Embed Size (px)
Citation preview

Pathology of Pathology of
Gestational Gestational
Trophoblastic DiseaseTrophoblastic Disease
Modified WHO classification of GTDModified WHO classification of GTD
�� Molar lesionsMolar lesions�� Hydatidiform moleHydatidiform mole
�� CHMCHM
�� PHMPHM
�� Invasive moleInvasive mole
�� Non molar lesionsNon molar lesions�� ChoriocarcinomaChoriocarcinoma
�� Placental site trophoblastic tumor (PSTT)Placental site trophoblastic tumor (PSTT)
�� Epithelioid trophoblastic tumor (ETT)Epithelioid trophoblastic tumor (ETT)
�� MiscellaneousMiscellaneous trophoblastictrophoblastic lesionslesions�� Exaggerated placental siteExaggerated placental site
�� Placental site nodulePlacental site nodule
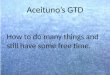
Normal Normal
pregnancypregnancyPHMPHM CHMCHM
10%10% 90%90%
PloidyPloidy 2N2N 3N3N 2N2N 2N2N
ChromosomeChromosome 46XX46XX
46XY46XY
69XXY 69XXY (70%)(70%)
69XXX 69XXX (27%)(27%)
69XYY 69XYY (3%)(3%)
46XX 46XX (89(89--97%)97%)
46XY 46XY (7(7--13%)13%)
No 46 YYNo 46 YY
ParentalityParentality BiparentalBiparental Biparental Biparental
DiandricDiandricPaternal Paternal
DiandricDiandric
Molar pregnancy
Pathology of CHMPathology of CHM
Macro : Vesicles, maximal diameter 2 cm.Macro : Vesicles, maximal diameter 2 cm.
Pathology of CHMPathology of CHM
�� MicroMicro
�� Enlarged villi, cavitation (necrosis)Enlarged villi, cavitation (necrosis)
�� Trophoblastic proliferation around villi Trophoblastic proliferation around villi with minimal atypiawith minimal atypia
�� Absence or paucity of fetal stromal BVsAbsence or paucity of fetal stromal BVs
�� Atypia of ITs atAtypia of ITs at decidual implantation decidual implantation site.site.

Large swollen villi Central cistern
CHM
CHMCHM
Concentric CT & ST hyperplasia Atypical implantation site
�� In the 1960s mean GA of CHM = 17 wksIn the 1960s mean GA of CHM = 17 wks
�� Nowadays = 9.4 wksNowadays = 9.4 wks
�� Common error is diagnosis of early CHM Common error is diagnosis of early CHM
as PHMas PHM
�� MacroMacro
�� Resemble abortus with some vesiclesResemble abortus with some vesicles
Pathology of early CHMPathology of early CHM Early CHMEarly CHM
�� MicroMicro�� Slight enlargement with Slight enlargement with scattered scattered cavitiescavities in villiin villi
�� Typical villous morphology : Typical villous morphology : cauliflower cauliflower likelike (lobulated appearance)(lobulated appearance)
�� Focal to diffuse trophoblastic atypiaFocal to diffuse trophoblastic atypia�� Villous stromaVillous stroma
�� HypercellularHypercellular (stellate mesenchymal cells in blue (stellate mesenchymal cells in blue myxoid matrix) = fibroadenoma likemyxoid matrix) = fibroadenoma like
�� Prominent karyorrhexis in villous mesnchymal Prominent karyorrhexis in villous mesnchymal cells, cells, stromal nuclear debrisstromal nuclear debris
�� Numerous vessels Numerous vessels with nucleated RBCswith nucleated RBCs
Early CHMEarly CHM
Typical features in early CHMTypical features in early CHM�� Abnormally shaped villi Abnormally shaped villi (bullous or (bullous or polypoid)polypoid)
�� Stromal mucinStromal mucin�� Stromal nuclear debrisStromal nuclear debris (resulted (resulted of increased stromal proloferation of increased stromal proloferation and apoptosisand apoptosis
•Moderate villous enlargement•Not prominent cistern•Concentric trophoblastic •hyperplasia
Hypercellular stromaBluish appearance
Irregular villous contours “knuckles or toes” Atypical implantation site
Early CHM

MacroMacro
••Vesicle appearance (partial change) vary to GAVesicle appearance (partial change) vary to GA
••Presence of fetus (more often malformed) or fetal partPresence of fetus (more often malformed) or fetal part
PHM
CHM
Pathology of PHMPathology of PHM
�� MicroMicro�� Two population of villiTwo population of villi
�� Smaller fibrotic normal appearing villiSmaller fibrotic normal appearing villi�� Larger irregular shaped hydropic villiLarger irregular shaped hydropic villi
�� Central cisternsCentral cisterns�� Irregular scalloped borderIrregular scalloped border (Norwegian fjord type , (Norwegian fjord type , sharp angulated) sharp angulated)
�� Invagination of trophoblast and Invagination of trophoblast and round inclusionsround inclusions(solid or cystic)(solid or cystic)
�� Evidence of fetal developmentEvidence of fetal development : No : No fetal tissue does not rule out PHM.fetal tissue does not rule out PHM.
