Embed Size (px)
Citation preview
Pathophysiology of Peripheral Nerve Lesions
David A. Lake, PT, PhD
Department of Physical Therapy
Armstrong Atlantic State University
Savannah, GA
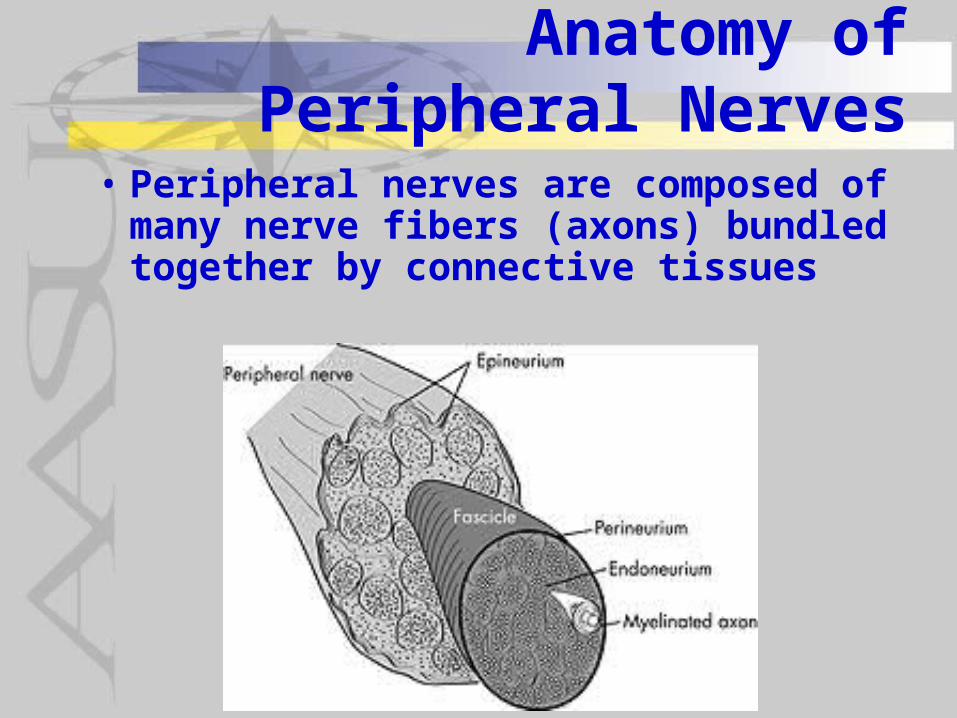
Anatomy of Peripheral Nerves
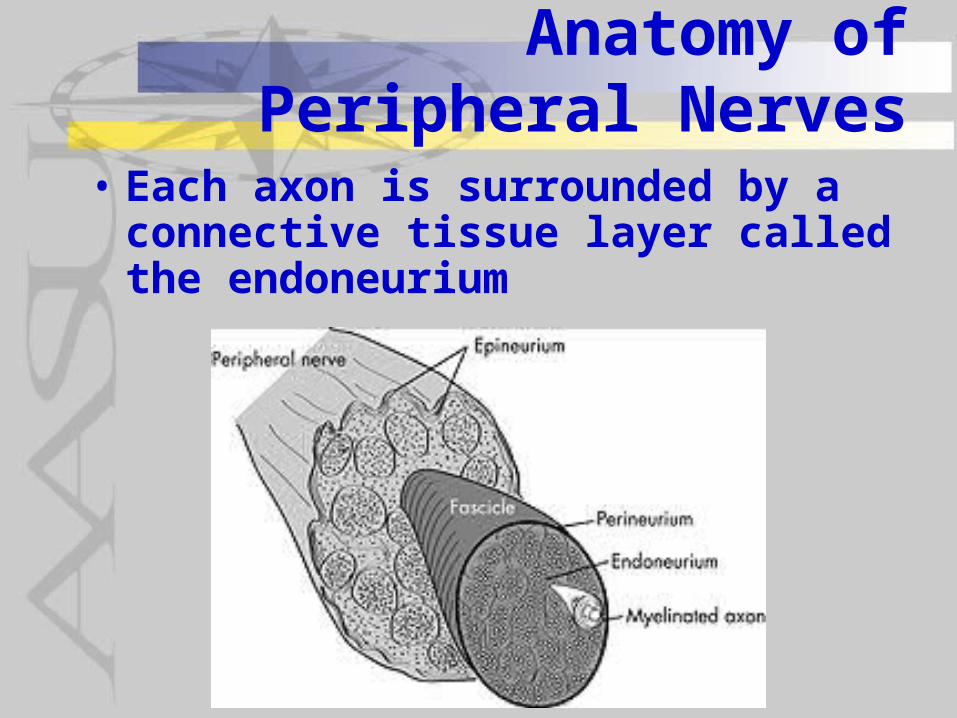
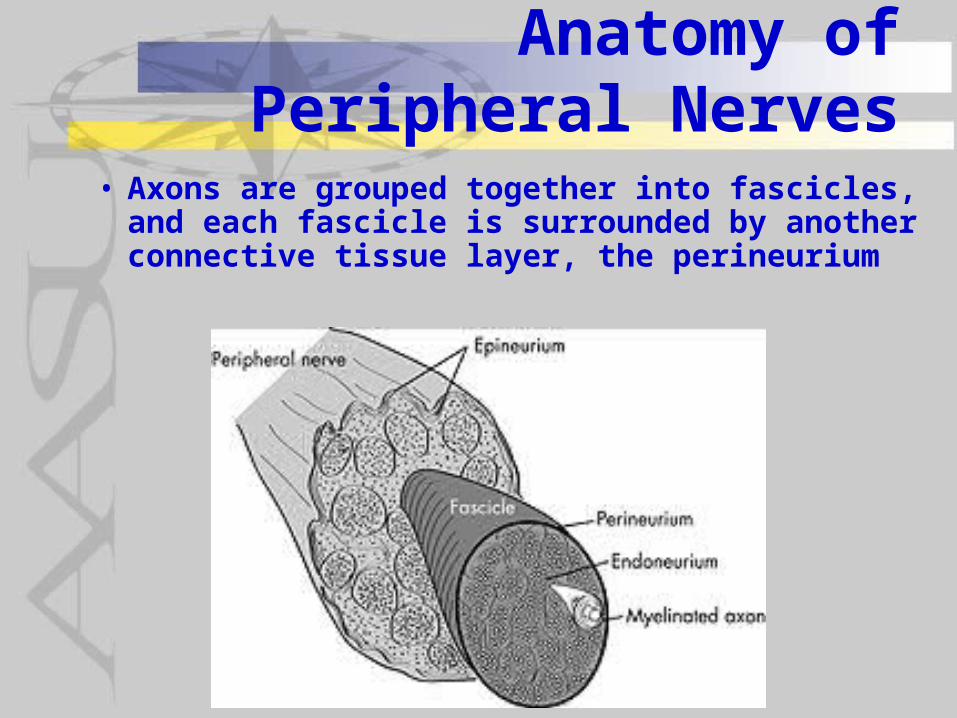
• Peripheral nerves are composed of many nerve fibers (axons) bundled together by connective tissues
Anatomy of Peripheral Nerves
• Each axon is surrounded by a connective tissue layer called the endoneurium
Anatomy of Peripheral Nerves
• Axons are grouped together into fascicles, and each fascicle is surrounded by another connective tissue layer, the perineurium

Anatomy of Peripheral Nerves
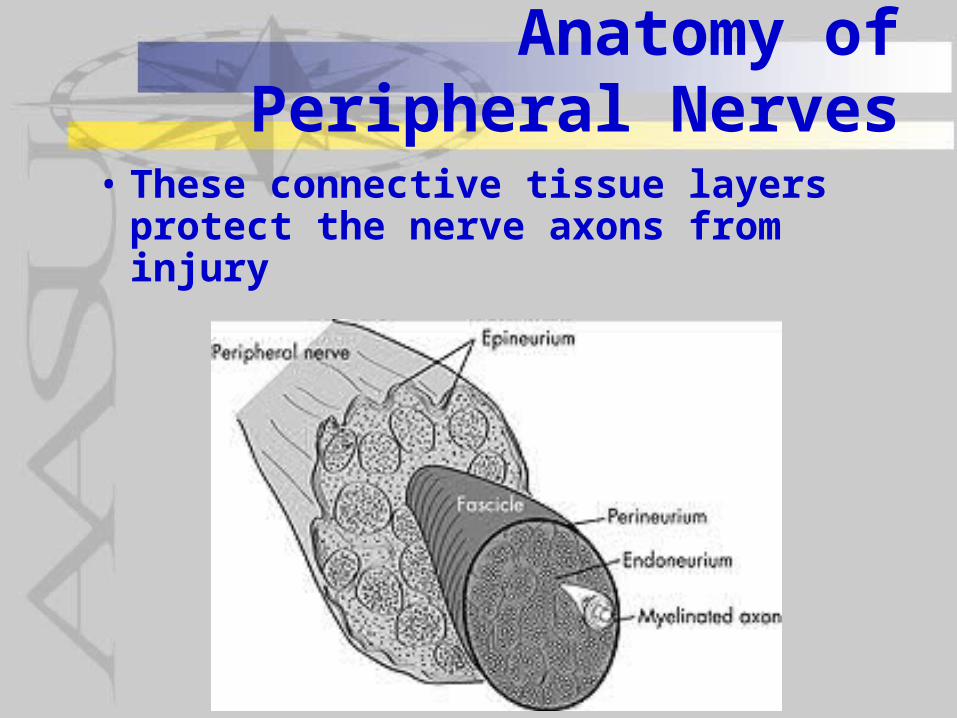
• Fascicles are grouped together, covered by an outer connective tissue layer, the epineurium, to form a peripheral nerve
Anatomy of Peripheral Nerves
• These connective tissue layers protect the nerve axons from injury
Damage to Peripheral Nerves
• Nerve injury is classified by the extent of the injury to the nerve into one of 3 classification– Neurapraxia– Axonotmesis– Neurotmesis

