Embed Size (px)
Citation preview
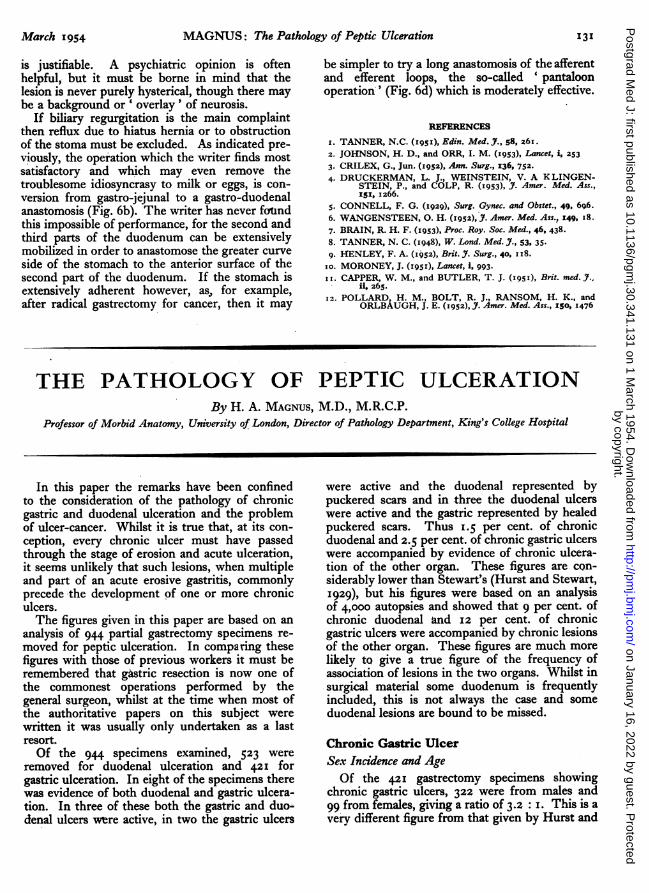
March 1954 MAGNUS: The Pathology of Peptic Ulceration 131
is justifiable. A psychiatric opinion is oftenhelpful, but it must be borne in mind that thelesion is never purely hysterical, though there maybe a background or ' overlay' of neurosis.
If biliary regurgitation is the main complaintthen reflux due to hiatus hernia or to obstructionof the stoma must be excluded. As indicated pre-viously, the operation which the writer finds mostsatisfactory and which may even remove thetroublesome idiosyncrasy to milk or eggs, is con-version from gastro-jejunal to a gastro-duodenalanastomosis (Fig. 6b). The writer has never foundthis impossible of performance, for the second andthird parts of the duodenum can be extensivelymobilized in order to anastomose the greater curveside of the stomach to the anterior surface of thesecond part of the duodenum. If the stomach isextensively adherent however, as, for example,after radical gastrectomy for cancer, then it may
be simpler to try a long anastomosis of the afferentand efferent loops, the so-called 'pantaloonoperation' (Fig. 6d) which is moderately effective.
REFERENCES
I. TANNER, N.C. (i9SI), Edin. Med. J., 58, 261.2. JOHNSON, H. D., and ORR, I. M. (I953), Lancet, i, 2533. CRILEX, G., Jun. (1952), Ann. Surg., 136, 752.4. DRUCKERMAN, L. J., WEINSTEIN, V. A KLINGEN-
STEIN, P., and COLP, R. (1953), J. Amer. Med. Ass.,151, 1266.
5. CONNELL, F. G. (1929), Surg. Gynec. and Obstet., 49, 696.6. WANGENSTEEN, O. H. (1952), 7. Amer. Med. Ass., 149, I8.7. BRAIN, R. H. F. (1953), Proc. Roy. Soc. Med., 46, 438.8. TANNER, N. C. (1948), W. Lond. Med. J., 53, 35.9. HENLEY, F. A. (I952), Brit. J. Surg., 40, I 8.
io. MORONEY, J. (i951), Lancet, i, 993.II. CAPPER, W. M., and BUTLER, T. J. (I95I), Brit. med. J..
ii 265.12. POLLARD, H. M., BOLT, R. J., RANSOM, H. K., and
ORLBAUGH, J. E. (1952), J. Amer. Med. Ass., I50, 1476
THE PATHOLOGY OF PEPTIC ULCERATIONBy H. A. MAGNUS, M.D., M.R.C.P.