�� Late PHMLate PHM……..Angiomatoid malformationAngiomatoid malformationSyndactyly
Mixed population of vliil Mild ST proliferation
Coexisting fetal tissue PHM
Cistern &scalloped villi
Mixed population of vliil Angiomatoid change
PHM
Round inclusions
Pathological mimics of PHMPathological mimics of PHM
�� Early CHMEarly CHM
�� Hydropic spontaneous miscarriageHydropic spontaneous miscarriage
�� Twin gestation with CHM and existing Twin gestation with CHM and existing
fetusfetus
�� Placental angiomatous malformationPlacental angiomatous malformation

FeaturesFeatures CHMCHM PHMPHM Hydropic Hydropic
abortusabortus
VilliVilli Hydropic & Hydropic &
cisternscisternsFocal hydropic, Focal hydropic,
double population double population
villivilli
Mild, seldom Mild, seldom
cisterns, very cisterns, very
rare large villirare large villi
Villous Villous
outlinesoutlines
��Rather smoothRather smooth
��Polypoid in early Polypoid in early
CHMCHM
Scalloped Scalloped
Villous Villous
inclusioninclusionIrregularIrregular, cystic , cystic
or solidor solidRoundRound, cystic or , cystic or
solidsolid
Villous Villous
stromastroma
Early CHM : Early CHM :
nuclear debris nuclear debris Nuclear debris Nuclear debris seen around VSSsseen around VSSs
Nuclear debris in Nuclear debris in
VSS wall or VSS wall or
lumenslumens
(occurring after (occurring after
embryonic embryonic
demise)demise)
FeaturesFeatures CHMCHM PHMPHM Hydropic Hydropic
abortusabortus
Villous Villous
VSSsVSSs
��Presence in early Presence in early
CHMCHM
��Absence in late Absence in late CHMCHM
Angiomatoid Angiomatoid malformation in malformation in late PHMlate PHM
PresencePresence
TrophoblastsTrophoblasts ��Multifocal or Multifocal or circumferentialcircumferential
��Significant Significant nuclear atypia at nuclear atypia at implantation siteimplantation site
��<7 % of cases <7 % of cases
show proliferationshow proliferation
��Multifocal > Multifocal > circumferentialcircumferential
��No sig atypiaNo sig atypia
��Presence in Presence in
early gestationearly gestation
��Polar or Polar or intervillousintervillous
��No sig. atypiaNo sig. atypia
Embryonic Embryonic
tissuetissue
AbsentAbsent Present, malformed Present, malformed fetus, IUGRfetus, IUGR
Often lostOften lost
KaryotypeKaryotype 46XX, Uniparental46XX, Uniparental Generally triploid, Generally triploid, biparentalbiparental
BiparentalBiparental
Genetics abnormality in PHMGenetics abnormality in PHM
�� 1% of conceptus = triploidy1% of conceptus = triploidy
�� TriploidyTriploidy 80% diandric80% diandric PHMPHM
20% digyny20% digyny Non molarNon molar
�� Most of PHMs are triploidMost of PHMs are triploid
�� Reported teraploid (> 1 paternal set of Reported teraploid (> 1 paternal set of
chromosome)chromosome)
Special investigation in Dx of Special investigation in Dx of
molar pregnancymolar pregnancy
ImmunohistochemistryImmunohistochemistry�� P57P57kip2kip2 (maternally expressed imprinted (maternally expressed imprinted
gene):gene): CHM VS non CHMCHM VS non CHM
Ploidy analysisPloidy analysis�� Triploid Triploid PHM VS non PHMPHM VS non PHM