Damage to Peripheral Nerves
• Neurapraxia• Defined as failure of
conduction in a nerve in the absence of structural changes, due to compression or ischemia
• Lack of conduction through the area of compression but conduction above and below the compression
• Return of function normally ensues.
Damage to Peripheral Nerves
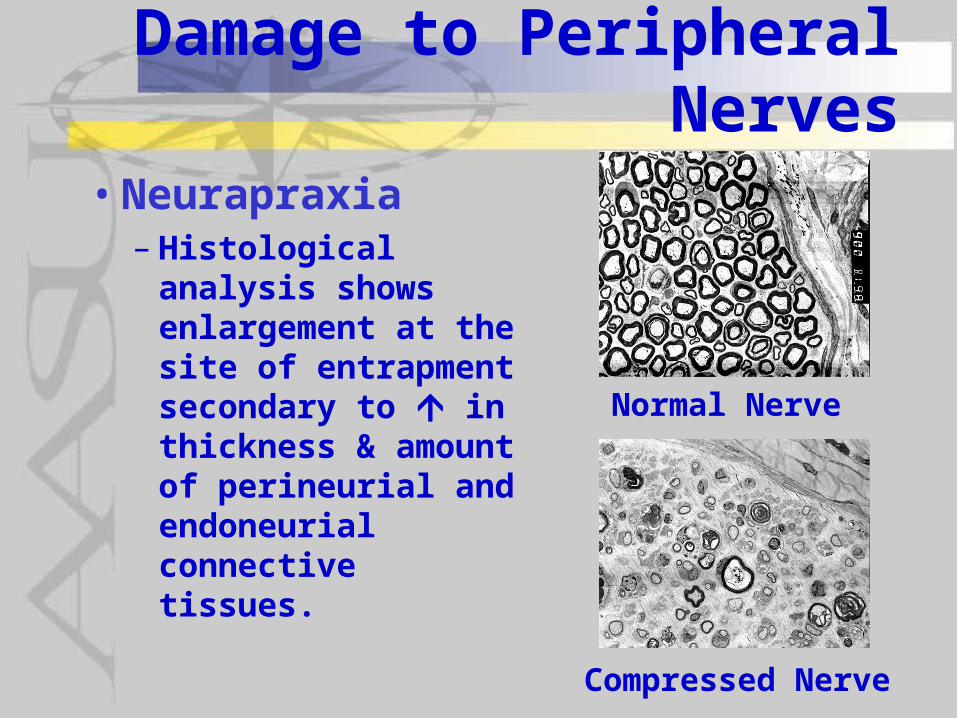
• Neurapraxia– Histological
analysis shows enlargement at the site of entrapment secondary to in thickness & amount of perineurial and endoneurial connective tissues.
Normal Nerve
Compressed Nerve
Damage to Peripheral Nerves
• Neurapraxia– Occasionally compression can result in
only slowed conduction through the region due to widened nodal regions (formerly referred to as axonostenosis)
– Sites of slowing often just distal & proximal to the site of compression
– Symptoms of compression (pain, numbness & paraesthesias) are more common and more intense when compression is combined with peripheral ischemia

Damage to Peripheral Nerves
• Neurapraxia– Characteristics more associated with
the degree of compression include:
• Amount of Action Potential slowing
• Decrease in sensory evoked potentials and sensory NCV.
• Numbness
• Amount of muscle denervation
• Muscle weakness & wasting
Damage to Peripheral Nerves
• Neurapraxia– Characteristics more associated with
ischemia include:
• Acute pain
• paraesthesias - particularly those of intermittent character
Damage to Peripheral Nerves
• Neurapraxia– Pain may be the result of direct irritation
of the abnormal spectrum of surviving nerve fibers (small > survival than large)
– Paraesthesias may result from spontaneous activity in the entrapped fibers resulting from ischemia
Damage to Peripheral Nerves
• Neurapraxia - Levels of Severity– Pre-symptomatic - in perineural and
endoneural microvasculature– Minimal - perineurial and epineurial
fibrosis without changes in the nerve fibers
– Moderate - thinning of myelin in large myelinated fibers
– Severe - change in distribution of fiber sizes with dramatic in large myelinated fibers and proportional in small unmyelinated fibers
Damage to Peripheral Nerves
• Axonotmesis– Nerve injury
characterized by: • Disruption of the
axon and myelin sheath distal to crush
• Preservation of the endoneurium, perineurium & epineurium

Damage to Peripheral Nerves
• Axonotmesis– Conduction block occurs immediately
across the site of injury
– Followed by irreversible loss of excitability of the nerve impulse beginning at the neuromuscular junction and then spreads proximally over the length of the distal segment
– Little change in the proximal segment at least initially
Damage to Peripheral Nerves
• Axonotmesis– Initially, conduction testing proximal to
injury cannot distinguish between neuropraxia & axonotmesis
– Once Wallerian degeneration completes its process, proximal nerve conduction velocity can be expected to be decreased by 30-40% of normal.
Damage to Peripheral Nerves
• Axonotmesis– Wallerian degeneration results and
takes 3-5 days– Degeneration lasts for several days
prior to any regenerative activity in the distal ends of the damaged nerve
– Regeneration occurs at a rate of 1 mm/day on average assuming normal oxygen tissue tensions
– Generally the prognosis for recovery is good
Damage to Peripheral Nerves
• Wallerian Degeneration - characterized by:
• Axonal enlargement into an amorphorous mass
• Breakdown of the axons, and schwann cell
• Ingestion of fragmented myelin to provide clean endoneural tubes for advancement of regenerating axons

Damage to Peripheral Nerves
• Wallerian Degeneration
Damage to Peripheral Nerves
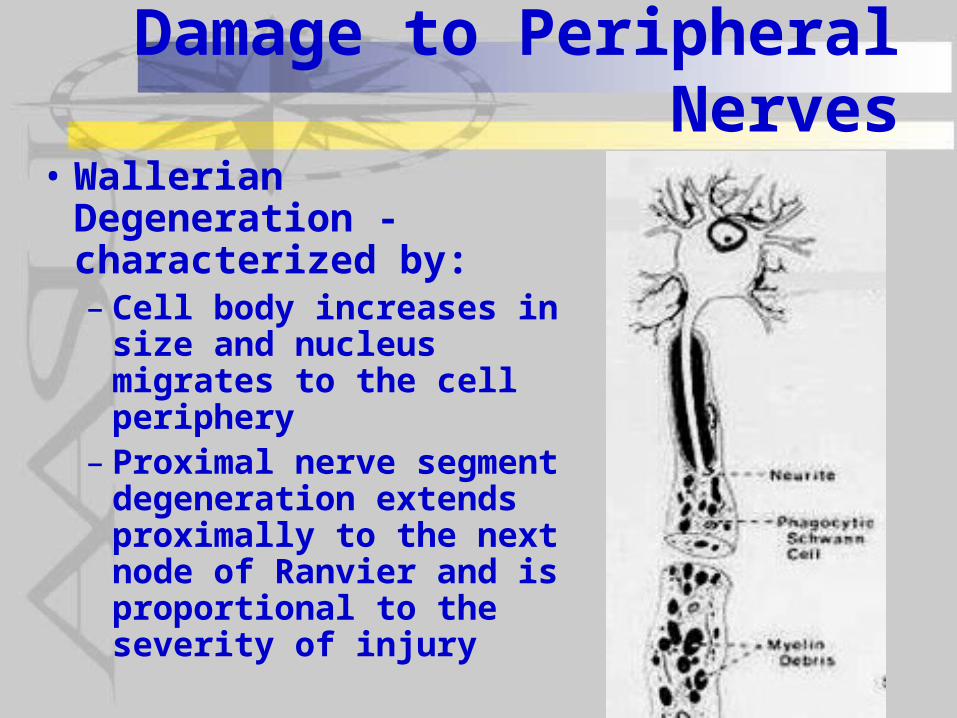
• Wallerian Degeneration - characterized by:– Cell body increases in
size and nucleus migrates to the cell periphery
– Proximal nerve segment degeneration extends proximally to the next node of Ranvier and is proportional to the severity of injury

Damage to Peripheral Nerves
• Wallerian Degeneration - characterized by:– Distal nerve segment has:
• Schwann cell proliferation • Collapse of endoneurium• Entire axonal material is
phagocytosed from the site of injury to the endplates
Damage to Peripheral Nerves
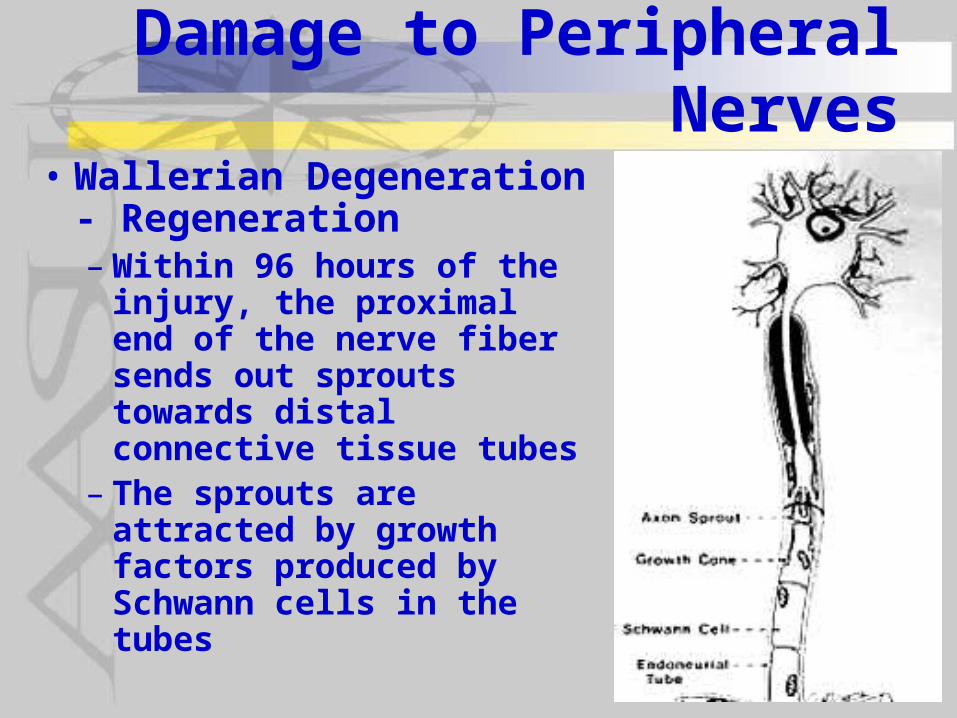
• Wallerian Degeneration - Regeneration– Within 96 hours of the
injury, the proximal end of the nerve fiber sends out sprouts towards distal connective tissue tubes
– The sprouts are attracted by growth factors produced by Schwann cells in the tubes
Damage to Peripheral Nerves
• Neurotmesis – Partial or complete
severance of a nerve– Disruption of the axon and
its myelin sheath and the connective tissue elements
– Regeneration may occur if peripheral distruption is incomplete but often the pattern and rate of regeneration in those cases amy be abnormal

