2 1:64 + -
PRD H None 1:8 1:64 + -
LWW H None 1:4 1:32 + -
RS H None 1:4 1:64 - +LCP 0 None <1:2 1:64 -
SMM 0 None 1:32 1:32 -
DEF 0 None 1:32 1:32 +NG 0 None 1:8 1 :8 +
a N.T.: Not tested.
FIG. 1. Method for obtaining epithelial cell scrap-ings in the field. Erythema was frequently the onlyphysical finding upon examination of the oropharynxof adenovirus-infected trainees.
390 APPL. MICROBIOL.
on May 25, 2020 by guest
http://aem.asm
.org/D
ownloaded from

PATHOLOGY OF INFECTED OROPHARYNGEAL CELLS
epithelial cells were smeared on a microscope slide,fixed in ethyl alcohol, and stained by the method ofPapanicolaou (13).
RESULTSDetection of adenovirus antigens. Table 1
includes the data of the patients from whomserological and fluorescent-antibody studieswere complete. Fluorescent staining detectedadenovirus in cells from 10 of the 12 traineestested, and virus was isolated from five of thetrainees. In four trainees the same adenovirustype was detected by both isolation and fluo-rescence; however, in one instance the adeno-virus type was incorrectly identified by fluo-rescence. Epithelial cell scrapings were re-corded as negative from trainee LCP, eventhough a complement-fixation test indicatedthat adenovirus disease had been present.Adenovirus type 4 was isolated from patientCQF on two occasions separated by a 7-dayperiod. The scraping was positive for fluores-cence only at the time of the second dispen-sary visit.Two additional trainees (DEF, NG) demon-
strated positive fluorescence even though therewas no fourfold rise in complement-fixing anti-bodies and no virus was isolated. Similarly,one patient (RJS) shed virus and demon-strated fluorescent epithelial cells in the ab-sence of a fourfold rise in antibody.
Pathology of the inflammatory response.A large number of leukocytes were admixedwith the epithelial cells obtained by scrapingthe oropharynx. The leukocyte response con-sisted mainly of polymorphonuclear leuko-cytes, although rare mononuclear cells werealso seen. Inflammatory cells were present ingreatest numbers in the hospitalized traineesin whom severe and sometimes exudativepharyngitis occurred. Increased numbers ofleukocytes were associated with increased de-struction and alteration of epithelial cells, andan increased amount of cellular debris waspresent, some of which demonstrated specificstaining for adenovirus antigens.Polymorphonuclear leukocytes emitted
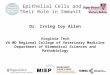
bright nonspecific autofluorescence when theepithelial cell scrapings were examined underthe fluorescence microscope (Fig. 2). Polymor-phonuclear leukocytes showed bright greenfluorescence regardless of the specificity of theconjugate which was applied, and fluorescenceoccurred in the complete absence of epithelialcell staining. It became important to differen-tiate on morphological grounds leukocytes withautofluorescence from epithelial cells with spe-cifically stained intracellular adenovirus anti-gens. Furthermore, we could not exclude thepossibility that some of the leukocytes hadingested or were infected by adenovirus anti-gens and were stained because they contained
VR.FIG. 2. Autofluorescence of polymorphonuclear leukocytes in preparations of scrapings from the infected
oropharynx. This type of green fluorescence can sometimes be confused with the specific fluorescence ofstained adenovirus-infected cells. Glycerine, x600.
VOL. 24, 1972 391
on May 25, 2020 by guest
http://aem.asm
.org/D
ownloaded from