Interphase cytogeneticsInterphase cytogenetics�� Identify chromosome aberrations by in situ Identify chromosome aberrations by in situ
hybridization (ISH) using chromosome hybridization (ISH) using chromosome specific probes (chromosome 1, X, Y)specific probes (chromosome 1, X, Y)
P57P57kip2 kip2 oror IPL/PHLDA2IPL/PHLDA2
�� Located at Located at chromosome 11p15.5chromosome 11p15.5�� Strongly Strongly paternally imprintedpaternally imprinted, being , being expressed predominantlyexpressed predominantly from maternal allele from maternal allele
�� Potent cell cycle inhibitor and tumor Potent cell cycle inhibitor and tumor suppressorsuppressor
�� lack of lts activity can lead to loss of cell cycle lack of lts activity can lead to loss of cell cycle control and hyperproliferationcontrol and hyperproliferation
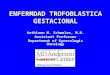
�� Normal pregnancy and PHM : positive at nuclei Normal pregnancy and PHM : positive at nuclei of villous stroma, villous CT, decidual and of villous stroma, villous CT, decidual and extravillous trophoblastextravillous trophoblast
�� CHM : negative at nuclei of villous stroma, CHM : negative at nuclei of villous stroma, villous CTvillous CT
Normal villous Hydropic villous
PHM CHM
P57P57kip2kip2

P57P57kip2kip2 expressionexpression
TissueTissue Villous Villous
mesenchymemesenchymeCTCT STST IVT*IVT* DeciduaDecidua
Normal Normal
placentaplacenta
(all GA)(all GA)
++ ++ -- ++ ++
Hydropic Hydropic
degenerationdegeneration++ ++ -- ++ ++
CHMCHM -- -- -- ++ ++
PHM(both PHM(both
hydropic and hydropic and
normal villi)normal villi)
++ ++ -- ++ ++
*Intervillous trophoblast
Diego H et al, Am J Sur Pathol 2001;25(10):1225-30
PHMPHM CHMCHM Hydropic Hydropic
abortusabortus
P57P57kip2 kip2
expressionexpressionNo lossNo loss LossLoss No lossNo loss
Proliferation Proliferation
indexindex
Intermediate Intermediate
(25(25--50%)50%)High High
(50-100%)
Low to Low to
intermediate intermediate
(0(0--50%)50%)
PloidyPloidy TriploidTriploid DiploidDiploid DiploidDiploid
Markers for molar pregnancyMarkers for molar pregnancy
Pathology of invasive molePathology of invasive mole
�� Hydatidiform in which hydropic Hydatidiform in which hydropic
villi invade villi invade myometriummyometrium oror
BVs BVs or even the or even the extrauterine extrauterine sitessites
�� Dependent on extent of invasionDependent on extent of invasion
Invasive mole

GTDGTD
�� GTDs are distinct from other tumors in the GTDs are distinct from other tumors in the human body in that they are genetically or human body in that they are genetically or allograft in the motherallograft in the mother’’s bodys body..
�� They are They are fetal tumorsfetal tumors that are arising in that are arising in the motherthe mother’’s body.s body.
�� The The remarkable curabilityremarkable curability of GTDs with of GTDs with chemoRx might reflect the underlying chemoRx might reflect the underlying immune response of the mother to paternal immune response of the mother to paternal antigens expressed on the surface of antigens expressed on the surface of trophoblastic cells.trophoblastic cells.