Damage to Peripheral Nerves
• Neurotmesis – With complete
severance of a nerve regeneration does not occur
– If regeneration does not occur often the nerve endings bundle up to form a neuroma

Damage to Peripheral Nerves
• Cell Body Changes – Large neurons have
abundant rough endoplasmic reticulum (RER) which forms aggregates, the Nissl granules
– If the axon is transected, the RER disaggregates and neuronal cell body swells
Neuron with Transected Axon
Normal Neuron
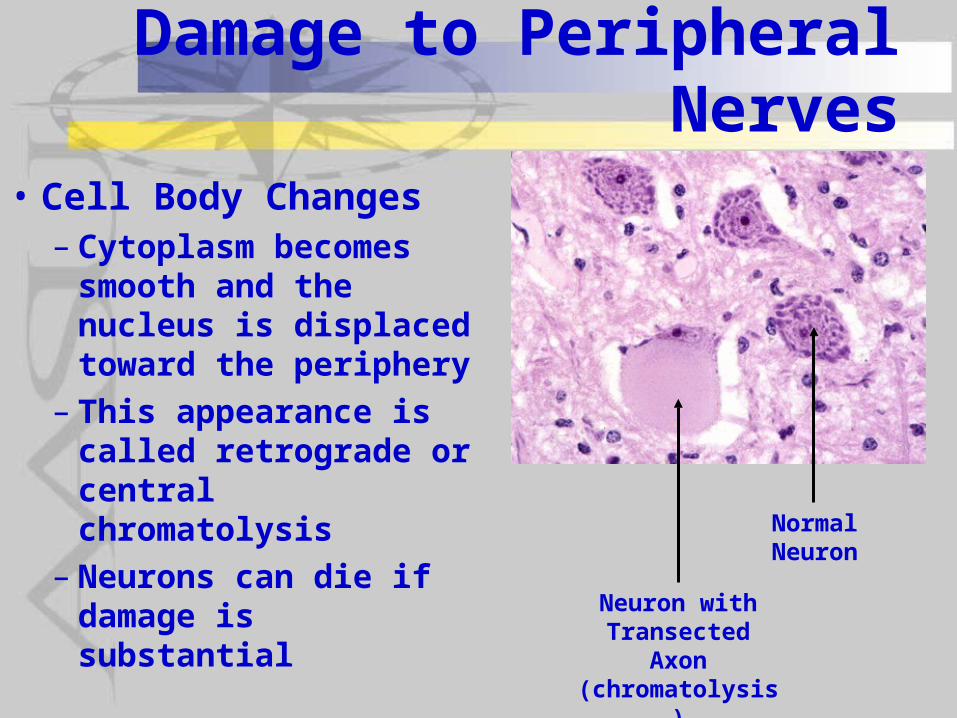
Damage to Peripheral Nerves
• Cell Body Changes – Cytoplasm becomes
smooth and the nucleus is displaced toward the periphery
– This appearance is called retrograde or central chromatolysis
– Neurons can die if damage is substantial
Neuron with Transected Axon (chromatolysis)
Normal Neuron
Radiculopathy• Damage along a peripheral nerve is
often secondary to entrapment• Entrapment can occur at particular
places along a peripheral nerve where the nerve is in a confined space where pressure can be applied
• This begins with the nerve roots and trauma to the nerve roots is called radiculopathy
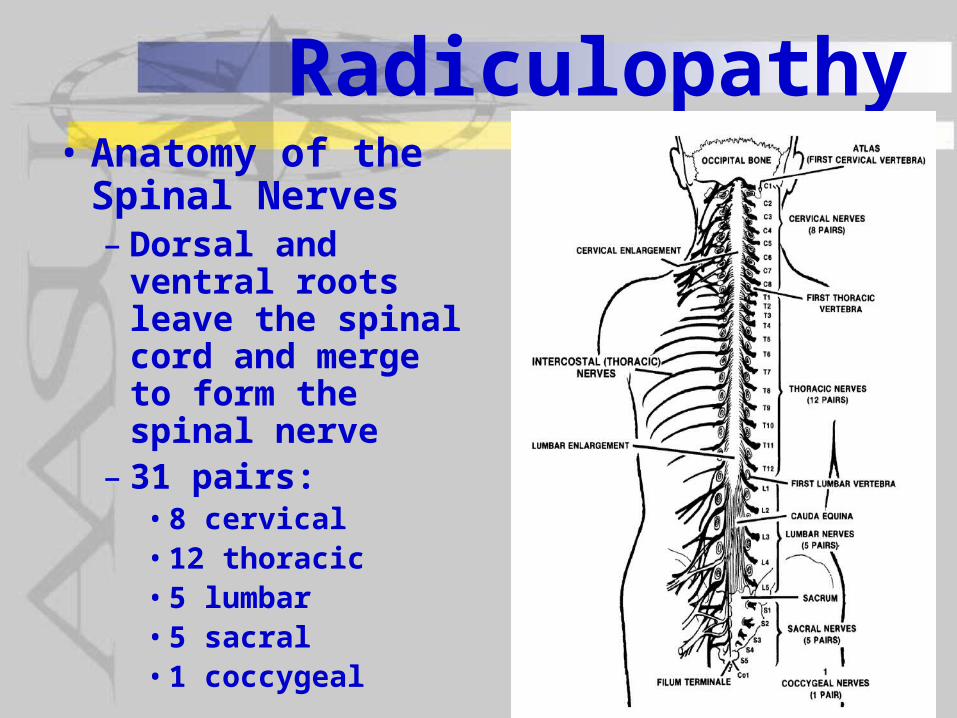
Radiculopathy• Anatomy of the
Spinal Nerves– Dorsal and ventral
roots leave the spinal cord and merge to form the spinal nerve
– 31 pairs:• 8 cervical• 12 thoracic• 5 lumbar• 5 sacral • 1 coccygeal
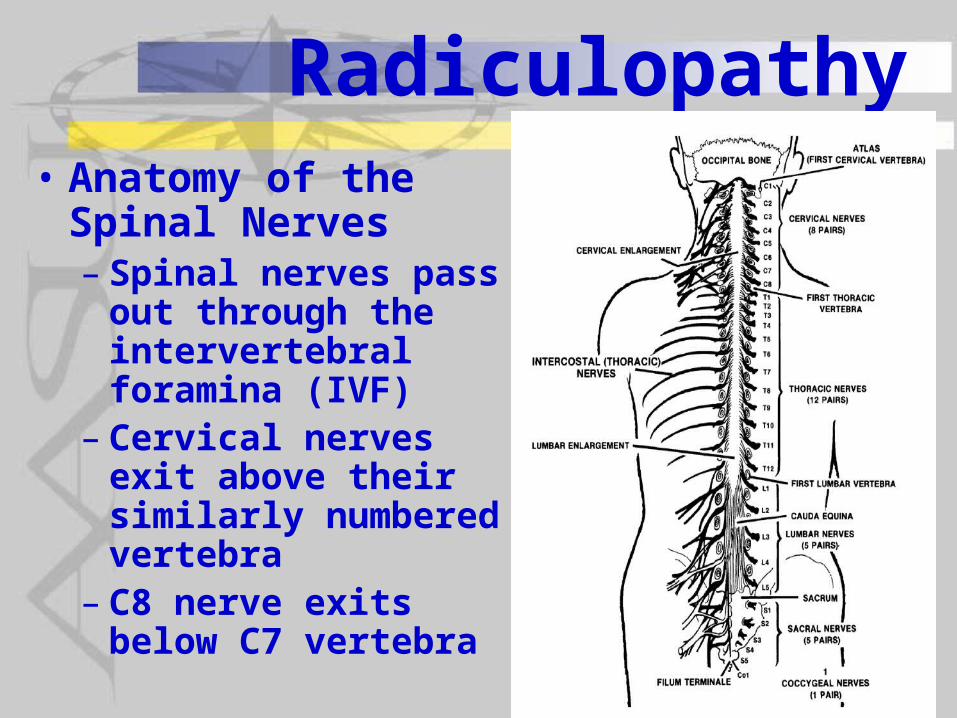
Radiculopathy• Anatomy of the
Spinal Nerves– Spinal nerves pass
out through the intervertebral foramina (IVF)
– Cervical nerves exit above their similarly numbered vertebra
– C8 nerve exits below C7 vertebra