McCORMICK, GALAPON, AND BERLING
such material. Studies with rhodamine-taggedantisera would have evaluated this possibility,because the leukocytes would have emittedgreen autofluorescence, whereas rhodamine-tagged antisera would have stained viral an-tigen red.Pathology of infected epithelial cells. Epi-
thelial cells scraped from the oropharynx ofinfected trainees demonstrated a cytopatho-genic effect typical of adenovirus-infectedtissue culture preparations. A striking featurewas the similarity between the appearance ofclusters of round cells in both the naturalinfection and in the infection of cell mono-layers in tissue culture. Clusters were noted inboth Papanicolaou-stained (Fig. 3) and fluores-cein-stained (Fig. 4) preparations from thethroat scrapings. Infected Papanicolaou-stained cells were characterized by enlarge-ment of the nucleus, lighter staining of nuclearmaterial, and shrinking of the cytoplasm untilit formed a narrow ring around the nucleus.Contrast adenovirus-infected epithelial cells(Fig. 3) with scrapings from the buccal mucosaof a volunteer who was uninfected by adeno-virus (Fig. 5).
Adenovirus antigens appeared in the nucleiof epithelial cells in the form of 10 to 25 gran-ular clusters (Fig. 6, 7). In other cells the entirenucleus was filled with antigen (Fig. 8). Fi-nally, cells were seen in which the staining was
confined chiefly to the cytoplasm with little orno nuclear staining (Fig. 9). As the antigenicmaterial in the nucleus increased and eventu-ally entered the cytoplasm, the cell nuclei in-creased in size and the cytoplasm became lessprominent. Cells at all stages of infection werenoted in the same individual; however, cellswith cytoplasmic viral antigens were foundseveral times more often than cells with densenuclear staining.
DISCUSSIONFluorescent-antibody methods were capable
of detecting adenovirus antigens in epithelialcell scrapings obtained from infected MarineCorps trainees. In trainees in whom studieswere complete, the fluorescent-antibody tech-nique demonstrated virus at approximately thesame frequency as standard virus isolationtechniques (Table 1); however, a major disad-vantage that will require further work withvarious dilutions of fluorescein-tagged antiserais that conjugates were not completely specificfor a given adenovirus type. Furthermore,there is also the possibility that fluorescein-tagged adenovirus antiserum might stain cellsobtained from trainees naturally infected withother viral agents such as coxsackie A-21, par-ainfluenza, or influenza strains.
After reagents were prepared, the fluores-cent-antibody method had the advantage of
0.. ...
FIG. 3. Small cluster of exfoliated epithelial cells showing adenovirus cytopathogenic effect. Papanicolaou-stained. Magnification, x430.
392 APPL. MICROBIOL.
sa.
on May 25, 2020 by guest
http://aem.asm
.org/D
ownloaded from

PATHOLOGY OF INFECTED OROPHARYNGEAL CELLS
FIG. 4. Cluster of adenovirus-infected epithelial cells similar to Fig. 3 except that staining is with fluores-cein-conjugated adenovirus type 4 antiserum diluted 1:20. Glycerine, x600.
FIG. 5. Papanicolaou-stained oropharyngeal epithelial cells from an uninfected volunteer. Note the small,dense nucleus, and the large area occupied by the cytoplasm. Magnification, x430.
VOL. 24, 1972 393
on May 25, 2020 by guest
http://aem.asm
.org/D
ownloaded from

McCORMICK, GALAPON, AND BERLING
m :7FIG. 6, 7. Fluorescent nuclear granules of adenovirus type 4-infected human epithelial cells. The increased
nuclear-cytoplasmic ratio indicates that the cell in Fig. 6 appears to be at a slightly more advanced stage ofinfection than that ofFig. 7. Glycerine, x600.
rapidity, since a diagnosis could be reachedapproximately 2 hr after a scraping was ob-tained, whereas the usual methods required 1to 3 weeks before virus proliferation caused acytopathogenic effect in tissue culture andbefore virus neutralization could be carriedout. The cost of cover slips, microscope slides,and reagents for fluorescence microscopy was
small as compared with tissue culture tubes,media, and neutralization plates required bythe standard procedures.
It was of additional interest that Papanico-laou-stained scrapings demonstrated a cyto-pathogenic effect similar to that seen in labo-ratory tissue cultures infected with adenovirusstrains. It is possible that a rapid presumptive
394 APPL. MICROBIOL.
on May 25, 2020 by guest
http://aem.asm
.org/D
ownloaded from