Professor of Morbid Anatomy, University of London, Director of Pathology Department, King's College Hospital
In this paper the remarks have been confinedto the consideration of the pathology of chronicgastric and duodenal ulceration and the problemof ulcer-cancer. Whilst it is true that, at its con-ception, every chronic ulcer must have passedthrough the stage of erosion and acute ulceration,it seems unlikely that such lesions, when multipleand part of an acute erosive gastritis, commonlyprecede the development of one or more chroniculcers.The figures given in this paper are based on an
analysis of 944 partial gastrectomy specimens re-moved for peptic ulceration. In comparing thesefigures with those of previous workers it must beremembered that gastric resection is now one ofthe commonest operations performed by thegeneral surgeon, whilst at the time when most ofthe authoritative papers on this subject werewritten it was usually only undertaken as a lastresort.Of the 944 specimens examined, 523 were
removed for duodenal ulceration and 421 forgastric ulceration. In eight of the specimens therewas evidence of both duodenal and gastric ulcera-tion. In three of these both the gastric and duo-denal ulcers were active, in two the gastric ulcers
were active and the duodenal represented bypuckered scars and in three the duodenal ulcerswere active and the gastric represented by healedpuckered scars. Thus 1.5 per cent. of chronicduodenal and 2.5 per cent. of chronic gastric ulcerswere accompanied by evidence of chronic ulcera-tion of the other organ. These figures are con-siderably lower than Stewart's (Hurst and Stewart,1929), but his figures were based on an analysisof 4,00o autopsies and showed that 9 per cent. ofchronic duodenal and 12 per cent. of chronicgastric ulcers were accompanied by chronic lesionsof the other organ. These figures are much morelikely to give a true figure of the frequency ofassociation of lesions in the two organs. Whilst insurgical material some duodenum is frequentlyincluded, this is not always the case and someduodenal lesions are bound to be missed.
Chronic Gastric UlcerSex Incidence and AgeOf the 42I gastrectomy specimens showing
chronic gastric ulcers, 322 were from males and99 from females, giving a ratio of 3.2 : I. This is avery different figure from that given by Hurst and
by copyright. on January 16, 2022 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.341.131 on 1 March 1954. D
ownloaded from

132 POSTGRADUATE MEDICAL JOURNAL March I954
Stewart in 1929. They investigated the sex in-cidence of chronic peptic ulcer in 9,000 autopsiesand their figures for the incidence of chronicgastric ulcer were 2.0 per cent. males and 2.6 percent. females, giving a ratio of o.8: I. Yet thewriter's figures are almost identical with thosegiven in a recent paper by Swynnerton and Tanner(1953), who report the results of a clinical in-vestigation of 498 patients with chronic gastriculcer These authors give a sex incidence of 3.5males to one female and state that the reason forthe rise in the male figure is the great reduction inthe incidence of gastric ulcer in young women.The age at which patients with chronic gastric
ulcer came to operation is shown in Table i.
TABLE ICHRONIC GASTRIC ULCERS: AGE AT WHICH PATIENTS
CAME TO OPERATIONMen Women
AgeGroup No. Per cent. No. Per cent.
20- 6 1.8 I 1.030- 28 8.7 6 6.o40- 89 27.6 33 33.350- 124 38.5 23 23.36o- 63 19.6 30 30.370- Io 3.2 6 6.08o- 2 0.6
Total 322 99
It will be seen that the peak period at whichmen come to operation is in the 50 to 6o agegroup, but that in women there are two peakswith almost identical figures, the first in the 40to 50 age group and the second in the 60 to 70.Number
Chronic gastric ulcers are almost always single.In the present series 28 specimens (6.6 per cent.)showed two or more active chronic ulcers, in onespecimen there being as many as five and in twofour chronic ulcers. In addition, six specimens(1.4 per cent.) showed an active chronic ulcer withthe scar of a healed ulcer, and one specimen (0.2per cent.) showed two scars of healed ulcers. In8.2 per cent. of the specimens removed for gastriculceration, therefore, there was evidence of two ormore chronic ulcers either active or healed. Hurstand Stewart's figures for multiple chronic lesionsin autopsy material are I2.6 per cent. and in partialgastrectomy specimens 6.6 per cent.