Int J Gynecol Cancer 2006;16:1500Int J Gynecol Cancer 2006;16:1500--1515
Trophoblast
Villous Nonvillousor
ExtravillousCT
STIT•First trimester•Developingcytotrophoblastic column
Proliferation and differentiation of CT of anchoring CV
Migrate as cell columns in first few wks of pregnancy to invade decidua
TrophoblastsTrophoblasts
�� Trophoblastic differentiation at 7 days Trophoblastic differentiation at 7 days blastocystblastocyst
�� TypeType�� Villous Villous CTCT
IT(small amount)IT(small amount)
STST
�� ExtravillousExtravillous ITIT
ST(small amount)ST(small amount)
Vacuolated TrophoblastVacuolated Trophoblast at at chorion in late pregnancy chorion in late pregnancy (described by Yeh 1989)(described by Yeh 1989)
Trophoblastic tumor differentiationTrophoblastic tumor differentiation
CTCT ChoriocarcinomaChoriocarcinoma
STST PSTTPSTT
Implantation site ITImplantation site IT Exaggerated placental Exaggerated placental
site site
Vacuolated T Vacuolated T ETTETT
Placental site nodulePlacental site nodule
Trophoblastic cellsTrophoblastic cellsFeaturesFeatures CTCT STST ITIT
Cell sizeCell size Small Small
polyhedralpolyhedralLargeLarge Medium polyhedral Medium polyhedral
to spindleto spindle
CytoplasmCytoplasm Clear, Clear,
distinct cell distinct cell
borderborder
��Amphophilic or Amphophilic or
eosinophiliceosinophilic
��Filmly to coarsely Filmly to coarsely
vacuolated (irregular vacuolated (irregular
lacy pattern)lacy pattern)
EosinophilicEosinophilic
NucleusNucleus Single, Single,
vesicularvesicularSmall, Small,
hyperchromatichyperchromaticSingle, bi, multiSingle, bi, multi--
nucleation at nucleation at
placental siteplacental site
MitosisMitosis ++ -- ++
LocationLocation Inner layer Inner layer
of villi of villi
coveringcovering
Outer layer of villi Outer layer of villi
coveringcovering��Sit in fibrin materialSit in fibrin material
��Within endoWithin endo--
myometriummyometrium
��In walls or lumens In walls or lumens
of spiral arteriolesof spiral arterioles
CT & ST hCG
Impantation site IT Epithelioid IT

Hormone productionHormone production
TrophoblastTrophoblast hCGhCG hPLhPL PLAPPLAP InhibinInhibin CytokeratinCytokeratin P63P63
CTCT -- -- -- ++ ++
∆∆N N
isoformisoform
STST ++++++ ++ ++
ITIT ++ focalfocal ++++ ++ ++
Vacuolated Vacuolated
ITIT++ ++++ ++ + +
TA TA
isoformisoform
+++ +
++
Pathology of ChoriocarcinomaPathology of Choriocarcinoma
Macro : Well circumscribed nodular lesion with Macro : Well circumscribed nodular lesion with
dominantly hemorrhagic structuredominantly hemorrhagic structure
Pathology of ChoriocarcinomaPathology of Choriocarcinoma
MicroMicro�� No chorionic villiNo chorionic villi�� Peripheral trophoblasts (lack intrinsic Peripheral trophoblasts (lack intrinsic tumor vasculatures)tumor vasculatures)
�� BiBi--laminar patternlaminar pattern (recapitulates (recapitulates trophoblast of early implanting trophoblast of early implanting blastocyst)blastocyst)
�� Extensive myometrial invasion Extensive myometrial invasion without destruction or necrosis of without destruction or necrosis of myometriummyometrium
�� Tumor in dilated vascular sinusesTumor in dilated vascular sinuses
Choriocarcinoma
Biphasic trophoblasts
Choriocarcinoma
Marked trophoblastic atypia
Hemorrhagic necrosis
Special studySpecial study of choriocarcinomaof choriocarcinoma
�� ImmunohistochemistryImmunohistochemistry�� UsefulUseful
�� Positive Positive �� hCGhCG (sig +ve), (sig +ve), CK, EMA, CEA, Ki67, hPLCK, EMA, CEA, Ki67, hPL(fewer cells), (fewer cells), PLAPPLAP (rare)(rare)
�� Genetic polymorphismsGenetic polymorphisms�� DDX gestation or non gestational DDX gestation or non gestational choriocarcinomachoriocarcinoma
�� To define prognosis and influencing therapeutic To define prognosis and influencing therapeutic decisiondecision
�� To understand biology of trophoblastic tumorTo understand biology of trophoblastic tumor

Pathology of PSTTPathology of PSTT
MacroMacro
�� Variable appearanceVariable appearance