PATHOLOGY OF INFECTED OROPHARYNGEAL CELLS
,,. ,, _ # . :'': i : : '.':°SsSE.°Zg~~~~~~~~~~~~~~~~~~~~~~~N;":.:-::.
FIG. 8. Two adenovirus-infected cells showing intense specific nuclear staining for adenovirus type 4.Glycerine, x600.
FIG. 9. Clusters of adenovirus-infected cells in which viral antigen appears mainly in the cytoplasm. Thistype of staining was seen more frequently than nuclear staining. Glycerine, x600.
diagnosis of adenovirus disease could be ob-tained in a large proportion of patients by theexamination of Papanicolaou-stained, exfo-liated, oropharyngeal cells. This likelihoodshould be evaluated if future epidemics occur.
Of particular interest was the cellular in-flammatory response which accompanied pha-ryngeal adenovirus infections. Leukocytesprobably play a role in the immune responseto viral respiratory disease. These authors and
395VOL. 24, 1972
on May 25, 2020 by guest
http://aem.asm
.org/D
ownloaded from

396 McCORMICK, GALA
many others have suggested that surfaceneoantigens induced by intracellular virusinfection may induce a cellular as well as anantibody-mediated immune reaction to virus-infected target cells (K. Hayashi, J. D. Rosen-thal, and A. L. Notkins. Abstr. Ann. Meet.Amer. Soc. Microbiol., p. 235, 1972; references3 and 11). It is possible that the inflammationpresent in the respiratory passages of patientsinfected with lytic viruses, such as adenovirustypes, may in part be due to the interaction ofspecific antibody and sensitized immune cellswith virus-infected cells. Notkins and co-workers have demonstrated that surfaceneoantigens coded for by the genetic materialof intracellular virus induce an antibody-me-diated immune response which results in thedestruction of infected cells even before virus-specific cell lysis had taken place (K. Hayashi,J. D. Rosenthal, and A. L. Notkins. Abstr.Ann. Meet. Amer. Soc. Microbiol., p. 235,1972; reference 3). Studies in this laboratoryhave shown that pre-existing serum immuno-globulin G and A molecules enter the nasalpassages during acute adenovirus disease. Spe-cific antibody and complement componentsreacting with infected cells as well as with ex-tracellular virus may release factors whichpromote the accumulation of inflammatorycells in the nasal and pharyngeal passages.The predominant leukocyte present in the
scrapings was the polymorphonuclear leuko-cyte, and there were only a few monocytes andlymphocytes present. Clyde has described aleukocyte response to experimental Myco-plasma pneumoniae infection in Syrian ham-sters (7). Polymorphonuclear leukocytesformed the predominant cell-mediated re-sponse beginning 9 days after infection. After 2weeks lymphocytes and other mononuclearcells entered the bronchial spaces in largenumbers. A characteristic phenomenon wasthe formation of "rosettes" of immunocytesaround epithelial cells which were also charac-teristic of the response when leukocytes werecultured in vitro. Clyde postulated that suchrosettes might be present in sputa obtainedfrom patients with M. pneumoniae pneu-monia. His studies of M. pneumoniae diseasein hamsters, combined with the observation ofa cellular response to adenovirus disease inman, should prompt further evaluation of cel-lular immunological responses in adenovirusinfections. In particular, it would be inter-esting to see whether the convalescent stagesof adenovirus disease are associated with anincreased number of mononuclear leukocytes
P'ON, AND BERLING APPL. MICROBIOL.
in the pharyngeal scrapings or nasal wash.This study clearly confirms earlier work
which described the distribution of intracel-lular antigen in adenovirus-infected cells (2,14). The later stages of adenovirus infectionin vitro were associated with large numbers ofcells in which antigen took up residence pri-marily in the cytoplasm. In this study, adeno-virus antigens were located most frequentlyin the cytoplasm of cells which were obtainedfrom the oropharynges of infected trainees.
After inoculation of throat gargle specimensonto tissue for virus isolation, epithelial cellsare frequently seen floating in the media. Thisstudy indicated that such epithelial cells maybe filled with virus. Single adenovirus-infectedcells have been estimated to contain up to20,000 infectious virus particles (14), and it isthese "packages" of virus which may providethe bulk of the infectious virus particles ob-tained in a throat gargle specimen.
ACKNOWLEDGMENTSWe thank the following individuals for their excellent
technical assistance: Edward P. Smith, Raymond S. Combs,Ronald F. Pettus, Gary Russell, Hannah B. Burns, DorothyD. Pierce, Roy F. Rhoads, William C. Jones, John A. Davies,and John R. Mitzel.
LITERATURE CITED1. Biegeleisen, J. Z., Jr., L. V. Scott, and V. Lewis, Jr.
1959. Rapid diagnosis of herpes simplex virus infec-tions with fluorescent antibody. Science 129:640-641.
2. Boyer, G. S., F. W. Denny, Jr., and H. S. Ginsberg.1959. Sequential cellular changes produced by types 5and 7 adenoviruses in HeLa cells and in human am-niotic cells. Cytological studies aided by fluorescent-labelled antibody. J. Exp. Med. 110:827-844.
3. Brier, A. M., C. Wohlenberg, J. Rosenthal, M. Mage,and A. L. Notkins. 1971. Inhibition or enhancement ofimmunological injury of virus infected cells. Proc.Nat. Acad. Sci. U.S.A. 68:3073-3077.
4. Bucca, M. A., D. F. Palmer, and L. A. White. 1968. Pro-cedural manual for production of viral and richettsialreagents., p. 2. National Communicable Disease Cen-ter, Atlanta.
5. Chanock, R. M., W. Ludwig, R. J. Heubner, T. R. Cate,and L. W. Chu. 1966. Immunization by selectiveinfection with type 4 adenovirus grown in human dip-loid tissue culture. I. Safety and lack of oncogenicityand tests for potency in volunteers. J. Amer. Med.Ass. 195:445-452.
6. Cherry, W. B. 1970. Fluorescent-antibody techniques, p.693-704. In John E. Blair, Edwin H. Lennette, JosephP. Truant (ed.), Manual of clinical microbiology. Wil-liams & Wilkins Co., Baltimore.
7. Clyde, W. A., Jr. 1971. Immunopathology of experi-mental Mycoplasma pneumoniae disease. Infect.Immunity 4:757-763.
8. Coyne, V. E., B. S. Blumberg, and I. Millman. 1972.Detection of Australia antigen in human tissue cul-ture preparations. Proc. Soc. Exp. Biol. Med. 138:1051-1057.
9. Edmondson, W. P., R. H. Purcell, B. F. Gundelfinger, J.W. P. Love, W. Ludwig, and R. M. Chanock. 1966.
on May 25, 2020 by guest
http://aem.asm
.org/D
ownloaded from