Radiculopathy• Anatomy of the
Spinal Nerves– Thoracic & lumbar
nerves exit below their similarly numbered vertebra
– Sacral nerves exit through the sacral foramina
– Coccygeal nerves exit just lateral to the coccyx bone
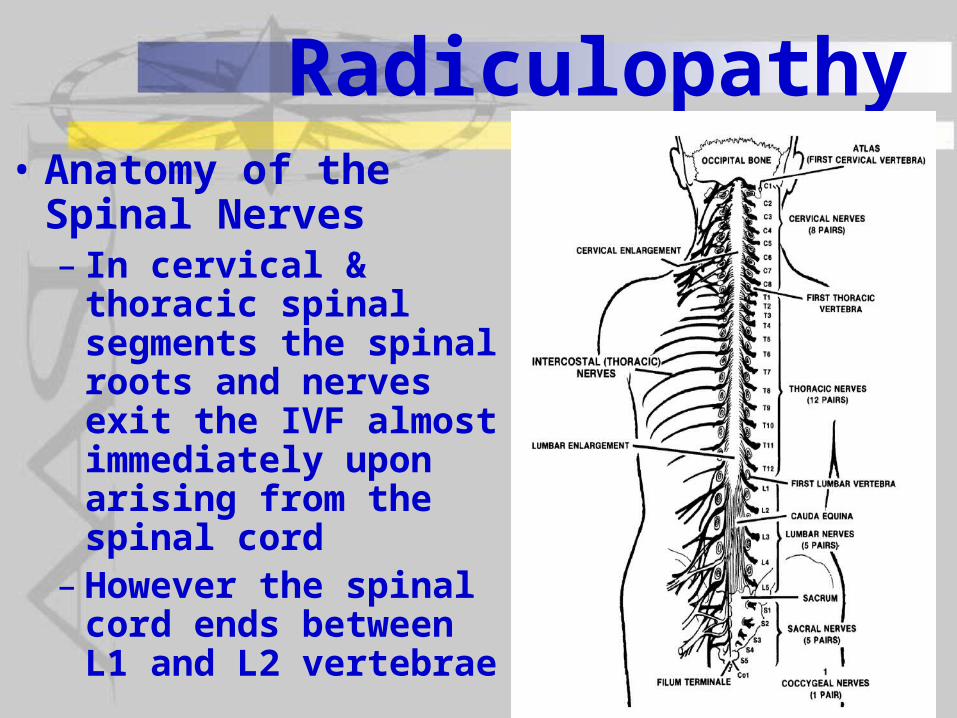
Radiculopathy• Anatomy of the Spinal
Nerves– In cervical & thoracic
spinal segments the spinal roots and nerves exit the IVF almost immediately upon arising from the spinal cord
– However the spinal cord ends between L1 and L2 vertebrae
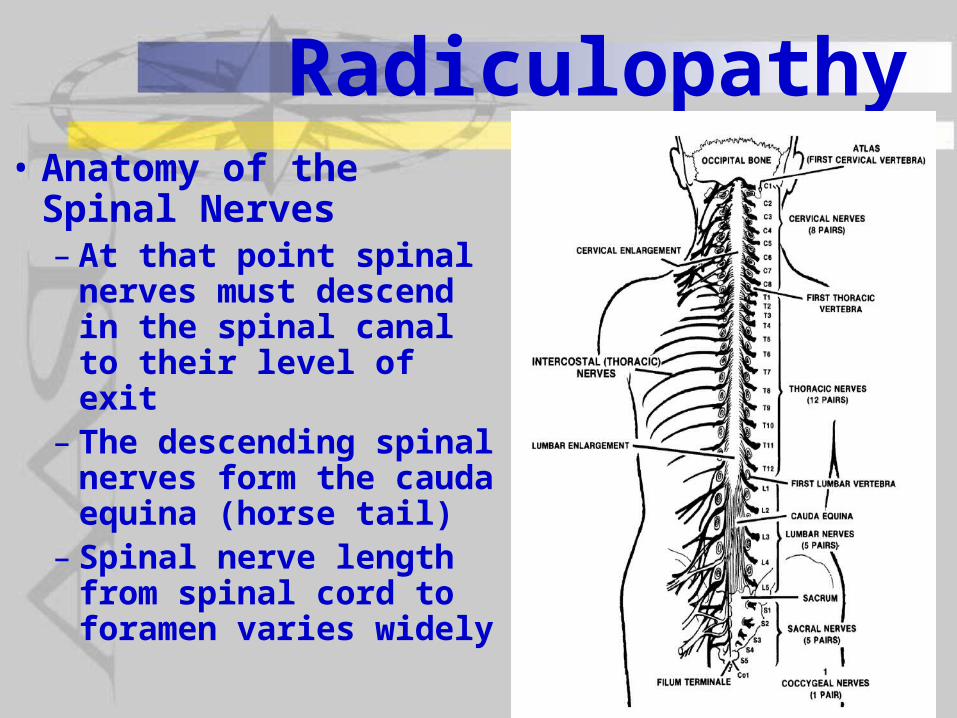
Radiculopathy• Anatomy of the Spinal
Nerves– At that point spinal
nerves must descend in the spinal canal to their level of exit
– The descending spinal nerves form the cauda equina (horse tail)
– Spinal nerve length from spinal cord to foramen varies widely
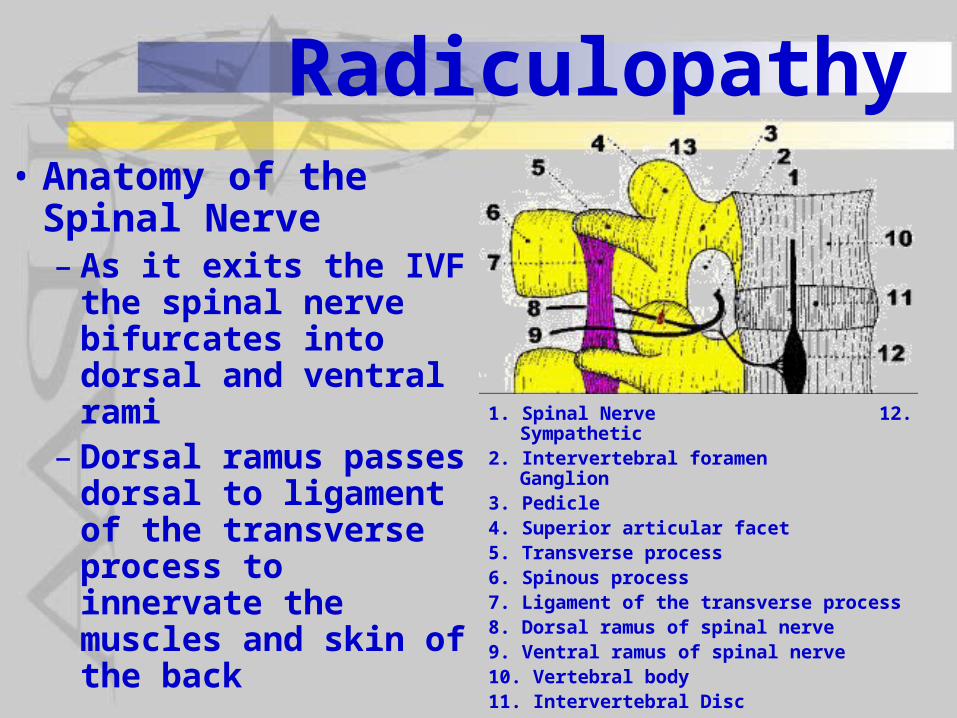
Radiculopathy• Anatomy of the
Spinal Nerve– As it exits the IVF the
spinal nerve bifurcates into dorsal and ventral rami
– Dorsal ramus passes dorsal to ligament of the transverse process to innervate the muscles and skin of the back
1. Spinal Nerve 12. Sympathetic2. Intervertebral foramen Ganglion3. Pedicle 4. Superior articular facet5. Transverse process6. Spinous process7. Ligament of the transverse process8. Dorsal ramus of spinal nerve9. Ventral ramus of spinal nerve10. Vertebral body11. Intervertebral Disc
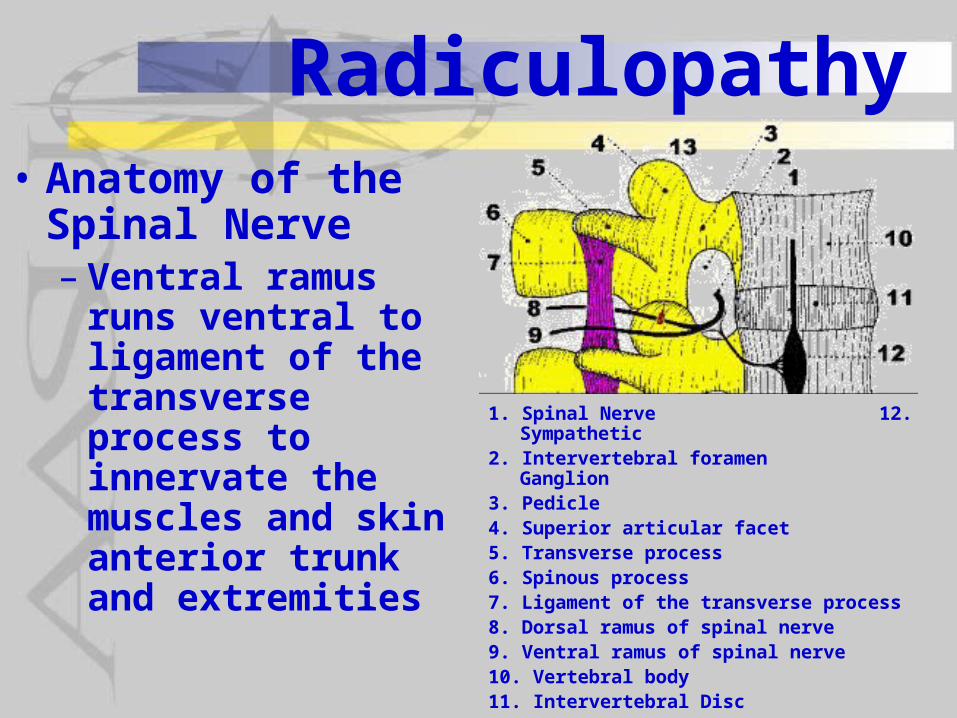
Radiculopathy• Anatomy of the
Spinal Nerve– Ventral ramus runs
ventral to ligament of the transverse process to innervate the muscles and skin anterior trunk and extremities
1. Spinal Nerve 12. Sympathetic2. Intervertebral foramen Ganglion3. Pedicle 4. Superior articular facet5. Transverse process6. Spinous process7. Ligament of the transverse process8. Dorsal ramus of spinal nerve9. Ventral ramus of spinal nerve10. Vertebral body11. Intervertebral Disc

Radiculopathy• Contents of inter-
vertebral foramen (area of picture where 1 & 2 are):– Spinal nerve– Dorsal root ganglion
when more laterally located
– Connective tissue - dural sleeve & loose areolar connective tissue
– Fat
1. Dorsal root ganglion 8. Gray matter2. Ventral root 9. White
matter3. Pia mater 10. Spinal Nerve4. Arachnoid5. Dura mater6. Dorsal root7. Subarachnoid space