�� IlledIlled--defined massdefined mass
��Well circumscribed noduleWell circumscribed nodule
�� In myometrium with or without In myometrium with or without
projection into endometrial cavityprojection into endometrial cavity
�� No striking hemorrhage or necrosisNo striking hemorrhage or necrosis
MicroMicro�� Recapitulate appearance seen at placental bedRecapitulate appearance seen at placental bed
�� Diffuse infiltration of mononuclear and multinuclear IT Diffuse infiltration of mononuclear and multinuclear IT arranged in cords, islands, sheets between arranged in cords, islands, sheets between myometrial bundlesmyometrial bundles
�� Vascular invasion recapitulates normal implantation Vascular invasion recapitulates normal implantation site : cell migrate through and replace vessel walls , site : cell migrate through and replace vessel walls , maintaining overall vascular architecturemaintaining overall vascular architecture
�� Less intravascular proliferationLess intravascular proliferation
�� Vary mitotic activityVary mitotic activity
�� Abundant extracellular eosinophilic fibrinoid materialAbundant extracellular eosinophilic fibrinoid material
Pathology of PSTTPathology of PSTT
PSTT
Sheets of atypical IT ITs dissecting through muscle fibers
PSTT
extracellular eosinophilic fibrinoid material
mononuclear and multinclear IT
Pathology of ETTPathology of ETTProposed by Mazur in 1989Proposed by Mazur in 1989
MacroMacro��Nodular expansile patternNodular expansile pattern
��50% of cases arise in lower 50% of cases arise in lower uterine segment or uterine segment or endocervixendocervix
Pathology of ETTPathology of ETT
MicroMicro�� Mixture of mononuclear cells with eosinophilic Mixture of mononuclear cells with eosinophilic or clear cytoplasm forming nests or cordsor clear cytoplasm forming nests or cords
�� Areas of hyalinization or eosinophilic debris Areas of hyalinization or eosinophilic debris simulating tumor cell necrosis at center of simulating tumor cell necrosis at center of tumor nests (resembling keratin material in tumor nests (resembling keratin material in SCC)SCC)
�� Characteristic geographic patternCharacteristic geographic pattern
�� Dysmorphic calcification in areas of necrosisDysmorphic calcification in areas of necrosis
�� Low mitotic activityLow mitotic activity

ETT
Nodular expansile pattern
Mononuclear cells with eosinophilic cytoplasm forming nests or cords
P63
Areas of hyalinization or eosinophilic debris
ETT
PSTT v.s. ETT and choriocarcinomaFeature PSTT ETT Choriocarcinoma
Cellular population
Monomorphic ;
implantation site ITMonomorphic ;
chorionic -type IT
Dimorphic ; primitive previllous -type trophoblast
Cell size and shape
Large and pleomorphic
Small round and uniform
Irregular , highly variable
Cytoplasm Abundant and eosinophilic
Eosinophilic or clear Eosinophilic to purple
Growth Pattern Infiltrating single cells or confluent sheets
Epithelioid nests or cords or solid masses
Dimorphic ; mononucleate trophoblast and ST
Margin Infiltrating Circumscribed Circumscribed , expansile
Hemorrhage Focal or haphazard Usually present Massive and cent ral
Cellular necrosis Usually Absent Extensive Extensive
Calcification Absent Usually present Absent
Vascular invasion
From periphery to lumen
Absent From lumen to periphery
Fibrinoid change Present Present Absent
Mitosis Variable ;0-6/10HPF
Variable ;1-10/10HPF
High ;2-22/10 HPF
Clinical features of PSTT , ETT and choriocarcinoma
Feature PSTT ETT Choriocarcinoma
Clinical Presentation
Missed Abortion Abnormal vaginal bleeding
Persistent GTD after HM
Last Pregnancy or GTD
Variable , can be remote
Variable , can be remote
months
History of mole 5-8% 14% 50%
Serum hCG Low (< 100-2,000IU/L)
Low (50 – 500IU/mL )
High (>10,000IU/mL )
Behavior Variable Variable Aggressive if untreated
Response to chemotherapy
Variable Variable Good
Treatment Surgery (hysterectomy )
Surgery (hysterectomy )
Chemotherapy
Markers for trophoblastsMarkers for trophoblasts
�� hCGhCG�� hPLhPL�� Inhibin Inhibin αα