PositionTable 2 shows the distance between the lower
edge of chronic gastric ulcers and the pylorus inthe 421 specimens investigated.
TABLE 2DISTANCE BETWEEN LOWER EDGE OF CHRONIC GASTRIC
ULCERS AND THE PYLORUS
Men WomenSite
No. Per cent. No. Per cent.
o -2.5 cms. .. Io 32.5 21 20.82.5-5.o cms. .. 46 13.6 4 4.05.o-7.5 cms. .. 87 25.7 21 20.87.5-0o.o cms. .. 55 6.3 26 25.7More than io cms.from pylorus .. 40 I.8 29 28.7
Total .. .. 338 101
NoTE.-g-pecimens showing multiple ulcers have beenincluded in this table.
There is a striking difference between the twosexes. In women 54.4 per cent. of chronic ulcersoccur over 7.5 cm. from the pylorus and 28.7 percent. are over Io.o cm. away. It will be noted,also, that 20.8 per cent. of chronic ulcers occur inthe pyloric canal and antrum. In men there is amuch more even distribution from the pylorus upthe lesser curvature, but the most frequent siteis the pyloric canal and antrum.The extraordinary preponderance of chronic
gastric ulcers high up on the lesser curvature inwomen is supported by clinical observation, thewriter's figures being very similar to those ofSwynnerton and Tanner (1953). The latter, how-ever, found that chronic ulcers in the pyloric canaland antrum were very rare in women, their figurebeing o.8 per cent. The figure of 32.6 per cent.for the frequency of chronic ulcers at the same sitein men is also nearly three times as high as thosegiven by Swynnerton and Tanner. A possibleexplanation for this discrepancy could be thatduodenal ulcers very near the pylorus have beenincluded in the present series as gastric ulcers, buta re-examination has shown that, in the majorityof cases, there is clearly pyloric mucosa on eitherside of the ulcers, sections of which are alwaystaken along the axis of the lesser curvature. It isno exaggeration to say that it is unknown for aduodenal ulcer to extend beyond the pylorus intothe stomach and vice versa.The topographical distribution of chronic gastric
ulcers is seen in Table 3.In both sexes the majority are found along the
lesser curvature and are usually saddle-shaped,with part of the ulcer on the anterior wall and parton the posterior. Only those ulcers clearly entirelyon the anterior or posterior wall have been sodesignated. In this respect it is nearly always im-possible to define ulcers in the pyloric canal andantrum. In this series no chronic ulcers occurredat the cardia, in the fundus or on the greater
by copyright. on January 16, 2022 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.341.131 on 1 March 1954. D
ownloaded from

March 1954 MAGNUS: The Pathology oj Peptic Ulceration
TABLE 3TOPOGRAPHICAL DISTRIBUTION OF CHRONIC
GASTRIC ULCERS
Men WomenSite
No. Per cent. No. Per cent.
Pyloric Canal andAntrum .. 1o 32.5 21 20.8
Lesser Curvature 176 52.1 66 65.3Anterior Wall .. 7 2.I 4 4.oPosterior Wall .. 45 13.3 10 9-9Total .. .. 338 I I
curvature. It can be seen from Table 3 that ineither sex it is rare for a chronic gastric ulcer tooccur on the anterior wall away from the lessercurvature.
Chronic Duodenal UlcerSex Incidence and AgeOf the 523 gastrectomy specimens removed for
duodenal ulceration, 438 were from males and 85from females, giving a ratio of 5.1: I. Thisfigure is very similar to that given by variousauthorities in the past.- Bockus (I946), in a reviewof 786 cases of duodenal ulcer, found an incidenceof 636 males and i50 females, giving a ratio of4.2: I.The age at which patients with duodenal ulcera-
tion came to operation is shown in Table 4.TABLE 4
DUODENAL ULCERATION: AGE AT WHICH PATIENTSCAME TO OPERATION
Men WomenAgeGroup No. Per cent. No. Per cent.