Radiculopathy• Contents of inter-
vertebral foramen:– Radicular artery– Veins vertebral
foramen– Radicular artery– Veins communi -
cating between internal and external venous plexuses
– 2-4 recurrent meningeal nerve branches
Not labeled are the radicular artery & communicating veins which are the large red and smaller blue objects respectively just below 1) Dorsal root ganglion and 2) the ventral root.
Not shown are the recurrent meningeal nerves branches
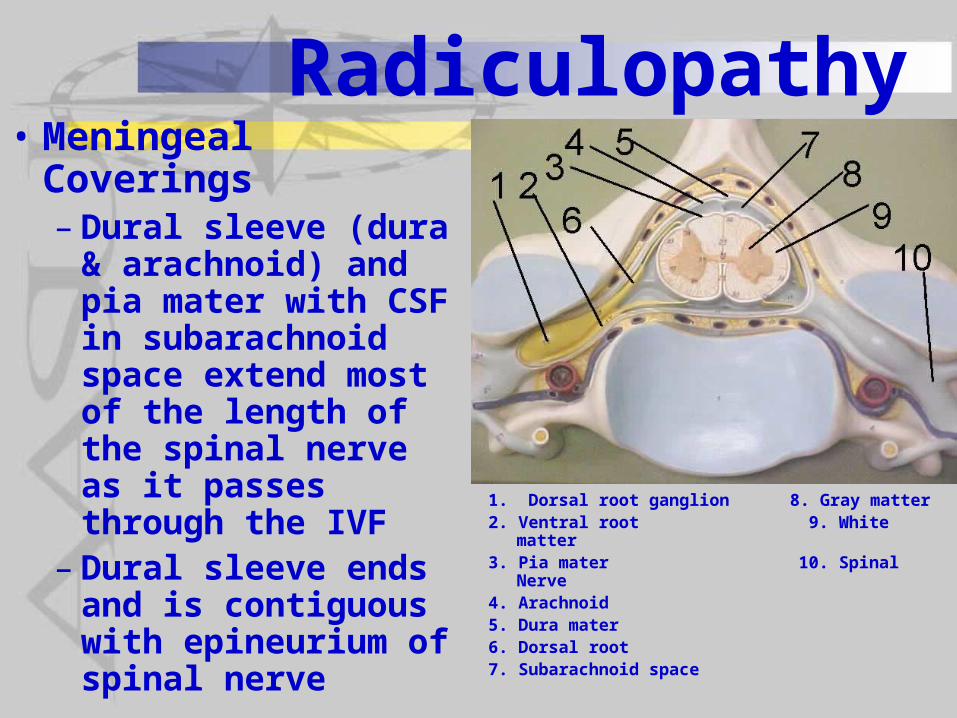
Radiculopathy• Meningeal
Coverings– Dural sleeve (dura &
arachnoid) and pia mater with CSF in subarachnoid space extend most of the length of the spinal nerve as it passes through the IVF
– Dural sleeve ends and is contiguous with epineurium of spinal nerve
1. Dorsal root ganglion 8. Gray matter2. Ventral root 9. White
matter3. Pia mater 10. Spinal Nerve4. Arachnoid5. Dura mater6. Dorsal root7. Subarachnoid space
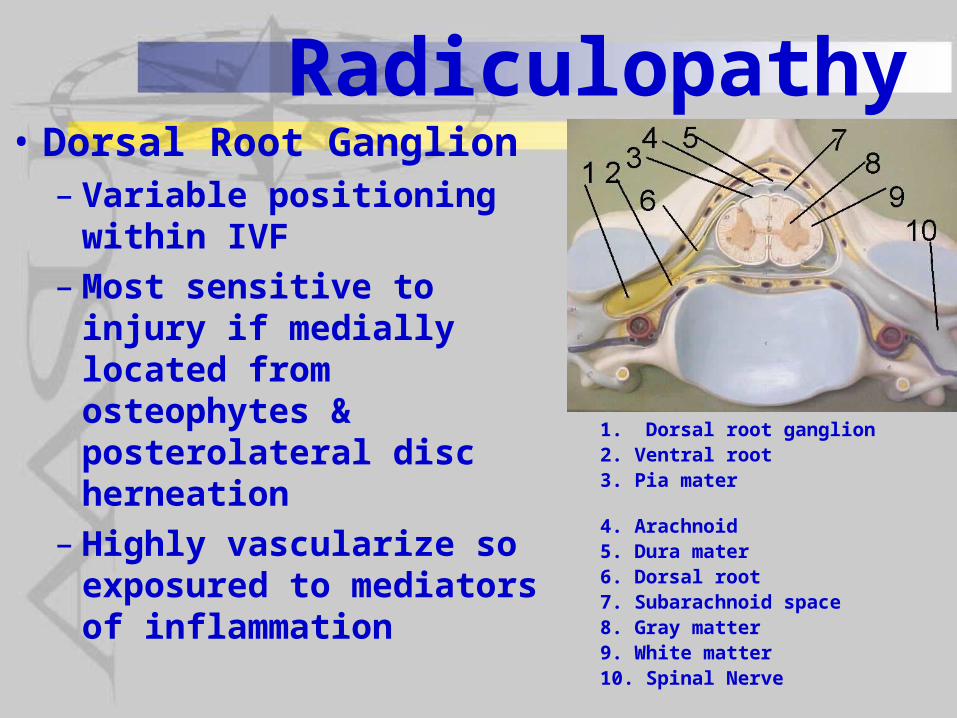
Radiculopathy• Dorsal Root Ganglion
– Variable positioning within IVF
– Most sensitive to injury if medially located from osteophytes & posterolateral disc herneation
– Highly vascularize so exposured to mediators of inflammation
1. Dorsal root ganglion2. Ventral root3. Pia mater 4. Arachnoid5. Dura mater6. Dorsal root7. Subarachnoid space8. Gray matter9. White matter10. Spinal Nerve
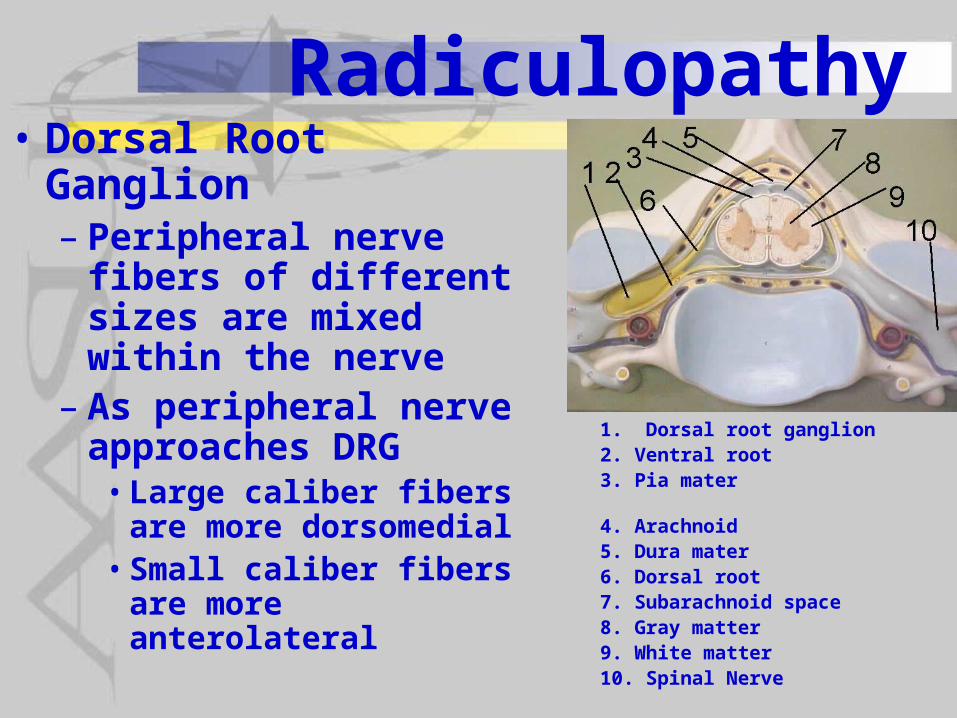
Radiculopathy• Dorsal Root Ganglion
– Peripheral nerve fibers of different sizes are mixed within the nerve
– As peripheral nerve approaches DRG
• Large caliber fibers are more dorsomedial
• Small caliber fibers are more anterolateral
1. Dorsal root ganglion2. Ventral root3. Pia mater 4. Arachnoid5. Dura mater6. Dorsal root7. Subarachnoid space8. Gray matter9. White matter10. Spinal Nerve
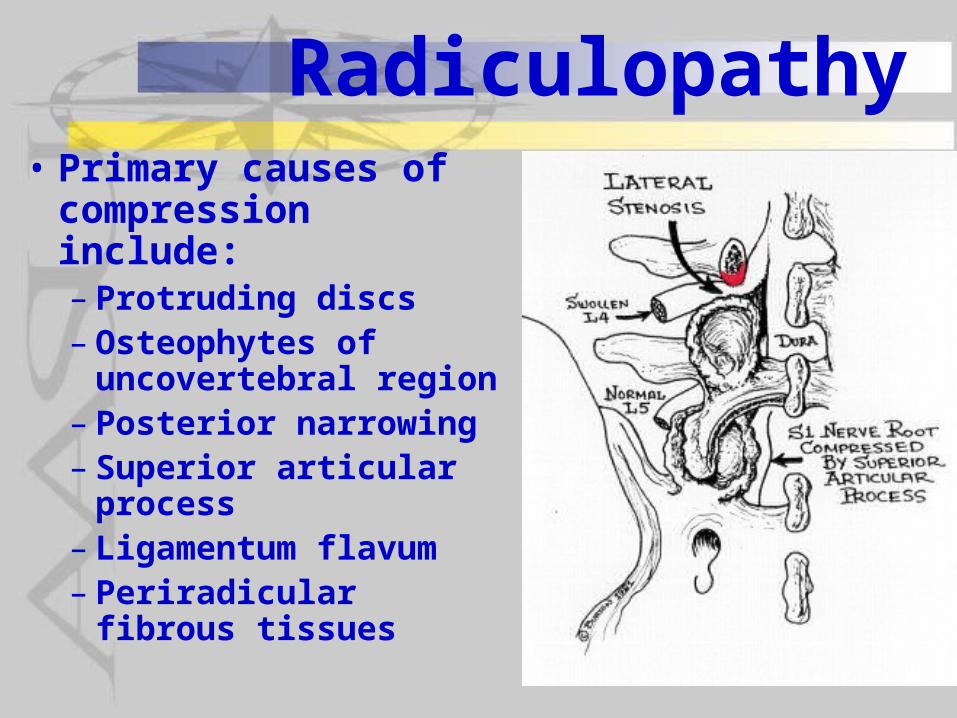
Radiculopathy• Primary causes of
compression include:– Protruding discs– Osteophytes of
uncovertebral region– Posterior narrowing– Superior articular
process– Ligamentum flavum– Periradicular fibrous
tissues
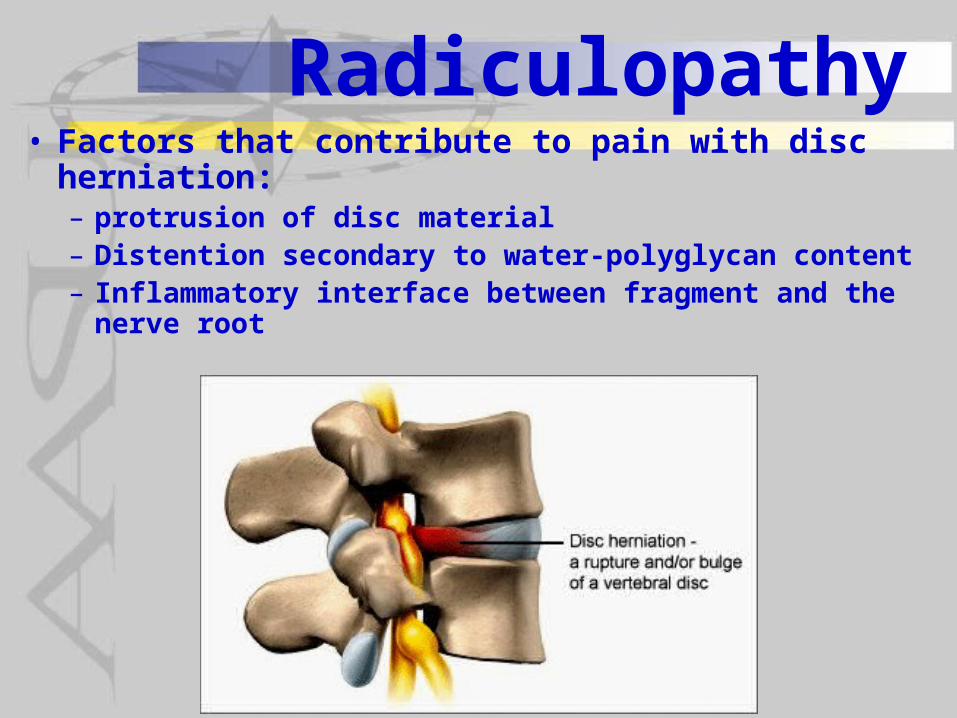
Radiculopathy• Factors that contribute to pain with disc
herniation:– protrusion of disc material– Distention secondary to water-polyglycan content– Inflammatory interface between fragment and the
nerve root
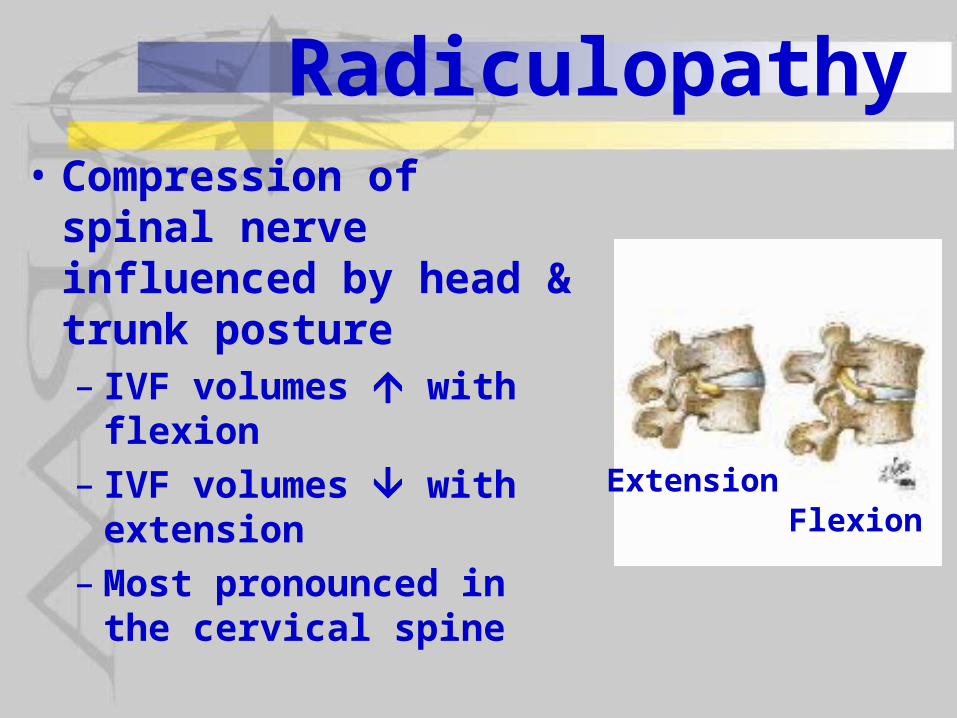
Radiculopathy• Compression of spinal
nerve influenced by head & trunk posture– IVF volumes with flexion– IVF volumes with
extension– Most pronounced in the
cervical spine
ExtensionFlexion