�� Shih & Kurman showed that Shih & Kurman showed that Inhibin Inhibin αα was expressed was expressed by all population of trophoblasts except CTby all population of trophoblasts except CT
�� Melanoma cell adhesion molecule (MelMelanoma cell adhesion molecule (Mel--CAM) = MUC18CAM) = MUC18�� Kurman found that MelKurman found that Mel--CAM is specific and sensitive CAM is specific and sensitive
marker for IT in normal placenta implantation site and marker for IT in normal placenta implantation site and GTD lesionGTD lesion
�� HLAHLA--GG (non classical major histocompatibility (non classical major histocompatibility class I)class I)�� Singer et al showed positivity in all GTD lesions, but Singer et al showed positivity in all GTD lesions, but
negative in non trophoblastic uterine neoplasmsnegative in non trophoblastic uterine neoplasms
Biomarkers for diagnosis GTDsBiomarkers for diagnosis GTDs
PSTTPSTT ETTETT ChorioCAChorioCA
hCGhCG focalfocal focalfocal diffusediffuse
hPLhPL diffusediffuse focalfocal Few cellsFew cells
PLAPPLAP Occasional Occasional
cellscellsfocalfocal rarerare
P63P63 -- ++ +/+/--
Ki67Ki67 >10%>10% >10%>10% >10%>10%
MelMel--CAMCAM ++ ++ focalfocal
Inhibin Inhibin αα ++ ++ focalfocal
CKCK ++ ++ ++
HLAHLA--GG ++ ++ ++

P63P63
�� Nuclear transcription factor belonging to P53 Nuclear transcription factor belonging to P53 familyfamily
�� Two major isoformsTwo major isoforms
�� CT expresses N isoformCT expresses N isoform
�� Chorionic type ITChorionic type IT expresses TA isoformexpresses TA isoform
�� Different P63 isoforms may be important in Different P63 isoforms may be important in control of trophoblastic differentiation and control of trophoblastic differentiation and placental developmentplacental development
Am J Sur Pathol 2004;28:1177Am J Sur Pathol 2004;28:1177--8383
P63 in normal villous and ETTP63 in normal villous and ETT
Normal villous ETT
HLAHLA--GG
�� Presence on all types of non villous trophoblast, Presence on all types of non villous trophoblast, but is not detected in villous CT and STbut is not detected in villous CT and ST
�� All trophoblastic tumors and tumor like All trophoblastic tumors and tumor like lesions express HLAlesions express HLA--G strongly and G strongly and diffusely diffusely
�� Vast majority of nonVast majority of non--trophoblastic tumors do not trophoblastic tumors do not express HLAexpress HLA--GG
�� Melanoma, renal cell , breast, ovarian and large Melanoma, renal cell , breast, ovarian and large cell carcinoma of lung may show focal cell carcinoma of lung may show focal expressionexpression
Practical immunohistochemistry approach to Practical immunohistochemistry approach to
diagnosis of lesions of nondiagnosis of lesions of non--villous trophoblast in villous trophoblast in
biopsy specimensbiopsy specimens
1.1. To confirm trophoblastic nature of To confirm trophoblastic nature of cellscells
�� hPL, inhibin hPL, inhibin αα, HLA, HLA--G, MelG, Mel--CAM(CD146)CAM(CD146)
�� CK (CAM5.2,AE1/AE3, CK18)CK (CAM5.2,AE1/AE3, CK18)
�� Discriminate trophoblast from CK Discriminate trophoblast from CK ––ve ve
maternal deciduamaternal decidua
2.2. To differentiate between nonTo differentiate between non--neoplastic and neoplastic trophoblastneoplastic and neoplastic trophoblast
�� IHC is of little helpIHC is of little help
�� KiKi--67 >10% in neoplastic lesions67 >10% in neoplastic lesions
33.. To differentiate neoplastic To differentiate neoplastic trophoblastic trophoblastic
cells from otherscells from others-- SCC SCC
-- Smooth muscle cell tumorSmooth muscle cell tumor
4.4. In practical terms, distinction In practical terms, distinction between PSTT and ETT is not really an between PSTT and ETT is not really an important oneimportant one
Practical immunohistochemistry approach to Practical immunohistochemistry approach to
diagnosis of lesions of nondiagnosis of lesions of non--villous trophoblast in villous trophoblast in
biopsy specimensbiopsy specimens