20 .. 24 5.530- .. 88 20.1 19 22.340- .. 149 34.I 26 30.650- .. 123 28.0 25 29.46o- 45 10.3 13 I5.370- .. 8 I.8 1.280- .. I 0.2 I 1.2
Total .. 438 85
From this it can be seen that the peak period forboth sexes is the 40 to 50 age group.Number
In contradistinction to the stomach it is com-mon, in the duodenum, to find two chronic ulcers,one on the anterior wall, and the other on theposterior. In surgical material duodenal ulcers arefrequently left behind, so that, in the presentseries, it is not possible to give any accurate figures.Stewart (Hurst and Stewart, 1929) gives a figure,
based on autopsy material, of 17.6 per cent. for thefrequency with which double chronic ulcers arefound.
PositionDuodenal ulcers are confined to the first part of
the duodenum and almost invariably arise from theanterior or posterior wall or both. Occasionally aposterior wall ulcer will partially encircle theduodenum, thereby involving the lateral walls.Duodenal ulcers and scars are equally common onthe anterior and posterior walls. In Stewart's(Hurst and Stewart, I929) series nearly half thecases showed a lesion in both situations. In aseries of 230 cases of duodenal ulcer, active orhealed, 64 were anterior, 62 posterior and in I04cases there was a double lesion. Duodenal ulcersmay be situated very close to the pylorus, althoughmost frequently they are I to 2 cm. away from it.
Morbid Anatomy of Chronic Gastric andDuodenal UlcersThe size of the chronic gastric ulcers in the
present series is shown in Table 5.TABLE 5
SIZE OF CHRONIC GASTRIC ULCERS IN 403PARTIAL GASTRECTOMY SPECIMENS
Greatest Diameter Chronic Gastric Ulcers
Under I.o cm. .. 1451-2 cms. .. 1412-3 cms. .. 673-4 cms. .. 244-5 cms. .. 15-6 cms. .. 66-7 cms. .. 37-8 cms. .. 3Over 8 cms. .. 3
The largest number fall into the under i cm. group.As many chronic gastric ulcers are prepyloric andmany are of this size, it must be very difficult todemonstrate their presence by radiology or gastro-scopy. It is possible, therefore, that a considerablenumber of these cases are thought to have duo-denal ulcers. This may be the explanation for thediscrepancy in the figures for the frequency of pre-pyloric ulcers seen in surgically removed specimensand those diagnosed on radiology and gastroscopyalone.
In the duodenum chronic ulcers on the posteriorwall tend to be considerably larger than those onthe anterior wall. The explanation for this is thatthose on the anterior wall that reach any size arelikely to perforate.Most chronic peptic ulcers have a rounded or
oval orifice to the ulcer. crater, which, typically, isflask-shaped with overhanging margins, but there
by copyright. on January 16, 2022 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.341.131 on 1 March 1954. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
is much variation. The size of the crater orificemay, therefore, be very misleading in relation tothe size of the ulcer. In the stomach ulcers on thelesser curvature are usually elongated because theystraddle the lesser curvature with their long axis atright angles to it.
Chronic peptic ulcers completely penetrate themuscle coat which is replaced by granulationtissue in which the amount of fibrosis depends onthe age of the ulcer. The muscle coat ends in theouter wall, and, in well-established ulcers, thefibres splay out and sweep upwards to mingle withthe muscularis mucosae in a very characteristicmanner. The floor of an active peptic ulcer iscovered by a thin slough which is usually firmlyadherent. Chronic gastric ulcers on the posteriorwall of the stomach frequently penetrate the under-lying pancreas, which becomes part of the ulcerfloor. Those on the anterior wall may becomeadherent to the left lobe of the liver, but this isnot common. Chronic duodenal ulcers on theposterior wall nearly always involve the head ofthe pancreas.The peritoneal surface of a chronic gastric ulcer
shows thickening of the serosa, which is whitish incolour and opaque. Fibrous adhesions may bepresent to adjacent structures. Not infrequently,in association with a chronic gastric ulcer, thelymph nodes along the lesser and greater curva-tures may be enlarged, firm and even whitish incolour from a marked degree of reactive hyper-plasia. This appearance may mislead the surgeoninto thinking that metastases are present and thathe is dealing with a gastric carcinoma.