Radiculopathy• Compression of
spinal nerve influenced by head & trunk posture– Cervical rotation
further IVF volume ipsilateral to the rotation direction
IVF volume contralateral to the rotation direction
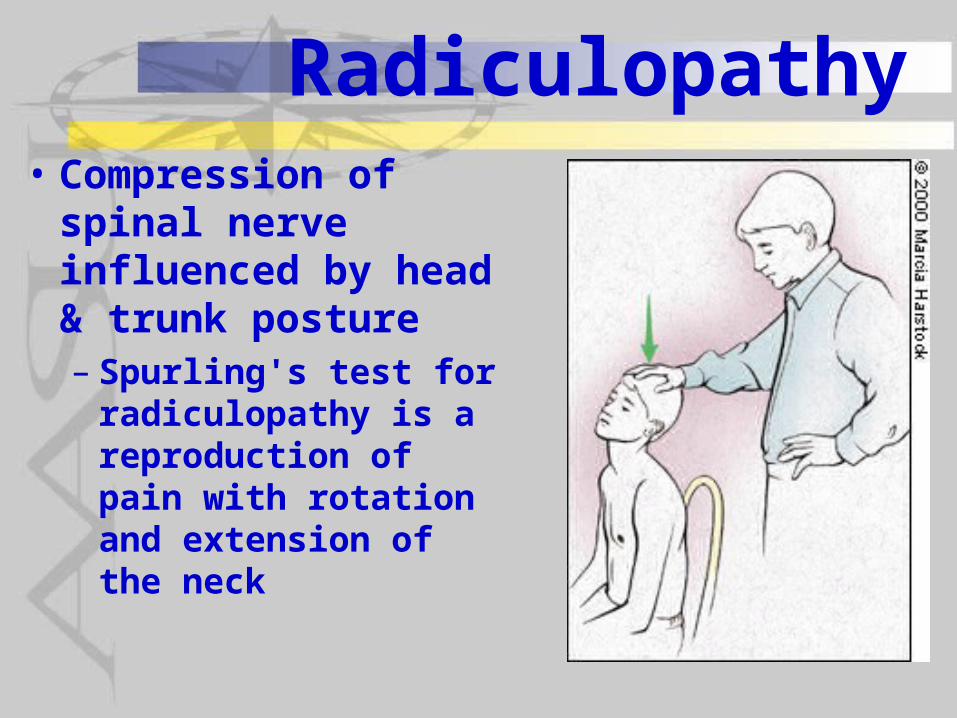
Radiculopathy• Compression of
spinal nerve influenced by head & trunk posture– Spurling's test for
radiculopathy is a reproduction of pain with rotation and extension of the neck
Radiculopathy• Compression of spinal nerve
influenced by head & trunk posture– Extension of the cervical spine relaxes
the spinal nerve root• Relaxing the nerve its diameter• The nerve dural sleeve is relaxed and thicker
so fills more of the IVF compression is applied to the spinal nerve
– Flexion stretches, straightens and thins nerve and the sheath and thus spinal nerve compression
Radiculopathy• Inflammation similar to seen
elsewhere: phospholipid A activity which
produces PGE2 & leukotrienes
Nitric oxide Cytokine release - such as
interleukins, TNF-– Macrophage invasion into inflamed site
Radiculopathy
Sequence of EventsCOMPRESSION edema fibroblast invasion
INJURY TO THE NERVE fibrotic tissues
risk of adhesion of
traction injuries the nerve which
to the nerve immobilizes it
Radiculopathy• Classic Signs and Symptoms
– Sensory Abnormalities• Pain• Paresthesia• hypesthesia & numbness• hypesthesia and numbness often follow
dermatomal patterns• pain & paresthesia may of may not
follow dermatomal patterns depending upon if there is paraspinal muscle involvement
Radiculopathy• Classic Signs and Symptoms
– Sensory Abnormalities• Progression from neuropraxia to
axonotmesis from conduction block to discontinuity of the axons
• There may be regeneration if axonotmesis, but if spouting occurs locally without regeneration can form neuromas which may be the cause of "electric pain" sensations
nerve irritability - hypersensitivity of the nerve to compression and stretch
Radiculopathy• Classic Signs and Symptoms
DTRs - muscle stretch reflexes– Paresis - muscle weakness– Muscle atrophy
– Dysautonomia & trophic changes (pilomotor, sweating, skin changes) are most associated with peripheral nerve damage but can also occur with radiculopathy
Radiculopathy• Classic Signs and Symptoms
– Complex pain patterns – Can be myotomal or sclerotomal as
well as dermotomal patterns incidence of peripheral pain
syndromes such as complex regional pain syndrome - CRPS (previously called reflex sympathetic dystrophy - RSD)
Radiculopathy• Diagnosis
– Most commonly diagnosed using needle EMG

Radiculopathy• Diagnosis
– Only useful in diagnosis of motor nerve disturbances - not seen with dorsal root lesions (sensory only)
– Seen as abnormal EMG activity in two or more muscles along same spinal nerve distribution (segmental innervation)
– Abnormal EMG activity in the paraspinals