PATHOLOGY OF INFECTED OROPHARYNGEAL CELLS
Immunization by selective infection with type 4 ade-novirus grown in human diploid tissue culture. II.Specific protective effect against epidemic disease. J.Amer. Med. Ass. 195:453-459.
10. Hirschman, S. Z. 1971. Approaches to antiviral chemo-therapy. Amer. J. Med. 51:699-703.
11. McCormick, D. P. 1972. Hypothesis: herpes simplexvirus as a cause of Bell's palsy. Lancet 1:937-939.
12. McCormick, D. P., Q. Galapon, C. Berling, E. P. Smith,R. Combs, G. Russell, and R. F. Pettus. 1972. Therapid diagnosis of acute respiratory disease due toadenovirus. Preparation and standardization of fluo-rescent antibody reagents. Naval Medical Field Re-search Laboratory, Camp Lejeune, N.C. Reports, vol.22, no. 11.
13. Papanicolaou, G. N. 1954. Atlas of exfoliative cytology,p. 6-7. Harvard University Press, Cambridge, Mass.
14. Pereira, H. G., A. G. Allison, and B. Balfour. 1959. Mul-
tiplication of adenovirus type 5 studied by infectivitytitrations and by the fluorescent antibody technique.Virology 7:300-314.
15. Scott, R. McN., B. A. Dudding, S. V. Romano, and P.K. Russell. 1972. Enteric immunization with live ade-novirus type 21 vaccine. II. Systemic and local im-mune responses following immunization. Infect.Immunity 5:300-310.
16. Sever, J. L. 1966. Application of a microtechnique toviral serological investigations. J. Immunol. 88:320-329.
17. Tateno, I., 0. Kitamoto, and A. Kawamura. 1966. Di-verse immunocytologic findings of nasal smears in in-fluenza. N. Engl. J. Med. 274:237-242.
18. Wenzel, R. P., D. P. McCormick, E. P. Smith, and W.E. Beam, Jr. 1971. Acute respiratory disease: clinicaland epidemiologic observations of military trainees.Mil. Med. 136:873-880.
VOL. 24, 1972 397
on May 25, 2020 by guest
http://aem.asm
.org/D
ownloaded from