In the technique used in the investigation of thespecimens in the series considered in this paper allulcers, whatever their size, have been sectionedwhole, the piece of tissue always being takenthrough the ulcer along the cardiac-pyloric axis.In the writer's experience chronic gastric ulcersnever occur in body mucosa, no matter where theyare situated. Sometimes, in high ulcers, bodymucosa is present at the upper edge of the ulcer,but the mucosa at the lower edge is invariablypyloric in type. The distribution of the pyloricmucosa in the stomach is extremely variable and,on occasion, it may extend along the lesser curva-ture almost to the cardia. Chronic gastric ulcerswhich are found high up on the lesser curvaturemay arise at the junction of the pyloric with thebody mucosa, although frequently sections willshow them completely surrounded by pyloricmucosa.
In the ulcer floor of a typical active chronicpeptic ulcer a section shows clearly the four distinctzones originally described by Askanazy (1920-24).First, there is a layer of purulent or fibrino-purulent exudate which is easily detached from
the underlying necrotic zone. The latter is narrowbut well defined and usually intensely acidophilic.It is a zone of fibroid necrosis and is usuallystructureless. The granulation tissue zone comesnext. It is of variable width and passes imper-ceptibly into the fourth or fibrous zone. It isinfiltrated by a varying number of chronic in-flammatory cells. The fibrous zone is composed ofdense fibrous tissue and fills the gap formed bythe penetration of the muscle coat. It containsvessels, nerves and frequently foci of lymphoidtissue. The smaller arteries show a varying degreeof obliterative endarteritis and some of the veinsmay be thrombosed.At the edges of a chronic ulcer the mucosa may
terminate abruptly or overhang. The muscularismucosae is usually thickened and extends right upto the wall of the crater. The submucosa isthickened and fibrotic. The muscle coat endsabruptly in the walls of the ulcer and, in ulcers ofsome chronicity, the muscle fibres are splayed outand sweep upwards to merge with the muscularismucosae.The early signs of healing of a chronic peptic
ulcer are the slow disappearance of the acute in-flammatory reaction in the tissues surrounding itwith progressive reduction in tissue oedema. Atthe same time the ulcer floor starts to be cleanedup with a separation of slough and fibrino-purulentexudate. The collagen fibres in the fibrous zoneof the ulcer floor contract more and more, therebygreatly reducing the size of the ulcer and the areato be re-epithelialized. New formed epitheliumcommences to grow inwards from the ulcer mar-gins over the healthy granulation tissue now lyingin the ulcer floor and the whole area eventuallybecomes epithelialized. At first the covering epi-thelium is thin and pinkish in colour, but it soonincreases in thickness by the formation of simpletubular glands. Even after the ulcer floor is com-pletely covered with epithelium contraction of thefibrous tissue in the floor continues, ending inthe formation of a puckered scar which may be amere fraction of the size of the original ulcer. Thebreach in the muscle coat is never restored bymuscle, but is filled by dense fibrous tissue,remaining as a permanent scar in the stomach wall.
The Pathology of Ulcer-CancerFor the last hundred years the pendulum has
swung one way and then the other with regard tothe frequency with which a chronic gastric ulcerundergoes malignant change. The peak of theswing towards a high frequency of ulcer-cancerwas reached in 1910, when Wilson and McCarthypublished a paper claiming that 71 per cent. of I53cases of gastric cancer showed histological evidencethat the cancer had arisen in a pre-existing gastric
March 1954134by copyright.