Radiculopathy• Diagnosis
– Abnormal EMG activity is characterized by:
• Prolonged or enhanced "insertional" activity
Radiculopathy• Diagnosis
– Abnormal EMG activity is characterized by:
• Spontaneous sharp positive waves and fibrillation of fasciculation potentials
• Altered morphology of motor unit action potentials
• Poor recruitment of MUAPs• If dorsal root disorder, normal MUAPs but
slowed or blocked H-wave evoked reflex or diminished somatosensory evoked potentials
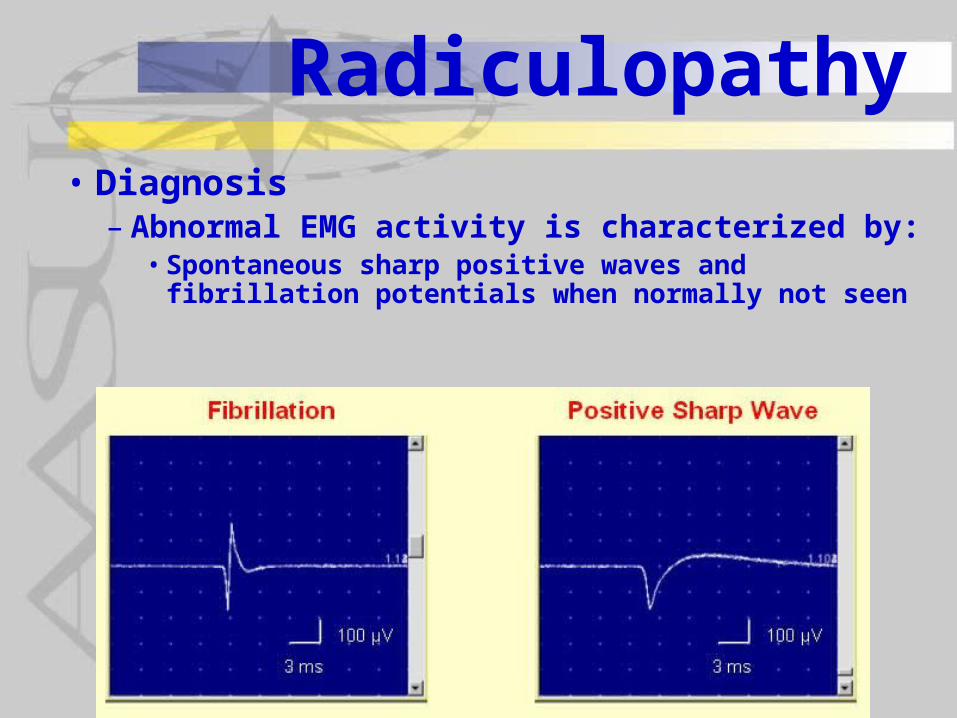
Radiculopathy• Diagnosis
– Abnormal EMG activity is characterized by:• Spontaneous sharp positive waves and
fibrillation potentials when normally not seen
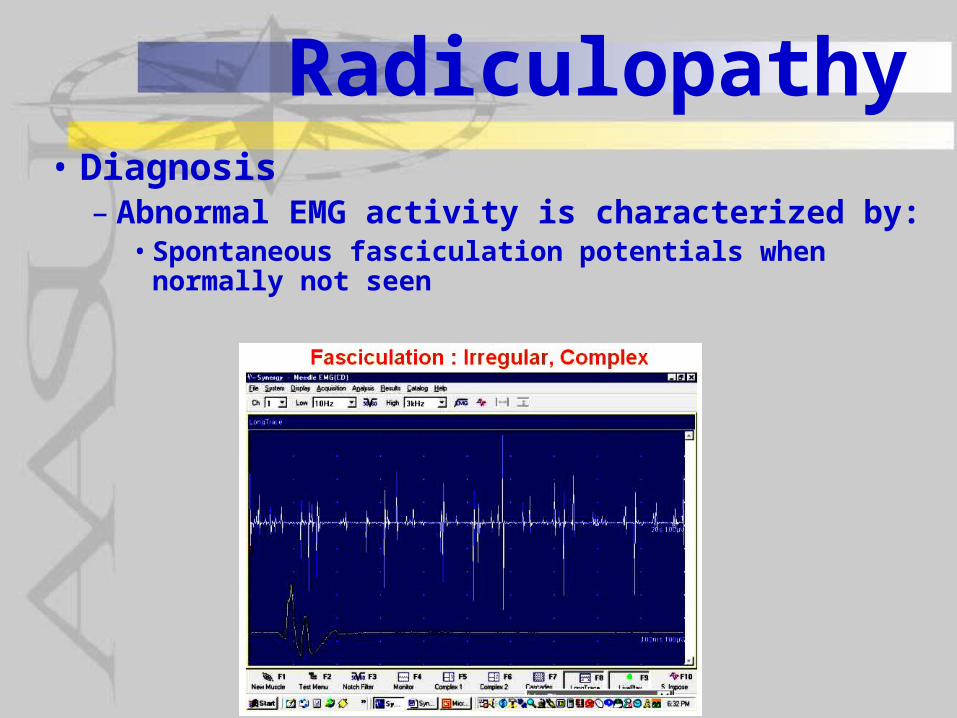
Radiculopathy• Diagnosis
– Abnormal EMG activity is characterized by:• Spontaneous fasciculation potentials when
normally not seen

Radiculopathy• Diagnosis
– Abnormal EMG activity is characterized by:
• Altered morphology of motor unit action potentials from normal biphasic to polyphasic potentials
Normal biphasic motor unit action potentials (MUAP) superimposed upon motor endplate potentials (MEPP)
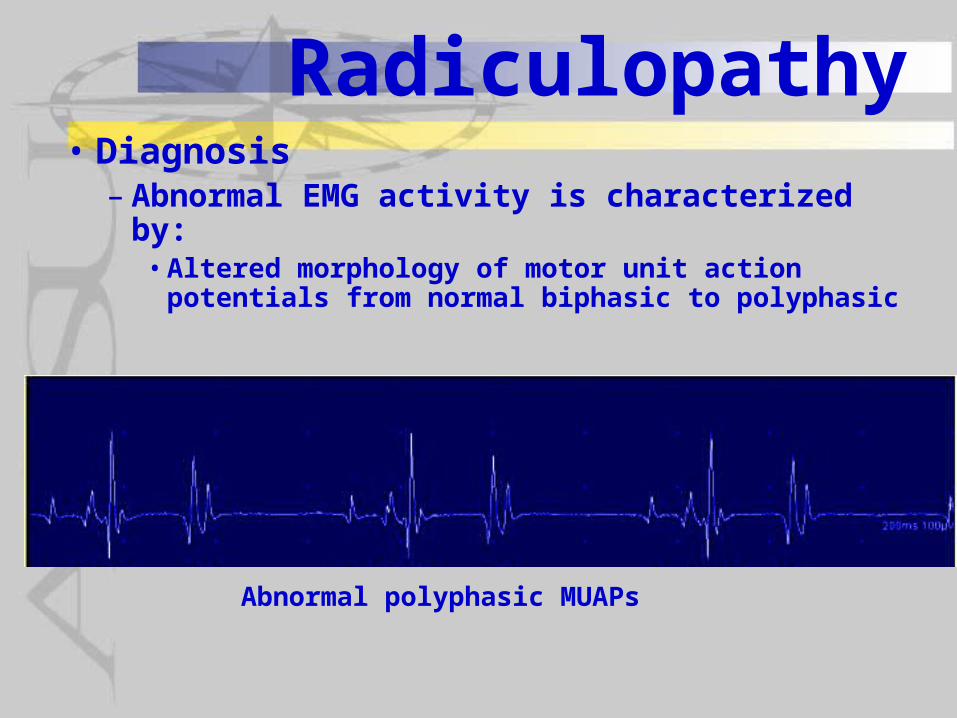
Radiculopathy• Diagnosis
– Abnormal EMG activity is characterized by:• Altered morphology of motor unit action
potentials from normal biphasic to polyphasic
Abnormal polyphasic MUAPs

Radiculopathy• Diagnosis
– Abnormal EMG activity is characterized by:• Poor recruitment of MUAPs seen as decreased
maximal activity (interference pattern) when maximal voluntary contraction
Reduced
Normal
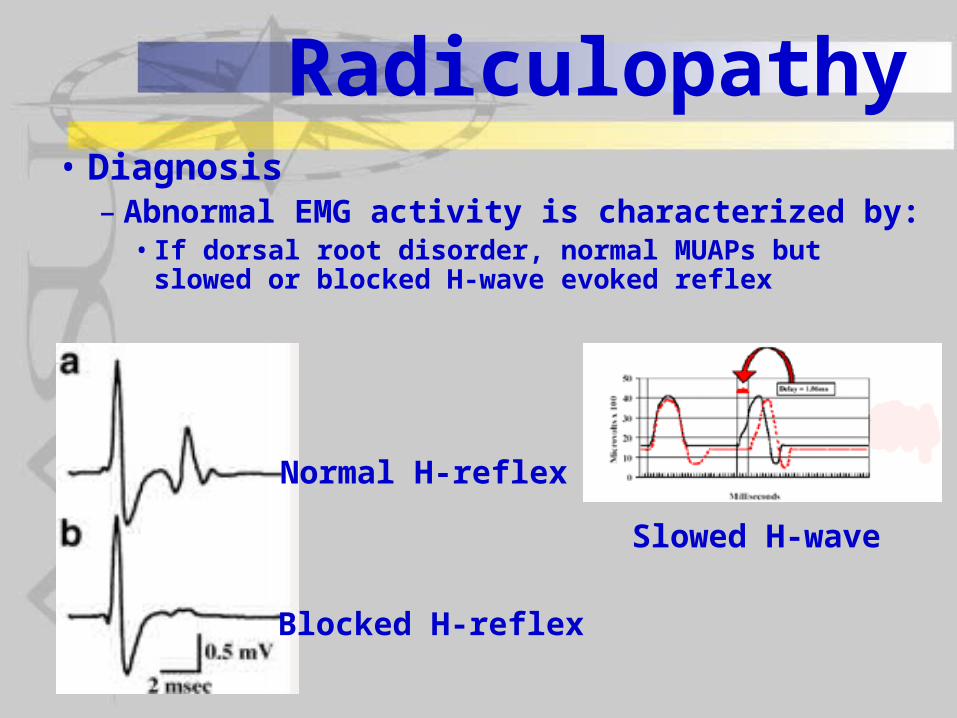
Radiculopathy• Diagnosis
– Abnormal EMG activity is characterized by:• If dorsal root disorder, normal MUAPs but slowed
or blocked H-wave evoked reflex
Normal H-reflex
Blocked H-reflex
Slowed H-wave

Radiculopathy• What is an H-reflex?
– Electrical stretch reflex– Stretch reflex - stretched muscle reflexively
contracts

Radiculopathy• What is an H-reflex?
– Electrically stimulate nerve to muscle so stimulate both sensory afferent (Ia) and motor efferent
– Record from muscle
Stimulate nerve to muscle which includes both motor & sensory fibers
Record electrical activity in the muscle