on January 16, 2022 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.341.131 on 1 M
arch 1954. Dow
nloaded from

March 1954 MAGNUS: The Pathology of Peptic Ulceration35
ulcer. These findings were not confirmed by sub-sequent investigators, who showed that epithelialhyperplasia at the edges of chronic gastric ulcersand its distortion by fibrosis could easily be mis-taken for evidence of early malignant change.Between 1925 and I935 the problem was mostcarefully investigated by Stewart (Hurst andStewart, 1929), Dible (I925) and Newcomb(I932-33). These three workers all applied thesame strict histological criteria to the diagnosis ofulcer-cancer and their figures were very differentfrom those of Wilson and McCarthy. Stewartfound cancer in the margins of i out of I8ochronic ulcers investigated, an incidence of 6.1 percent. Dible investigated 33 cases of gastric cancerand found that in two cases, i.e. 6 per cent., thecancer had arisen in a gastric ulcer. Newcombfound that 3.75 per cent. of the chronic gastriculcers he investigated showed evidence of cancerin their margins.The present position in this country would seem
to be that, whilst most pathologists believe thatabout 5 per cent. of chronic gastric ulcers undergomalignant change, many clinicians have swung tothe opposite extreme and doubt if a chronic gastriculcer ever becomes malignant. In America, how-ever, most clinicians believe that at least io percent. of chronic gastric ulcers eventually becomemalignant. To the writer it seems rather likeburying one's head in the sand to state that achronic gastric ulcer never becomes malignant andthat all such lesions can be explained on the basisof an excavating primary carcinoma. Chronicindolent ulcers in other parts of the body occasion-ally become malignant and there is no reason whythis should not happen in the stomach.The histological criteria to be strictly applied
before the diagnosis of ulcer-cancer. can be estab-lished are twofold. Firstly, there must be definite
evidence of a pre-existing chronic gastric ulcerand, secondly, there must be irrefutable evidencethat malignant change has occurred at the edgesof the ulcer. In the present series of cases thefour histological criteria laid down by Newcomb(1932-33) as being necessary for the diagnosis of apre-existing chronic gastric ulcer have beenfollowed. These criteria are:
I. Complete destruction of an area of musclecorresponding in size roughly to the floor of theulcer.
2. The presence of a large area of dense fibrosisand granulation tissue in the floor of the lesion.
3. The presence of endarteritis obliterans andthrombophlebitis in the vessels around.
4. Fusion or close approximation of the mus-cularis mucosae and muscularis at the margin ofthe ulcer.The final criterion of malignant change is the
occurrence of metastases which were present in themajority of the cases to be considered. When agastric ulcer becomes malignant the process com-mences in the margin of the ulcer and spreadsslowly round the ulcer, the cancer cells also in-filtrating the muscle lying in the ulcer wall. Theinfiltration does not extend into the ulcer flooruntil a very late stage and it was not present in anyof the cases to be described. It is difficult to thinkof a primary ulcerating carcinoma in which not asingle cancer cell remains in the whole ulcer floor.Applying the above criteria to the present series,
eight cases were found to be ulcer-cancers, anincidence of 1.9 per cent. It must be rememberedthat we are only dealing with partial gastrectomyspecimens, so that the figure for the incidence ofulcer-cancer could be expected to be considerablylower for chronic gastric ulcers as a whole.The salient features of the eight cases of ulcer-
cancer are summarized in Table 6.
TABLE 6EIGHT CASES OF ULCER-CANCER
Length ofAge Sex History Site Size of Ulcer Fate
43 F 3 years Prepyloric 4.0 cms. Died from metastases i year after operation52 M 4 years io cms. from pylorus
on lesser curvature 1.5 cms. Died from metastases 3* years after operation35 F i year Prepyloric 2.0 cms. Metastases in lymph nodes. i year after opera-
tion alive and well38 M 7 years Prepyloric 3.0 cms. Died from metastases 2j years after operation38 M 5 years 2 cms. from pylorus 2.0 cms. No metastases in regional lymph nodes. Died
2 years after operation from cerebral hae-morrhage. No post mortem
46 M 20 years 3 cms. from pylorus 3.0 cms. Metastases in lymph nodes. Last seen 5 yearsafter operation-lost much weight, believedto have metastases
64 M 4 years Prepyloric 3.0 cms. Died from metastases i year after operation40 M 2 years Prepyloric 1.0 cm. No metastases in lymph nodes. Alive and well
8 months after operation
by copyright. on January 16, 2022 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.341.131 on 1 March 1954. D
ownloaded from

136 POSTGRADUATE MEDICAL JOURNAL March I954
It will be seen that three of the cases wereunder forty and two under forty-five. Except forone case, the length of history was measured inyears. Seven of the eight ulcer-cancers occurred inthe pyloric antrum, thus confirming that it is thechronic ulcer in this situation which is particularlyliable to undergo malignant change. Five of thepatients are dead, one was dying when last seenand two are still alive and well, but these wereoperated on within the last i8 months.From the present series, therefore, it may be
concluded that it is rare for a chronic gastriculcer to undergo malignant change, but that it does
occur there can be no doubt. The prognosis isextremely bad.
BIBLIOGRAPHYASKANAZY M. (1920), Rev. mdd. de la Suisse Romande, 40, 477.ASKANAZY, M. (1924), Virch. Arch., 250, 370.BOCKUS, H. L. (1946), 'Gastro-enterology,' Vol. I, p. 364.
Saunders.DIBLE, J. H. (i925), Brit. J. Surg., 12, 666.HURST, A. F., and STEWART, M. J. (I929), 'Gastric and
Duodenal Ulcer,' Oxford University Press.NEWCOMB, W. D. (1932-33), Brit. J. Surg., 20, 279.SWYNNERTON, B. F., and TANNER, N. C. (I953), Brit. med. J.,
ii, 841.WILSON, L. B., and McCARTHY, W. C. (I9I0), Amer. J. Med.
Sci., 138, 846.
THE ACUTE COMPLICATIONS OFPEPTIC ULCER AND THEIRSURGICAL TREATMENT
By A. G. R. LOWDON, O.B.E., F.R.C.S.E.From the Department of Surgery, University of Edinburgh
Perforation and haemorrhage, the acute com-plications of peptic ulcer, are of importance mainlybecause they may be the cause of death in a diseasewhich otherwise does not usually threaten the lifeof the patient; these complications are also ofspecial interest at the present time because theviews of physicians and surgeons about their treat-ment have recently changed and are, indeed, stillundetermined.
PerforationThe term ' perforation' is used to describe the
free perforation of a peptic ulcer into the peritonealcavity in distinction to the 'penetration' whichoccurs when an ulcer invades a neighbouring organsuch as the pancreas.
Perforation occurs most commonly in ulcers onthe anterior surfaces of duodenum or stomach, butoccasionally a posterior ulcer perforates freely intothe lesser sac. Perforation may also occur in agastrojejunal ulcer or in an ulcer related to Meckel'sdiverticulum, and an oesophageal peptic ulcer mayperforate into the pleural cavity. The simultaneousperforation of two ulcers has been reported.Most perforated ulcers are of a chronic type,
but the complication may occur in relatively acuteulcers which have been present for at most one ortwo weeks (Fig. I).
IncidenceBecause perforation of a peptic ulcer almost
invariably leads to admission to hospital and toaccurate diagnosis, studies of the frequency of thecomplication are comparatively reliable. In theIgth century perforation was an uncommon eventand the majority of cases occurred in young women(Brinton, I857), but a remarkable change of theincidence has occurred since the first decade ofthis century (Stewart and Winser, I942; Tidy,1945). Perforation is now relatively common andoccurs much more frequently in men--about 15men to one woman. It may occur at any age, butis rare before adolescence; it is most frequentbetween 30 and 45 years, but it is now not un-common in the aged. The perforation of an ulcerdoes not appear to be related in time to the eatingof food or to physical exertion. There is moredanger of the complication when the patient isphysically or mentally tired; the incidence ofperforation rises in the winter months, at the endof the working week and at the end of the workingday (Illingworth et al., I944; Jamieson, 1947).The Clinical Features of PerforationThe typical clinical picture of an acute perfora-
tion in a patient who gives a history of pepticulcer symptoms is easily recognized from the
by copyright. on January 16, 2022 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.341.131 on 1 March 1954. D
ownloaded from








![BMC Microbiology BioMed Central - core.ac.uk · mucosa of a patient with gastritis and peptic ulceration by Marshall and Warren in 1982 [1]. It is an important human pathogen, responsible](https://img.pdfslide.net/doc/110x75/5ceaa81388c9933e668d0daa/bmc-microbiology-biomed-central-coreacuk-mucosa-of-a-patient-with-gastritis.jpg)


