Radiculopathy• What is an H-reflex?
– When stimulate motor fibers there is a short distance traveled
– A short distance traveled will produce a short latency potential recorded from muscle
Stimulate motor fibers
Record electrical activity in the
muscle
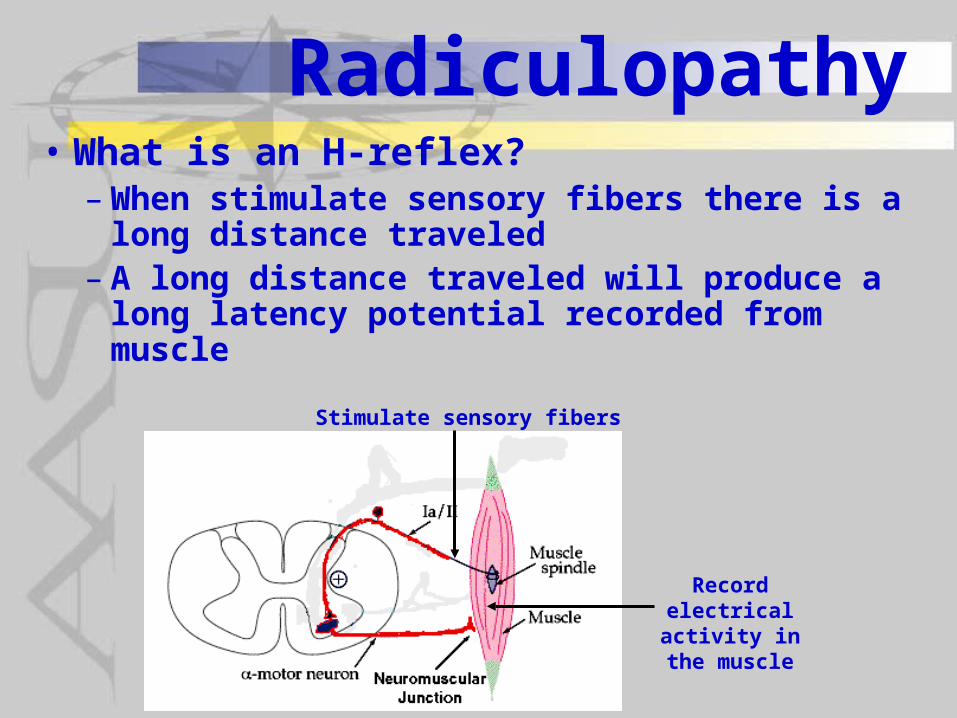
Radiculopathy• What is an H-reflex?
– When stimulate sensory fibers there is a long distance traveled
– A long distance traveled will produce a long latency potential recorded from muscle
Stimulate sensory fibers
Record electrical activity in the
muscle
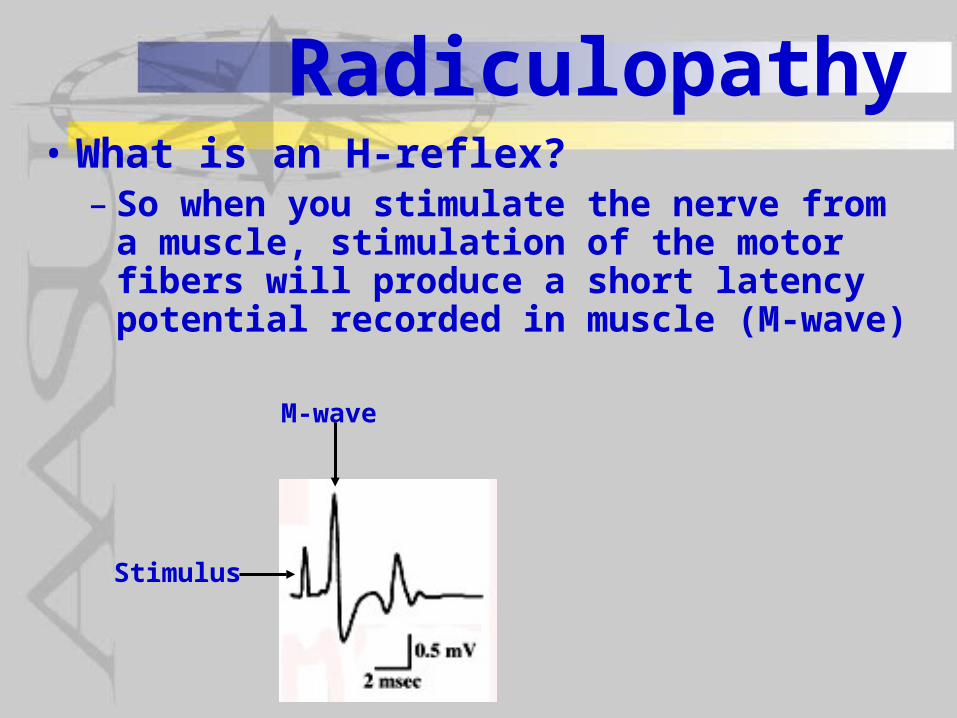
Radiculopathy• What is an H-reflex?
– So when you stimulate the nerve from a muscle, stimulation of the motor fibers will produce a short latency potential recorded in muscle (M-wave)
Stimulus
M-wave
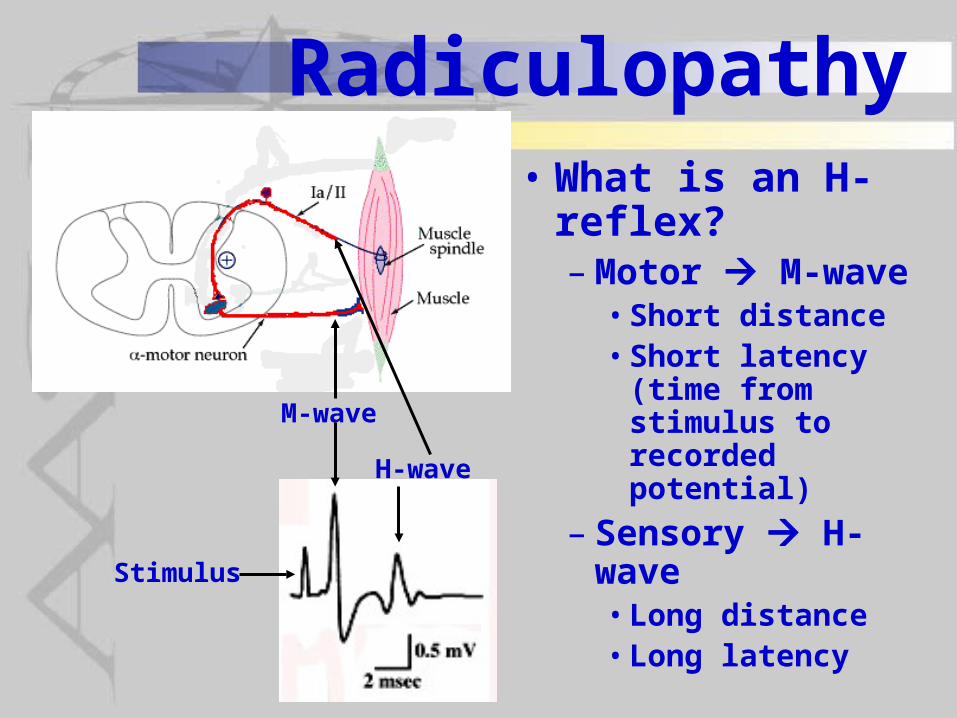
Radiculopathy• What is an H-
reflex?– Motor M-wave
• Short distance• Short latency (time
from stimulus to recorded potential)
– Sensory H-wave• Long distance• Long latencyStimulus
M-wave
H-wave

Radiculopathy• If damage is along
the dorsal root– There should be no
effect on the motor response (M-wave)
– However the sensory response (H-wave) should be blocked
Stimulus
M-wave
H-wave
X
XSite of Damage
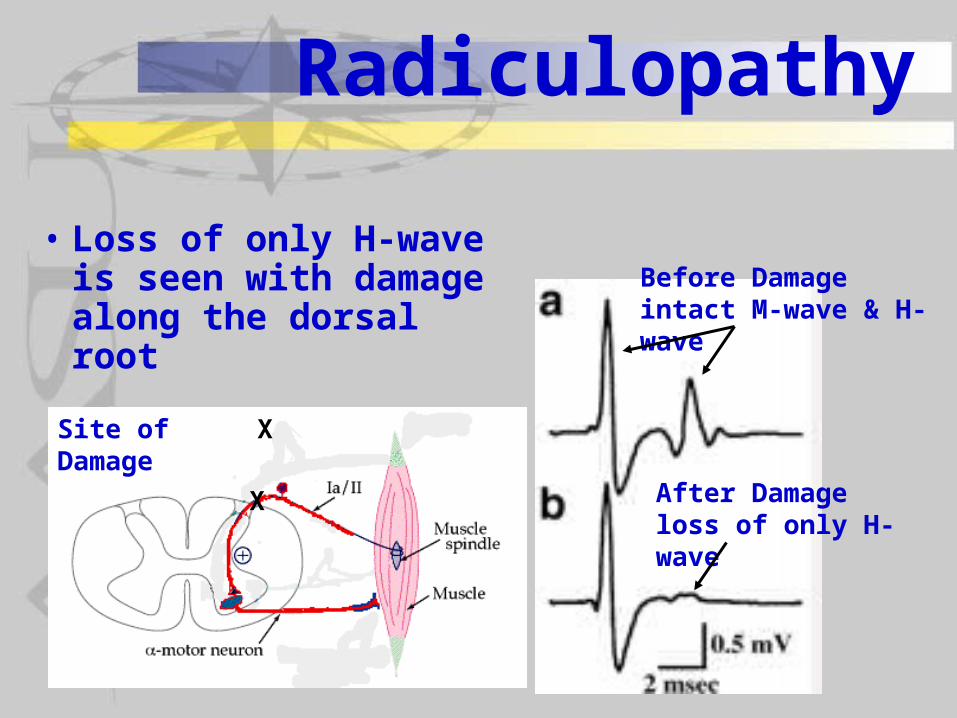
Radiculopathy
• Loss of only H-wave is seen with damage along the dorsal root
X
XSite of Damage
Before Damage intact M-wave & H-wave
After Damage loss of only H-wave
Radiculopathy• What is an H-reflex?
– So when you stimulate the nerve from a muscle, stimulation of the motor fibers will produce a short latency potential recorded in muscle (M-wave)